
Abstract
Use of social media in health promotion and public health continues to grow in popularity, though most of what is reported in literature represents one-way messaging devoid of attributes associated with engagement, a core attribute, if not the central purpose, of social media. This article defines engagement, describes its value in maximizing the potential of social media in health promotion, proposes an evaluation hierarchy for social media engagement, and uses Twitter as a case study to illustrate how the hierarchy might function in practice. Partnership and participation are proposed as culminating outcomes for social media use in health promotion. As use of social media in health promotion moves toward this end, evaluation metrics that verify progress and inform subsequent strategies will become increasingly important.
The use of social media to communicate with customers and audiences continues to increase substantially in both the private and public sectors, including public health and health promotion (Barnes, Lescault, & Andonian, 2012; Hanson et al., 2011; Stelzner, 2012; Thackeray, Neiger, Smith, & Van Wagenen, 2012). Despite their growing popularity, there is little evidence to suggest that social media are being used in a way that maximizes their capacity to create conversations and engage audiences, or that appropriate evaluation metrics have been identified and are being used to measure associated outcomes.
To use social media effectively, strategies to engage audiences and measure related outcomes must be developed. The purposes of this article are to (a) define engagement and describe its value in helping maximize the potential of social media in health promotion settings, (b) present an evaluation hierarchy for social media engagement, and (c) use Twitter metrics as a case study to illustrate how the evaluation hierarchy might function in practice.
The vast majority of social media use reported to date in the public and nonprofit sectors involves one-way messaging to audiences much like traditional media (Bortree & Seltzer, 2009; Thackeray et al., 2012; Waters, Burnett, Lamm, & Lucas, 2009). Although one-way messaging may benefit health promotion efforts to a degree, a sole focus on this type of messaging neglects a core attribute of social media, if not their central purpose, which is to help create engaged communities through dialogic or two-way messaging (Lovejoy, Waters, & Saxton, 2012).
By their very nature, social media are designed to create conversations among audiences. From a health promotion perspective, these conversations can lead to varying levels of engagement, which in turn, can result in a range of outcomes, including increased awareness or knowledge of health-related information, feelings of belonging and social connection, and involvement with health promotion programs either as partners who help guide actual program development and implementation or as participants who receive direct services or products. In this regard, engagement can be viewed in multiple stages with corresponding effects or outcomes.
Engagement in the context of social media and health promotion has been defined as connections between people that contribute to a common good (Neiger et al., 2012). This suggests that both the health promotion organization and its audience members receive a benefit. For example, if audience members engage with the organization via social media in successful advocacy to reduce public exposure to secondhand smoke from cigarettes, both have contributed to an improved condition that is conducive to health. The organization fulfills its responsibility and the audience members benefit by improved air quality.
It is proposed here that the use of social media in health promotion must lead to engagement between the health promotion organization and its audience members, that engagement must provide mutual benefit, and that an engagement hierarchy culminates in program involvement with audience members in the form of partnership or participation (as recipients of program services). Furthermore, high engagement will not occur if social media use is restricted to one-way messaging.
Before attempting to create a social media presence that transcends one-way messaging and actually engages audiences, health promotion practitioners should consider four key strategic issues: (a) decide what the organization is trying to accomplish with social media (e.g., goals and objectives), (b) identify specific audiences of interest to the organization and its programs and tailor strategies to invite them into the social media conversation, (c) identify benefits the organization can offer audience members within the context of predetermined goals and objectives, and (d) identify what the organization wants audiences to do (e.g., create or promote content, respond to messages, share experiences, participate with the organization off-line). Addressing these strategic issues will clarify the purposes for using social media and help develop appropriate outcome measures and corresponding evaluation metrics including those associated with engagement.
To measure engagement with social media, appropriate evaluation standards and metrics must be applied. In what appears to be the first organization of its kind, the #SMMStandards coalition was developed in 2011 to promote standards for measuring social media (#SMMStandards, 2012). The coalition, consisting of the Institute for Public Relations, the Council of Public Relations Firms, and the International Association for Measurement and Evaluation of Communication, met at a summit in Dublin, Ireland, in June 2012, where six initial priorities were developed for standardization: (a) content sourcing and methods, (b) reach and impressions, (c) engagement, (d) influence and relevance, (e) opinion and advocacy, and (f) impact and value.
It was proposed at the Dublin summit that engagement in particular should be measured at three levels: (a) low (e.g., Facebook likes and Twitter followers), (b) medium (e.g., blog video comments and Twitter retweets), and (c) high (e.g., Facebook shares and original content/video posts; Marklein & Paine, 2012). In an article predating the Dublin summit, Neiger et al. (2012) presented a comparable hierarchy of key performance indicators for social media related to low, medium, and high engagement with associated metrics.
Based on similarities for engagement measures presented by Neiger et al. (2012) and the coalition at the Dublin summit (Marklein & Paine, 2012), an evaluation hierarchy is displayed in Figure 1. One difference between the engagement measures proposed by Neiger et al. (2012) and the Dublin coalition pertains to high engagement. As per Neiger et al.’s hierarchy represented in Figure 1, high engagement or involvement of audience members with programs as either partners or participants is viewed as the culminating outcome of engagement.
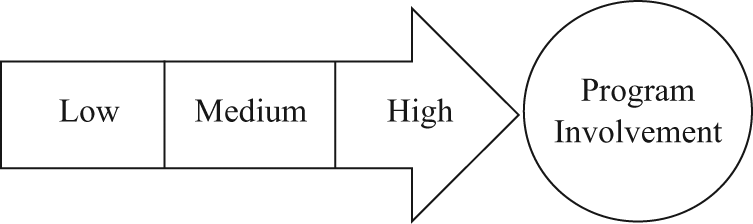
Evaluation Hierarchy for Social Media Engagement
Although outcomes associated with low and medium engagement are important within the three stages and have value independent of the hierarchy, they are viewed primarily as intermediary steps that lead to high engagement. The underlying assumptions of the hierarchy are that one stage of engagement leads to the next, that unique metrics are stage specific, and that the highest stage of engagement links audiences with programs.
The evaluation hierarchy presented in Figure 1 is similar in theory to an evaluation hierarchy familiar to health promotion specialists who use process, impact and outcome evaluations. Process evaluation, which measures variables associated with implementation, leads to impact evaluation, which generally measures changes in behavior, which leads to outcome evaluation, which typically measures changes in disease states associated with mortality and morbidity data (McKenzie, Neiger, & Thackeray, 2013). In a similar manner, low engagement measures early stages of implementation (i.e., establishing a social media presence), medium engagement measures the presence of dialogic conversations (i.e., similar to an impact measure assessing some type of change or progression), and high engagement parallels outcome evaluation with a culminating indicator, in this case, audience involvement with programs. Whereas the process, impact, and outcome hierarchy flow to data and information that represent more in-depth and sophisticated levels of analysis, the evaluation hierarchy in Figure 1 flows to increasingly more complex yet meaningful stages of engagement.
Table 1 displays Twitter metrics associated with low, medium, and high engagement. Twitter is a microblogging or messaging service that allows subscribers to send and receive short messages of no more than 140 characters. Although Twitter metrics are used here as a case study or example to illustrate how the evaluation hierarchy might function in practice, the hierarchy could also be used to categorize metrics from other social media applications. Table 1 displays metrics for each level of engagement and defines each metric.
Twitter Metrics Associated With Low, Medium, and High Engagement

These metrics do not relate to Twitter use per se. Rather, they are associated with audience member involvement with programs (e.g., partners or participants) and represent more traditional process evaluation measures often collected in health promotion practice.
An additional metric will usually be included here by the health promotion organization to measure the degree to which health behaviors have been improved. This could serve as further evidence of high engagement.
Low Engagement
Low engagement marks the beginning of a social media relationship between a health promotion organization or program and its audiences. In this stage, the organization is attempting to create a Twitter presence and recruit and retain followers (i.e., other Twitter users who are following the organization or subscribing to its tweets or messages). This level of engagement is characterized by one-way messaging from the organization to its followers and does not ask for a response or for action but merely provides information. The goal in low engagement is to establish a critical mass of followers who can later engage with the organization. Evaluation metrics tend to be fairly simple and straightforward. This is the stage of engagement where most social media efforts in public health and health promotion languish or terminate.
As displayed in Table 1, Twitter metrics associated with low engagement involve the number of tweets posted by the organization. In addition, the number of the organization’s followers (i.e., other Twitter users who subscribe to the organization’s Twitter account) shows the potential reach and exposure of tweets. Also, the number of second-level followers (i.e., followers of followers), also referred to as second-level networks, demonstrates the potential reach through retweets (i.e., forwarding another user’s tweets) and provides a sense of the relative prominence of the organization’s direct followers.
In addition to simply posting tweets, the organization can direct them toward specific users with the @user-name syntax. These directed messages are a step toward greater personal involvement and yet are limited to the organization pushing out information, as opposed to a dialogic conversation.
Medium Engagement
Medium engagement marks the beginning of dialogic messaging. Whereas low engagement typically measures the actions of the organization to promote itself, medium engagement reflects the audience’s response to the tweets. In this stage, the organization helps develop meaningful conversations compelling enough for followers to retweet or share. The organization is careful to respond to messages posted on their Twitter account in a timely and thoughtful manner in order to increase the likelihood of progression toward high engagement. More specifically, the organization is asking questions of followers and expecting responses and is otherwise nurturing conversations to identify followers who are good candidates for program involvement (i.e., high engagement).
As displayed by the types of metrics in Table 1, in addition to simply having a large number of mutual followers, medium engagement is demonstrated by users mentioning the organization and posting messages directed to the organization (in both cases using the @user-name syntax). By mentioning the organization, users both raise its visibility and establish its credibility to their friends. Medium engagement also includes the frequency with which followers respond to questions or inquiries posted by the organization. For example an organization may tweet, “Today is take your bike to work day, let us know how far you pedaled,” and followers respond. Medium engagement is also characterized by followers responding to requests from the organization to stay connected (e.g., follow us, stay tuned, join us).
Twitter messages can be directed to a user in two ways: either by starting a public tweet with the “@user-name” syntax or by sending a private “direct message” that is only seen by the two parties involved. Although the privacy of the direct message restricts its use to the organization as an evaluation metric and does not raise the visibility of the organization to the user’s social network, the desire for private communication likely indicates a level of trust related to a more meaningful or personal topic. Private and direct messages may also result in the organization identifying potential champions or key advocates for certain programmatic purposes.
In addition to recognizing the immediate followers of the organization, mentions of the organization (i.e., the name of the organization is mentioned in a tweet) raise its visibility to followers’ followers. Thus, effects of medium engagement can be seen in not just the number of retweets and mentions but also the number of unique users who retweet, as well as the number of their followers. Collectively, these metrics measure the total number of people exposed to the message. Furthermore, the amount of an organization’s followers that also follow each other may indicate a sense of community of which the organization is a part.
Computing values for low and medium engagement metrics will range from simple to more sophisticated. Many of the metrics in Table 1 can be computed automatically by popular Twitter Analytics software, such as Tweet Grader (2012), TweetReach (2012), and the Twitter engagement rate developed by socialbakers.com (Rezab, 2012), or through custom tools that make use of the public Twitter application programming interface.
High Engagement
High engagement relates to either online or off-line audience member involvement with a health promotion program either as a partner or as a participant. A partner is either an individual or other entity that takes action to help the organization achieve its goals. For example, an organization may involve audience members in formative research to provide feedback on certain components of a program prior to implementation. Or the organization could have a conversation with audience members about its brand and what could be done to increase recognition. It might involve audience members helping the organization identify program priorities. Partnership might also involve asking audience members to advocate for the passage of legislation or policies that improve conditions that are conducive to health, such as creating more green or open space. Partnership could also generate viral communication promoting an event sponsored by the organization (e.g., fun run, health fair).
High engagement also involves audience members as program participants, meaning individuals who take advantage of services offered by the organization. This might involve participation in support groups, health screenings, or lifestyle programs (e.g., smoking cessation, weight loss, stress management).
The metrics included in Table 1 for high engagement do not relate to Twitter use per se. Rather, they are associated with audience member involvement with programs and represent more traditional process evaluation measures typically collected in health promotion practice. Although these metrics will require evaluators to link Twitter followers to specific aspects of program involvement (i.e., partnerships or participation), the data are not retrieved directly from Twitter. In this regard, high engagement will require health promotion organizations to track engagement beyond Twitter or other social media platforms.
Conclusion
Ultimately, health promotion organizations and their practitioners must decide what they are trying to accomplish by using social media and then match appropriate strategies and evaluation metrics to their predetermined goals and objectives. As reported earlier, research suggests that early adopters of social media in health promotion and public health have underused their potential by limiting their application primarily to one-way messaging. If an organization simply wants to create a social media presence to communicate information to its audiences, one-way messaging may be appropriate. This stage of development, or low engagement, is actually a prerequisite stage for high engagement. This suggests that even if past efforts to use social media have been shortsighted, they are necessary steps to take full advantage of social media.
Health promotion must build on its initial efforts in social media and move from low engagement to medium and then high engagement. Engaged conversations reflected in medium engagement must develop to the type of involvement represented in high engagement. Although social media should not be viewed as a solution to the complexities of behavior change and improved health outcomes (Neiger et al., 2012), they can help in getting people involved in creating environmental and social conditions conducive to health. They can also help draw people to programs and services wherein they can improve personal health. These two outcomes, partnerships and participation, are viewed as the culmination of social media use in health promotion. As health promotion moves toward this end, evaluation metrics that verify progress and inform subsequent strategies will become increasingly important.