
Abstract
Background
The U.S. Preventive Services Task Force recommends referral of all obese children to intensive weight management programs. When available, programs are limited to clinical settings and do not address social determinants of health barriers to healthy weight among Latinx immigrant families. Active and Healthy Families, a Spanish-language, culturally tailored group visit intervention has demonstrated effectiveness in decreasing child body mass index but does not address barriers to frequent engagement with the health care system nor social determinants other than immigration. Adapting the intervention for community-based delivery, and to address additional social determinants, may facilitate participation and increase acceptability and engagement among Latinx immigrant families.
Purpose
To engage a stakeholder network in planning adaptations of an evidence-based weight management intervention for community-based implementation.
Method
Guided by the intervention mapping-adapt process, we solicited feedback from a stakeholder network from August 2018 to March 2020. The stakeholder network assessed fit, planned adaptations and identified essential intervention components using photovoice, a Participatory Action Research method, and meetings incorporating user-centered design approaches.
Results
The stakeholder network membership included Latinx immigrant families, community leaders, health care delivery experts, and researchers. Planned adaptations included curriculum changes to discuss social determinants barriers to behavior change and goal setting to mitigate them.
Conclusions
We successfully engaged a stakeholder network and, using a systematic process, identified adaptations of an evidence-based weight management intervention to allow for community-based implementation. Sustainably addressing obesity disparities for Latinx children also requires addressing structural factors to reduce social determinants of health barriers at the population level.
Keywords
Latinx children have the highest rates of childhood obesity among any of the U.S. racial or ethnic group (Ogden et al., 2012; Skinner et al., 2016). The Centers for Disease Control reports that among U.S. children and youth aged 2 to 19 years, 26% of Latinx children are obese compared with 22% of non-Latinx Black children and 14% non-Latinx White Children (Centers for Disease Control and Prevention, 2019). U.S.-born Latinx children in immigrant families have a higher rate of childhood obesity than other Latinx children (Gordon-Larsen et al., 2003). Out of more than 18 million Latinx children in the United States, about half are members of immigrant families (Mather & Foxen, 2016). Both a disproportionately high prevalence of low income, which is a strong independent risk factor for childhood obesity, and factors related to acculturation to the United States contribute to a higher risk of childhood obesity for Latinx children in immigrant families (Gordon-Larsen et al., 2003; Lee et al., 2014).
There is a critical public health need to decrease lifetime cardiovascular disease (CVD) risk among Latinx children in immigrant families that stems from childhood obesity (de Ferranti et al., 2019). Among obese children ages 5 to 17 years, 70% already have at least one CVD risk factor in addition to obesity such as high blood pressure or an unfavorable lipid profile (Freedman et al., 2007). In a study of 8- to 16-year-old obese Latinx children, where nearly all had immigrant parents, 16.5% already had prediabetes/diabetes based on the blood tests performed as part of the study (Isasi et al., 2016).
Though obesity prevention remains an important goal, the persistent and pervasive disparities in childhood obesity for children of color and low-income children and the negative health effects of obesity across the lifecourse have resulted in an increasing focus on its treatment. The U.S. Preventive Services Task Force has recommended that all obese children be referred to an intensive weight management program to prompt behavior changes to decrease body mass index (Grossman et al., 2017). Intensive programs are mainly found in clinical settings, are limited in number, and are frequently impractical for Latinx immigrant families facing transportation, language, financial, trust, and other barriers to frequent engagement with health care systems (Thornton et al., 2017). Reducing obesity disparities for Latinx children requires addressing the gap in availability of evidence-based obesity treatment programs tailored to the sociocultural needs of Latinx immigrant families.
In this study, we applied community-based participatory research (CBPR) principles to a multisector stakeholder network, including Latinx immigrant families and Latinx-serving community organizations, to take steps to bridge the gap between current recommendations and effective and practical treatment programs addressing childhood obesity disparities among Latinx children. A core tenet of CBPR is the equitable involvement of community stakeholders in defining priority health problems in their communities and identifying solutions (Page-Reeves, 2019). Our stakeholders had previously identified childhood obesity as a priority health problem and the need for adaptation of an existing obesity treatment program to meet community goals and priorities. Adaptation of an evidence-based intervention is a threat to fidelity and maintaining effectiveness. A systematic approach to intervention adaptation with a focus on maintaining essential intervention components can mitigate any negative impact on effectiveness and promote rigor in the evaluation of adaptations (Bartholomew Eldredge, 2016). In this study, we also employed intervention mapping-adapt, a systematic process that leverages health behavior theory and the best available evidence to identify adaptations of evidence-based interventions for a new population or context (Bartholomew Eldredge, 2016). A fundamental aspect of intervention mapping-adapt is stakeholder engagement to ensure integration of priorities, preferences, and current practices of organizations involved in delivering the intervention, the local community, and potential intervention participants into the adapted intervention and its implementation (Bartholomew Eldredge, 2016). Intervention mapping has been used successfully in adapting and implementing health interventions among immigrant Latinx in the United States (Cabassa et al., 2018; Rodriguez et al., 2018).
The weight management program identified for adaptation was Active and Healthy Families (AHF), a Spanish-language, culturally tailored group visit intervention for children ages 5 to 12 years and their families with demonstrated effectiveness in decreasing child body mass index (Falbe et al., 2015). The AHF curriculum is based on obesity practice guidelines and stakeholder input and employs the behavioral theory of the transtheoretical model of change. The curriculum was designed to be delivered in Spanish and culturally appropriate for immigrant Latinx families. AHF, however, does not address families’ barriers to frequent engagement with the health care system, nor social determinants of health barriers other than immigration. Stakeholders had identified that community-based delivery could improve feasibility and acceptability. Delivery in a community setting is also more consistent with immigrant family views of obesity as a multifaceted issue that reflects the complexities of family life and the influences of social determinants of health at the community-level (Martinez et al., 2017). Accordingly, the purpose of our study was to characterize the work of a stakeholder network to determine adaptations of the evidence-based weight management intervention for community-based implementation using the intervention mapping-adapt processes to advance the overall goal of reducing obesity disparities through development and implementation of family-centered obesity treatment for Latinx children in immigrant families.
Method
Study Setting
This project was conducted in Baltimore, Maryland, an emerging immigrant city for Latinx. The Baltimore Latinx population nearly tripled between 2000 and 2010, while Baltimore’s overall population decreased by 4.6% (Office of Minority Health and Health Disparities, & Maryland Department of Health and Mental Hygiene, 2013). Baltimore’s Latinx community is composed mostly of immigrants from Central America and Mexico. Latinx immigrants to the United States have been settling in nontraditional destination states in the southeastern and mid-Atlantic regions in recent years (Filomeno, 2017). Engagement of immigrant Latinx populations may be particularly important in nontraditional immigrant destinations because local programs may have limited capacity to meet the health and social welfare needs of immigrant families. Additionally, immigrant social networks may not be well established, resulting in limited collective knowledge about availability and use of existing health services (Filomeno, 2017).
Stakeholder Network Members
Stakeholder engagement based on CBPR principles is foundational to the intervention mapping-adapt process. We engaged a multidisciplinary and multisector stakeholder network using CBPR principles to adapt AHF for community-based implementation from August 2018 to March 2020. The overarching task of the stakeholder network was to inform the development of an effective, financially sustainable, community-based weight management intervention for Latinx children in immigrant families that could be implemented in the study community and would be generalizable to immigrant Latinx communities across the United States. As shown in Figure 1, the stakeholder network convened included four subcommittees and a Steering Committee (see Figure 1). The Institutional Review Board at Johns Hopkins Medicine approved this study.

Stakeholder Network Organization
The Patient Engagement and Community Engagement Subcommittees of the stakeholder network leveraged existing relationships and the community engagement infrastructure of an academic center focused on Latinx health, Centro SOL (Center for Salud/Health and Opportunities for Latinos). Since its inception in 2013, Centro SOL has developed close partnerships with key leaders and organizations in the Latinx community in order to promote equity in health and opportunity for Latinx (Polk et al., 2019). A core program of Centro SOL is the Latino Family Advisory Board (LFAB; DeCamp et al., 2015). LFAB members comprised the majority of members of the Patient Engagement Subcommittee to leverage the infrastructure and processes of LFAB meetings, which include bilingual facilitators (pediatrician, social worker, and Centro SOL staff), a meal, child care, and monetary support for attendees ($30/family). In addition to LFAB members, Patient Engagement Subcommittee Meetings included members of the Youth Advisory Board who were aged 12 to 19 years and were members of Latinx immigrant families. Parents who had previously completed traditional AHF conducted by an academic general pediatrics clinic comprised the balance of the Patient Engagement Committee.
The Community Engagement Subcommittee was led by a community partner of Centro SOL, Comité Latino de Baltimore (hereafter referred to as Comité). Consistent with CBPR principles, the research team engaged with Comité during development of the project and the submission of the funding proposal, and there was shared leadership between Centro SOL and Comité during the project. Comité is a trusted organization within the local Latinx immigrant community and primary point of contact for local government and agencies to engage with immigrant families. Comité selected the other members of the Community Engagement Subcommittee who represented nonprofit organizations, community-based clinics, and immigration advocacy organizations. Comité led the Community Engagement Subcommittee meetings and coled the Steering Committee with the research team.
The project’s research team, Centro SOL investigators, and staff with expertise in health disparities, Latinx health, and implementation science served as the Research Subcommittee, obtained informed consent from participants, and also recruited and engaged with the Healthcare Delivery Subcommittee. The Healthcare Delivery Subcommittee consisted of program leaders across the health care system with which Centro SOL is affiliated. Program leaders include those involved with Health Equity and community health worker (CHW) initiatives, programs to provide care to the uninsured (e.g., undocumented immigrants), and pediatric specialty care focused on obese youth, and those with public health and policy leadership experience.
Stakeholder Network Processes
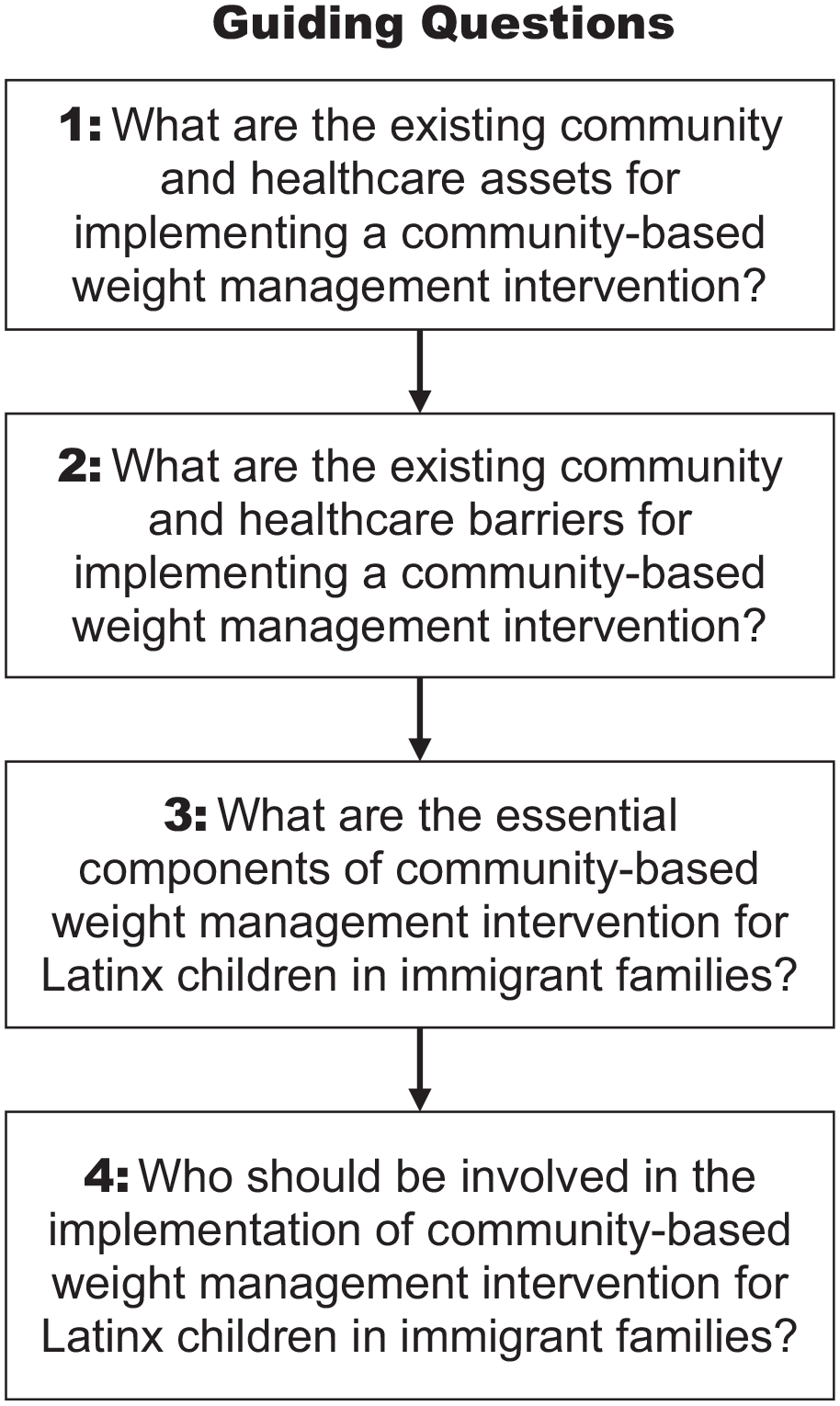
According to the intervention mapping-adapt process, once a candidate’s evidence-based intervention (EBI) has been identified, the next step is to assess fit and plan adaptations where there is not a good fit between the EBI and the implementation context. Fit of AHF was assessed in the following areas: behavioral, environmental, determinants, change methods, delivery, design, cultural, and implementation. After assessing fit we planned adaptations of AHF to improve fit. A primary activity during the planning of adaptations was identifying the essential components of AHF and how to retain these components in the adapted intervention. Four guiding questions were posed to subcommittees to determine AHF fit, potential adaptations, essential components of the intervention, and childhood obesity treatment for children in Latinx immigrant families more generally (see Figure 2). The strategy of guiding questions was used to promote a broad and open discussion and decrease time spent on details of research methods. To synthesize the stakeholder process and determine the adaptations of AHF to enable community-based implementation, we utilized the characterization of complex health interventions as having functions (essential components) and forms (strategies to meet each function; Perez Jolles et al., 2019). Figure 3 displays an overview of the process used (see Figure 3).
Stakeholder Network Guiding Questions

Overview of Stakeholder Network Processes to Complete Intervention Mapping-Adapt
The Patient Engagement Subcommittee addressed Guiding Questions 1 and 2 using the Participatory Action Research method, photovoice. In photovoice, community members take photos related to the project’s theme and then engage in group discussion of the significance of their photos in order to describe assets and challenges in their communities and identify change actions (Wang & Burris, 1997). A subset of Patient Engagement Committee members participated as photographers and completed extra group sessions to complete the photovoice process. All members of the Patient Engagement Subcommittee provided feedback on the themes that emerged from photovoice and participated in the closing photo exhibition. The data generated through the photovoice subproject were analyzed using established methods (Wang & Burris, 1997). The remaining two guiding questions were addressed through meetings during which Patient Engagement Subcommittee members worked in small groups using user-centered design principles, including ranking and prioritizing exercises and generating importance/effort matrices (IDEO.org, 2015).
The Community Engagement, Healthcare Delivery Subcommittees, and Steering Committees addressed the guiding questions through traditional meetings, some of which included user-centered design activities similar to those employed with the Patient Engagement Subcommittee. Most meetings were in-person, though some Healthcare Delivery Subcommittee members attended meetings by phone or via videoconferencing technology. During the process of addressing the guiding questions in the Healthcare Delivery Subcommittee, it was identified that additional expertise in particular areas (e.g., insurance reimbursement for community-based health programs) was needed to inform decision making on AHF adaptations. Thus, we included information from ad hoc members of the Healthcare Delivery Subcommittee via semistructured individual interviews tailored to the interviewee’s expertise.
Stakeholder network meetings for the Patient and Engagement and Community Engagement Subcommittees were conducted in Spanish, a language common to all members. All research team members spoke Spanish. Healthcare Delivery meetings and ad hoc member interviews were conducted in English. Steering Committee meetings were conducted primarily in Spanish with simultaneous interpretation for Healthcare Delivery Subcommittee representatives. Regardless of meeting language or format, detailed meeting notes were taken by Centro SOL research staff. Photovoice analysis sessions and ad hoc member interviews were digitally recorded for reference in finalizing written notes but were not transcribed. Detailed meeting notes were reviewed by the Research Subcommittee to create a summary. Summaries across subcommittees were compared and integrated into materials for review by the Steering Committee to determine fit, essential elements, and potential adaptations. Meeting note summaries and preliminary Steering Committee conclusions regarding fit, essential elements, and potential intervention adaptations were shared during subsequent subcommittee meetings and refined if the conclusions were not felt to reflect prior work.
Results
Stakeholder network meetings for each subcommittee occurred approximately quarterly in various community and hospital-based locations. Most stakeholder network meetings attendees were women, though the photovoice group and Healthcare Delivery Subcommittee had members who were men. Details about stakeholder network meetings and participants are provided in Table 1.
Stakeholder Network Memberships and Processes

Table 2 displays the summary of the fit assessments of the stakeholder network. Differences of fit were identified for environmental, determinants, design, and implementation. The assessment of determinants fit was particularly informed by the results of the photovoice project and their identification of social determinants of health that might render the EBI less effective. Photovoice participants identified four main themes during sessions: food environment in a new community, cultural influences on food, marketing emphasis on unhealthy foods, and the positive and negative aspects of family habits on childhood weight. AHF addresses the cultural and family habits explicitly in the existing curriculum and the social determinant of immigration, which subcommittee members reaffirmed as important. However, community-level determinants affecting food choices and the structural determinant of food marketing were not. Similarly, the Patient and Community Engagement Subcommittees emphasized the need to address neighborhood safety as a barrier to physical activity. Subcommittee members recognized the tension between factors that they had more and less control over in regards to promoting a healthy child weight. They felt the curriculum should be adapted to explicitly address strategies to mitigate negative community- and structural-level determinants. Subcommittee members also emphasized the need to couple the intervention to efforts to address social determinants of health at the community or population level.
Assessment of Fit and Planned Adaptations for Community-Based Implementation of Active and Health Families (Community AHF)
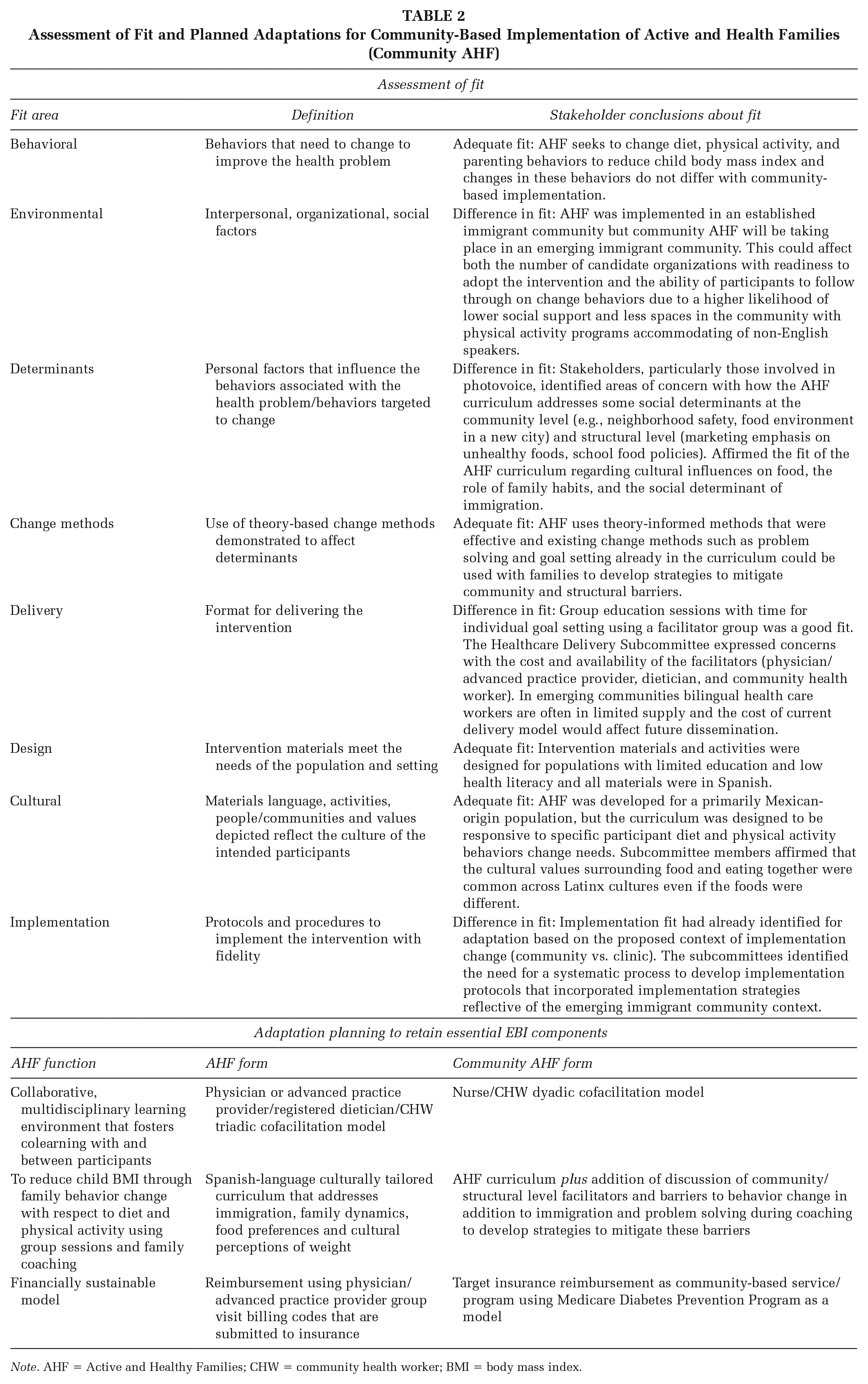
Note. AHF = Active and Healthy Families; CHW = community health worker; BMI = body mass index.
Table 2 also displays the essential components or functions of AHF and the three planned adaptions or form changes for community-based implementation. Key form changes include a change in group session facilitators from a triadic model of a pediatric provider, registered dietician, and CHW to a dyadic model with a nurse and CHW. This planned adaptation would decrease the cost of intervention delivery and address the concern of limited supply of bilingual health professions in the new community. The AHF curriculum and associated behavior goal setting do not require physician-level expertise, but stakeholders prioritized some level of medical training for legitimacy and selected a nurse as an acceptable physician replacement. The second form change is adding to the curriculum an acknowledgement of community and structural barriers to healthy child weight and including a discussion of mitigation strategies in family goal setting sessions. Structural barriers may already be discussed during goal setting sessions with families who bring them up independently, but formal incorporation of goal setting around mitigating social determinants would allow for fidelity measurement and evaluation of impact. The final form change reflects the need for financial sustainability as the group visit insurance billing codes used in AHF could not be used with community-based implementation. The Healthcare Delivery Subcommittee identified that the Medicare Diabetes Prevention Program has key elements that align with goals and strategies of AHF and provides example implementation strategies to facilitate health care to community referral and bidirectional communication to coordinate patient care/follow up. Though reimbursement using this mechanism would not be available in the short term, the Healthcare Delivery Subcommittee identified community-based reimbursable services as a growth area across public and private insurers.
Discussion
In this study, we successfully engaged a stakeholder network and identified adaptations of an existing evidence-based weight management intervention to allow for community-based implementation in a new setting using a systematic process, intervention mapping-adapt. Use of a systematic process ensured that all components of the intervention were assessed so that the proposed adapted intervention retained AHF functions while incorporating form changes to meet the specific needs of the community and new implementation setting. The focus of our stakeholder-engaged process was adaptation of AHF to better address social determinants of health barriers. We anticipated addressing social determinants of health primarily with the change to community-based implementation. Stakeholder network discussions, however, identified additional opportunities to adapt the curriculum in order to address additional social determinants of health barriers to healthy child weight experienced by immigrant Latinx families.
In addition to the planned adaptations, stakeholders prioritized linking the adapted intervention with efforts to reduce community- and structural-level barriers to healthy child weight. To meet this stakeholder priority, the adapted intervention may need to be nested within a multilevel intervention. This is an area for future work for the stakeholder network and highlights a key area of need within implementation research. As the field of implementation research evolves, effective methods to couple dissemination of evidence-based individual/family-level interventions to communities experiencing health disparities with effective interventions to address social determinants of health at the population level are needed.
Our findings provide important information about stakeholder engagement during intervention mapping-adapt to increase knowledge about effective methods and processes to identify adaptations that reflect stakeholder priorities. The importance of leveraging existing community-based partnerships to engage stakeholders to complete the work of intervention mapping-adapt cannot be understated. The Centro SOL research team used existing partnerships and advisory board structures for the Community and Patient Engagement Subcommittees and applied CBPR principles to the process. Of particular importance was shared leadership with Comité. Comité’s broad focus on community needs, resources and resiliency, and not specifically health or health care, was invaluable. Their grounding in the social determinants of health led naturally to consideration of key social determinants in assessing fit and planned adaptations. As existing partnerships were used, there was less focus on partnership development and maturation. Balancing CBPR best practices for assessing and strengthening partnerships and time for practical tasks as part of the adaptation process was challenging. We did complete two rounds of partnership evaluation surveys with Comité and used the standing annual partnership evaluation survey with LFAB/YAB (Youth Advisory Board) members. This limited formal feedback and informal comments of stakeholders indicated this work had an overall positive impact on the existing partnerships.
We believe several methods employed during stakeholder network meetings were also important in achieving stakeholder network goals. First, we used a guiding questions framework that incorporated reflection on synthesized information to assess fit and plan adaptations. Our straightforward, iterative process made the work approachable for members of the Patient Engagement Subcommittees and Comité Latino, most of whom had limited formal education, health literacy and familiarity with research methods. Healthcare Delivery Subcommittee members, some of whom were not researchers, were also able to more efficiently provide input using this format. Second, we used multiple methods of information gathering. A multimodal approach generated discussions and prompted reflection that would have been difficult to achieve with standard group discussion. We believe varying activities during meetings maintained interest and engagement in the project. Additionally, the multiple methods also created additional opportunities for interaction between stakeholder network members and created opportunities for advocacy. The community photovoice exhibition, for example, was attended by local hospital and policy leaders many of whom have limited contact with immigrant families. In the long term, community events may help address the challenge of connecting the intervention to addressing social determinants of health. Finally, the bulk of our meetings were conducted in Spanish, which was the primary language of most stakeholder network members. The use of Spanish as the default language for meetings was a concrete way of supporting shared leadership between the academic researchers and Comité. It also helped balance power between Healthcare Delivery Subcommittee representatives to the Steering Committee and representatives from the Patient and Community Engagement Subcommittees. While conducting stakeholder network activities in non-English languages with immigrant communities may not always be possible or necessary, we believe it was an important aspect of lifting up the voices of a marginalized community and meaningfully integrating them into adaptation and implementation planning.
Limitations
This work is not without limitations. We did not apply formal qualitative methods to the analysis and synthesis of data from stakeholders, with the exception of photovoice data. All members of the research team had experience in qualitative research so discussion of meeting notes and analytic synthesis reflected their experience with qualitative methods. We also relied on continual member checking with stakeholders to ensure that our conclusions reflected meeting discussions. It remains an open question how much analytic rigor is needed when integrating stakeholder perspectives in the adaption process. Time and cost are significant barriers. Rapid qualitative analytic techniques may reduce these barriers, but not enough to make them universally feasible (Burgess-Allen & Owen-Smith, 2010; Gale et al., 2019). Next, our stakeholders included few men. We initially engaged some fathers, but work commitments prevented their continued participation. There is consistent underrepresentation of fathers in childhood obesity prevention and treatment, though their participation may be particularly important to weight management effectiveness (Morgan et al., 2017). A lack of their inclusion as stakeholders prevents adaptation and implementation planning that addresses their particular needs and priorities and could perpetuate low rates of participation in childhood obesity programs. Finally, we acknowledge that defining essential components of any intervention is difficult and that implementation can reveal additional essential components that were not previously appreciated (Wiltsey Stirman et al., 2019). A key next step to maintaining effectiveness is developing implementation protocols via a systematic process to facilitate prompt identification of additional essential components. We plan to employ implementation mapping and retain the current stakeholder network throughout that process (Fernandez et al., 2019).
Implications
First, we believe our findings provide important information on the process of using stakeholder engagement within an immigrant community to adapt an evidence-based intervention to better address social determinants of health that contribute to health disparities. We leveraged existing relationships with stakeholders, many of whose lived experiences provide key insight into social determinants of health barriers and how to address them in the adaptation and implementation planning. Our methods exemplify the successful integration of health disparities research, CBPR, and implementation science methods to more effectively advancing health equity (Chinman et al., 2017). Research teams with experience across these disciplines are critical to advancing the pace at which research contributes to health disparities reduction.
Second, our findings highlight an important challenge for the field of implementation research. Our stakeholders prioritized coupling individual or family-level evidence-based interventions with efforts to attend to structural factors and social determinants of health that contribute to the health problem that the evidence-based intervention was developed to address. Responding to their priority highlights a need to expand the designing for dissemination paradigm beyond dissemination of the evidence-based intervention and efforts to promote financial sustainability, to dissemination activities that also focus on addressing negative social determinants of health at the population level. As we move forward to plan implementation of the adapted intervention, stakeholders involved in implementation mapping will include the community, health care, and policy experts who will continue to work collaboratively to identify opportunities for linkage of the intervention implementation to addressing social determinants of health at the community and policy levels. Health equity for patients and communities will only occur if the focus of implementation research extends beyond adapting interventions and implementation strategies to account for contexts and settings affected by structural marginalization and discrimination. Efforts to adapt evidence-based interventions for implementation in marginalized contexts must be balanced by advancing the science and building partnerships aimed at adapting these contexts.
Footnotes
Authors’ Note:
The authors thank all stakeholders involved in this project. We especially appreciate the time and energy of Comité Latino and members of the Latino Family and Youth Advisory Boards. This project was funded through a Patient-Centered Outcomes Research Institute (PCORI) Eugene Washington Engagement Award (8549-JHU) and a Cross-Cutting Funding Bloomberg American Health Initiative Award.