
Abstract
Health care disparities in minority populations can be attributed to a number of factors, including lack of access to coordinated primary care and chronic disease management programming. Interventions using a data-centric, coordinated, multidisciplinary, team-based approach to address patients with complex chronic comorbidities have demonstrated improvements in patient outcomes. The use of hospital admission and billing data coupled with care management teams to care for high-risk patients with chronic conditions may be an effective model for improving quality of care while reducing health care costs. This article describes how Camden city, the poorest city in the nation, has made headway toward developing an integrated approach to improving care while reducing costs for the city’s most vulnerable.
Introduction
Five percent of the U.S. population use health care resources far in excess of the rest of the population and accounts for nearly 50% of health care expenditures (Cohen & Uberoi, 2012). These “high-utilizer” patients, many of whom suffer from chronic medical conditions compounded by an array of social and behavioral health issues, tend to receive most of their care in hospitals—sometimes multiple hospitals in the same city. This pattern of utilization is both a symptom and a cause of costly, uncoordinated care. States faced with increasing health care costs are searching for ways to improve the quality of care while decreasing costs for their most complex patients. Data sharing and transparency are key components to reaching this challenging goal (Einbinder & Bates, 2007; Marchibroda, 2008; Walker et al., 2005).
The Health Information Technology for Economic and Clinical Health Act of 2009 was established to help support the development and implementation of health information exchanges (HIEs), electronic networks that share clinical data across health care providers and practice settings that are not part of the same organizational entity (Adler-Milstein & Jha, 2012; Williams, Mostashari, Mertz, Hogin, & Atwal, 2012). With this support, a growing number of hospitals and clinics are now participating in HIE initiatives (Adler-Milstein, Bates, & Jha, 2013; Furukawa, Patel, Charles, Swain, & Mostashari, 2013). Efficient data sharing through the expansion of HIEs has paved the way for improved care coordination, communication, and case management for high utilizers of health services. Evidence suggests that HIEs allow for improved identification of high utilizers, particularly in the emergency department (ED). In New York, a study using regional HIE data identified 20.3% more frequent ED users and 16.0% more ED visits compared to using site-specific data, highlighting the potential of HIEs to improve targeting of case management services to those patients most in need (Shapiro et al., 2013).
Several studies have investigated the effects of case management interventions on high utilizers of health services, though most have relied on either site-specific data or provider referrals to identify patients in need of more specialized services (Althaus et al., 2011; Kumar & Klein, 2013). In California, the Frequent Users of Health Services Initiative (2008) has been successful in reducing ED visits and hospital inpatient days among high utilizers through the use of care coordination strategies to connect these at-risk patients to support services in the community. In addition, two recent systematic reviews of interventions targeting frequent users of EDs found that case management is the most frequently cited and most effective strategy in reducing ED visits among this population (Althaus et al., 2011; Kumar & Klein, 2013). Furthermore, the intensity of the case management intervention appears to correlate with improved outcomes, reinforcing the need for comprehensive, highly individualized strategies (Kumar & Klein, 2013).
The Camden Coalition of Healthcare Providers (CCHP) has been a leader in using population-level health data. They have created a health information technology infrastructure to better understand the complexities of the city’s vulnerable population. The Coalition’s “hot-spotting” approach to identifying the most complex patients has given way to a national dialogue around using innovative data strategies to target complex patients. Allocating resources to the small proportion of the population that accounts for the majority of the city’s health care costs is proving to be beneficial (Gawande, 2011). This pilot study with promising preliminary results seeks to build on previous research by demonstrating how data sharing can be successfully used to not only organize and improve communication within the wider health care community but, more important, also identify and serve vulnerable populations through an intensive care management intervention.
Theoretical Framework
The Coalition’s Care Management Program was designed to target high-cost, complex patients for improved care coordination based on the principles of the chronic care model (CCM) and the patient-centered medical home (PCMH). Components of the models overlap and can work synergistically in the same care setting. The CCM identifies the essential elements of providing high-quality chronic disease care, including patient-centered health delivery, self-management support, improved decision making, community involvement, clinical information systems, and organizational support (Bodenheimer, Wagner, & Grumbach, 2002; Rothman & Wagner, 2003; Wagner, Austin, & Davis, 2002). The creators of the CCM have developed a care coordination model, which looks at care coordination from the perspective of a PCMH and recognizes that there are several external providers and organizations with which a PCMH must interact. The model identifies four elements that contribute to successful referrals and care transitions: assuming accountability, providing patient support, building relationships among providers, and developing connectivity to support timely and effective information flow among providers (MacColl Institute for Healthcare Innovation, 2010). The Coalition used this model as a guiding framework to harness the data collected through the HIE to identify and target care coordination services to Camden’s most at-risk patients with diabetes and other chronic diseases.
Methods/Strategies/Intervention
The city of Camden occupies only 9 square miles and has a population of 77,334 that is largely Black (48%) and Hispanic (47%; U.S. Census Bureau, 2010). Health care in Camden is fragmented among two inpatient hospitals, three EDs, and multiple primary care and specialty care providers. Providing care in one of the poorest (U.S. Census Bureau, 2012) and deadliest (Federal Bureau of Investigation, 2012) cities in the country has created a great deal of frustration and a unique set of challenges. Making health care delivery affordable and accessible is crucial to the redevelopment of a city that has endured government corruption, high crime, and severe poverty in the past four decades.
As Dr. Jeffrey Brenner, a practicing family physician, witnessed the daily frustrations and health care challenges of city residents, he quickly became frustrated with the state of affairs in Camden and decided to start tackling them at the systems level. Dr. Brenner treated a significant number of Medicaid patients, many of whom had chronic conditions, mental illness, substance abuse, social isolation, and unstable housing. He quickly learned that the best way to stabilize their medical situation was to provide intensive, repetitive, hands-on care while addressing psychosocial needs; however, frequent telephone check-ins were not reimbursed by the Medicaid program, and it was becoming increasingly difficult to care for patients with extremely complex problems in an office setting. He knew a different care model was required to provide support to the sickest and neediest patients and realized that this might be easier if providers came together to assume accountability for improving care to this population.
Development of the Coalition and Camden Health Database
In 2002, Dr. Brenner began meeting with a small group of Camden primary care providers (PCPs) over breakfast to discuss the issues they faced while practicing in the city. Meeting every few months, it was largely an open forum and a welcome opportunity for these providers to share experiences, struggles, and frustrations. They quickly found that barriers or problems any one practice experienced were common and familiar to all. Steadily, the meetings grew in number and drew a diverse group of interested participants, including family physicians, internists, nurse practitioners, and representatives from health services organizations across the city. Over time, it was determined that the group would be better served if it formalized its structure and purpose. The CCHP was created as an independent, nonprofit organization receiving support from a combination of foundation and government funding, as well as member dues from local hospitals.
CCHP spent its first 5 years almost solely on building relationships across the Camden health care provider community—from community-based private practices to frontline hospital staff to social workers across the city. Using those relationships led to the creation of an all-payer database known as the Camden Health Database to inform and evaluate at the citywide level. Examination of these billing data revealed that more than half of all Camden residents received hospital-based services in 2011. Of the $108 million in receipts associated with this hospital-based care, $79 million (73%) was spent on inpatient care and $29 million (27%) was spent on ED care. Total receipts averaged $1,400 per resident or $2,480 per patient. Analysis of hospital claims data indicated that the top diagnoses for Camden residents visiting local EDs were head colds, sprains, and strains, indicating that patients used ED services for illnesses not requiring that level of care. Diabetes and asthma were among the top 10 most frequent inpatient diagnoses and resulted in $37.0 million in charges for 591 patients with these illnesses (Gross, Brenner, Truchil, Post, & Riley, 2013). If properly managed in an outpatient setting, these conditions typically should not result in hospitalization.
Through this database, CCHP pioneered the technique of health care “hot-spotting,” an approach used to analyze data identifying the most frequent users of community health care resources. The findings help inform decisions on how to better care for patients at risk of a major health event before costly ED visits and hospitalizations are necessary. The data showed that costs were highly concentrated within a small subset of all patients; the most expensive (by charges) 1% of patients accounted for 29% of all charges, and the top 20% of patients account for 84% of all charges (Gross et al., 2013). Further analysis of claims data revealed clusters of these costliest patients resided in two buildings in Camden—a nursing home facility and a subsidized high-rise building for seniors—providing a prime opportunity to direct health care resources and services to this subset of patients (see Figure 1).
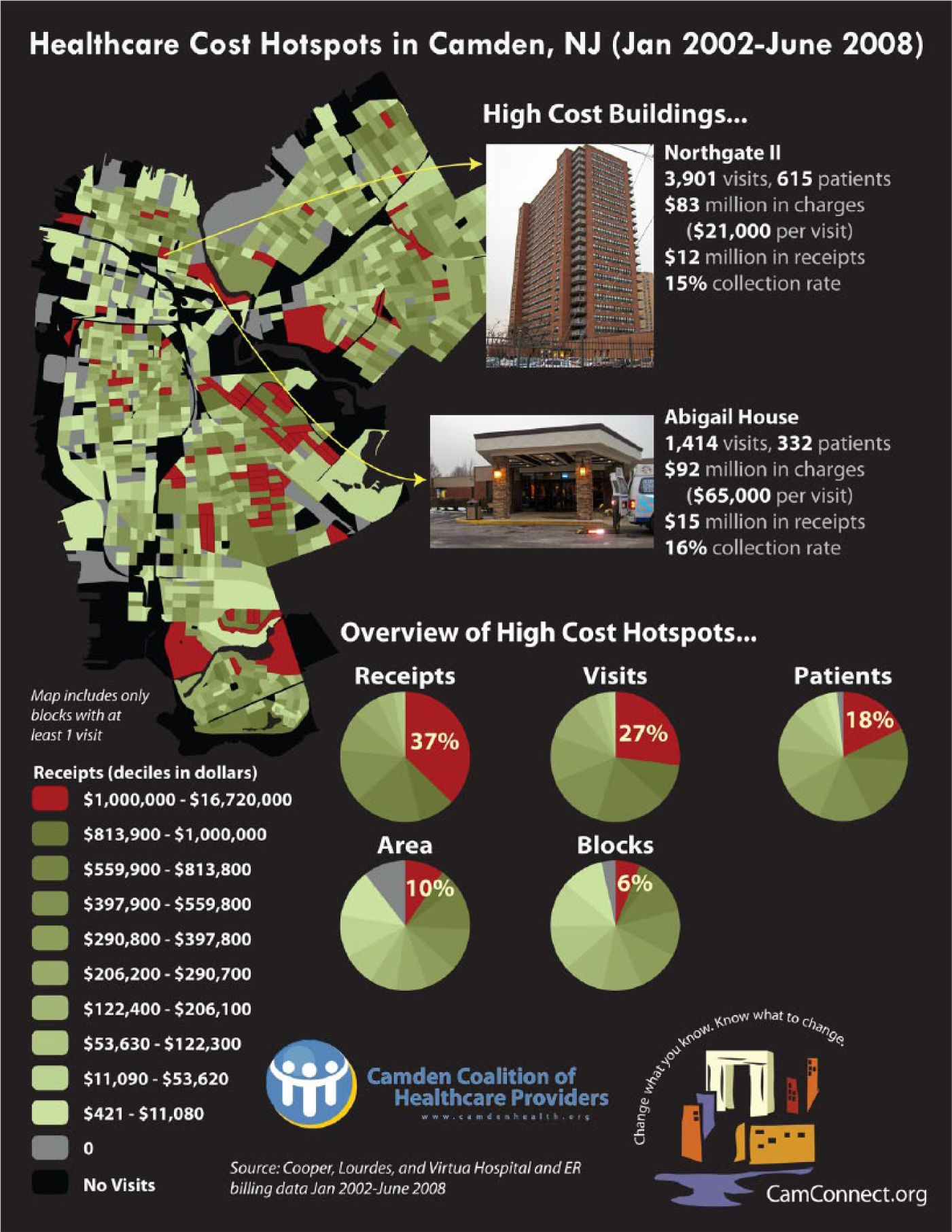
Spatial Analysis of Patient-Level Claims Data to Identify Utilization Hot Spots
Following this analysis, CCHP received additional grant funding to begin piloting an intensive care management model that included frequent check-ins and home visits. The need for real-time data sharing between hospitals and primary care practices became increasingly evident to facilitate communication among health care providers in Camden.
Health Information Exchange
By leveraging existing relationships with hospitals and other health care providers with a shared desire to improve the city’s health care system, CCHP launched the Camden HIE in 2010 through financial contributions from the three Camden hospital systems and grant funding. The Camden HIE is a community-wide HIE developed and managed by CCHP. The HIE currently contains health care information for over 100,000 Camden patients and includes admit/discharge/transfer feeds, laboratory results, radiology results, and discharge summaries from all three Camden hospitals and one lab. Currently, these data are made available to the hospitals and several local primary care practices. The Web-based HIE portal is used by clinicians across Camden to access clinical information about their patients. For example, a clinician can quickly view a patient’s discharge summary or lab result during a visit instead of waiting for the medical record to arrive from the hospital. A clinician can also send a secure message to another provider through the HIE to establish a referral, discuss the patient’s condition, or plan a course of care. In addition to improved provider access to real-time patient information, CCHP has harnessed the data in the Camden HIE to identify high-utilizer patients appropriate for the care management intervention.
Care Management Intervention
The high-utilizer patients eligible for the care management intervention are those who have at least two inpatient admissions within a 6-month period. Eligible patients are identified from a list of potential participants generated by the HIE, which includes data on key demographic variables, diagnosis codes, length of stay, hospital utilization rates, and payer and PCP information. Each day, the lists are reviewed using a qualitative checklist. First, the staff member triaging the patient determines whether he or she had two or more inpatient admissions in the past 6 months. From that group, patients are ruled out by type of admission, including oncology, pregnancy, a surgical procedure, complications of a progressive chronic disease with limited treatment, or mental health–only diagnoses with no comorbid condition (those with a mental health diagnosis and another condition were eligible). Remaining patients are identified for intervention if they have three or more of the following characteristics: two or more chronic conditions; prescribed five or more medications; difficulty accessing services due to a language barrier, low health literacy, or transportation; lack of social support; mental health disorder; actively using illicit drugs; homelessness; or uninsured.
Using this real-time data to target high-risk patients is crucial for timely outreach by CCHP’s care management intervention team. There are currently three outreach teams, each comprising a registered nurse, licensed practical nurses, a community health worker, and health coaches. These teams are also provided with support from social work staff. Each team has an average caseload of 20 to 25 patients. This multidisciplinary team receives daily operational and clinical oversight from a program manager and nurse care manager and strategic direction from a program director and associate clinical director. Training is provided on the ground, in the community alongside other experienced frontline providers coupled with ongoing training on chronic disease management, motivational interviewing, and philosophies surrounding harm reduction and trauma-informed care. The outreach teams are currently supported by a combination of government and foundation grant funding.
CCHP’s high-utilizer intervention is time sensitive and occurs over a 30- to 90-day period. A general example of the workflow can be found in Figure 2. The first 30 days focus heavily on clinical support provided by nurses and social workers. Meeting the patients while they are still in the hospital is a crucial step in the intervention process. This first visit allows the outreach team to make an immediate connection with patients at a time when they need the most help. Once a patient agrees to take part in the intervention, the outreach team can begin coordinating discharge plans with the patient. The nurse provider helps determine if home care or transportation services are needed to get the patient back home. Once the patient is discharged, he or she is visited at home within 48 hours.
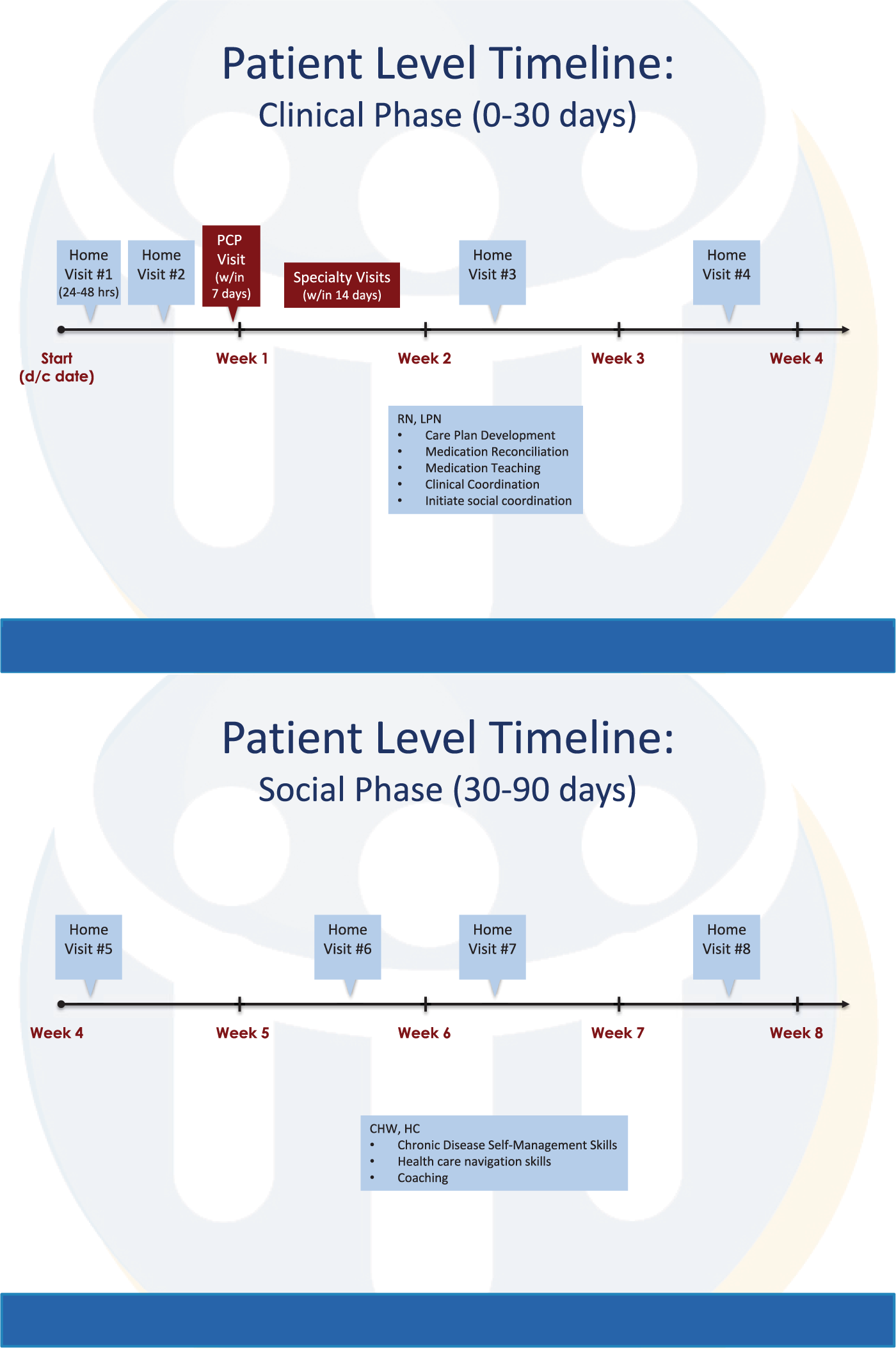
Care Management Team Workflow
The first home visit is critical for both the patient and the outreach team, as it provides an opportunity for the patient to set his or her own health goals and develop a relationship with the team. The success of the intervention heavily depends on the attitude and motivation of the patient. During the initial home visit, the nurse will complete a medication reconciliation, which can often significantly decrease the number of medications the patient is taking. The nurse will also perform a medical equipment assessment if necessary, and a psychosocial assessment during the home visit. The outreach team will then set up a primary care appointment for the patient within 7 days of discharge. A member of the team will attend the appointment with the patient and help facilitate the necessary transportation. The outreach team continues to work directly with the patient through the first 30 days postdischarge. By making weekly home visits, the nurse is able to educate patients on issues such as care for chronic conditions like diabetes and asthma.
After the first 30 days, the nurse transitions the patient to the health coaches and community health workers who will continue to provide social support and education while coordinating appointments and transportation. During the next 60 days, the patient will ideally develop skills to take control of his or her own health care. He or she will learn to make appointments and arrange transportation while simultaneously gaining the skills to manage chronic conditions properly. By consistently keeping primary care appointments, the patient will now have a relationship with and have his or her medical needs met by the PCP, thereby eliminating the need for frequent ED visits and hospital admissions.
Results
The development of Camden’s HIE has involved exceptional collaboration from a variety of stakeholders who came together with the common goal of improving care for the city’s most vulnerable residents. The evolution of CCHP’s care management program has relied on three key achievements: (a) understanding a locality’s population through hot-spotting, (b) developing a technological tool to share information within a fragmented system, and (c) using real-time information to outreach to patients. The linkage of these three components has been essential to improving the care of Camden’s high-utilizer population. In this article, pilot findings on the impact of CCHP’s early care management intervention efforts demonstrate favorable results.
Data from 25 high-utilizer patients with multiple chronic conditions who have received the care management intervention demonstrate reduced utilization comparing 6 months preintervention to 6 months postintervention. Demographic characteristics of these patients are presented in Table 1. Women made up 64% of the sample, and the majority of patients identified as Black/African American, reported English as their primary language, and received insurance through either Medicare (60%) or Medicaid (40%). Close to half of the patients in the sample had diabetes as a comorbidity.
Demographic Characteristics of High Utilizers (n = 25)

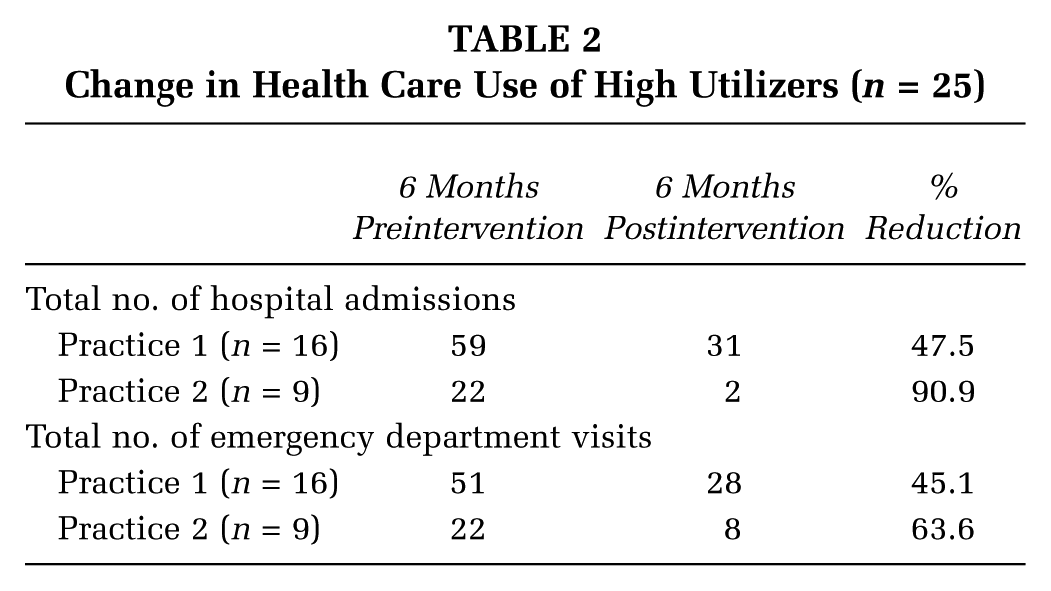
Preliminary health care use data for these patients showed an impressive decline in hospital admissions during the 6-month postintervention period (Table 2). Within this cohort, patients seen by one primary care practice (n = 16) in Camden experienced a 47.5% reduction in the number of hospital admissions 6 months postintervention compared to 6 months preintervention, whereas a second practice (n = 9) has seen over a 90% reduction in the number of hospital admissions for their high utilizers enrolled in the program. Data suggest that patients who received the care management intervention had fewer hospital admissions and therefore incurred lower costs associated with their health care.
Change in Health Care Use of High Utilizers (n = 25)
An example of this initial success can be found in DL’s story. DL is a 50-year-old African American male living in Camden. The year prior to being enrolled in the care management intervention, DL had three inpatient admissions and one ED visit for uncontrolled diabetes. As a veteran, DL struggled with posttraumatic stress disorder and often used alcohol as a coping mechanism. During these periods of excessive drinking, DL would often lose consciousness and find himself hospitalized. The outreach team was able to connect him with the local Veterans Affairs branch for substance abuse counseling, which greatly improved his ability to care for himself and serve as an advocate for his care. Additionally, the team was able to secure regular food for him through a local partnership. DL saw a diabetes educator multiple times and began taking his insulin regularly. To date, now over 1 year postintervention, DL has had no inpatient admissions and one ED room visit. This decrease in utilization has dramatically lowered DL’s health care costs from $20,975 preintervention to $347 postintervention, a 98% reduction.
Discussion and Next Steps
CCHP’s efforts demonstrate that it is possible to create a movement around care for the sickest, most costly patients. The care coordination model proved to be a useful framework for uniting providers in Camden around the common mission of improving care for the city’s high utilizers through linking data sharing with an intensive care management intervention. Now that the care management program has been solidified to ensure that all of the enrolled patients receive a very streamlined intervention, a next step is to examine the impact of this model at the aggregate level. Controlling for regression to the mean and finding an appropriate comparison group will present challenges to modeling hospital utilization at the population level. The promising pilot results from this study are being used by CCHP to partner with academic institutions in implementing a large randomized control trial for the care management intervention, which will help evaluate the program on a macro level.
Although the early results of the care management program provide promising evidence for the potential of HIEs to direct intensive services to high utilizers, challenges remain to this technology becoming widespread. Efficient data sharing within and across organizations requires aligning the incentives and goals of multiple stakeholders, including physicians, hospitals, and health plans, which can be difficult due to concerns about data misuse and loss of competitive advantage (Grossman, Bodenheimer, & McKenzie, 2006; Grossman, Kushner, & November, 2008; Leaver, 2013; Marchibroda, 2008). The success of the Camden HIE is a result of the Coalition’s time and effort in building relationships and trust among providers in the city first, which made the technology much easier to implement. Another key to success was building a basic HIE model to get the data flowing—CCHP did not focus on building an HIE that was too elaborate for the local patient and provider population. Many small provider offices in Camden are barely getting by and have the most basic of resources. An expensive and elaborate HIE might have been overwhelming to local PCPs, causing providers to limit their use.
PCP acceptance of the HIE has been instrumental to the success of the care management program. When CCHP initially began building the program, they relied on referrals from providers, which proved problematic since the patients referred were not always high utilizers, and the real high utilizers were not part of any PCP’s practice. Focusing on the needs of the patient and provider populations along with ongoing collaboration are critical elements for a successful program. CCHP has been a great vehicle to bring large, competing institutions together with small practices toward a common goal.
Another major challenge facing HIEs is ensuring long-term financial viability. Many of these initiatives, including Camden’s, have been made possible at least in part by grant funding, and there is a need to identify permanent funding sources or self-sustaining business models to continue the work (Adler-Milstein et al., 2013; eHealth Initiative, 2012). In conjunction with other groups around the country who are implementing HIEs, CCHP will be working to identify ways to support these efforts into the future, such as shared savings. Long-term funding for care management programs also remains a concern, though there may be opportunities in the current era of new care models, including accountable care organizations (ACOs), PCMHs, and pay-for-performance systems, all of which depend on HIE to deliver high-quality, coordinated, and efficient care (eHealth Initiative, 2014). CCHP has been instrumental in achieving ACO legislation enacted in New Jersey and is in the process of becoming certified as a Medicaid ACO. Last, new policies, particularly around payment systems that require regular cross-provider coordination and participation in HIE, will be crucial to ensuring true sustainability in the long term (NORC, 2009).
The lessons learned and findings from CCHP’s work in a vulnerable, low-resource community suggest this approach may have broad application to other populations and communities struggling to improve quality of care while lowering health care costs. Through a Health Care Innovation Award from the Centers for Medicare and Medicaid Services, CCHP is currently working with four communities across the country, providing technical assistance, resources, mentoring, and remote support, to help them develop local and regional models of care, including a community-based high-utilizer team, a high-utilizer clinic, and targeted care and case management services. In addition, the Robert Wood Johnson Foundation has built on CCHP’s work to support six Aligning Forces for Quality sites around the country that are implementing pilot projects to reduce both ED utilization and hospitalizations among “super utilizers” of health care services. Each site has implemented different models of patient care that are proving to be successful in reducing both costs and ED visits for the patients enrolled in their programs (Putre, 2014).
Conclusion
Improving health care in the United States will require approaches that are both “high tech” and “high touch.” The CCHP has implemented a promising framework that uses data as the link to bring care coordination services to the forefront for high-utilizer populations. This approach has the potential to improve the health of the most vulnerable and costly patients in communities throughout the United States.
Footnotes
Supplement Note:
This article is part of a journal supplement entitled “The Alliance to Reduce Disparities in Diabetes: Infusing Policy and System Change with Local Experience.” The supplement was supported by a grant to the Society for Public Health Education from the Merck Foundation. The Merck Foundation had no role in the development, writing, editing, review, or approval of the content of any of the articles in this issue.