
Abstract
The term institutional betrayal (Smith and Freyd, 2014) builds on the conceptual framework of betrayal trauma theory (see Freyd, 1996) to describe the ways that institutions (e.g., universities, workplaces) fail to take appropriate steps to prevent and/or respond appropriately to interpersonal trauma. A nascent literature has begun to describe individual costs associated with institutional betrayal throughout the United States (U.S.), with implications for public policy and institutional practice. A scoping review was conducted to quantify existing study characteristics and key findings to guide research and practice going forward. Multiple academic databases were searched for keywords (i.e., “institutional betrayal” and “organizational betrayal”). Thirty-seven articles met inclusion criteria (i.e., peer-reviewed empirical studies of institutional betrayal) and were included in analyses. Results identified research approaches, populations and settings, and predictor and outcome variables frequently studied in relation to institutional betrayal. This scoping review describes a strong foundation of published studies and provides recommendations for future research, including longitudinal research with diverse individuals across diverse institutional settings. The growing evidence for action has broad implications for research-informed policy and institutional practice.
More than twenty years ago, betrayal trauma theory (BTT) articulated the central role of interpersonal betrayal in abuse (see Freyd, 1996). In particular, betrayal trauma theory drew on attachment theory (Bowlby, 1982; Bowlby 1988; Ainsworth & Bowlby, 1991; Ainsworth, 1973) and social contracts (Cosmides, 1989) to propose that victims who depend on their abusers face pressures to minimize awareness of the abuse in order to maintain necessary attachments. At a time when the field was largely focused on the fear component of trauma, the theory pointed out that traumas could vary in the degree to which they involved social betrayal. When traumas were high in betrayal, such as in cases of abuse perpetrated by parents or intimate partners, the theory predicted that dissociation as well as disruptions in attention and memory could help victims maintain the necessary-but-abusive attachments. Indeed, victims of trauma with high betrayal report greater dissociation as well as disruptions in memory and attention compared to those who experience traumas that are lower betrayal (e.g., DePrince et al., 2012). High betrayal traumas have also been linked with more severe psychological symptoms, more physical health problems (Goldsmith et al., 2012), and greater disruptions in interpersonal relationships than those who did not experience high betrayal (DePrince et al., 2009).
As research on betrayal traumas has grown, so has recognition that people can also be dependent on institutions, such as schools and faith organizations. Institutions have the potential to put those who depend on them in harm’s way, through acts of omission or commission. For example, investigations into child abuse allegations in the Catholic Church revealed patterns of allowing priests previously accused of child abuse continued contact with children (e.g., Böhm et al., 2013; Dale & Alpert, 2008). Here, abusive individuals with institutionally sanctioned power actively harmed those who were entrusted to their care (act of commission). In tandem, the Church’s lack of action to disrupt abusive patterns, allowing continued abuse by church leaders, further betrayed the institution’s members (act of omission). Similarly, investigative reporting in recent years has revealed that institutions of higher education can also fail students through action and inaction (e.g., Bunn, 2022; Dwyer, 2019). For example, some universities have supported campus subcultures where abuse is normalized (commission) or minimized and dismissed their responsibility to protect their students (omission), such as by allowing accusations of sexual assault involving student athletes to remain unresolved during the sport season (e.g., Moorman & Osborne, 2015).
Building on the conceptual framework of betrayal trauma theory, Smith and Freyd elevated the term institutional betrayal in the American Psychologist in 2014. The term described institutional (e.g., university, workplace, church) actions that failed to take appropriate steps to prevent an interpersonal trauma from occurring and/or respond adequately after a trauma occurred. Identifying the ways in which institutions actively and passively contribute to harming those who depend upon them is critical to developing policies and practice that can interrupt and repair institutional betrayal.
Since Smith and Freyd’s American Psychologist paper was published, a growing number of studies have appeared in academic journals to describe individual costs associated with institutional betrayals in the U.S., from healthcare (Smith, 2017) to academic (Wright et al., 2017) settings. In turn, academic and public calls to understand and address institutional betrayal have grown (e.g., Brown, 2021), with enormous implications for public policy and institutional practice. In light of the scientific and cultural relevance of institutional betrayal, a scoping review is urgently needed to quantify study characteristics and key findings to date to guide research and practice going forward.
Scoping reviews are a relatively new approach to synthesizing research and are meant to capture the state of the literature regarding a specific and relatively new topic (Arksey & O’Malley, 2005; Munn et al., 2018). In particular, scoping reviews provide information regarding the quantity and characteristics of relevant studies and are conducted when a field of study is beginning to grow (Arksey & O’Malley, 2005; Munn et al., 2018). Quantifying and describing the available research in this way should provide information about gaps in the literature, positing additional research questions that may be important to explore (Arksey & O’Malley, 2005; Munn et al., 2018). Therefore, this scoping review summarizes the state of the literature on institutional betrayal in terms of 1) study designs used and variables of interest studied to date; 2) key findings; and 3) researchers’ calls for future directions. With a focus on institutional acts of omission or commission that inflict trauma, violence, and abuse through a betrayal trauma theory lens, the scoping review will elucidate implications for policy and practice as well as next steps for the field.
Methods
Industry guidelines for conducting scoping reviews were employed for the current review, in accordance with the Arksey and O’Malley framework and the Joanna Briggs Institute (JBI) method (Arksey & O’Malley, 2005; Peters et al., 2015). We identified institutional betrayal as our research focus, with the intentional decision to not impose strict limitations on search terms and study designs. PsychINFO, ERIC, Academic Search Complete, and Business Source Complete were searched in early 2021 (i.e., February of 2021). An initial search employing "institutional betrayal," the key term utilized in the betrayal trauma literature to refer to systemic offenses against members of an institution, was conducted to identify related key words that should be included in the larger search. One additional keyword was identified during this process; therefore keywords utilized to search for relevant articles to be considered for the scoping review included “institutional betrayal” and “organizational betrayal.” From these searches, 492 studies were imported to Covidence (Veritas Health Innovation, 2021), a software program designed to assist researchers in conducting reviews. Covidence removed 322 duplicate studies, leaving 170 studies to be screened by two researchers. After screening the remaining studies, using article titles and abstracts, 44 studies remained, which were then examined for full-text eligibility (Table 1). Inclusion criteria indicated that articles included in analyses should be: (1) empirical studies of institutional betrayal and (2) peer-reviewed articles or dissertation projects. Dissertation projects were included because Bobek’s dissertation (2011) first introduced the term “institutional betrayal” demonstrating the value of relatively new researchers expanding the trauma literature in meaningful ways.
PRISMA.


Per the JBI method, we selected the studies aligned with the objective of this review and adhered to the guidelines for extracting studies, as depicted in search decision flowchart (Table 1). Thirty-seven (n = 37) articles met the established criteria. Prior to initiating data coding, the reviewers developed a standardized approach aligned with the existing literature on coding for scoping reviews. After determining the target variables of the scoping review (i.e., year of publication, field of study, purpose, inclusion criteria, demographic information, sample size, study design, measure of institutional betrayal, predictor and outcome variables, cultural considerations, and key findings related to institutional betrayal), three graduate-level students coded those variables across the 37 identified articles. Each study was exclusively charted by one coder, without blinding due to the exploratory nature of this review.
Results
Study Design and Variables of Interest
The final data set consisted of 37 peer-reviewed articles and dissertations published between 2011 to 2022, reporting findings related to institutional betrayal. The majority of articles (73%; n = 27) were published in psychological journals. Meanwhile, the remaining ten articles were published in journals from a variety of fields including: healthcare (n = 2), nursing (n = 2), higher education (n = 2), public health (n = 1), disability studies (n = 1), social work (n = 1), and psychiatry (n = 1).
Study Aims
Among the 37 articles, most primarily aimed to systematically examine institutional betrayal in some capacity. Bobek’s dissertation (2011) was the first paper to explore institutional betrayal, specifically identifying what type of experiences constitute betrayal among U.S. military veterans using primarily qualitative methods. Subsequently, two articles focused on measure development of the Institutional Betrayal Questionnaire (IBQ; Smith & Freyd, 2013). First, Smith and Freyd described the creation and initial validation of the IBQ, consisting of 10 items, that assess respondents’ experiences of institutional betrayal. Second, eight years after the introduction of the IBQ, Reffi, Pinciotti, and Orcutt (2021) assessed the construct validity of the IBQ-Version 2 and evaluated the factor structure, which included additional items that had been developed in Smith’s dissertation (2017).
Nearly a quarter of the studies (22%, n = 8) aimed to assess the occurrence of institutional betrayal in specific populations, such as university graduate students or U.S. military veterans, establishing the presence of institutional betrayal across a variety of unique populations. Similarly, researchers also were interested in examining institutional betrayal in relation to formal systems such as the healthcare system, government institutions, and the U.S. military (24%, n = 9). About one in three studies (32%, n = 12) set out to measure negative outcomes, such as psychological symptoms, physical problems, and academic outcomes, in relation to experiences of institutional betrayal within these populations and settings. Aims to identify relationships between experiences of institutional betrayal and variables related to identity (e.g., LGBT identity, race) were specifically stated by five studies (14%). Thirty-eight percent of the studies (n = 14) included additional aims that were not specific to institutional betrayal, indicating the examination of institutional betrayal in tandem with other research questions and aims.
Study Population and Settings
The majority of studies were conducted with U.S. military veterans and college/university members (See Table 2). The volume of work within these settings evinces a well-established relationship between institutional betrayal and these major U.S. institutions. Specifically, more than a quarter of the studies (27%, n = 10) involved U.S. military populations, and almost half (49%, n = 18) involved college or university members.
Study Characteristics.
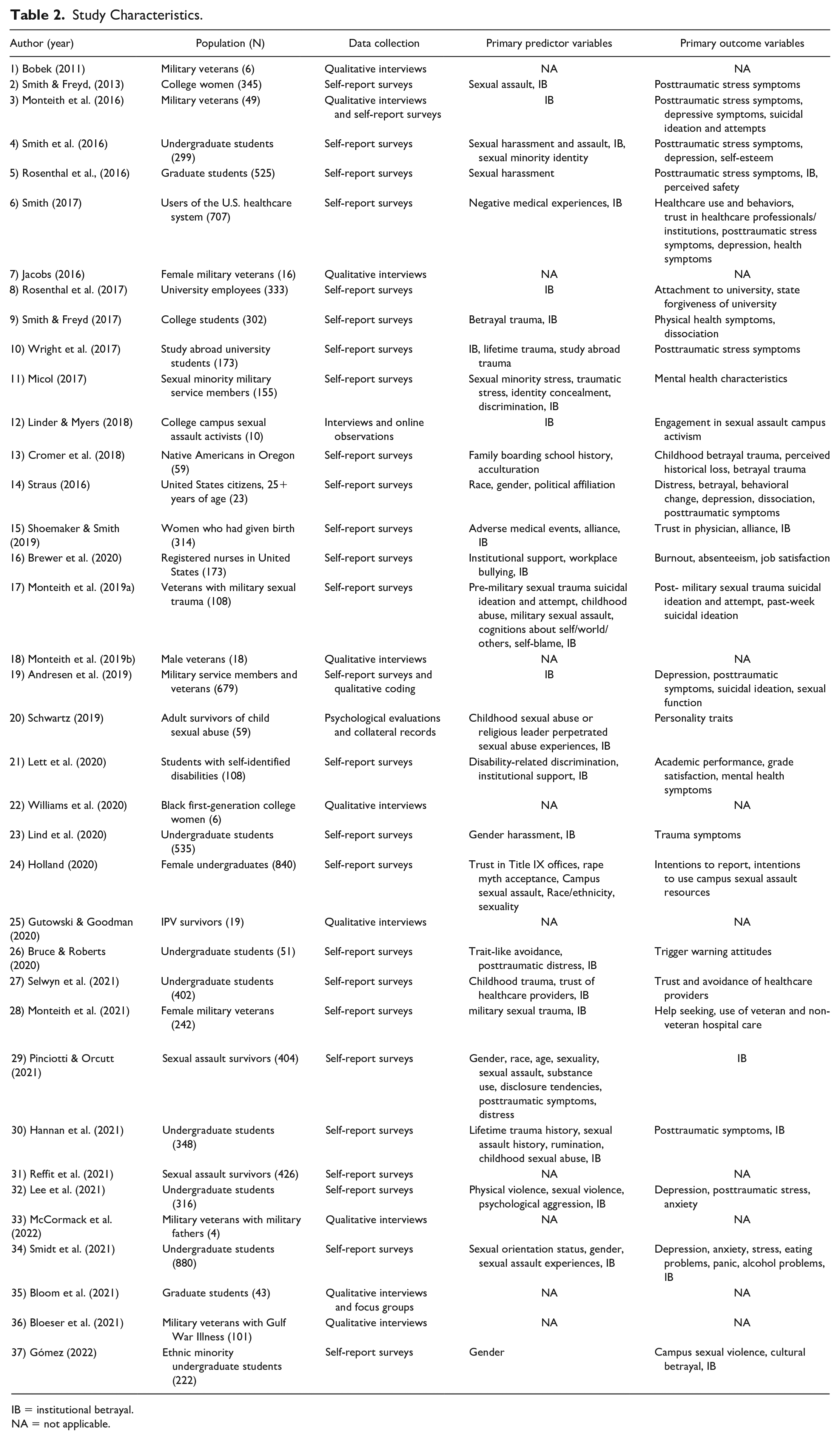
IB = institutional betrayal.
NA = not applicable.
Undergraduate students were the most studied population within the university setting, which could reflect that institutional betrayal is a particular concern in this population or that this population is one that is frequently studied, perhaps due to the accessibility of this population for researchers. In a rare exception to the undergraduate focus, Bloom and colleagues (2021) conducted the only study of graduate students’ experiences with sexual violence and harassment in relation to institutional betrayal, highlighting the especially precarious situations of graduate students within university systems. Among university-based studies, work has been evolving to address institutional betrayal in the context of other forms of oppression. For example, Williams et al. (2020) and Gómez (2022) sought to understand the role of undergraduates’ racial-ethnic minority identity in relation to institutional betrayal at Predominately White Institutions. Lett et al.’s (2020) work focused on whether institutional betrayal was related to disability status, and in turn, associations with academic performance and mental health symptoms.
Beyond general student populations, other groups within university settings have also received attention. Specifically, Rosenthal et al. (2017) examined university employees’ experiences of institutional betrayal after experiencing sexual assault on their campus. The following year, Linder and Myers (2018) published their work examining the relationship between institutional betrayal and campus sexual assault activists.
A minority of studies included in this review took place outside university or military settings. Three studies (8%) focused on U.S. healthcare systems, involving both healthcare users (Smith, 2017; Shoemaker & Smith, 2019) and providers (i.e., registered nurses; Brewer et al., 2020). Even though the volume of studies demonstrating the relationship between institutional betrayal within the U.S. healthcare system is not as robust compared to military and university settings, the small number of studies spanning across different populations within those systems (i.e., both patrons and providers) points to the possibility of vast instances and iterations of institutional betrayal perpetrated by healthcare systems in the U.S.
Evidence to support that institutional betrayal is also found within government institutions within the U.S. includes studies that examined institutional betrayal among a variety of broad populations. For example, Straus (2018) surveyed more than 200 adult U.S. citizens regarding their experiences of institutional betrayal related to ten controversial events perpetrated by U.S. political or public institutions (e.g., government’s respond to Hurricane Katrina, police shootings of unarmed African Americans, police corruption). Gutowski and Goodman (2020) documented the negative experiences of mothers seeking legal custody of their children through the U.S. court system in the context of intimate partner violence. Similarly, Cromer et al. (2018) surveyed a sample of Native Americans located in Oregon regarding institutional betrayal related to historical trauma. These studies demonstrate that entities central to individuals’ lives, such as government institutions, can also perpetrate institutional betrayal.
A potentially surprising result from this scoping review revealed that only one study examined experiences of institutional betrayal within a religious setting. Schwartz’s dissertation (2019) was the only study to examine child sexual abuse in relation to abuse perpetrated by religious leaders. The lack of studies examining institutional betrayal within a religious setting is surprising given that child sexual abuse perpetrated by religious leaders has been a major public critique of religious institutions.
Study Demographics
Among the ten studies conducted with U.S. military personnel, six studies had majority White participants. Among the studies that were conducted within the military, only one study centered sexual group membership as an important factor to consider (Micol, 2017), and only an additional two studies included participants’ sexual orientation in the demographic information. Both of these studies reported relatively low participation of individuals with minoritized sexual identities (Monteith et al., 2019a; Monteith et al., 2019b). The lack of representation of sexual minorities within the majority of the military-based settings may signal an important gap in the literature given well-known anti-LGBTQIA+ discrimination (e.g., “Don’t Ask, Don’t Tell” legislation; see Burks, 2011).
Across the eighteen studies that involved college or university members (i.e., students and employees), the majority of the participants were also White, and eight studies reported information on sexual minority group membership. Although Holland (2020) hypothesized an interaction between trust in Title IX offices and racial/ethnic and sexual identities among female college students, the predominantly White and heterosexual sample limited the ability to examine these potentially important factors. Two studies, both within the university context, centered the experiences of students with racially/ethnically minoritized identities (Williams et al., 2020; Gómez, 2022). Although studies conducted within the university context have centered the role of minoritized identities relatively more frequently compared to those within the military setting, a significant gap addressing how institutional betrayal and minoritized and intersectional identities are related is severely lacking.
Sample Sizes
Sample sizes widely differed across the articles, ranging from less than 10 participants to nearly 900 participants. Eight percent (n = 3) of studies consisted of sample sizes of less than 10, which were all qualitative studies conducting qualitative interviews. Sixteen percent (n = 6) of studies had 10 to 50 participants. Three (8%) studies had between 51 and 99 participants. Six studies (16%) had participants within the 100 range, and another 16% (n = 6) had between 300 and 399 participants. Eleven percent (n = 4) of the studies had 200-299 participants. Another 8% n = 3) had between 400 and 499 participants. The remaining six studies (16%) had 500 or more participants. In contrast to qualitative interviews, studies reporting these higher number of participants relied primarily on self-report as well as convenience samples, such as undergraduate students required to participate in psychology studies.
Study Designs
Almost all of the studies utilized a cross-sectional design (97%, n = 36). Eight of the studies involved qualitative interviews (22%) and 25 used self-report surveys (68%). Two studies used a mixed methods approach. Specifically, Monteith et al. (2016) conducted qualitative interviews and administered self-report surveys. Linder and Myers (2018) utilized a unique approach to collect data related to sexual assault activists’ experiences with campus sexual assault by observing online communities as well as conducting qualitative interviews in their study. Schwartz (2019) was the only study that used archival data from two different samples. Taken together, qualitative interviews and self-reported data has been heavily relied upon by researchers examining institutional betrayal and related factors. This can be understood in the context of the relatively recent introduction of institutional betrayal, stemming from betrayal trauma theory; however, some researchers have also begun to explore additional means of assessing experiences of institutional betrayal.
Institutional Betrayal Measures Used
A majority of studies (62%, n = 23) used some form of the Institutional Betrayal Questionnaire (Smith & Freyd, 2013). Of the studies that used the IBQ, 19 used a modified version of the IBQ (51%). Smith and Freyd created the 10-item IBQ to assess institutional betrayal for the purposes of their 2013 study (referenced in this review). Four studies used the IBQ-Healthcare which is a 15-item modified version of the IBQ that assesses institutional betrayal specifically in healthcare settings. An additional four studies used the Institutional Betrayal and Support Questionnaire (IBSQ), a 26-item scale that assesses institutional failure to prevent sexual violence, active mishandling of reported cases, betrayals specific to race and sexual orientation, and institutional responses to reported cases. Lett and colleagues (2020) adapted the IBSQ to ask about events related to disability discrimination.
Beyond the variations of the IBQ, researchers relied on other methods to capture participants’ experiences of institutional betrayal. Cromer et al. (2018) used the Brief Betrayal Trauma Survey (BBTS), the Native American Acculturation Scale, and the Historical Losses Scale to examine the association between enculturation of Native American culture and awareness of historical trauma among Indigenous Peoples at the hands of the U.S. government through the lens of institutional betrayal. Straus (2018) created the Political Event Rating Form for their study to explore levels of distress and betrayal in response to controversial events that involved public institutions in the United States. Lastly, Holland (2020) developed two measures of trust for their study to assess trust in the Title IX Office’s ability to handle reports of sexual assault and to assess participant’s trust in the sexual assault center’s ability to assist survivors. These few studies demonstrate other avenues to capture individuals’ experiences of institutional betrayal beyond the IBQ.
Predictor Variables
Utilizing selected institutional betrayal measures, more than half of the total number of studies reviewed (n = 22, 60%) investigated relationships between institutional betrayal and harm with institutional betrayal as a predictor variable. In contrast, only two articles (5%) examined institutional support (Brewer et al., 2020; Lett et al., 2020). As might be expected, other variables measuring victimization were frequently included as predictors (n = 26, 70%), such as stalking, dating violence, betrayal trauma, traumatic stress, work-place bullying, military sexual assault, religious-leader perpetrated sexual abuse, experiences of discrimination, gender harassment, lifetime physical abuse, and lifetime sexual abuse. For example, researchers found that a history of child sexual abuse moderated the relationship between reports of rape in adolescence or adulthood and institutional betrayal, where those who reported histories of child sexual abuse and rape in adolescence or adulthood reported higher levels of institutional betrayal (Hannan et al., 2021). One in three studies (32%) systematically examined demographics variables as predictors (e.g., race, gender, sexuality, age, political affiliation) (see Table 2 and Table 3).
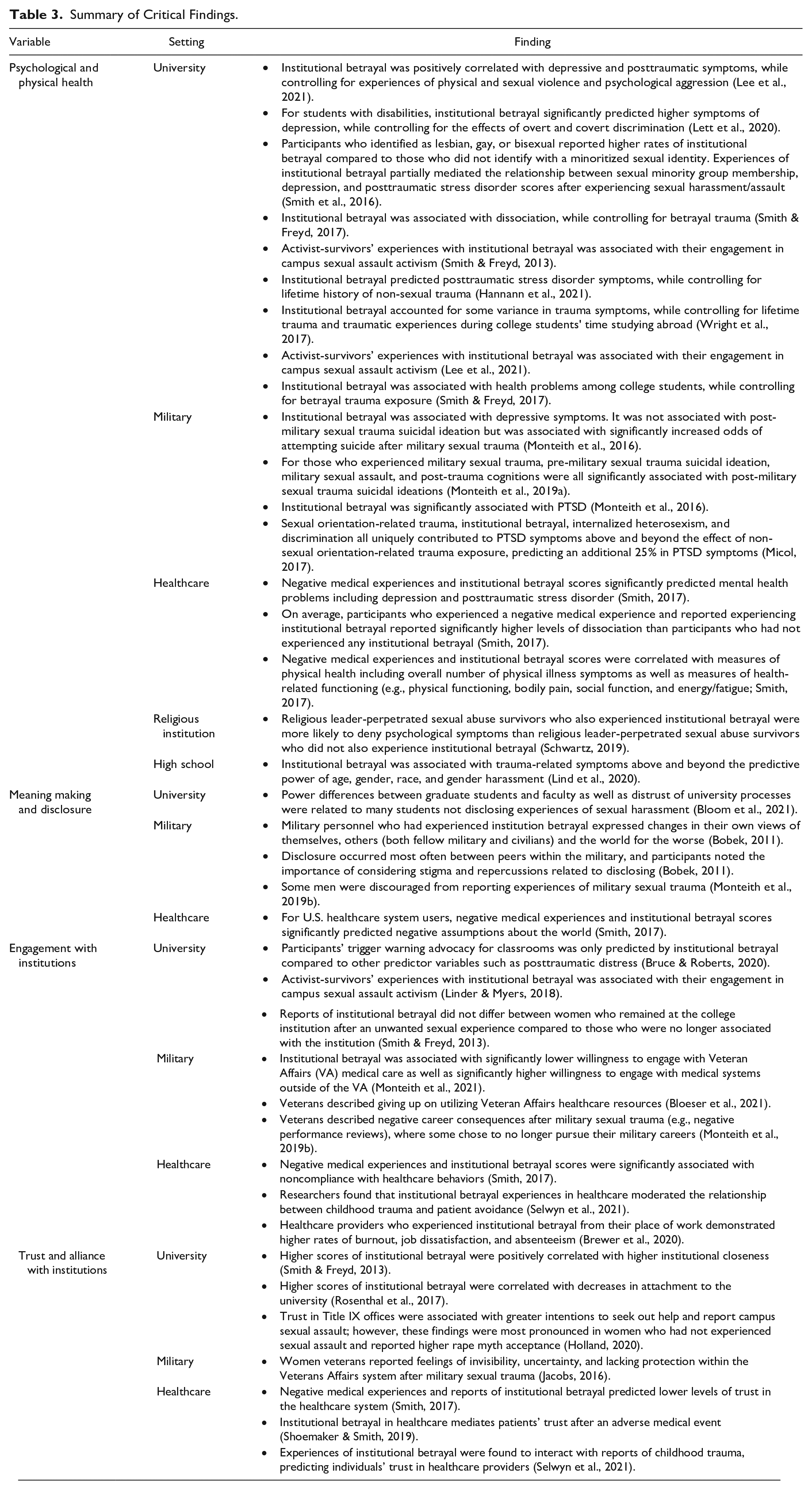
Summary of Critical Findings.
Outcome Variables
Of the 37 studies reviewed, only six (16%) tested institutional betrayal as an outcome variable, relative to the 60% that tested institutional betrayal as a predictor. This suggests that research has been more focused on documenting the consequences of institutional betrayal relative to the factors that predict its occurrence. Indeed, studies frequently examined mental health outcomes related to institutional betrayal (41%, n = 15). More general mental health outcomes examined included anxiety (11%, n = 4) and depression (27%, n = 10). More closely tied to participants’ mental health issues after traumatic experiences, eleven of the studies (30%) reported on posttraumatic stress disorder (PTSD) symptoms, six (16.2%) on dissociation, four (10.8%) on problematic sexual functioning, four (10.8%) on suicidal ideation and/or attempts, and three (8.1%) on experiences of sleep disturbance (see Table 2 and Table 3).
Beyond mental health outcomes, which were the most heavily researched outcome variables, seven studies (19%) examined behavioral outcomes such as engagement in campus sexual assault activism, help seeking behaviors, and absenteeism. A small number of studies (8%, n = 3) were interested in examining participants’ trust in healthcare institutions and providers as outcome variables. Additional outcome variables included experiences of distress, burnout, job satisfaction, state of forgiveness, feelings of attachment to their university, physical health, collective self-esteem, perceived safety around campus, academic performance, and grade satisfaction (see Table 2 and Table 3).
Key Findings
Prevalence of Institutional Betrayal
Much of the growing literature has focused on documenting the prevalence of institutional betrayal, which is not surprising given the study aims summarized earlier. Bobek’s 2011 study was the first to study institutional betrayal in a small military sample, documenting that all (N = 6) reported at least one instance of institutional betrayal by the military. Similarly, a sample of 49 U.S. military veterans revealed that nearly all (95.9%) participants reported at least one experience of institutional betrayal; and the most common types of betrayal included creating an environment which military sexual trauma was common, making it difficult to report military sexual trauma, and not taking preventative measures (Monteith et al., 2016). A sample of military veteran men who had histories of military sexual trauma reported similar experiences, suggesting that the U.S. military culture had contributed to their experiences with military sexual trauma through hazing rituals or perpetuating a highly sexualized environment (Monteith, 2019b). Across 101 qualitative interviews of U.S. military veterans living with Gulf War Illness, institutional betrayal was coded in nearly half of the veteran interviews, and institutional betrayal themes in interviews shaped how veterans engaged in future healthcare (Bloeser et al., 2021).
Within higher education, a handful of studies (11%, n = 4) examined the presence of institutional betrayal at universities in terms of both student and employee. Within a sample of 345 college women, Smith and Freyd (2013) found that nearly half (46%) of the women, who reported unwanted sexual experiences, reported experiencing at least one form of institutional betrayal regardless of the specific type of unwanted sexual experience. Similar to the evidence pertaining to military settings, the most frequent form of reported institutional betrayal involved perceptions of the institution creating an environment where unwanted sexual experiences seemed common and likely to occur (Smith & Freyd, 2013). In a sample of 222 racial-ethnic minority undergraduate students attending a Predominantly White University, over 90% of the participants who had been victimized reported experiencing institutional betrayal as well (Gómez, 2020). For university students who studied abroad outside of the U.S. (N = 173), 35.4% of students who reported any form of traumatic experience while studying abroad also reported experiencing at least one form of institutional betrayal (Wright et al., 2017). A substantial percentage of university employees (83%) also reported at least one experience of institutional betrayal (Rosenthal et al., 2017).
The volume of studies documenting institutional betrayal in both military and university settings is relatively large compared to those on institutional betrayal in other settings (i.e., healthcare, legal, and religious settings). To examine the occurrence of institutional betrayal within a healthcare context, Smith (2017) surveyed 707 U.S. healthcare system users online. Sixty-six percent of participants reported experiencing institutional betrayal in healthcare settings. Within the criminal-legal realm, Gutowski and Goodman’s content analysis demonstrated themes related to institutional betrayal, such as survivors experiencing harmful interactions with court professionals and court environments by implicitly presuming the absence of trauma (Gutowski and Goodman, 2020). Within a religious context, Schwartz and colleagues (2019) found no differences in Minnesota Multiphasic Personality Inventory scores (MMPI-2; a measure used to determine individuals’ mental illness symptoms or personality disorder) between those who reported child sexual abuse perpetrated by a religious leader with and without reports of institutional betrayal and those who reported child sexual abuse by a non-religious leader with and without reports of institutional betrayal.
Role of Social Identities
Five articles (13.5%) reported results highlighting the role of participants’ social identities. Two articles examined the role of sexual minority’s experiences within the context of institutional betrayal. Lesbian, gay, and bisexual college undergraduates reported higher rates of institutional betrayal compared to their straight counterparts, while controlling for the increased number of unwanted sexual experiences (Smith et al., 2016). Similar findings were reported in 2021, indicating that sexual minority groups were 1.67 times at risk for experiencing institutional betrayal compared to non-sexual minorities. Furthermore, sexual minority individuals were shown to experience more types of institutional betrayal compared to their peers (Smidt et al., 2021).
In contrast to the findings within the university setting, Pinciotti and Orcutt’s work (2021) —with sexual assault survivors via Amazon Turk— demonstrated that participants were more likely to report institutional betrayal if they identified as heterosexual. These differences may be due to differences in sampling methods and/or population and are important to highlight. Further work disentangling the role of minoritized sexual identities is needed to clarify these relationships.
Two articles reported findings related to racial identity. In a small qualitative study, researchers found that all six Black first generation college students reported experiencing or witnessing discrimination leading to institutional betrayal (William et al., 2020). Cromer and colleagues (2018) found evidence suggesting that institutional betrayal is an underlying mechanism in the negative impact of historical trauma within the Native American community. More specifically, researchers found that higher levels of identification with American Indian culture was associated with more thoughts related to historical loss. In contrast, the more individuals identified with White culture, the less they thought about historical loss (Cromer et al., 2018). However, Pinciotti and Orcutt (2021) revealed that race nor gender predicted institutional betrayal—again amplifying the need for additional research in different populations.
When comparing male to female experiences, two articles reported relevant findings. Researchers found evidence that graduate students that identify as male or female differ on factors that are associated with institutional betrayal. Specifically, sexual harassment by faculty or staff at graduate students’ university was significantly associated with institutional betrayal for female-identifying graduate students. In contrast, male-identifying students’ experiences of institutional betrayal were significantly associated with dating violence (Rosenthal et al., 2016). For ethnic minority undergraduate students, 97.7% of women reported institutional betrayal after campus sexual assault, which was significantly higher than their male peers (80.0%). In terms of institutional support, ethnic minority undergraduates did not experience gender differences (Gómez, 2022).
Results highlighting the role of intersectional identities and betrayal were reported by two articles. Race, gender, and political affiliation were reported to interact in complex ways to predict betrayal, as well as distress and self-reports of behavioral change in response to political events in the United States (Straus, 2018). Among U.S. adult residents, institutional betrayal was more likely to be reported by sexual assault survivors who identified as heterosexual, endorsed more severe symptoms of PTSD, and were older in age. In contrast, gender, race, assault characteristics, and disclosure tendencies did not predict risk for institutional betrayal (Pinciotti & Orcutt, 2021).
Psychological and Physical Health
A third of studies (35%, n = 13) reported on associations between institutional betrayal and psychological symptoms and demonstrated that experiences of institutional betrayal were important to consider in the aftermath of trauma when examining psychological outcomes. For example, within a university environment, Lee and colleagues’ (2021) survey of 316 undergraduate students at a private university uncovered that institutional betrayal was positively correlated with depressive symptoms, posttraumatic stress symptoms, and anxiety while controlling for experiences of physical and sexual violence and psychological aggression. Smith and Freyd (2013) found that college women who experienced both sexual assault and institutional betrayal reported higher levels of several posttraumatic stress symptoms than those who did not endorse institutional betrayal. Furthermore, institutional betrayal has also been associated with dissociation even when controlling for betrayal trauma (Smith & Freyd, 2017). In a similar vein, data from students at a private U.S. university revealed that institutional betrayal predicted PTSD symptoms even after controlling for lifetime history of non-sexual trauma. High rumination scores and institutional betrayal also independently predicted PTSD symptoms, although there was no significant interaction between the two (Hannan et al., 2021). For students who identified as having a disability, institutional betrayal significantly predicted higher symptoms of depression even after controlling for the effects of overt and covert discrimination. Importantly, institutional support did not appear to buffer against these experiences (Lett et al., 2020). Lastly, among undergraduate students who were studying abroad, experiences of institutional betrayal accounted for some variance in trauma symptoms even when controlling for lifetime trauma and traumatic experiences during time studying abroad (Wright et al., 2017). The findings from these studies demonstrate that institutions do in fact play a unique role apart from others experiences of trauma.
Lind and colleagues (2020) also helped establish that institutional betrayal occurs in high school settings, highlighting the presence and impact of institutional betrayal during adolescence. They investigated rates of gender harassment and institutional betrayal in high school and whether institutional betrayal moderated the relation between high school gender harassment and trauma symptoms during students’ undergraduate years. Although high school institutional betrayal did not moderate the relationship between previous gender harassment and college trauma-related symptoms, institutional betrayal was associated with trauma-related symptoms above and beyond the predictive power of age, gender, race, and gender harassment.
The role of institutional betrayal within the U.S. military on victims’ psychological well-being has also been examined. In a sample of U.S. military veterans, Monteith et al. (2016) found that perceived institutional betrayal was significantly associated with PTSD and depressive symptoms. However, in this study, institutional betrayal was not associate with post-military sexual trauma suicidal ideation but was associated with significantly increased odds of attempting suicide after military sexual trauma. Monteith and colleagues (2019a) found that among military veterans who had experienced military sexual trauma, pre-military sexual trauma suicidal ideation, military sexual assault, and post-trauma cognitions were all significantly associated with post- military sexual trauma suicidal ideations.
Two articles highlighted individuals with minoritized sexual identities and distress in relation to institutional betrayal. Smith and colleagues (2017) sought out to explore the relation between lesbian, gay, and bisexual identity, sexual harassment/assault, institutional betrayal, and psychological outcomes. They discovered that participants who identified as lesbian, gay, or bisexual reported higher rates of institutional betrayal. Furthermore, experiences of institutional betrayal partially mediated the relationship between sexual minority group membership, depression, and PTSD scores after experiencing sexual harassment/assault. Micol (2017) examined the relation between trauma exposure, sexual minority stress, and posttraumatic stress symptoms in sexual minority military service members. Through online surveys of 155 participants, Micol (2017) revealed that sexual orientation-related trauma, institutional betrayal, internalized heterosexism, and discrimination all uniquely contributed to PTSD symptoms above and beyond the effect of non-sexual orientation-related trauma exposure, predicting an additional 25% in PTSD symptoms.
Schwartz’s 2019 study examined the impact of religious leader-perpetrated sexual abuse on survivors’ personality profile as well as the role of institutional betrayal on psychological functioning for adult survivors of both religious leader-perpetrated sexual abuse and non-clerical child sexual abuse. Through comprehensive psychological evaluations and interviews of 59 adult survivors, the findings suggested that religious leader-perpetrated sexual abuse survivors who also experienced institutional betrayal were more likely to deny psychological symptoms than religious leader-perpetrated sexual abuse survivors who did not also experience institutional betrayal.
Smith (2017) explored institutional betrayal in healthcare settings, the relationship between racism and socio-economic status and negative medical experiences, institutional betrayal, and trust in healthcare professionals and organizations. Results showed that negative medical experiences and institutional betrayal scores significantly predicted mental health problems such as dissociation, symptoms of PTSD, and depression. Additionally, on average, the participants who had experienced institutional betrayal reported significantly higher levels of dissociation than participants who had not experienced any institutional betrayal.
Two articles presented findings on links between institutional betrayal and physical health. Smith (2017) reported that negative medical experiences and institutional betrayal scores were correlated with measures of physical health including overall number of physical illness symptoms and measures of health-related functioning (e.g., physical functioning, bodily pain, social function, and energy/fatigue). Smith and Freyd (2017) reported that institutional betrayal was associated with health problems among college students, even when controlling for betrayal trauma exposure.
Meaning Making and Disclosure
Smith (2017) and Bobek (2011) reported on meaning making associated with institutional betrayal. Smith (2017) demonstrated that among U.S. healthcare system users, negative medical experiences and institutional betrayal scores significantly predicted negative assumptions about the world. Similarly, Bobek (2011) reported that military personnel who had experienced institution betrayal expressed changes in their own views of themselves, others (both fellow military and civilians) and the world for the worse.
Approximately 8% of studies reported findings related to disclosing traumatic experiences in the context of institutional betrayal. Bobek (2011) found that disclosure occurred most often between peers within the military and noted the importance of considering stigma and repercussions related to disclosing. Another study set within the military (Monteith et al., 2019) found that some men were discouraged from reporting experiences of military sexual trauma. Lastly, within the university context, researchers found that power differences between graduate students and faculty as well as distrust of university processes were related to many students not disclosing experiences of sexual harassment (Bloom et al., 2021).
Engagement with Institutions
More than a quarter of studies (27%) described findings related to service engagement. Within veteran affair (VA) settings, two studies reported findings related to patient engagement with VA services after military sexual trauma. Monteith and colleagues (2021) found that institutional betrayal was associated with significantly lower willingness to engage with VA medical care as well as significantly higher willingness to engage with medical systems outside of the VA. Similar findings were reported by Bloeser et al. 2021, where themes emerged among veterans describing giving up on utilizing VA healthcare resources. Negative consequences for veterans were also described related to their careers within the military after military sexual trauma, such as negative performance reviews, where some chose to no longer pursue their military careers (Monteith et al., 2019b).
Within the university system, three studies described engagement with the academic institution in the context of institutional betrayal. Two studies found that experiences of institutional betrayal were associated with campus advocacy. Participants’ trigger warning advocacy for classrooms was only predicted by institutional betrayal compared to other predictor variables such as posttraumatic distress (Bruce & Roberts, 2020). Linder and Myers (2018) found that activist-survivors’ experiences with institutional betrayal was associated with their engagement in campus sexual assault activism. Smith & Freyd (2013) found that reports of institutional betrayal did not differ between women who remained at the college institution after the unwanted sexual experience compared to those who were no longer associated with the institution.
Institutional betrayal within the healthcare realm was shown to be related to patients’ medical engagement. Smith (2017) found that negative medical experiences and institutional betrayal scores were significantly associated with noncompliance with healthcare behaviors. In a different study, researchers found that institutional betrayal experiences in healthcare moderated the relationship between childhood trauma and patient avoidance (Selwyn et al., 2021). Parallel to patient experiences, healthcare providers who experienced institutional betrayal from their place of work demonstrated higher rates of burnout, job dissatisfaction, and absenteeism (Brewer et al., 2020).
Trust and Alliance with Institutions
The current literature also provides some information regarding individuals’ trust and alliance with institutions. Individuals’ relationships with universities demonstrated an important role in the context of institutional betrayal. Higher scores of institutional betrayal were positively correlated with higher institutional closeness (Smith & Freyd, 2013) and decreases in attachment to the university (Rosenthal et al., 2017). Furthermore, trust in Title IX offices were associated with greater intentions to seek out help and report campus sexual assault; however, these findings were most pronounced in women who had not experienced sexual assault and reported higher rape myth acceptance (Holland, 2020).
For patients seeking healthcare, negative medical experiences and reports of institutional betrayal predicted lower levels of trust in the healthcare system (Smith, 2017). Similarly, researchers found that institutional betrayal in healthcare mediates patients’ trust after an adverse medical event (Shoemaker & Smith, 2019). Experiences of institutional betrayal in healthcare were also found to interact with reports of childhood trauma, predicting individuals’ trust in health care providers (Selwyn et al., 2021). Women veterans reported feelings of invisibility, uncertainty, and lacking protection within the VA system after military sexual trauma (Jacobs, 2016).
Expanding the Concept of Institutional Betrayal
Two articles introduced novel ways to conceptualize experiences of institutional betrayal. Rosenthal, Smidt, and Freyd (2016) argued that any instance of sexual harassment that occurs in the context of an institution constitutes as institutional betrayal due to the institution’s failure to protect students. While Rosenthal and colleagues argue for a broader conceptualization of institutional betrayal, researchers also argued for a specific form of institutional betrayal that occurs between military service fathers and sons (McCormack et al., 2022). Specifically, they argue that veteran fathers who resist sharing personal combat narratives with their military-service sons breeds distance and resentment that is compounded by the military’s betrayal of not preparing them for the “cultural threats of war.”
Researchers’ Recommendations for Future Directions
Longitudinal Studies
The majority of studies identified specific recommendations for future studies on institutional betrayal. Nearly half of the articles (43%) encouraged future research to prioritize longitudinal research. For example, researchers described the need to determine causal relationships between historical variables such as childhood trauma and institutional betrayal and proposed outcome variables such as trust and avoidance of the betraying institution (Selwyn et al., 2021). Other researchers highlighted the need to examine these effects over time. In the military, Bobek described measuring betrayal prior to deployment, during deployment, and after deployment to examine the relationships between previous and later betrayal (2011). Similarly, Monteith and colleagues (2019a) described the need to identify when survivors of military sexual trauma are at the greatest risk for suicidal ideation and self-harm using longitudinal studies. At a more institutional level, researchers described how changes in reports of institutional betrayal may be tracked as universities make policy changes longitudinally (Smidt et al., 2021).
Building More Inclusive Research
In a quarter of studies (24%, n =9), researchers called for expanding research to include new populations, such as family members of those serving in the military (Bobek, 2011), active-duty military personnel (Monteith et al., 2016), physicians and other healthcare providers (Smith, 2017), male military sexual trauma survivors (Jacobs, 2016), and non-college populations (Pinciotti & Orcutt, 2021; Smith & Freyd, 2017).
Similarly, 14 (37.8%) of the included articles described the need for institutional betrayal research in more diverse populations. The need for research with racial-ethnic, gender, and/or sexual minorities was described by six articles (16%; Micol, 2017; Monteith et al., 2021; Reffi et al., 2021; Smidt et al., 2021; Gómez, 2022; Gutowski & Goodman, 2020). Lett and colleagues (2020) suggested researchers examine the role of specific types of disability.
Two articles highlighted the importance of cross-cultural studies. Lee and colleagues (2021) suggested future work examine for potential racial differences in relation to experiences of institutional betrayal, which may elucidate information related to variation in psychological outcomes. Bobek (2011) proposed cross-cultural studies among subcultures in the military.
Larger Samples
Several articles described the need for larger samples (14%, n = 5). Similarly, three articles pointed to research with greater variation of institutional betrayal in their samples (Reffi et al., 2021; Monteith et al., 2021; Rosenthal et al., 2016). Monteith et al. (2021) noted how individuals with the most severe reports of institutional betrayal may not be participating in research and suggested future work address potential barriers.
Variables
A variety of predictor and outcome variables were suggested across studies (50%, n = 17). Among predictors, researchers pointed to the need for studies of institutional perceptions (Monteith et al., 2016; Gómez, 2022), including identification with an institution (Smith & Freyd, 2013) as well as prior institutional betrayals (Shoemaker & Smith, 2019), substance use (Wright et al., 2017), prior trauma histories (Lind et al., 2020), institutional courage (Bloeser et al., 2021; Lind et al., 2020), supportive reactions and help seeking (Monteith et al., 2019a), social/peer groups (Holland, 2020), and provider-focused variables such as compassion (Monteith et al., 2021). Examples of suggested outcome variables include health related outcomes (Andresen et al., 2019; Monteith et al., 2016), help seeking (Monteith et al., 2021), burnout and job satisfaction (Brewer et al., 2020), and long-term psychological symptoms and willingness to engage with care (Monteith et al., 2019b).
Interventions
Three articles called for intervention work related to institutional betrayal (Smith, 2017; Monteith, 2019a; Monteith, 2019b). Smith (2017) described institution-level interventions where healthcare providers receive the intervention and learn how to address risk factors contributing to institutional betrayal. Specific examples of what other interventions may be useful were lacking and may present an important avenue for future work.
Discussion
From 2011 to 2022, research examining institutional betrayal developed rapidly, resulting in more than three dozen (N = 37) empirical studies included in the current review. This body of work offers evidence that institutional betrayal is common and linked with multiple forms of harm, including both physical and psychological health problems as well as career consequences, such as absenteeism. The costs of institutional betrayal may be worse for individuals with minoritized identities, as suggested by studies examining sexual minority group membership for instance. There is also good evidence that institutional betrayal is linked with negative perceptions of institutions and various forms of disengagement, from lack of compliance with healthcare advice to abandoning one’s career in the military.
The rapid advancement of research into institutional betrayal appears to be aided by the availability of the Institutional Betrayal Questionnaire/IBQ. The majority of studies used versions of the IBQ, which means the emerging literature benefits from shared measurement across studies. The IBQ items offer the field opportunities to better understand the frequency of specific institutional acts of omission or commission as well as their correlates, which will be essential for applying the growing literature to practice and policy recommendations. Early iterations of the IBQ were developed to assess institutional betrayal in healthcare and campus settings, and investigators have modified the IBQ over time to also consider supportive actions or institutional courage (e.g., Freyd, & Smidt, 2019). Researchers have begun to examine the psychometric properties of the IBQ (Smith & Freyd, 2013; Smith & Freyd 2017) and the IBQ 2.0 (Reffi et al., 2021). Differences in the researcher’s findings regarding the relationship between institutional betrayal and distress (e.g., PTSD, anxiety, depression; Reffi et al., 2021) when examining the IBQ have been noted. While widespread use of the IBQ allows researchers to compare findings across different studies, further measurement of analysis of the IBQ in relation to distress after trauma would further validate the use of this research tool for future studies. Furthermore, the examination of the IBQ’s psychometric properties in other pertinent populations, outside the university setting, may help elucidate information regarding the validity within other populations.
Several aspects of the literature seem less well developed, including research on correlates of institutional betrayal beyond mental health, such as cognitive, relational, academic, and economic impacts that have been studied in greater detail over time in the betrayal trauma literature and which are likely also relevant after institutional betrayal. Further, several limitations are common across the literature that future research should address. For example, relatively little is known about institutional betrayal among youth, despite how common sexual abuse can be among youth-serving institutions, such as in churches, schools, child-protective services, or extra-curriculars (e.g., sports, boy scouts). It is striking that concepts of institutional betrayal built on the foundation of betrayal trauma theory, which focused initially on child abuse; and yet, little research is available on institutional betrayal in the context of child abuse. Of course, research with youth presents many challenges, from building partnerships with schools or faith-based organizations to carry out research or seeking/receiving parental consent. However, many examples from betrayal trauma theory and the larger literature on child maltreatment could guide the way to developing research that examines the impact of institutional betrayal among youth.
Military, health, and university settings are well-represented in the literature to date, though other institutions are not yet as well represented. For example, research on institutional betrayal and its consequences in K-12 schools, police or other government agencies, and diverse workplaces is relatively lacking. Further, while the development and refinement of the IBQ has allowed the field to move forward rapidly, studies to date largely rely on this or other self-report methods. Future work should consider additional methods, which may help address questions about detection of and responses to institutional betrayal, such as laboratory behavioral tasks or record reviews. In addition to examining institutional betrayal in these populations and settings, research is lacking when it comes to examining the role of institutional courage (Freyd, 2017). Addressing these gaps will help guide practice by highlighting the protective roles these institutions are meant to serve.
Finally, two of the most important areas for development in this literature include addressing the reliance on cross-sectional methods and primarily White samples. To date, most of the research on institutional betrayal is cross-sectional, which has been essential for measurement development and establishing initial relationships between institutional betrayals and a host of variables. Next, longitudinal research is urgently needed to examine relevant predictor and outcome variables over time, including to determine the degree to which institutional responses impact outcomes relative to the original trauma over time, which is essential to understanding both harm and healing as well as steps to prevent institutional betrayal and ensure institutions respond effectively. Further, longitudinal as well as cross sectional studies with individuals minoritized and marginalized by their identities is also needed given the reliance on samples that are primarily White. The handful of studies available that focus on lesbian, gay, and bisexual persons point to the importance of examining the intersections of trauma, institutional betrayal, and discrimination across many forms, including systematic racism.
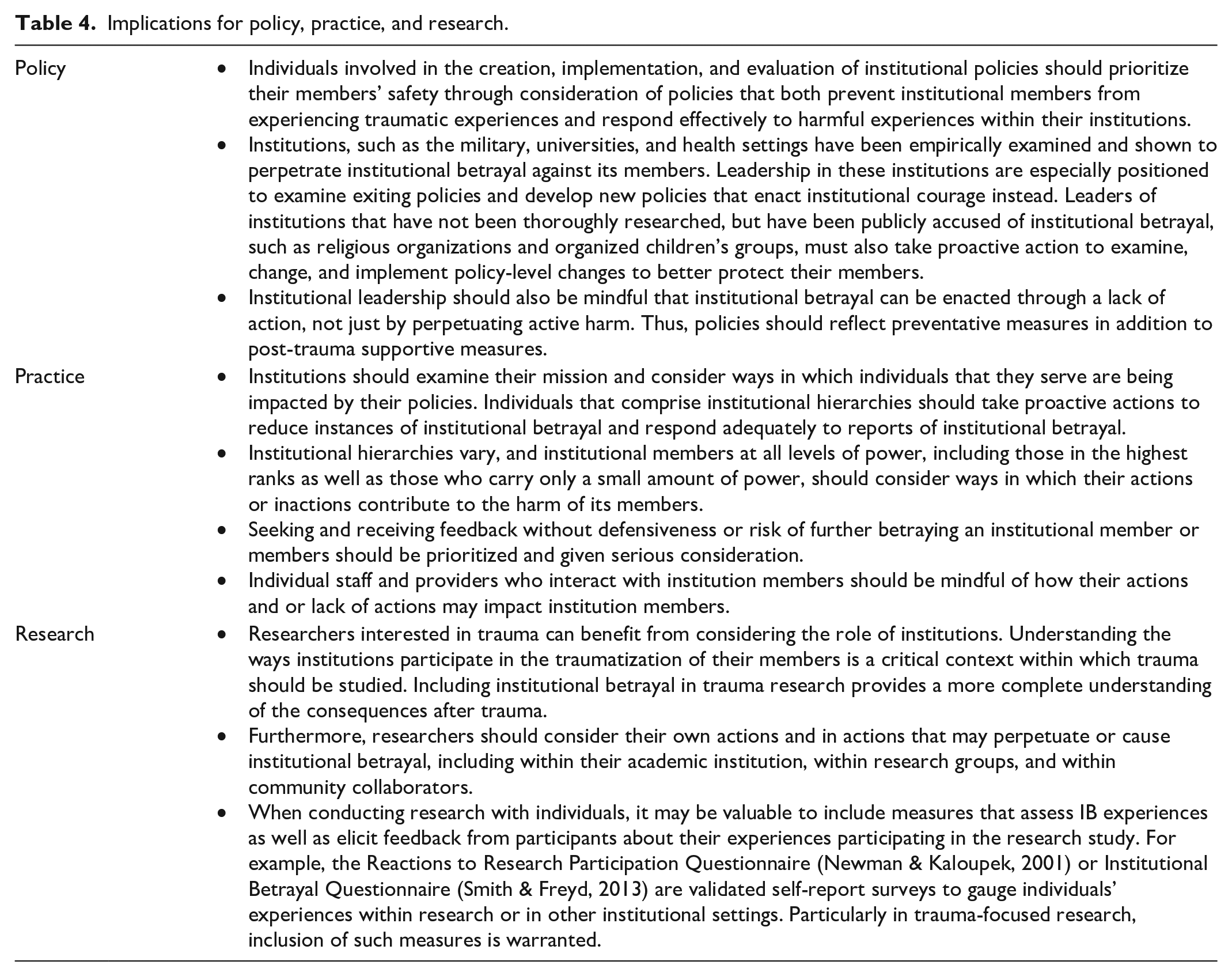
The growing body of work related to institutional betrayal provides an opportune moment for researchers, policymakers, and practitioners to improve systems on which individuals depend (see Table 4). Furthermore, the impact of this work is also applicable to institutional leaders generally. Institutions and those who can enact meaningful changes or develop institutional policies to best support their members can utilize the findings from this field to minimize harm and better support their communities. For example, entities with longstanding power may wish to self-examine current policies and practices in relation to institutional betrayal. Those who are building or establishing institutions intended to support their community may benefit from considering ways in which they can prevent harm and improve responses when reports of harm are issued from the outset. Researchers can aid this work by developing projects that aim to inform policy and practice. Policymakers at all levels—private, public, and governmental— can utilize our understanding of institutions’ role in supporting and protecting their members, especially those most vulnerable, and practitioners may wish to consider their power and how this impacts their interactions with those whom they serve.
Implications for policy, practice, and research.
In sum, institutional betrayal is an important, relatively new area of study. The research base to date points to the importance of studying institutional betrayal across diverse settings to understand harm as well as identify actions that institutions can take to minimize additional harm and support their community members. The strong foundation of study paves the way for future research, including longitudinal research with diverse individuals across diverse institutional settings. The growing evidence of harm related to institutional betrayal and the possibility for action has broad implications for research-informed policy and institutional practice.
Footnotes
Acknowledgements
Thank you to the Traumatic Stress Studies Group for project support, particularly Christine McGrath.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.