
Abstract
Salud America! is a national network created to engage Latino researchers, health professionals and community leaders in actions to reduce Latino childhood obesity. An online survey of 148 Salud America! network members investigated relationships between (1) their levels of engagement with the network, (2) self- and collective-efficacy, and (3) behavioral intentions to engage in advocacy for policies that can help reduce Latino childhood obesity. Analyses of these data found that higher levels of Salud America! engagement was associated with collective-advocacy efficacy—greater confidence in organized group advocacy as a way of advancing policies to reduce Latino childhood obesity. A multiple regression analysis found that this sense of collective-efficacy moderately predicted intentions to engage in advocacy behaviors. Salud America! engagement levels were less strongly associated with members’ confidence in their personal ability to be an effective advocate, yet this sense of self-efficacy was a very strong predictor of a behavioral intention to advocate. Based on these findings, new online applications aimed at increasing self- and collective-efficacy through peer modeling are being developed for Salud America! in order to help individuals interested in Latino childhood obesity prevention to connect with each other and with opportunities for concerted local actions in their communities.
The prevalence of obesity remains significantly higher among Latino and African American adults and children in the United States compared to non-Hispanic Whites (Ogden, Carroll, Kit, & Flegal, 2014). Twenty-two percent of Latino children (age 2-19 years) are obese compared with 20% of African American and 14% of non-Hispanic White children (Ogden et al., 2014). Furthermore, rates of severe obesity are highest among Latino children compared with other race/ethnic groups (Skinner & Skelton, 2014). While traditional approaches to reducing the prevalence of obesity among children have focused on individual, household, and community level programs and interventions, increasing emphasis has been placed on the enactment of health-promoting policies, that have the potential to influence obesity at a systems and/or population level (Gortmaker et al., 2011; McKinnon et al., 2009).
To continue these efforts in a culturally relevant manner, Salud America! The Robert Wood Johnson Foundation (RWJF) Research Network to Prevent Obesity Among Latino Children (Salud America!) was established in 2007. As of early 2015, Salud America! is a national network of more than 50,000 researchers, community leaders, policy makers, and other stakeholders who are vested in reducing the prevalence of Latino childhood obesity. Between 2007 and 2012, Salud America! worked to increase the field of evidence on Latino childhood obesity. Since then, Salud America! has focused its efforts on empowering network members to advocate for the creation of obesity prevention policies in predominantly Latino communities.
Network members receive Salud America!’s electronic newsletters and daily information via multiple online (i.e., SaludToday blog) and social media channels (i.e., Twitter, Facebook, YouTube). In addition to generating and disseminating Latino-specific information on childhood obesity, Salud America! launched the first-of-its-kind online Growing Healthy Change platform in 2014. The Growing Healthy Change platform serves as a clearinghouse where individuals can find the latest research, news and policies in progress related to the prevention of Latino childhood obesity. The primary purpose of Salud America!’s Growing Healthy Change platform is to raise awareness of Latino childhood obesity and to encourage network members, and the public, to take action toward reducing childhood obesity in areas with large Latino populations.
Literature Review
Salud America!’s work is grounded in increasing network members’ intentions to advocate by improving self- and collective-efficacy for advocacy. The theoretical framework used to accomplish this is social cognitive theory (SCT). More specifically, SCT constructs of personal cognition, such as self-efficacy and outcome expectations, may be key for fostering an intention to advocate (Bandura, 1986). Self-efficacy reflects one’s confidence in their ability to take effective action, while outcome expectations depict what one believes will occur as a result of a given behavior (Bandura, 1977, 1995). While these two factors partially explain human behavior, social constructs like collective-efficacy are also likely to influence a person’s decision to take action (Bandura, 1998). Collective-efficacy reflects one’s confidence in a group or organizational setting to take effective actions to produce a desired outcome (Bandura, 1995, 1998). Because group achievements are deeply rooted in self-efficacy, a high sense of efficacy among group members is a valuable trait, which may ultimately influence collective-efficacy (Bandura, 1998). The application of these concepts have been demonstrated in numerous empirical studies (Chen & Kao, 2011; Stajkovic, Lee, & Nyberg, 2009; Perrin, Flower, Garrett, & Ammerman, 2005). For instance, one study found that lower levels of self-efficacy among pediatricians acted as a barrier to treatment of pediatric obesity (Perrin, et al., 2005). The authors also found that if given the proper tools to advocate, these pediatricians might be more likely to advocate for policies aimed at improving the weight status of children (Perrin et al., 2005).
Another important component for improving advocacy-efficacy is the communication channel used to empower individuals. Previous studies suggest that online/Internet-based interventions have been successful at influencing individual-level behaviors and improving self-efficacy (Hsu, Ju, Yen, & Chang, 2007; Williams, Bowen, & Ei, 2010). However, research on the effectiveness of social media and online social networking sites for increasing both self- and collective-efficacy for advocacy is limited, and more studies are needed to examine how these constructs might interact to influence individual and group advocacy (Bagozzi & Dholakia, 2002; Korda & Itani, 2013).
The work carried out by Salud America! is aimed at studying how online communication channels can be used to establish, grow and maintain online networks, with the purpose of educating and empowering individuals to take action to improve health for Latino children. The purpose of this study was to document the self- and collective-efficacy for advocacy of Salud America! network members in 2012, prior to the launch of the Growing Healthy Change platform. Specific objectives were to (1) establish a baseline for network members’ individual- and collective-advocacy efficacy, (2) determine network members use of Salud America! Products, and (3) determine if increased use/engagement with Salud America! network and products was associated with increased individual- and collective-advocacy efficacy and intention to advocate.
Method
Survey Design and Development
The survey developed for this study was designed to address the three research objectives listed in the previous section. To establish a baseline for network members’ individual- and collective-advocacy, three questions were developed based on the SCT constructs of self- and collective-efficacy. To capture the core components of these constructs as they relate to advocacy for childhood obesity policies, the following framing statement was developed: Advocacy is about identifying an issue, organizing, and coalition-building, making a case by compiling facts and data, and drawing attention to the issue to work for a solution. The ultimate goal of advocacy is to influence policy development. Support from advocates helps assure that policymakers will adopt, implement, and maintain important obesity prevention policies.
The initial question, “Do you perceive yourself as an advocate for childhood obesity prevention policy?” aimed to categorize respondents as either self-identified advocates or non-advocates. Two statements then aimed to directly capture participants’ self- and collective-efficacy and assess participants’ confidence in engaging in advocacy (“I am confident in my ability as an individual to engage in advocacy activities that effectively help get new policies to reduce childhood obesity” and “I am confident in the collective ability of other people and organizations involved in childhood obesity advocacy to effectively support policy and program changes”). A 10-point Likert-type scale was used to capture participants’ confidence in engaging in advocacy from 0 (not at all confident) to 10 (extremely confident). To capture participants’ intention to advocate, participants could respond unlikely, somewhat unlikely, undecided, somewhat likely, and likely to this question: “In the next 3 months, how likely are you to personally engage in childhood obesity related advocacy and policy development actions?”
To determine network members’ use of Salud America! products, the survey asked quantitative and qualitative questions related to frequency of product use. More specifically, this survey assessed network members’ use of (1) quarterly e-newsletters, (2) monthly e-alerts, (3) program website (http://www.salud-america.org), (4) a daily-populated SaludToday blog (http://www.saludtoday.com/), and content for (5) Twitter, (6) Facebook, and (7) YouTube social media sites. To assess use of these seven products/services, participants were asked “How frequently do you read and/or view the following Salud America! network products?” Participants could respond by selecting one of the following: never, rarely, sometimes, often, or all the time.
In addition to these questions, the survey captured demographic information (i.e., gender, age, race, education, occupation) and participants were asked about other network products/materials they would find beneficial for becoming engaged in advocacy for Latino childhood obesity prevention (i.e., understanding lobbying rules, packaging research for policymakers, etc.).
Statistical Approach
Descriptive statistics were used to determine respondent characteristics. To determine if increased use/engagement with the Salud America! network and products was associated with increased individual- and collective-advocacy efficacy, a Salud America! engagement index variable (EIV) was generated. The EIV summed respondents’ self-reported frequency of use for all seven network services. The use of an index variable to measure online engagement is an approach that has previously been used by communications researchers (Gil de Zúñiga, Jung, & Valenzuela, 2012). Each of the seven network services contributed equally to the EIV. Individuals who indicated “never” using one of the seven products received a value of 1 and those who indicated “all time time” received a value of 5. This allowed EIV scores to range from 7 to 35. The EIV was used to determine variable correlations and to perform a multiple regression analysis to determine if exposure to the Salud America! network components mediated network members’ self- and collective-efficacy and intention to advocate for Latino childhood obesity prevention policies.
The SPSS V.19 statistical software was used to conduct all study analysis. A pair- and variable-wise deletion method was used to account for as many cases as possible. These data were not weighted and complex sampling designs were not used.
Survey Administration
The developed survey was distributed via email to all Salud America! network members in early December 2012 and remained active until the end of January 2013. A survey reminder email was sent 2 weeks after the initial email and once more the day before the survey deadline. Although the Salud America! network has now grown beyond 50,000 members, the network had 2,010 members at the time of survey administration (December 2012). Participation in this survey was voluntary for all network members and the survey was not incentivized.
Results
Descriptive Statistics
A total of 148 individuals, approximately 7% of the 2,010 member network at the time of dissemination, participated in the Salud America! Survey (demographic characteristics of participants are given in Table 1). The majority of respondents were between ages 50-59 years (30%) and female (80%). More than half the respondents were Latino (65%) and approximately 70% identified their race as White, followed by Black or African American (8%), American Indian or Alaska native (4%), and Asian (3%). Twenty-five percent of the sample identified themselves as multiracial. Most respondents had a master’s or doctoral degree (35% and 38%, respectively), followed by 21% who had bachelor’s degrees. Respondents’ main occupations were in public health (52%), research (31%), and/or academia (26%).
Demographic Characteristics of Survey Participants
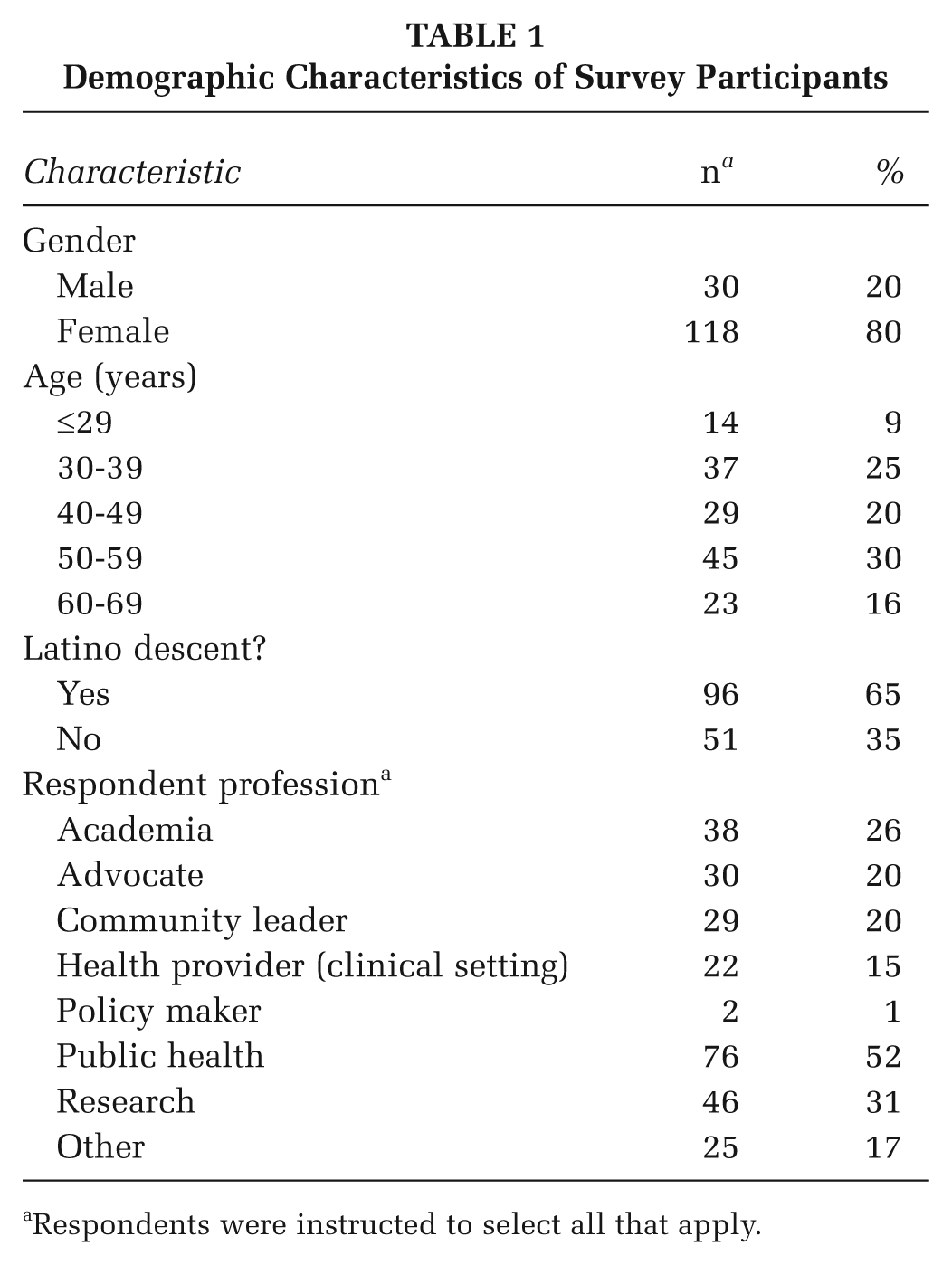
Respondents were instructed to select all that apply.
Network Services
When asked how often they read Salud America!’s quarterly e-newsletter and monthly e-alerts, 25.7% of respondents indicated all the time and 39.3% indicated often (Table 2). In response to visiting Salud America!’s website, while nearly half the respondents (46.1%) indicated sometimes visiting, 27.7% rarely visited the website.
Percentage of Respondents Who Use Salud America! Network Offerings
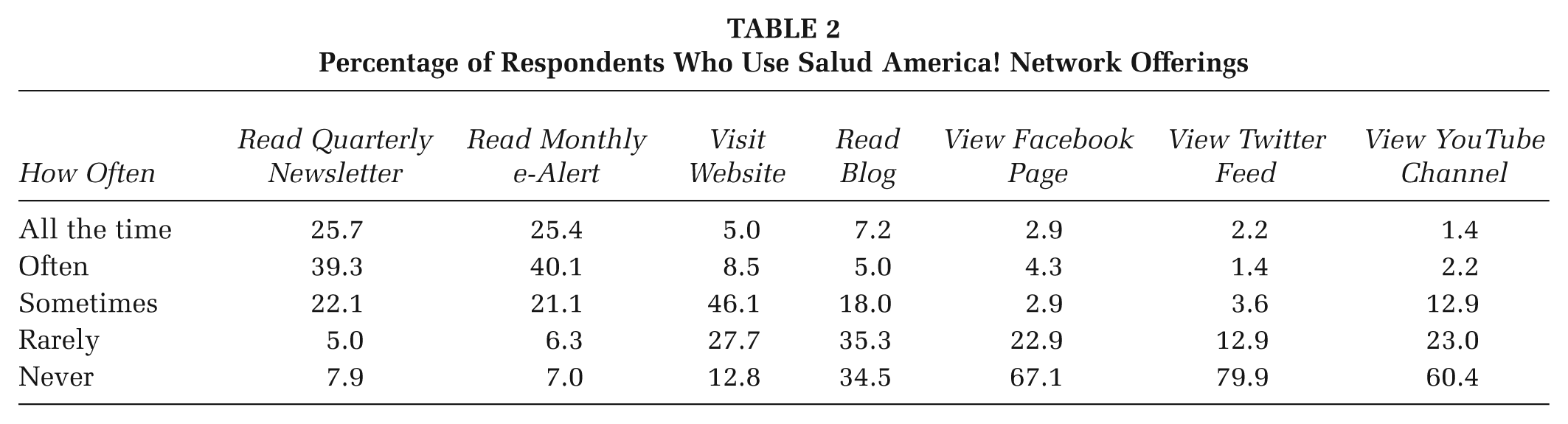
Use of social media network services appeared to be dependent on member demographics, namely age. Of those surveyed, approximately 40% of individuals aged 39 years and younger visited Salud America!’s Facebook (40%), Twitter (41%), and YouTube (39%) channels. Network users between the ages of 40 and 69 years used social media platforms like Facebook, Twitter, and YouTube, less frequently at levels of 17%, 5%, and 30% respectively.
Self- and Collective-Efficacy for Intentions to Advocate
The mean score for individual confidence to engage in advocacy (M = 6.98, SD = 2.4) was slightly lower than confidence in the group’s ability to support policy and program changes (M = 7.66, SD = 1.72). Regarding intentions to advocate in the next 3 months, 38% indicated that they were very likely and 24% indicated that they were likely to engage in childhood obesity–related advocacy. The remaining 38% stated that they were either undecided, somewhat unlikely or unlikely to engage in childhood obesity related advocacy. Initial examination of variable correlations indicated that higher EIV scores were positively associated with greater confidence for collective-advocacy efficacy as a way to advance policies to reduce childhood obesity (see Figure 1). However, higher EIV scores were not associated with members’ individual confidence to advocate for policies to reduce childhood obesity. Additionally, intention to engage in advocacy was strongly predicted by self-efficacy and only moderately predicted by collective-efficacy.
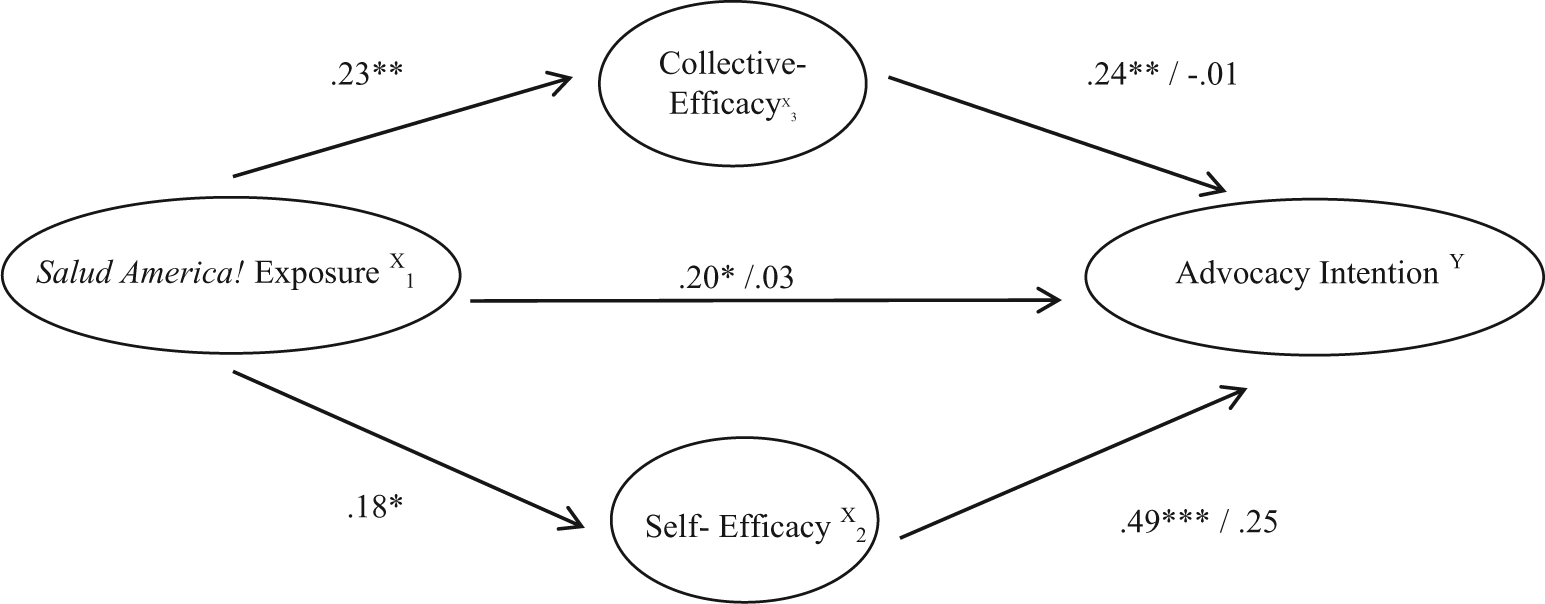
Mediated Pathway of Salud America! Exposure, Efficacy, and Advocacy Intention
Multiple regression results determined that when Salud America! exposure (measured via the EIV), self- and collective-efficacy were used as predictors, 26% of the variance in intention to advocate could be predicted (R = .51 and R2 = .26). The overall model was statistically significant, F(3, 111) = 12.45(p < .001). Complete results for the multiple regression analysis are presented in Table 3.
Multiple Regression Model to Predict Advocacy Intention from Salud America! Exposure, Self-Efficacy, and Collective-Efficacy

NOTE: R2 = .257; R2adj = .236. N = 112.
p < .05. **p < .01. ***p < .001 (all two-tailed).
Only self-efficacy was predictive of intention when exposure and collective-efficacy were controlled for: t(111) = 5.07, p < .001. The positive slope for self-efficacy indicated that there was about a 0.25 point increase in intention for each 1 point increase in self-efficacy, controlling for exposure and collective-efficacy. The squared semi-partial estimate of how much variance in intention was uniquely predictable from self-efficacy was sr2 = .176. About 18% of the variance in intention was uniquely predictable from self-efficacy (exposure and collective-efficacy was statistically controlled). Neither exposure nor collective-efficacy was predictive of intention in the regression model. Overall, intention was highly predictable from this set of predictors, with self-efficacy as the strongest contributor. Correlations and regression coefficients are presented in model results displayed in Figure 1.
Discussion
The primary purpose of this study was to document the self- and collective advocacy-efficacy of Salud America! network members and to determine if increased use/engagement with Salud America!’s network and products was associated with increased individual- and collective-advocacy efficacy and intention to advocate. Results of this study determined that Salud America! online and social media engagement appears to reinforce and possibly strengthen collective-efficacy among its network members, which is a moderate predictor of advocacy intentions. Salud America! engagement, however, is not strongly correlated with self-efficacy, which is a powerful predictor of behavior (Bandura, 1977).
Limitations
This study is not without limitations. Survey questions were specifically designed to assess objectives for childhood obesity advocacy and the instrument used was not validated or tested for reliability. However, the questions posed were selected to best measure the SCT constructs, self-efficacy and collective-efficacy. Additional limitations to this study include having a small sample size relative to the network (7%) and the lack of a randomly selected sample. However, it should be noted that the response rate for other online surveys ranged between 9% and 30% (Cook, Heath, & Thompson, 2000; Deutskens, de Ruyter, Wetzels, & Oosterveld, 2004). Finally, the data collected for this study are based on self-reported measures of online network engagement, rather than on views tracked by website metrics, which is prone to some amount of error due to bias.
Future Research
Despite these limitations, this is one of the few studies that has attempted to measure self- and collective-advocacy efficacy in an online network. In addition, to the authors’ knowledge, this is the first study to measure both advocacy efficacy and intention to advocate among an online network with the sole purpose of reducing childhood obesity in predominantly Latino communities. To more effectively promote advocacy for policies to reduce Latino childhood obesity, Salud America! continues to strengthen both self- and collective-efficacy through peer modeling, increased use of social media tools, and by connecting network members and the public to advocacy efforts for effective childhood obesity prevention policies (Vet, de Wit, & Das, 2011).
Conclusion
As online advocacy becomes more prominent, the development of online networks and online network structures may be an effective means for increasing individual- and collective-advocacy efficacy for health-related policies. The findings of this study show support and promise for the development of online networks and potential for increasing individuals’ collective-advocacy efficacy for health-related policies. Ultimately, increasing self- and collective-advocacy efficacy among Salud America! network members may serve as a way to mobilize individuals toward action, to reinforce community grassroots efforts, and to engage individuals in policy-related work aimed at curbing Latino childhood obesity.
Through developing and refining online resources that target Latinos, and having an understanding of how these materials influence an individual’s sense of self- and collective-efficacy for advocacy, online networks like Salud America! have the potential to drive support for change and potentially even shift the dynamics in which policy issues are addressed by providing an online environment of true community engagement.