
Abstract
Learning collaboratives (LCs) are a popular tool for supporting collaboration and shared learning among health programs. Many variations of LCs have been reported in the literature. However, descriptions of key LC components and implementation lack standardization, making it hard to compare and contrast different LC approaches. To advance the field’s understanding of how primary elements of LCs are implemented, we describe the implementation of an LC in the Ryan White HIV/AIDS Program using a recently established taxonomy of four primary elements of LCs—innovation, social systems, communication, and time. Additionally, we explain the strengths and challenges we encountered with regard to each of these elements when implementing this LC. We then offer recommendations to others on how to leverage LC facilitators and mitigate challenges in future projects. This information can guide other programs to replicate beneficial practices and avoid pitfalls in future LC projects.
Learning collaboratives (LCs) have a long-standing history in health programs. An LC is a network of participants, which could be individuals, organizations, or organizational systems, that come together to share information, work toward a goal, and/or conduct work on a particular topic (Institute for Healthcare Improvement, 2003; Wenger-Trayner & Wenger-Trayner, 2015). Examples of topics LCs have helped address include increasing uptake of routine HIV testing (Rodriguez et al., 2016), promoting evidence-based engagement strategies in early intervention programs for young children (Haine-Schlagel et al., 2013), and addressing health disparities (Chin et al., 2004; Chin et al., 2007; DeLorenzo et al., 2019; Fernandes et al., 2012; Landon et al., 2004; Landon et al., 2007; Oyeku et al., 2012; Taplin et al., 2008). LC projects in health care are typically related to achieving health care quality measures.
Although the idea of bringing participants together to share knowledge and collectively problem solve seems inherently beneficial, the demonstrated outcomes of LCs are mixed (Nadeem et al., 2013; Schouten et al., 2008; Wells et al., 2018). A challenge to demonstrating LC utility and effectiveness across programs is lack of clear articulation of LC elements and implementation from project to project (Solberg, 2005; Wilson et al., 2003). LCs described in the literature use various models and implementation approaches (Nadeem et al., 2013). This flexibility has benefits for practice because it shows LCs can be tweaked, adapted, and molded to fit nearly any project, but there is no widely accepted, standard framework for reporting on LC implementation to compare and contrast key elements of different LC approaches. Lack of a reporting framework complicates research and evaluation because LC attributes are not consistently described, implemented, or measured. Using a standard framework to describe LC implementation can assist researchers with comparing outcomes of similar LC approaches, rather than comparing outcomes of drastically different models.
To help advance the understanding of LCs by clarifying key elements, Nix et al. (2018) developed a taxonomy to describe LCs and thus ground LC outcomes research. The taxonomy describes four primary elements of LCs: innovation, social systems, communication, and time. Table 1 shows these elements and their corresponding subdomains. Innovation refers to characteristics of the idea or practice being taken up by the LC. Social systems refers to the collaborative element of the LC—that is, the environment and structure in which participants interact, work together, and learn. Communication refers to how participants and stakeholders in the LC interact with each other to share information and work toward goals. Finally, time describes the temporal aspects of the LC—for example, the duration of the LC and time taken to recruit participants.
Learning Collaborative Taxonomy
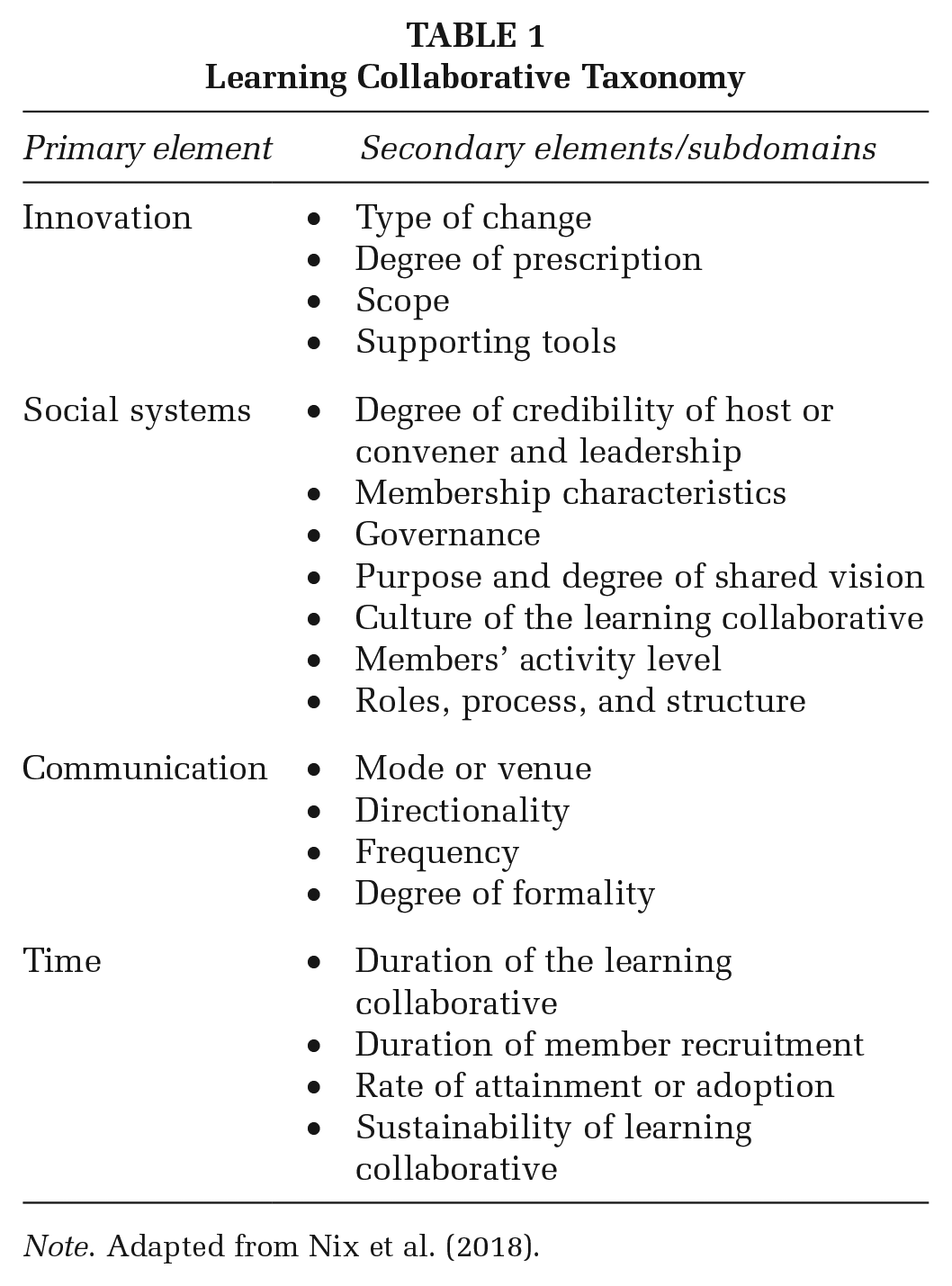
Note. Adapted from Nix et al. (2018).
The objective of this article is to use these four elements (innovation, social systems, communication, and time) to describe how we developed and implemented an LC to improve data capacity—that is, the ability to collect, manage, and use data—and increase uptake of evidence-based interventions in the Ryan White HIV/AIDS Program (RWHAP). We explain the strengths and challenges we encountered respective to each element and provide recommendations to leverage these strengths and address these challenges. This information will guide health programs to amplify and replicate beneficial practices and avoid pitfalls in future LC projects.
Learning Collaborative Context
More than 1 million people are living with HIV in the United States (Centers for Disease Control and Prevention [CDC], 2019), and some geographic areas shoulder a disproportionate share of the HIV burden. More than 50% of newly diagnosed HIV cases in 2017 occurred in 48 counties (representing only 2% of all U.S. counties); Washington, DC; and Puerto Rico (HIV.gov, 2019). The Health Resources and Services Administration (HRSA) HIV/AIDS Bureau (HAB) administers the RWHAP, the largest federal program focused on HIV/AIDS care and treatment. RWHAP provides emergency funding for HIV medical and support services—such as treatment adherence, medical case management, and mental health services—to cities and counties (jurisdictions) most severely affected by the HIV epidemic (HRSA, 2017). Funds are administered to a lead agency in the jurisdiction that then distributes them among a network of organizations that provide direct services to people with HIV. We use the term jurisdiction in this article to describe the lead agency and its associated network of direct service organizations.
Disparities in HIV care and treatment persist in the United Sates despite advances to curb HIV transmission and ensure the health and well-being of people with HIV (Fauci et al., 2019; Frieden et al., 2015). The HIV care continuum is a structure for understanding disparities along the steps from HIV diagnosis to successful treatment with antiretroviral medications (see Supplemental Appendix Figure 1; (CDC, Division of HIV/AIDS Prevention, 2018). Data are routinely compiled at the jurisdiction, state, and national levels, and indicators along the HIV care continuum are monitored to gauge HIV response effectiveness. National indicators show that, among all people with diagnosed HIV in the United Sates, only 73% are receiving HIV primary care, 57% are retained in HIV primary care, and 60% are virally suppressed (CDC, Division of HIV/AIDS Prevention, 2018). Reducing disparities along the HIV care continuum would improve public health by decreasing HIV transmission and HIV-related morbidity and mortality (Gardner et al., 2011). RWHAP jurisdictions are uniquely positioned to improve HIV care continuum indicators at the national level because they provide care to a disproportionate share of people with HIV in the United Sates.
Jurisdictions, however, encounter substantial barriers to addressing disparities along the HIV care continuum including inadequate technology, poor care coordination, and limited availability of services (Hirschhorn et al., 2009). Jurisdictions also report barriers with sharing information and data, service overlap and duplication, and unwelcoming clinical environments that dissuade people with HIV from seeking health care (Philbin et al., 2014). Opportunities therefore exist among jurisdictions to share information and best practices, improve data capacity and utilization to inform decision making, and leverage community partnerships to better track, target, and reduce disparities along the HIV care continuum. The collaborative, rapid-learning approach of an LC, and its focus on affecting system-level change and uptake of evidence-based interventions, provides a useful tool for jurisdictions to address these barriers and improve disparities along the HIV care continuum. Furthermore, LCs were used to address similar problems in other programs (see DeLorenzo et al., 2019; Haine-Schlagel et al., 2013; and Selk et al., 2015 for examples).
In 2015, HRSA HAB funded the Care Continuum Learning Collaborative (CCLC). Abt Associates and its partners from Mission Analytics Group, National Alliance of State and Territorial AIDS Directors (NASTAD), and Isenberg Consulting designed, implemented, and evaluated the CCLC. The CCLC aimed to reduce disparities along the HIV care continuum by improving data capacity and utilization and increasing uptake and replication of evidence-based interventions among participating jurisdictions.
Method
Innovation
Generally, the CCLC sought to effect change along the HIV care continuum. However, it set out to do that by working with jurisdictions on more proximal changes—particularly focusing on improving data capacity and data use and improving uptake of evidence-based interventions. These were the innovations on which the CCLC focused. We borrowed the concept of Communities of Practice—defined as people with a shared interest who engage in collective learning to identify and test ways to address an issue—to help inform how we organized the CCLC to make progress in improving data capacity and uptake of interventions. Communities of Practice organize around a shared domain, or area, of interest, and each participant decides which goal(s) they will work toward within that domain (Wenger-Trayner & Wenger-Trayner, 2015). Following that idea, the CCLC prescribed a set of broad domains into which jurisdictions self-selected. Then, from there, jurisdictions would each define specific goals and strategies they would implement within their chosen domain. Almost all domains were related to improving data capacity and use and/or improving uptake of evidence-based interventions.
CCLC domains were selected using the following process: First, on CCLC launch, the CCLC’s expert committee (described in the next section) provided input on potential domains based on HRSA HAB priority areas. Second, all 52 RWHAP jurisdictions were invited to participate in a meeting to identify domains that would be organized under the CCLC. The goal was to select a set of domains relevant to jurisdictions’ needs that were related to data capacity and intervention uptake and that would yield an impact on HIV care continuum measures. Jurisdictions that opted to participate in the domain selection process (42 of the 52 [81%]) were formed into eight small groups, and a 90-minute, web-based meeting was held for each group. Groups were formed based on jurisdictions’ availability to attend the meeting during a specific time slot. Meeting attendees included up to two representatives per jurisdiction who were likely to be project directors for the RWHAP jurisdictions, data managers, and/or evaluation leads. During these meetings, a facilitator presented the list of proposed domains, described the vetting process, and sought feedback using a semistructured interview approach. The Abt Associates project director, who was selected due to having more than 20 years of qualitative interviewing and focus group experience, facilitated the meetings. Finally, feedback was compiled, synthesized, and posted online for comments. Jurisdictions were charged with reviewing the meeting notes and posting comments, edits, and feedback online during a 2-week period.
The CCLC organizers reviewed feedback and used it to select five domains for the CCLC’s first year. HRSA HAB priorities determined which domains were offered in Year 1 as compared with Year 2. These domains were (1) data access and coordination; (2) using data to inform the need for, and selection of, evidence-informed approaches; (3) identifying and implementing targeted evidence-informed interventions; (4) linkage to care; and (5) changing health care landscape. The two domains selected for the CCLC’s second year were (6) pay for performance and (7) data to care, which were chosen by jurisdictions from four potential domains put forth by HRSA HAB. In total, the CCLC supported work in seven domains (see Table 2).
Care Continuum Learning Collaborative Domains
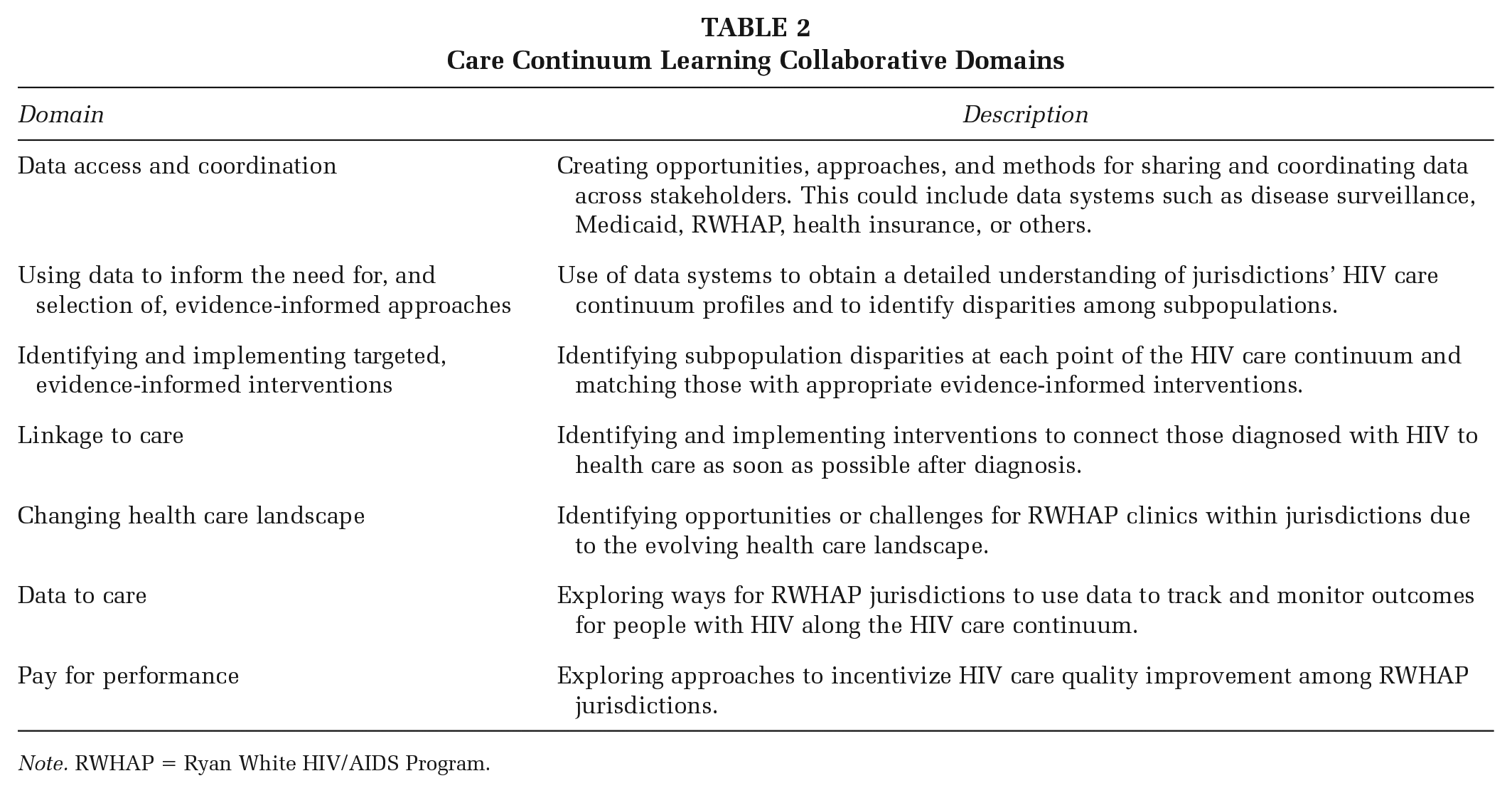
Note. RWHAP = Ryan White HIV/AIDS Program.
Once domains were determined, all jurisdictions were then invited to participate in the CCLC and sign up for a domain at the start of each year of CCLC implementation. Participation was voluntary, and jurisdictions were not funded to participate in the CCLC. By promoting jurisdiction-directed goals and outcomes—and not being heavily prescriptive—the CCLC aimed to inspire participation while providing the structure through which jurisdictions could conduct work in areas they felt were beneficial and useful to them.
Social Systems
The CCLC’s structure and activities were informed by the Breakthrough Series (BTS) LC model developed by the Institute for Healthcare Improvement (2003). Aspects of the BTS include topic (domain) selection; recruiting experts who establish the vision for the collaborative, develop content, and provide coaching; participant enrollment; conducting learning sessions during which participants learn strategies, develop improvement tests and share information; action periods during which organizations test and track changes; dissemination; and evaluation (see Supplemental Appendix Figure 2).
Staff from Abt Associates, Mission Analytics, NASTAD, and HRSA HAB led the CCLC and comprised its core implementation team (Figure 1). The team conducted the planning and operations of the project, including establishing the CCLC infrastructure, engaging jurisdictions, and providing training and technical assistance (T/TA) for participating jurisdictions. An expert committee was assembled of 10 members with subject matter expertise in HIV research, practice, advocacy, and program oversight. The committee worked alongside the implementation team to identify HIV care continuum priority areas, deliver T/TA on specialized topics, and provide input on CCLC activities when their assistance was needed. Domain leads from the implementation team coordinated and oversaw work in each domain. An independent evaluator worked in parallel with the implementation team and designed the evaluation, developed data collection protocols, collected and analyzed data, and reported results. This core team was perceived by project staff to have strong credibility among jurisdictions in that it was comprised of a main funder, field and policy experts, and HIV evaluation and implementation specialists with decades of experience.

Structure of the Care Continuum Learning Collaborative
The culture of the CCLC was self-directed, flexible, and supportive. Each jurisdiction determined their own goals and how they would go about achieving them. Peer jurisdictions—that is, other jurisdictions participating in the collaborative—were included to share helpful strategies and provide encouragement, and the CCLC offered tailored T/TA on requested topics. The domain lead helped jurisdictions articulate their goals, develop strategies, and troubleshoot barriers.
The CCLC set initial expectations for participation. Jurisdictions were asked to complete a readiness assessment (see details in Supplemental Appendix) as part of the CCLC onboarding process that equipped domain leads with preliminary information, such as readiness for change, data capacity, and current efforts. Participating jurisdictions were uniquely positioned to take up CCLC work because of their experience in data-driven, community-based needs assessments; procurement of HIV medical and supportive services; working with providers to coordinate services; and serving diverse populations. They were also committed to employing efforts to positively affect the HIV care continuum. Another expectation was that each jurisdiction develop action plans to improve processes related to their specific goal(s), which aligned to the domain in which they were participating. Action plans articulated each jurisdiction’s objectives to achieve their stated goal, proposed strategies to be tested, stakeholders to engage, timeline for completion, and measures of success. Domain leads monitored jurisdictions’ progress, assessed TA needs, and held jurisdictions accountable for testing improvement strategies.
The evaluation was a prominent component of the CCLC’s structure and process, in that it informed the implementation team’s activities, assessed jurisdictions’ progress, and collected information about the barriers and challenges jurisdictions faced while conducting their work. The evaluation aimed to assess the extent to which the CCLC activities were implemented as planned, were of high quality, and had the desired results. The evaluator engaged stakeholders to inform the evaluation, including the design, implementation, data collection, and analysis. T/TA activities were tracked, and jurisdictions completed an online survey about perceived quality of CCLC activities, challenges and successes, and outcomes achieved. Outcomes included improved data capacity, increased use of data to identify gaps along the HIV care continuum, increased implementation of interventions to address disparities, improved staff capacity, and whether or not jurisdictions were able to determine the feasibility of pay-for-performance activities (see additional details in Supplemental Appendix). Jurisdictions were invited to participate in a 30-minute phone interview following survey completion in the first year to gather qualitative data about the perceived impact of the CCLC and experiences with CCLC participation. Data were collected and synthesized by the evaluator. Results were shared with the implementation team to identify areas of success as well as any needed improvements.
Communication
The CCLC used several modes of communication. First, the Advancing Collaboration through Interactive Online Networks (ACTION) portal was an online platform that enabled online collaboration both among jurisdictions and between the implementation team, experts, and jurisdictions. Similar online platforms have proven to be a useful tool for LCs (Gray, 2004; John et al., 2014). The ACTION portal was critical to the project since the majority of CCLC activities were conducted virtually. Information, such as best practices and relevant journal articles, was regularly posted to the portal by the implementation team. The portal also housed a document repository where jurisdictions could post resources (e.g., tool kits) and share updates on action plans. Discussion boards were available for troubleshooting challenges in real time and for routine interaction between jurisdictions and domain leads. Additionally, jurisdictions could use the portal to meet and interact with each other by video conference.
Second, the CCLC held monthly learning sessions to foster communication among jurisdictions. Learning sessions entailed convening jurisdictions in each domain to develop and refine their action plans and share their activities and progress. These learning sessions provided cross-jurisdiction information sharing and an opportunity to troubleshoot any challenges. They were facilitated by domain leads and occurred by video conference.
Third, the CCLC implementation team shared information with jurisdictions by conducting targeted T/TA. Jurisdictions were able to request customized T/TA to complete the work described in their action plans. T/TA requests were vetted and coordinated by the domain leads. Local, regional, or national experts on the topic area then provided the T/TA to the specific jurisdiction(s) that made the request.
Finally, the CCLC communicated information externally, beyond the CCLC’s boundaries, to other stakeholders in the HIV field. External dissemination consisted of presenting lessons learned through HRSA-sponsored webinars, meetings, and conferences.
Time
CCLC implementation took place over the course of 2 years (July 2016 through June 2018). The initial domain selection and recruitment process spanned approximately 6 months, and recruitment for the second year spanned approximately 2 months. Work on the first year’s domains took place for approximately 12 months, whereas work on the second year’s domains took place over a period of about only 6 months due to the funding timeline. Individual participant time commitments involved attending an hour-long learning session each month and to up to four additional hours per month implementing action plans.
Findings and Recommendations for Practice
This section describes findings and recommendations for practice determined from (1) evaluation data; (2) information gleaned from process documents, such as progress reports and project call notes; and (3) perceptions of the implementation team about what worked well and areas for improvement. Table 3 summarizes our recommendations that correspond to each LC element.
Summary of Recommendations by Learning Collaborative (LC) Element

Innovation
Characteristics of the innovation include the type of change being addressed by the CCLC, extent to which that change was prescribed by the CCLC organizers, and the scope of the innovation (i.e., broad or narrow; see Table 1).
Strengths/Challenges
Twenty-seven RWHAP jurisdictions, which represent 52% of all RWHAP jurisdictions (n = 52), participated in the CCLC. Participating jurisdictions represented 27 urban and suburban cities in 17 different states (see Figure 1). The flexibility the CCLC offered in terms of allowing jurisdictions to choose their domain and specify their own goals was a strength that promoted participation. The CCLC helped facilitate—rather than revamp—their work. For example, one jurisdiction representative reported, “I probably would have been able to complete this [on my own] but it would have taken me longer.” Some jurisdictions, however, found the level of flexibility challenging. These jurisdictions were accustomed to the original BTS model, where all participants work toward the same prespecified goal, and criticized the CCLC for lacking a common goal for each domain. For example, one survey respondent reported, “All [jurisdictions] had good projects but [the projects] weren’t connected so we could learn from each other.” The flexibility in goal setting offered by the CCLC was a strength for some jurisdictions but a challenge for others.
Action plans varied widely across jurisdictions in terms of goals and strategies. Jurisdictions’ goals ranged from using data to examine gaps along the care continuum (e.g., using data to understand the extent of viral suppression), to plans to address identified gaps (e.g., increase retention in care rates to 80% among all RWHAP clients in the jurisdiction), to addressing staff burnout and retention (e.g., instituting clinical supervision to reduce caseworker burnout). Another strength of the CCLC was that it supported jurisdictions to accomplish what they already set out to do while providing a structure to learn from peers and experts throughout the process.
Recommendations
We recommend conducting a thorough assessment during the project planning phase, to figure out whether a structured approach, in which participants work toward the same prespecified goal, or a flexible approach, in which participants name different goals that align with a particular domain, is most suitable. First, consider the objective of the LC. If the main objective is to enable information sharing to assist participants with reaching their own goals in a general area, such as raising awareness around domestic violence, then a flexible approach is appropriate. If, however, the main objective is progression on a particular, narrow outcome, such as increasing flu vaccination rates, then a structured approach is appropriate. Additionally, ensuring that LC participants are supportive of the LC’s flexibility level at the outset is necessary for their engagement. Collecting information about participants’ flexibility tolerance during the project planning process, by either collecting that information in a readiness assessment or conducting a preliminary focus group, is essential.
Social Systems
Features of the social system include the degree of credibility of CCLC leadership; its defined roles, structure, and culture; and participants’ characteristics and involvement (see Table 1).
Strengths
One strength was that jurisdictions found the shared structure, timeline, and accountability provided by the CCLC useful for implementing their action plans and achieving goals. One jurisdiction representative reported, “[The CCLC] kept me on track and allowed me to focus.” Another strength was the caliber of the implementation team and T/TA providers. One jurisdiction representative reported, “[The domain lead] was phenomenally good.”
Challenges
The major challenges reported by jurisdictions related to social systems were lack of engagement of some jurisdictions and too much heterogeneity among jurisdictions participating in the domain. One jurisdiction representative reported as a challenge that “all members couldn’t/didn’t participate in all meetings, so their expertise was missed.” Furthermore, another jurisdiction representative reflected on the other jurisdictions in their domain, “So many of us were at different starting points.” This heterogeneity made it difficult for domain leads to identify and provide T/TA that was equally relevant and useful to all jurisdictions in the domain. Additionally, jurisdictions reported challenges specific to implementing the work in their action plans. These were predominantly organizational barriers such as staff turnover, absent leadership, and competing organizational priorities.
Recommendations
To ensure that the necessary organizational support is in place as part of the recruitment process, meeting with participants’ leadership to gather more information about their motivation for participation and also convey the LC’s expectations for participation would be helpful. Allocating time during the project development phase to help participants build the organizational infrastructure needed for optimal participation by obtaining leadership support, engaging stakeholders, and ramping up staffing to ensure the work of the project is adequately resourced will help mitigate some organizational challenges later in the project. Then, the LC should routinely monitor organizational barriers and assist participants with resolving them as needs arise. One concrete way to provide assistance is by providing T/TA on resolving organizational barriers (e.g., gaining leadership buy in), and not only providing T/TA on topics specific to the LC’s content area (e.g., HIV data utilization).
Communication
Characteristics of communication include the modes of information sharing within the CCLC, directionality and frequency of information sharing, and degree of communication formality (see Table 1).
Strengths
Throughout the CCLC, jurisdictions exchanged data collection tools, standard operating procedures, helpful strategies, and lessons of what not to do. Jurisdictions found this aspect of the project invaluable and unique—no other formal mechanism currently exists for jurisdictions to coordinate and collaborate on HIV care continuum activities. One jurisdiction representative reported that the CCLC was an “excellent forum for discussion and idea sharing,” and another expressed, “We benefitted from the resources shared, and learned from other participants as well.”
One strength was that the learning sessions and T/TA activities were valued by jurisdictions. On a scale of 1 to 5 (1 = poor; 5 = excellent), jurisdictions gave the learning sessions an average score of 4.2. Twenty-nine T/TA activities were provided over the implementation period, and the jurisdictions provided an average rating of 4 on a 1 to 5 scale (1 = poor; 5 = excellent) when asked to what extent the TA provided was of high quality.
Another strength was that using the ACTION portal as a tool for communication enabled more jurisdictions to participate in learning sessions than would have been possible if they were conducted in person. The portal allowed real-time collaboration and information sharing while minimizing costs. The areas of the ACTION portal most frequently utilized by jurisdictions were discussion boards, virtual meetings, and resources pages.
Challenges
The ACTION portal had an average of about 22 users per month but use slowly declined over the course of the project. One drawback that jurisdictions noted was that the ACTION portal was not an efficient way to share documents. They expressed it was sometimes easier to email documents rather than logging into the portal to access them. Jurisdictions generally liked the idea of the portal and its design but found it clunky to use.
Recommendations
To address the drawbacks of the ACTION portal, we recommend selecting low-barrier tools and online platforms that participants are already familiar with to share resources, such as common file sharing applications like Dropbox. Learning to use a foreign system could be daunting and off-putting to some and thus act as a barrier to participation. Also, having so much of the LC be virtual discourages those who are not as comfortable with technology from participating, and that could be a lost learning opportunity. Conducting a focus group at the beginning of the LC to ask potential participants the types of online tools and technology they are comfortable using (or learning to use) would help avoid this challenge. An important theme is to determine participants’ preferences and shaping the LC tools to meet participant preferences. Having the first meeting of LC participants in person is recommended, if financially feasible.
Time
Characteristics of time include the duration of the LC overall, time period of participant recruitment and activities, and plans for sustainability (see Table 1).
Strengths
The 6-month duration for domain selection was adequate, and the 12-month duration for conducting work in the first year’s domains was reasonable for jurisdictions to accomplish the majority of their goals.
Challenges
The timeline for work on the second year’s domains was limited to 6 months, which hampered jurisdictions in terms of achieving the goals they articulated in their action plans. Jurisdictions reported that 6 months was too short to effect major change, given that action plan development alone took most jurisdictions several months.
Recommendations
Two recommendations to address timing constraints in LC projects are first ensure the time allocated for participants to conduct their work is sufficient—a good practice is to expect it to take about 30% longer than anticipated. This was determined based on the experience with CCLC participants as they worked to achieve their goals. Second, ensure that the planned work is adequately scoped for the duration of the LC. One strategy to do this is to encourage participants to start with a 1-month mini project to become accustomed to the process and potential pitfalls, then scale the project up as time allows. Doing so enables participants to celebrate a small accomplishment and build momentum toward tackling larger goals.
Conclusion
This article contributes to the body of research on LCs by using the four elements of LCs to describe implementation of an LC in the RWHAP. LCs are a widely-used and useful tool for much of the work we do; this article highlights the attention required for the different aspects of LCs in terms of the type of change it aims to foster, how best to structure an LC, communication channels and modes, and timing. Altogether, the information presented in this article shares our experiences gleaned from the project so that others can more effectively implement LCs in future work.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399211019983 – Supplemental material for Strengths and Challenges of Implementing a Learning Collaborative in the Ryan White HIV/AIDS Program
Supplemental material, sj-docx-1-hpp-10.1177_15248399211019983 for Strengths and Challenges of Implementing a Learning Collaborative in the Ryan White HIV/AIDS Program by Leigh Evans, Jennifer Carter, Michael Costa, Deborah Isenberg, Luigi S. Procopio, II, BA and Steven R. Young in Health Promotion Practice
Footnotes
Authors’ Note:
The authors would like to thank Diane Fraser and Monique Richards for their guidance and work on this project, as well as our project partners at NASTAD and Mission Analytics Group. We would also like to thank the 52 Ryan White Part A jurisdictions for their engagement and participation and Jane Fox for her thoughtful review of the manuscript. This article was funded by the U.S. Department of Health and Human Services (HHS), Health Resources and Services Administration (HRSA), under cooperative agreement no. U69HA292980302. The views expressed in this publication are solely the opinions of the authors and do not necessarily reflect the official policies of HHS or HRSA, nor does mention of the department or agency names imply endorsement by the U.S. Government. The authors declare that there is no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.