
Abstract
The objective of this scoping review was to describe and synthesize the measures, methods, and key findings of published quantitative research examining the influence of child maltreatment (i.e., abuse and/or neglect) and adult trauma exposure on mental health symptoms among women Veterans. A systematic search from database inception to June 2023 generated 18,861 unique articles retrieved and independently screened for eligibility. A total of 21 articles met pre-established inclusion criteria: (a) quantitative data and results within a sample or subsample of U.S. women veterans, (b) published in a peer-reviewed journal, and (c) examining variables of interest simultaneously (i.e., child maltreatment, adult trauma exposure, mental health symptom) in quantitative analyses. Reviewed literature showed a lack of uniformity in measurement and methodologies to evaluate women veterans’ lifetime trauma exposure in relation to mental health. Studies most frequently used self-report survey data to evaluate exposure to child maltreatment and/or adult trauma with convenience samples of women veterans (52.4%, n = 11) and examined depressive and/or posttraumatic stress symptomatology. Findings demonstrate the need for additional research attending to the interplay between child maltreatment and adult trauma exposures in relation to women veterans’ mental health using comprehensive assessment, longitudinal methods, and understudied as well as more representative samples.
Introduction
Women veterans 1 are exposed to high rates of trauma over the course of their lifetimes, including child maltreatment, intimate partner violence (IPV), and military sexual trauma (MST), rates of which are notably higher among women relative to Veteran men (Barth et al., 2016; Maguen et al., 2012; Portnoy et al., 2018). Exposure to repeated, potentially chronic, and interpersonally based trauma is associated with elevations in mental health symptomology; indeed, women veterans in the U.S. demonstrate higher rates of mental health disorders than do veteran men (Harrington et al., 2019) and the most frequent mental health diagnoses for women veterans include depression, posttraumatic stress, and anxiety (Sheahan et al., 2022; Harrington et al., 2019). This scoping review synthesizes quantitative studies that examine relations between child maltreatment and adult trauma exposure with mental health symptomatology, as well as common measures, sampling methods, and statistical approaches used in this body of research. Heeding the call for more research on women veterans and gender-tailored services (Hamilton et al., 2017), this review presents a compelling rationale for attending to trauma prevention across the lifespan and the importance of considering lifetime trauma exposure in mental health treatments for women veterans.
Child Maltreatment
Child maltreatment includes physical, sexual, and emotional abuse and neglect within one’s family before age 18 (Bernstein et al., 2003). Veterans and service members’ exposure to child maltreatment is high, with estimated exposure rates ranging from 16% to 73% (Griffith, 2014; Lapp et al., 2005; Scoglio et al., 2019; Van Voorhees et al., 2012). Moreover, women in the military report child maltreatment rates exceeding those of men in the military (Goncharenko et al., 2021; Koola et al., 2013; Schry et al., 2016; Young et al., 2018). Child maltreatment places women veterans at risk for mental health problems such as depression, posttraumatic stress, and suicidal ideation (Curry et al., 2021; Simons et al., 2019; Young et al., 2018).
Adult Trauma Exposure
Child maltreatment is, for many women veterans, only the beginning of exposure to interpersonal violence. Incurring additional risk for mental health challenges, women veterans also report exposure to interpersonal violence in adulthood that exceeds exposure among veteran men, such as for MST (Katz et al., 2012; Polusny et al., 2014; Relyea et al., 2020). For example, a recent meta-analysis estimated that 38.4% of women military personnel and veterans experienced sexual harassment or assault in the military compared to 3.9% of male military personnel and veterans (Wilson, 2018). Women’s exposure to physical violence during military service is also high, with a recent study reporting that about one in four women veterans are exposed to military physical violence (Holliday et al., 2021). These exposures portend heightened mental health-related risks for women veterans. Specifically, research on women veterans shows that interpersonal trauma exposure is associated with increased risk for mental health disorders, including major depressive disorder (MDD), posttraumatic stress disorder (PTSD), and substance use disorders (Campbell et al., 2008; Creech & Orchowski, 2016; Curry et al., 2021; Goldberg et al., 2019; Kimerling et al., 2010; Lehavot et al., 2018), as well as elevated risk for suicidal ideation and behavior (Brignone et al., 2018; Khan et al., 2019; Monteith et al., 2019). Further, a recent systematic review demonstrated that more frequent and more severe MST is associated with increased risk for women to experience future sexual victimization (Tirone et al., 2020) indicating a clear need for intervention with women veterans exposed to sexual violence to try to reduce further revictimization.
Cumulative Trauma Exposure Over the Lifespan
Child maltreatment may serve as a risk factor for interpersonal victimization later in life and during military service (Schry et al., 2016). Rates of revictimization, defined as experiencing maltreatment as a child and later experiencing physical or sexual assault as an adult (Messman & Long, 1996), are also higher for veteran women than veteran men both during and following military service (Scoglio et al., 2022). A recent study showed that women veterans who experienced child sexual abuse were more than twice as likely to experience unwanted sexual attention while in the military compared to women veterans who did not experience sexual abuse during childhood (Doucette et al., 2022). As such, research more accurately reflects many women service members’ lived experiences when it examines the effects of cumulative interpersonal violence and trauma over the lifespan rather than considering adult interpersonal victimization and child maltreatment in isolation.
Exposure to maltreatment in childhood sets the stage for women veterans to experience later revictimization, and both the unique exposure to child maltreatment and cumulative interpersonal traumas across developmental stages have been shown to increase the likelihood of psychopathology among women veterans (Creech & Orchowski, 2016). A study by Scoglio et al. (2019) showed childhood sexual and physical abuse, and adult sexual and physical assault had both unique and cumulative effects on severity of posttraumatic stress symptoms in women veterans such that each of these victimization experiences independently predicted an increase in posttraumatic stress, and experiencing multiple victimizations increased the risk of posttraumatic stress more than experiencing one or two types.
Findings that women veterans are exposed to high rates of child maltreatment coupled with elevated rates of exposure to interpersonal violence suggest such exposure, at least in part, contributes to elevated risk for mental health symptoms (e.g., PTSD, depression, and suicidal ideation) (Baca et al., 2021; Scoglio et al., 2019). Indeed, some research shows that child maltreatment combined with adult trauma may contribute to worsened mental health in both mixed-sex and women Veteran and service member samples (Baca et al., 2021; Creech & Orchowski, 2016). Yet, other research results indicate that child maltreatment does not directly influence Veterans’ mental health when accounting for trauma exposure in adulthood (Arditte Hall et al., 2018; Hassija et al., 2012). Some scholars have purported that child maltreatment may even protect against adult psychopathology for service members exposed to trauma in adulthood, such as during combat (Owens et al., 2009; Stein et al., 2005). Some of this variability may be explained by studies’ different analytic methods, measures, differences in samples (clinical vs. non-clinical), or because of the challenging nature of disaggregating the individual and interactive effects of multiple trauma exposures over time (Searle et al., 2017). The state of the empirical literature has yet to be investigated systematically or specifically for the unique influences of child maltreatment and adult trauma exposure on mental health symptoms among women veterans.
A synthesis of findings across available quantitative studies will elucidate the role of child maltreatment and distinct trauma exposures in adulthood, including revictimization, on women veterans’ mental health symptoms. The current scoping review examined commonly used measures, methods, and statistical approaches to studying child maltreatment and adult forms of trauma exposure in tandem as they relate to women veterans’ mental health to inform future research directions and clinical practice recommendations.
Method
The Preferred Reporting Items for Systematic Reviews and Meta-analyses Extension for Scoping Reviews (PRISMA-ScR) were used to guide the reporting in this study, and the checklists can be found in Supplemental Appendix 1 (Tricco et al., 2018). The protocol was registered on Open Science Framework (https://osf.io/kvthr/).
Data Sources and Search Strategy
An exhaustive search of the literature was conducted by a medical librarian (fourth author) in APA PsycArticles, APA PsycExtra, APA PsycInfo, Cochrane Library, Google Scholar, Ovid Embase, Ovid MEDLINE, PTSDPub, Scopus, and Web of Science Core Collection databases to identify relevant articles published from the inception of each database to June 2023. The final searches were performed in all the databases in June 2023. The search was peer-reviewed by a second medical librarian using PRESS (Peer Review of Electronic Search Strategies; McGowan et al., 2016). Databases were searched using a combination of controlled vocabulary and free text terms for child maltreatment and military service. The search was not limited by publication type, language, or year. Details of the full search strategies are listed in Supplemental Appendix 2. CitationChaser (Haddaway, Grainger, & Gray, 2021) was used to search the reference lists of included studies to find additional relevant studies not retrieved by the database search.
Study Selection
References from all databases were imported into an Endnote 20 library (https://support.clarivate.com/Endnote/s/article/Citing-the-EndNote-program-as-a-reference?language=en_US). The Yale Reference Deduplicator was used to remove duplicate citations, and the results were uploaded into Covidence (Yale University Harvey Cushing/John Hay Whitney Medical Library, 2021). The title and abstracts of all retrieved citations were reviewed by two authors independently. All relevant articles were then reviewed in full text by two independent reviewers. Eligibility disagreements were reconciled through discussion with the senior author. Inclusion criteria were: (a) use of a sample or subsample of U.S. women veterans or military personnel (with findings disaggregated), (b) inclusion of measures or indices of maltreatment, adult trauma exposure, and adult mental health symptom, diagnosis, or condition, (c) use of a quantitative analytic approach that included both child and adult forms of trauma exposure in relation to mental health, (d) published in a peer-reviewed journal. Studies that did not meet these criteria were excluded from the review.
Data Extraction
Two researchers independently extracted all included studies’ data using a pre-established data extraction form in Microsoft Excel. The researchers’ data extractions were compared to ensure consistency. The data extraction form included the following domains: (a) description of and size of sample, (b) demographics, (c) identification of measures used along with rates of exposure and diagnoses (when available), (d) data collection methods and analytic approach, and (e) quantitative findings.
Results
Data Synthesis
Database searches resulted in 18,861 citations (Figure 1). After removing duplicates, 9,309 citations underwent title and abstract screening. Of these, 176 citations met criteria for full-text review. Subsequently, 19 studies met the inclusion criteria for the study. Two additional studies were found through reference chasing for a total of 21 included manuscripts. Studies were excluded for ineligible sample, analytic approach, no child measure(s), no adult trauma measure(s), no mental health symptom(s), no original data, and conference abstracts (Supplemental Appendix 3). Summaries of the articles reviewed are provided in Table 1.

Preferred reporting items for systematic reviews and meta-analyses extension summary of scoping review process.
Summary of Data Extraction Results (N = 21).

Note. The frequencies provided in this table are for the full sample unless otherwise specified. ASA = Adult sexual assault; CPA = child physical abuse; CSA = child sexual abuse; CTQ = Childhood Trauma Questionnaire; IPV = intimate partner violence; MDD = major depressive disorder; MSA = Military Sexual Assault; MST = military sexual trauma; PTSD = posttraumatic stress disorder; SAEQ = Sexual Abuse Exposure Questionnaire; SES = Sexual Experiences Survey; SUD = Substance use disorder; TLEQ = Traumatic Life Events Questionnaire.
Designates studies with mixed gender samples.
Samples
Over half of studies reviewed used convenience samples of veterans accessing or enrolled in VA care at specific institutions (52.4%, n = 11), with some studies using national convenience (n = 6), national representative (n = 1), VA care representative (n = 1), or a random sampling of veteran women connected to VA care (n = 2). Women veterans were often recruited either from within VA-based clinics as a part of routine care (e.g., during intake) or via lists of women veterans who had accessed care at specific VA facilities. Participants in these samples were, on average, 40 to 50 years old and predominately White, non-Hispanic. Some studies also investigated specific demographics of women Veteran such as women identifying as lesbian, gay, and/or bisexual (e.g., Lehavot & Simpson, 2014) or from the Vietnam era (e.g., Fontana et al., 1997; Lang et al., 2008). Five studies (23.8%) included both women and men veterans with disaggregated findings by gender/sex, so findings only pertaining to women veterans were extracted for synthesis in this review. Five studies used two of the same samples (Booth et al., 2011; Browne et al., 2018; Lehavot et al., 2014; Lehavot & Simpson, 2014; Pulverman et al., 2019). Sample sizes of women veterans ranged from 101 to 1,004, with a median of 298.
Tools, Measures, and Methods Used
We found variation with respect to the measures used to evaluate child maltreatment and adult trauma across studies. Most studies utilized standardized self-report questionnaires (n = 14). The most commonly used standardized measures of child maltreatment were the Childhood Trauma Questionnaire (CTQ) (Bernstein & Fink, 1998) (n = 6) and the Trauma Life Events Questionnaire (TLEQ) (Kubany et al., 2000) (n = 4). Other measures used were the Trauma History Screen (Carlson et al., 2011) (n = 2), the Trauma Questionnaire (McIntyre et al., 1999) (n = 1), and the Sexual Abuse Exposure Questionnaire (SAEQ) (Ryan et al., 1992) (n = 1). Five studies gathered data via other self-report methods, including clinical screening tools or single dichotomous items, two of which additionally collected a standardized measure or interview. In two articles, both using the same data set, child maltreatment was assessed through interview questioning alone (Booth et al., 2011; Pulverman et al., 2019). Eight studies used the same measure or interview to assess for child maltreatment and adult trauma exposure (e.g., Booth et al., 2011; Hassija et al., 2012). For adult trauma exposure, use of standardized self-report measures varied considerably given there were also different types of trauma under study (e.g., combat exposure, IPV, sexual assault). For adult sexual trauma, the Sexual Experiences Survey (SES) (Koss et al., 1985; Koss et al., 2007) was most commonly used across studies (n = 4) (Browne et al. 2018; Campbell et al., 2008; Lehavot & Simpson, 2014; Lehavot et al., 2014); however, three of these studies were with the same sample. Studies also used self-report questions (not as a part of a standardized measure) (n = 7) (e.g., Browne et al., 2018; Scott et al., 2014), interviews (n = 5) (e.g., Wilson et al., 2020), or medical records data (n = 1) (Surís et al., 2004) to evaluate exposure to adult trauma.
Despite variability in how constructs were measured, studies primarily used self-report surveys (n = 16). Eleven studies derived data from interviews, eight in conjunction with self-report surveys and three with medical chart data. In terms of analytic approaches, aligning with the multivariate nature of this investigation, regression analyses (including path analysis) were most commonly used to examine child maltreatment and adult trauma exposure-mental health associations; structural equation modeling (Fontana et al., 1997) and machine learning analyses (Sampson et al., 2021) were represented as well.
Rates of Child Maltreatment and Adult Trauma
Most studies reported rates of child maltreatment and other forms of trauma exposure. Of those providing rates, child maltreatment rates were found to vary depending on the type of trauma under study. Child maltreatment rates across studies ranged between 7% (Hassija et al., 2012) and 68.5% (Strauss et al., 2011). Among studies with clinical samples (n = 4) (i.e., those with mental health diagnoses or in mental health treatment), rates of child maltreatment were notably high (35.2%–68.5%; Benda, 2005; Curry et al., 2021; Luterek et al., 2011; Strauss et al., 2011); however, similarly high rates were also found in convenience samples of veterans (i.e., Browne et al., 2018, 48%; Scott et al., 2014, 59.7%).
Rates of adult trauma varied across studies, ranging between 3.9% (Fontana et al., 1997) and 74% (Campbell et al., 2008). MST/MSA, the most commonly studied of adult trauma exposure (n = 12) was reported by between 3.9% (Fontana et al., 1997; nationally representative sample) and 67% (Strauss et al., 2011; clinical mental health sample) of women veterans. Rates of revictimization were reported seldomly (n = 4) but were also high, ranging between 13.3% (Booth et al., 2011) and 68% (Mercado et al., 2015). Six studies included in our review reported frequencies of adult physical assault or violence as follows: Campbell et al. (2008) on adult IPV physical violence (74%), Hassija et al. (2012) on noncombat physical assault (21.7%), Arditte Hall et al. (2018) on adult physical assault (21.5%), Lehavot et al. (2014) on military physical victimization (52%–60%), and Luterek et al. (2011) on a number of adult forms of physical violence (e.g., spousal physical abuse before, during, or after the military [23.7%–31.7%]).
Among studies with samples comprised of predominately Black or African American women (n = 3; Campbell et al., 2008; Curry et al., 2021; Strauss et al., 2011), high rates of child maltreatment were also found (31%–68.5%), yet these studies were with clinical samples. Two of these studies also reported especially high rates of interpersonal violence exposure in adulthood: 39% adult sexual assault and 74% physical violence IPV (Campbell et al., 2008) and 67% MST (Strauss et al., 2011). Two studies using the same dataset with a sexual minoritized women sample did not report rates of child maltreatment but reported experiences of adult sexual and physical violence at high rates, particularly prior to and during military service (Lehavot & Simpson, 2014; Lehavot et al., 2014).
Use of standardized self-report measures (n = 14) to evaluate child maltreatment coincided with the highest rates among clinical and non-clinical samples. Specifically, studies using the TLEQ (n = 3) and SAEQ (n = 1), which includes also exposure to family violence, reported the highest rates of child maltreatment (59.7%–68.5%; Curry et al., 2021, Luterek et al., 2011; Scott et al., 2014; Strauss et al., 2011); studies using other self-report measures, such as single items (e.g., Finkelhor et al., 1990) indicated the greatest spread of rates (i.e., 7%–59%). Studies using interview strategies (n = 4) all found child maltreatment among roughly one third of their samples (27%–35.2%; Benda, 2005; Booth et al., 2011; Pulverman et al., 2019; Surís et al., 2004).
For adult trauma exposure rates, use of differing instruments and varied constructs across studies did not allow for comparisons by type of measurement.
Mental Health Symptoms
The most common mental health symptoms studied in relation to child and adult forms of trauma exposure across studies were PTSD or PTSD symptom severity (n = 16), depression/mood disorders and symptoms (including suicidal thoughts and attempts) (n = 12), and/or substance use (n = 4). Studies consistently reported that exposure to various forms of trauma was positively associated to mental health symptomatology. Yet, there was variation in terms of specific trauma types’ influence on mental health. Some studies showed that child maltreatment when examined concurrently with adult trauma, had no significant associations with outcomes of interest, such as disordered eating, depression, PTSD, and substance use disorders (Arditte Hall et al., 2018; Browne et al., 2018; Sampson et al., 2021). However, other studies found that child maltreatment was positively associated with depression, PTSD symptoms (Asmundson et al., 2004), attempted and completed suicide (Benda, 2005), and disorders of extreme stress (Luterek et al., 2011) when examined in tandem with adult trauma. In some cases, specific types of child maltreatment were risk factors for mental health difficulties. One study found that child nonsexual trauma was positively associated with PTSD, whereas CSA was removed from the model due to non-significance (Lang et al., 2008).
With regard to trauma in adulthood, all but one study examining MST and assault found it to positively associate with mental health symptoms, including PTSD symptoms/PTSD (Asmundson et al., 2004; Scott et al., 2014; Fontana et al., 1997; Lehavot et al., 2018), substance use (Browne et al., 2018), depression (Mercado et al., 2015), other-directed violent and suicidal behavior (Wilson et al., 2020), risky sexual behavior (Strauss et al., 2011), sexual pain (Pulverman et al., 2019), and other disorders of extreme stress (Luterek et al., 2011). Military sexual assault was also found to associate with alcohol misuse indirectly through depressive and posttraumatic stress symptoms (Lehavot & Simpson, 2014). Booth et al. (2011) found that when childhood, prior to military, in-military, and postmilitary rape were all considered in a logistic regression model concomitantly, postmilitary rape was the only variable positively associated with a lifetime substance use disorder.
Lifetime trauma exposure, which included either child or adult exposure, was positively associated with the likelihood of mental health disorders, including a lifetime substance use disorder (Booth et al., 2011) and PTSD (Surís et al., 2004). Further, among the five studies with mixed-sex samples, unique patterns of findings emerged for men and women. For example, one study found that CSA was positively associated with suicide attempts for men but not for women, whereas military sexual assault was positively associated with other-directed violence and risk of suicide attempts for women only (Wilson et al., 2020). More detailed study-specific findings can be found in Supplemental Table 3.
Discussion
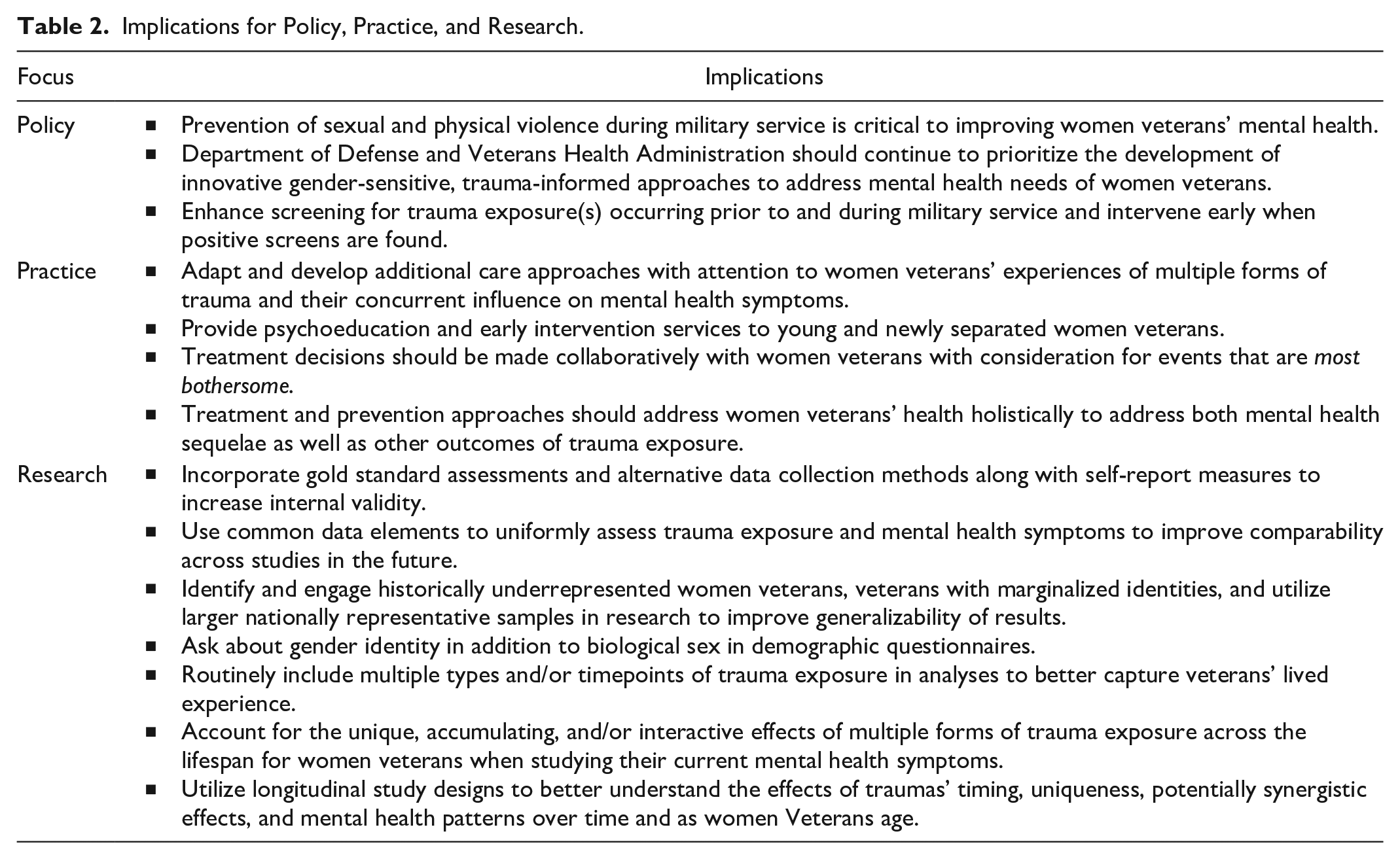
This scoping review of 21 articles synthesized available peer-reviewed quantitative research on the unique influences of child maltreatment and adult trauma exposure on mental health symptoms among women veterans. As the population of women veterans grows, the extant literature may inform the development and adaptation of existing healthcare practices for the specific needs of this population. Toward this aim, the current review’s findings affirmed the need for additional research exploring the impact of specific, cumulative forms of trauma exposure within and across samples of women veterans with consideration for traumas’ timing, uniqueness, and potential for synergistic effects on mental health symptomatology. Implications of this review for policy, practice, and research are summarized in Table 2.
Implications for Policy, Practice, and Research.
Across studies, this review found high rates of exposure to various forms of interpersonal violence among women veterans (i.e., child maltreatment, MST, adult physical and sexual assault, IPV). These rates align with those reported in prior studies of community and veteran women samples (Barth et al., 2016; Maguen et al., 2012; Portnoy et al., 2018). Nonetheless, the current review found variation in trauma exposure rates depending on the sample and type of trauma under investigation and how constructs were measured across studies. For example, the earliest study that reported rates of sexual harassment during military service (Fontana et al., 1997) reported that only 3.9% of women endorsed sexual harassment during their time in the service, whereas more recent studies reported much higher endorsement of sexual harassment during service (e.g., 34.8%) (Scott et al., 2014). Across studies, when women who are asked about trauma exposure across the life course in VA-based and research settings report common exposure to interpersonal violence and sexual victimization. Furthermore, the elevated rates of trauma exposures appear to be greater prior to or during military service compared to after discharge from the military. These time periods coincide developmentally with periods when all women in the U.S. are at heightened risk for exposure to sexual violence, particularly during early adulthood (Black et al., 2011; Rinehart et al., 2014).
Mental health clinicians and scholars alike implicate early life trauma as instrumental in shaping subsequent mental health and relationship functioning (Copeland et al., 2018; Jones et al., 2018). Yet, many studies did not meet inclusion criteria for this review due to not including a measure of child maltreatment, not differentiating child maltreatment from non-traumatic childhood stressors (e.g., parental divorce), or not accounting for child maltreatment in analyses beyond simply reporting rates. Despite the trauma literature’s emphasis on early life trauma exposure(s) as a predisposing risk factor for subsequent victimization (i.e., revictimization; Messman & Long, 1996; Schry et al., 2016; Scoglio et al., 2022) and the disproportionately high rates of such exposure among women veterans (Holliday et al., 2021), many studies did not measure child maltreatment. It is unclear why the extant literature does not routinely include multiple timepoints of trauma exposure in their models. However, given the evidence that many women veterans experience multiple traumas across the life course, child maltreatment and/or other forms of child trauma are important to include to best capture veterans’ lived experiences. Such exclusions can lead to incomplete or inaccurate conclusions and conceptualizations among women veterans who may be prone to revictimization. For instance, findings not accounting for child maltreatment may attribute negative adult mental health consequences to adult traumas that are better explained by retraumatization. Given evidence that those who experience abuse and neglect during childhood are at heightened risk for latter trauma exposure (Scoglio et al., 2019), it is noteworthy that among reviewed studies, authors rarely provided rates of revictimization (i.e., frequency of those who experienced multiple forms of trauma exposure) or accounted for revictimization in analyses. There is a broad empirical evidence base demonstrating biological and epigenetic alterations from childhood trauma which can affect mental health outcomes in adulthood (Nöthling et al., 2020; Van der Kolk, 2003) which should be accounted for empirically in emergent research.
The literature examining the role of child maltreatment on mental health and its potential for interactive effects with adult trauma exposure has been mixed (Searle et al., 2017), and results gathered herein align with those reported in prior literature. Although some included studies showed significant associations between child maltreatment and negative adult mental health outcomes when considered alongside other forms of adult trauma exposure, this trend was not consistent across studies. Further, military sexual trauma/assault (MST/MSA) demonstrated the most consistent positive associations with negative mental health outcomes, a finding that was particularly salient when MST/MSA represented a revictimization experience and was studied in relation to posttraumatic stress symptoms. In the one study where MST was not positively associated with a mental health outcome, that is, lifetime SUD (Booth et al., 2011), revictimization was not taken into account in the analyses. Taken together, the current scoping review’s mixed results underscore the importance of attending to trauma exposure across the lifespan to optimally address mental health needs of women veterans. Considering the potential for unique and cumulative effects of various types of trauma exposures on mental health, they should be considered in relation to prevention and treatment efforts by VHA and Department of Defense.
This scoping review provided additional evidence that discrepant findings about the child maltreatment-adult mental health linkage may be due to methodological differences across studies. Furthermore, there are inherent methodological challenges when evaluating the unique contributions of multiple traumas on mental health symptoms, especially when using self-report questionnaires and retrospective reporting. Use of interviewing provided the most consistency in rates of child maltreatment (i.e., about one third of their samples). Given that for trauma-related symptoms are anchored to a single, specific traumatic event, it is notable that among studies including PTSD or PTSD symptoms as outcomes, symptoms were rarely linked to specific traumatic event(s) endorsed. The pervasive and diffuse impact(s) of multiple trauma exposures may be challenging to assess, even with clinical/structured interviews or gold-standard assessment measures. Affective and psychosocial changes following trauma can be delayed, long-standing, and difficult to attribute to particular time periods and or to match with specific experiences. It is imperative that researchers and clinicians evaluate and consider the roles of accumulating trauma exposures when examining women veterans’ mental health so that the literature can more accurately reflect the common revictimization experiences of this population, especially in investigations designed to examine etiology through a gender-sensitive, ecological lens.
Clinical Implications
Trends observed in the current literature echo prior findings showing that trauma-mental health linkages vary depending on the type of trauma, outcome, and/or socio-contextual factors under investigation for military personnel and veterans (Combellick et al., 2019; Presseau et al., 2019; Shea et al., 2017). Some research has started to disentangle gender-specific phenomenology that may underlie interpersonal violence exposure and subsequent mental health outcomes (Portnoy et al., 2018), but more is needed. For example, post-9/11 women veterans may experience greater exposure to interpersonal violence than their male counterparts, yet exhibit comparable resilience following trauma exposure only when type of trauma is accounted for (Portnoy et al., 2018). For the VA healthcare system to provide care for women veterans following interpersonal trauma exposure, a nuanced approach to examining unique and accumulating impacts of different trauma exposures across the life span is of great importance.
The current scoping review lends credence to the notion that “all traumas are not created equal” as has been established in prior work (Gebauer et al., 2019). Criterion A trauma as a catch all does not offer the most utility when point-of-care decisions are made, particularly in the presence of chronic exposure. Rather, individualizing treatment (Steenkamp, 2016) and/or adapting treatments to account for specific types of exposures (e.g., child trauma, IPV, MST) and their accumulating effects (Landes et al., 2013) represent practical approaches to addressing the variability of trauma sequalae for specialized populations of veterans. For example, interventions such as Recovering from IPV through Strengths and Empowerment (Iverson et al., 2022) which addresses IPV-related difficulties and Skills Training in Affective and Interpersonal Regulation via telehealth (Azevedo et al., 2016) are promising approaches that are well-aligned with this review’s findings. Nonetheless, treatment decisions should be made collaboratively with women veterans while considering events they find most bothersome and most impact their functioning (i.e., event centrality) (Reiland & Clark, 2017) while providing specific attention to the role of revictimization in assessment and treatment. For example, offering education and creating space to explore how repeated traumas have shaped belief systems and coping strategies may help women veterans better understand their presenting concerns in a non-pathologizing manner. Treatment and prevention approaches with an emphasis on holistic health may also be helpful as our findings demonstrated that trauma exposure occurring over the life span is positively associated with a variety of mental health symptoms and health behaviors (e.g., substance use, suicidal thoughts, PTSD symptoms).
Regarding high rates of violence exposure that occur prior to and during military service, prevention, and early intervention may be more strategically targeted toward these time periods to minimize incidence and the long-term impact of these experiences on women’s health. Although there is burgeoning effort to enhance healthcare for women veterans (Foynes et al., 2018) and to reduce violence among military personnel and veterans (Turchik & Wilson, 2010), more work is needed to screen, assess, and ultimately connect women with the resources and services that best align with their experiences and associated needs. In addition to the aforementioned interventions, programming that offers opportunities for healing with attention to gender-specific barriers to care are critical to serving women veterans (Brooks et al., 2016).
Limitations
This scoping review included literature largely from convenience samples of U.S. VA-affiliated women veterans, and as such cannot intuit how frequently child maltreatment and other types of adult trauma exposure occur among women veterans or how these exposures relate to the mental health of women veterans in the U.S. general population or other regions. Several population-based or U. S. national samples of veterans did not provide results disaggregated by sex or gender and were therefore excluded from the review. Relatedly, the current review was additionally restricted in its interpretation due to the lack of demographic data available in the broader literature, much of which did not differentiate between birth sex and preferred gender. Although these are limitations of our work, they lend further support for the efforts in place to better engage women veterans in research and to access and target women who may not already be accessing VA healthcare or who are historically understudied, such as racial, ethnic, gender, sexual or other minoritized groups of women (Chrystal et al., 2022; Gerber et al., 2014); Lehavot & Simpson, 2014; Yano et al., 2006, 2010).
This review focused specifically on mental health symptomatology, thereby excluding research that examined child maltreatment and adult trauma exposure in relation to other potential outcomes (e.g., physical health, epigenetics, healthcare utilization). The review also included only peer-reviewed literature, which may result in inherent biases due to a lack of integration of gray literature (e.g., failure to report non-significant results). To allow for synthesis across studies, the review was restricted to quantitative studies wherein all constructs were considered concomitantly, thus not including other types of data (i.e., qualitative, case studies) relevant to this area of study. Lastly, our results showed heavy reliance on self-report questionnaires. Future research should consider incorporating gold standard assessments such as for the evaluation of PTSD and PTSD symptoms, which may yield results that differ from those obtained through self-report (Kramer et al., 2022). There is ample room to build on findings gathered in this review and to incorporate additional health and protective factors that may promote improved understanding of the linkages between child maltreatment, adult trauma exposure, and mental health among women veterans so that adaptations to conceptualization and treatment can follow.
Future Research Directions
The current scoping review’s findings demonstrate the need for additional research on the intersectionality of women veterans’ lived experiences as women, as veterans, and as having overcome trauma(s), with attention to other minoritized identities that may be present and predispose them to risk of violence or other forms of marginalization. More research is needed on women veterans who have not been historically represented in the literature, women veterans who are not already connected to VA care, and representative samples of U.S. women veterans to enhance generalizability of results to this rapidly growing population. Researchers should also consider use and consistency of measurement within and across studies to better understand how specific forms of traumatic exposure (e.g., military vs. non-military, physical vs. sexual) differentially associate with outcomes of interest and weigh the benefits and drawbacks of using the same measures to evaluate early life and subsequent forms of trauma exposure. Furthermore, researchers should attend more precisely to contextual (e.g., socioeconomic) and proximal (e.g., chronicity) factors that may coincide with trauma exposure; such factors may provide information about their respective sequalae, especially when there are multiple exposures (see Holder et al., 2022; Xue et al., 2015 for review). As the measures used to assess trauma exposure varied so widely, and this variability likely contributed to discrepancies in findings across studies, use of common data elements may be beneficial to ensure some uniformity moving forward. Additionally, researchers working with samples of women veterans are encouraged to disaggregate child trauma from adult trauma exposure and specific forms of adult traumas (physical, sexual, military vs. non-military) in future studies so as to continue to elucidate the differing effects of trauma exposure in different developmental stages and contexts. Lastly, the current review highlights a dearth of longitudinal and mechanistic studies, including those which emphasize enhanced understanding of risk and protective factors as well as trajectories of mental health symptoms among women veterans (e.g., Stefanovics et al., 2023). Such investigations are essential to the evolving response to women veterans’ unique needs and experiences from a strengths-based perspective as this population continues to grow.
Supplemental Material
sj-docx-1-tva-10.1177_15248380241234345 – Supplemental material for Child Maltreatment, Adult Trauma, and Mental Health Symptoms Among Women Veterans: A Scoping Review of Published Quantitative Research
Supplemental material, sj-docx-1-tva-10.1177_15248380241234345 for Child Maltreatment, Adult Trauma, and Mental Health Symptoms Among Women Veterans: A Scoping Review of Published Quantitative Research by Candice Presseau, Jessica R. Carney, Nora K. Kline, Alyssa A. Grimshaw, Lauren DeMoss, Craig Gunderson and Galina A. Portnoy in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
We would like to acknowledge that this work was supported by time and resources made available to the IPV Center for Innovation and Research, an IPV Assistance Program Innovation Hub, which receives funding from The National Social Work Program Office of the Veterans Health Administration.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government. The authors had full access to the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. No financial disclosures were reported by the authors of this paper.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.