
Abstract
The primary focus of this research study was to examine the benefit of a using a multimodal approach to speech sound correction with preschool children. The approach uses the auditory, tactile, and kinesthetic modalities and includes a unique, interactive visual focus that attempts to provide a visual representation of a phonemic category. The research compared the effectiveness of traditional articulation therapy with this multimodal approach to articulation therapy for each of two 4-year-old children. Participants demonstrated severe articulation deficiencies in the presence of two very different receptive-expressive language profiles. The findings indicated that the multimodal intervention not only directly improved both participants’ articulation abilities, but also enhanced their developing phonemic awareness and literacy skills. The analysis suggests that early speech sound intervention using a multimodal approach that emphasizes symbols may be more beneficial than a traditional articulation therapy approach for some children, because it promotes phonemic awareness and sound–symbol correspondence.
Phonology, one of the earliest systems of language to develop, is essential to the development of speech sounds, sound patterns, and the rules used to create words with those sounds (Chomsky & Halle, 1968; Wagner & Torgesen, 1987). Phonological processing, or the ability to use phonological information to process oral and written language (Wagner et al., 1997), is vital for linguistic and academic success (Kamhi, Catts, & Adlof, 2012; Shaywitz, 2004; Shaywitz, Morris, & Shaywitz, 2008; Wolf & Bowers, 1999). If a child has phonological processing difficulties, he or she may face problems with phonological input (auditory processing), lexical representation, and/or phonological output (speech; Hodson, 1997; Stackhouse, 1997). Simply put, a sound phonological system is required for efficient phonological processing. Efficient phonological processing is directly related to phonological awareness and phonics development, both of which are among the pre-requisites to future reading and writing achievement (Lyon, Shaywitz, & Shaywitz, 2003; Torgesen, Wagner, & Rashotte, 1994; Wolf, 2007). While phonological awareness is defined as “the ability to attend to and make judgments about the general sound structure of language” (Schuele & Boudreau, 2008, p. 6), namely words, syllables, and sounds, phonemic awareness is more specific. It is the ability to identify and manipulate individual phonemes in words (Gillon, 2004). Phonemic awareness is necessary if a child is to master the alphabetic principle and develop phonics, or the understanding that the visually represented letters of the alphabet represent the phoneme segments in words (I. Y. Liberman, 1983; I. Y. Liberman & Shankweiler, 1985; I. Y. Liberman, Shankweiler, & Liberman, 1989). This is often referred to as sound–symbol correspondence (Gillon, 2004). Compared with other phonological awareness skills, such as onset-rime skills, phonemic awareness has the distinction of being the best predictor of early reading skill (Hulme et al., 2002). The report of the National Early Literacy Panel (Lonigan, Schatschneider, Westberg, & National Early Literacy Panel, 2008) includes phonemic awareness among the essential early literacy skills that must be monitored and developed. Furthermore, research indicates that although it is harder for disabled readers than for normal readers to acquire phonemic awareness skills, they can improve their phonemic awareness with training (National Reading Panel [NRP], 2000). Therefore, if children do not acquire phonemic awareness independently, it should be taught explicitly (Shaywitz, 2004) in an attempt to promote literacy development.
It is widely accepted that articulation errors, phonological processes, and/or a limited phoneme inventory may be indications of a phonological disorder rather than an articulation disorder. In such cases, targeting phonology itself is often more effective (Fey, 1992; Hodson, 1992, 1997; Pena-Brooks & Hegde, 2007). Because phonemic awareness and articulation are directly linked (Roberts, 2005), both are fundamental to academic achievement and literacy. A. M. Liberman (1999) demonstrated that articulation has a greater impact on young children’s perception of speech than do the sounds associated with those gestures, and training in articulation has also been shown to concurrently increase phonemic awareness (Roberts, 2005). Inversely, Kamhi (2006) found that children with speech delays can benefit from training in phonemic awareness because it may lead to improved articulation.
Phonological stimulation must begin as early as possible to encourage later language (Locke, 1997; Shriberg, Gruber, & Kwiatkowski, 1994; Shriberg, Kwiatkowski, & Gruber, 1994) and literacy competence (Goldsworthy, 2003) because a large number of children with early speech and language problems have been shown to have persistent academic problems (Lewis, Freebairn, & Taylor, 2000). In general, research indicates that 50% or more of children with language impairments in preschool or kindergarten go on to have language-based reading disabilities in primary or secondary grades (Bashir & Scavuzzo, 1992; Kamhi et al., 2012). It is also important to recognize that many students with speech and/or language disorders, even those with seemingly adequate receptive language abilities, demonstrate difficulty with the auditory modality (Goldsworthy & Lambert, 2010). Continued research involving phonologically based preschool articulation therapy approaches that support, clarify, and enhance the auditory channels in new and meaningful ways is warranted. The research conducted in this study examines the efficacy of two approaches to preschool speech–sound intervention: a traditional approach that focuses on motor learning with tactile and kinesthetic cues and a multimodal approach that attempts to integrate phonemic awareness and phonics with motor learning.
Traditional Articulation Therapy: The Case for a Multimodal Approach
Traditional articulation therapy is rarely “unimodal.” The child is usually seated. Sensory stimulation is often comprised of some combination of increased auditory modeling and feedback, tactile stimulation of the articulators, and visual feedback through clinician modeling, pictured models of correct articulatory placement, and the use of mirrors (Secord, Boyce, Donahue, Fox, & Shine, 2007). Cognitive connections to phonological awareness or phonics are commonly made informally through alphabetic representations on picture cards. These visuals may indirectly support phonologic–orthographic connections. The resulting methodology may or may not correspond to the learning style of the child in therapy.
Learning styles refer to individual differences in the way individuals perceive and process information. Proponents of the learning styles movement classify students by their optimal means of observing and recalling information: auditory, visual, tactile, or kinesthetic (R. Dunn, 1984). These modalities are believed to ultimately lead to a student’s basic learning style. Trying to match individual styles with instructional strategies is often logistically impossible (Baines, 2008). Furthermore, each human brain is unique, which suggests that there is not one “best” way to teach or learn (Jensen, 2007). The brain learns better under frequent and varied multisensory stimulation and when learners use a variety of cognitive strategies (Baines, 2008; Moats & Farrell, 1999). Adoption of approaches that use multiple avenues to the brain involves students more fully in the learning experience (Baines, 2008).
FONEMZ: A Multimodal Approach
The research discussed in this article adopted the FONEMZ (pronounced /fonimz/) program as a multimodal approach for early speech sound correction and compared its efficacy with traditional articulation intervention methods. FONEMZ was designed to support learners who may have weak auditory skills, including auditory discrimination and processing skills. It was initially used with deaf and hard of hearing populations. Many therapy approaches have been developed to encourage phonological and phonics development (Allor, Gansle, & Denny, 2006; Foster, Gold, & Petzold, 1993; Goldsworthy & Pieretti, 2013). FONEMZ is unique in its attempt to target articulation in a phonologically rich environment: The program is a phonological approach to speech sound correction that emphasizes phonemic awareness by using a different color and shape to represent each of the main phonemes of English.
A FONEMZ kit consists of manipulable symbols that have a distinct color and shape for each of the 40 main phonemes of General American English. To be used in a variety of activities with individuals of all ages, the shapes are made in pairs out of felt, flat magnets, and cardstock. The name used to identify each symbol is the actual phonemic production, or sound, of the phoneme (e.g., /k/), as opposed to the commonly used names of the letters that may make that sound (e.g., “kay”). Some of the symbols partially resemble their corresponding letters, some resemble the shape of the mouth during the production of the sound, and some resemble the International Phonetic Alphabet (IPA) symbol for the sound. The FONEMZ symbols were designed to be somewhat dissociated from the letters of the alphabet to eliminate any confusion that new readers have when presented with letter names and letter sounds at the same time.
FONEMZ uses a hierarchical approach and maintains an inherent focus on the sound system. No prior knowledge is required of a student before beginning. To initiate therapy, the child simply needs to recall 3 to 6 symbols and the sounds associated with them. The auditory, tactile, proprioceptive, kinesthetic, and visual modalities are simultaneously used in an interpersonal and interactive approach: The felt FONEMZ symbols can be stuck to clothing or crumpled up and placed in pockets or containers during phoneme production activities. They can be placed on a felt board to match or contrast the sounds they make, create a shape resembling the vowel quadrilateral, or build words when arranged left to right. The cardstock and magnetic FONEMZ can be fanned out like a hand of cards for the client to select the next one, or placed in a pocket chart or on a white board to create syllables and words. The symbols can be hidden around the room for the client to find and return to the clinician before producing the target phonemes with multiple repetitions in multiple sound combinations. The visual symbol provides something concrete to mark the sound in memory, an anchor for the abstract, fleeting phonemes in language, aiding with discriminating one sound from another.
FONEMZ, the Visual Modality, and Sound–Symbol Correspondence
Multisensory approaches for teaching phonics and letters to young children have long been recommended (Baines, 2008; Gillingham & Stillman, 1997; Justice & Ezell, 2004). The ability to form accurate, phonologically based memory codes is a basic cognitive process. A FONEMZ symbol may provide a visual representation of a phonetic category without the complications of English orthography, which often uses a variety of symbols to produce the same sound (e.g., “c” or “k” for /k/). This visual may help the child mark the sound in memory and promote metalinguistic awareness, or the ability to think about and reflect upon language, particularly in the area of phonological awareness, one of the metalinguistic awareness skills necessary for word recognition when reading (Gillon, 2004). FONEMZ employs a unique visual focus: Each of the FONEMZ symbols represents a single phoneme, providing one-to-one sound–symbol correspondence. This is vastly simpler than the irregular, complex spelling patterns of English which uses more than 250 letters or letter combinations to symbolize 40 distinctive phonemes. To become proficient with an alphabetic writing system, one must first understand the segmental nature of speech and its relationship to print (Blachman, 1991). FONEMZ introduces the alphabetic principle in a way that may be easier for young children to grasp than traditional spelling with letters, providing a bridge to phonics.
Little research has been conducted on the use of specific symbolic visual aids in the remediation of articulation disorders and phonemic awareness. Most of the research that has been conducted has focused on the visibility of other people’s speech (Teinonen, Aslin, Alku, & Csibra, 2008) or on visible methods of biofeedback during speech (Ruscello, 1995), not on the use of symbols to represent spoken sounds. Research does support incorporating a visual aspect to speech and language training. The two neural systems for language and images are reinforcing and interrelated (Gardner, 1979; Menard, Kosslyn, Thompson, Alpert, & Rauch, 1996). The association of sounds with images may be beneficial to the establishment of accurate phonologically based memory codes (Kosslyn, 1976) because children rely on imagery for long-term memory retrieval. Velleman (2002) emphasizes the visual importance of word and syllable shapes for creating meaningful contrasts in a developing phonological system. FONEMZ accomplishes the same goal, using the visual stimuli of shapes and colors to create meaningful contrasts between sounds, promoting the automatic visual recognition discussed by Triedman and Cullen (2002). FONEMZ reinforces the links between articulation, phonological awareness, and phonics, as phonemic awareness of sounds is addressed first in isolation, then in syllables and words.
Research
The study examined the speech and language development of two preschoolers over the course of 20 weeks and was designed to answer the following research questions:
Method
In an attempt to document patterns of acquisition and generalization for individual clients (Gierut, 2001), a single-subject multiple-baseline ABCA research design was used to compare the effectiveness of traditional articulation therapy and FONEMZ therapy for each of two, 4-year-old children.
Participants
The two participants chosen for the study, J.F. and A.F., exhibited severely unintelligible speech, and classroom teachers and instructional aides reported that they each became frustrated during communicative exchanges with family members, teachers, and peers. The participants were selected for this project because of the severity of their speech deficiency and because neither had received any previous speech or language therapy. They were also chosen because their primary language was English and there was no evidence of hearing or vision deficits, intellectual disability, or emotional disorder. Each participant’s articulation was subsequently evaluated using the Arizona Articulation Proficiency Scale–Third Edition (AAPS-3; Fudala, 2000). Their phonological awareness was assessed using the Phonological Awareness Literacy Screening–PreK (PALS-PreK; Invernizzi, Sullivan, Meier, & Swank, 2007), a phonological awareness and literacy screening designed to be administered to 4-year-old children in preschool. A baseline receptive vocabulary measure was obtained with the Peabody Picture Vocabulary Test–Third Edition (PPVT-III; L. M. Dunn & Dunn, 1997). Receptive and Expressive language were measured with the Preschool Language Scale–4 (PLS-4; Zimmerman, Steiner, & Pond, 2002) and a language sample compiled during play-based activities and transcribed by the assessing clinician. The tests used were current at the time of the study and had been validated for the specific purpose for which they were used and the results were considered to be valid.
Participant 1: J.F.
At the time of initial assessment, J.F. was 4 years 1 month old. He received an AAPS-3 rating score of 67.5, which is classified by that assessment as a severe articulation deficiency, characterized by multiple sound substitutions, distortions, and omissions. His speech contained the phonological processes of fronting, final consonant deletion, prevocalic voicing, and cluster simplification. During the course of the assessment, it was noted that J.F. displayed difficulties with focus and did not appear to process many of the simple directions and requests. The results of the PALS-PreK, as reported in Appendix A, indicated that his phonological awareness was below that expected for early reading success: He could not identify any of the initial sounds in the words presented or associate sounds with letters of the alphabet; in fact, he scored zero on every subtest of the PALS-PreK. As a baseline measure, he was presented with a preliminary array of FONEMZ symbols. He was unable to identify any of them. The PPVT-III (standard score 78) and PLS-4 (Total Language standard score 70) indicated that J.F. had significant deficits in both receptive and expressive language. The language sample demonstrated that he consistently produced unintelligible utterances with sentence-like intonation patterns. He also frequently repeated the last one or two words that he had heard. He averaged one intelligible word per utterance, which made comparison with a norm difficult. The predicted average Mean Length of Utterance (MLU) for a student J.F.’s age, however, is at least 4.5 (Lanza & Flahive, 2009).
Participant 2: A.F.
At the time of initial assessment, A.F. was 4 years 3 months old. His AAPS-3 rating score of was 64, which the test classifies as a severe articulation deficiency, characterized by multiple sound substitutions, distortions, and omissions. His speech contained the phonological processes of fronting, final consonant deletion, prevocalic voicing, and cluster simplification. In all but the areas of Beginning Sound Awareness and Rhyme Awareness on the PALS-PreK, as reported in Appendix B, A.F.’s phonological awareness skills were below that expected for early reading success. When presented with a preliminary array of FONEMZ symbols, he was unable to identify any of them. The PPVT-III (standard score 118) and PLS-4 (Total Language score of 114) indicated that A.F.’s receptive and expressive language were in the average to above-average range for his age. The language sample revealed an MLU of 4.0, but 25% of his words were judged to be unintelligible. The predicted average MLU for a student A.F.’s age is at least 4.5 (Lanza & Flahive, 2009).
Selection of treatment targets
In choosing the target consonant sound for each participant, many factors were considered, including consistency of error production and developmental appropriateness. J.F. was beginning to correctly produce /f/, so that sound was excluded. While /l/ is a slightly later developing sound for his age range, it was considered to be an attainable target, given his stimulability for correct articulatory placement. For A.F., /f/ was determined to be an attainable target. Later developing sounds were chosen to give further assurance that sound improvement could not be easily attributed to developmental acquisition. In an attempt to track overall articulatory improvement, two other consonant phonemes consistently misarticulated by each participant were randomly selected to be monitored for improvement. These phonemes were not targeted in therapy. J.F.’s non-target error phonemes were /θ/ and /k/, whereas A.F.’s were /k/ and /t/.
General Procedures
Setting
All therapy and testing was conducted in a speech/language therapy room at one preschool site over the course of 20 sessions. Each biweekly therapy session lasted for 30 min. The clinician for all therapy sessions was the developer of the FONEMZ approach.
Multiple baseline design
A single-subject multiple-baseline ABCA research design was implemented for each participant. The first “A” phase comprised of four baseline sessions focused on language-based therapy activities in which no articulation therapy was performed. This baseline period was followed by the “B” phase, comprised of four sessions of traditional articulation therapy, including repeated drill with typical auditory/verbal and visual presentations. Next, each participant was trained in the use of the FONEMZ program over eight sessions, which made up the “C” phase. The second “A” phase had the same format as the first “A” phase, focusing on language-based therapy with a withdrawal of any articulation-based therapy. Each “A” phase occurred over four sessions, using the same assessment probe that was used throughout the study.
Baseline and treatment sessions
During the baseline phase, the clinician focused on language therapy, including basic concepts (e.g., “same/different,” “not,” spatial concepts, etc.) and interactive activities involving the development of reciprocal dialogs with shared intent (e.g., dollhouse play, book reading, object to picture matching, etc.).
The period of traditional articulation therapy consisted of tactile and kinesthetic stimulation for phonetic placement, as needed, and auditory bombardment of target sounds in various environments (isolation, syllables, words). Most activities required repetition following an auditory stimulus. The participant was seated throughout each session and was presented with a verbal model by the therapist before attempting to imitate the sound. Oral stimulation and/or prompts were given to assist in sound production. Mirrors or pinwheels were used to demonstrate articulator placement and air flow. Tokens or stamps were given for articulation attempts. Consonant plus vowel and vowel plus consonant combinations were used to model combined articulatory movements. Various pictured words containing the target sounds in the initial position of words were presented. These pictures were different from those used in the probes.
During the FONEMZ phase, the clinician first oriented each participant to the FONEMZ symbol system by presenting several FONEMZ symbols in conjunction with a verbal model of each corresponding phoneme. The vowels /α, u, i/ and the consonants /b, p, m/ were chosen because they were different from the target and non-target phonemes selected for the study and because they represented sounds that each participant could already produce. In turn, each participant was asked to choose each of these pre-selected felt FONEMZ from a container. He then listened to the clinician’s production as the clinician held the shape near her mouth. The shape was then placed on the participant’s clothing with the expectation that he repeat it before feeding it to a puppet. Next, the participant placed the shape on the felt board or in the pocket chart for further examination and comparison, and the process was repeated for the next FONEMZ symbol. At the end of each session, the FONEMZ used were sorted by the participant and the clinician and placed in their proper containers to review and reflect on the lesson. When the participant was able to volitionally label these FONEMZ symbols without the clinician’s model, the actual target phoneme was introduced. For example, on Day 2 of FONEMZ therapy, J.F. chose the /α/ FONEMZ symbol and said /α/ without a model from the therapist. On the third day, he did this with three other FONEMZ symbols, so the /l/ FONEMZ symbol was introduced. Therapy then focused on blending the /l/ symbol with vowel FONEMZ symbols and associating these combinations with syllables in a left-to-right progression on the felt board with felt FONEMZ or on a pocket chart with FUN FONEMZ (cardstock versions of the felt FONEMZ) emphasizing emerging VC and CV patterns. Finally, therapy progressed to blending combinations of /l/ with the other vowel sounds to strengthen his comprehension of phoneme blending and the construction of syllables and words using the target phoneme. Whenever possible, spoken words, objects, and pictures were associated with these combinations.
Probes and follow-up assessments
At the end of each of the 20 therapy sessions, each participant’s production accuracy of the target phoneme and two non-target phonemes were probed using cards with pictures containing the target and non-target phonemes in word-initial position. There were 5 cards per phoneme, totaling 15 picture cards per probe. During each probe, the cards were presented in a random order. The second part of the probe included the presentation of each of the three FONEMZ symbols corresponding to the participant’s target and non-target phonemes. The participant was asked to identify the FONEMZ symbol by producing the sound it represented. In addition, each participant was re-administered the AAPS-3 and the PALS-PreK immediately following the intervention period.
Results
Reliability
All of the probes were video-recorded. A DVD was made for each participant with the probes presented in random order. Six judges watched the DVDs separately and transcribed the participants’ productions on each of the probe items. Three of the judges transcribed the videos of all 20 probes for each participant to confirm interrater reliability. The judges were undergraduate students in the Speech Pathology and Audiology program at California State University, Sacramento. Each participant had successfully completed a course in phonetics designed for speech-language pathology transcription and was trained to transcribe the most accurate phonetic representation of what they heard. The judges were provided with a list of the 15 words that each participant would say during the probes. They were not told which phoneme was the participant’s target. Each time a probe was conducted, the pictures of each of the 15 words were presented as a stimulus for the participant, enabling the judges to locate it on the assessment form. The judges were allowed to replay the video as needed to determine the actual production of the participant. Because the probes were presented in random order, preconceptions or expectations for improvement based on session type were eliminated and ensured intrarater reliability. After the judges had completed their transcription, each item transcribed was coded as either a correct (1) or an incorrect (0) production on a spreadsheet for further analysis using IBM® SPSS® Statistics (2012), an advanced statistical analysis software program.
J.F.’s Results
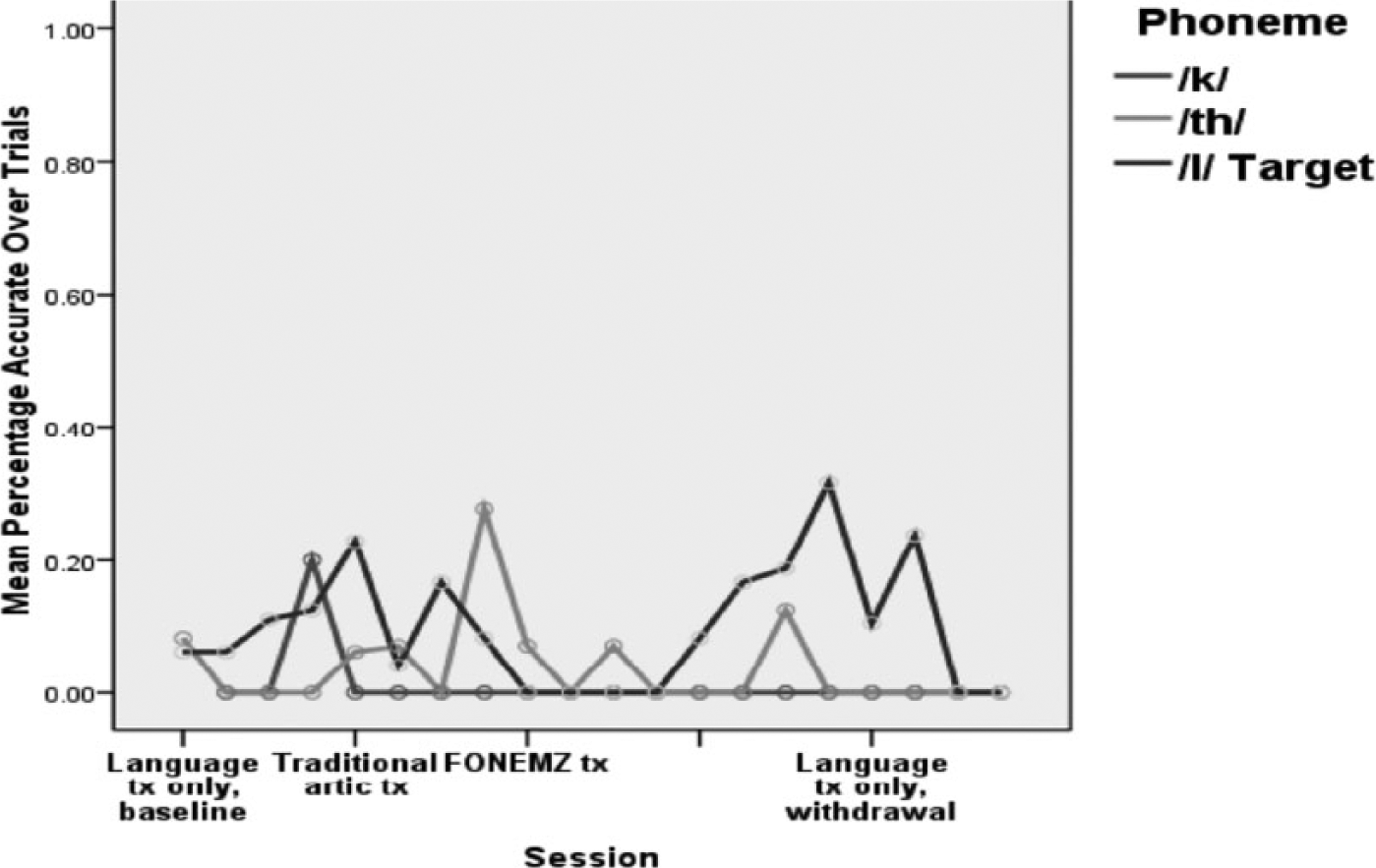
The results of J.F.’s probes by session are highlighted in Figure 1. During the baseline and traditional articulation therapy periods, J.F. demonstrated a range of accuracy across the three phonemes: The target /l/ and non-target error phonemes /θ, k/ were produced with high variability, ranging from 0% to approximately 30% accuracy. J.F. began FONEMZ therapy with the introduction of only non-target FONEMZ for 2 days, during which time he produced a percentage of accuracy below 10% on all three phonemes. The target FONEMZ symbol was introduced on the third day of the FONEMZ period. J.F. began to demonstrate variably improved numbers of correct productions on the fifth day of FONEMZ therapy with the target phoneme. During the period of withdrawal of therapy, J.F. continued to display variable accuracy of production of the target phoneme, with a marked decrease to 0% accuracy on all three phonemes during the last two sessions.
J.F.’s correct productions as generated by SPSS.
An SPSS (IBM, 2012) univariate analysis of variance (ANOVA) was conducted to compare the effect of the phonemes targeted and the therapy conditions on accurate productions. Despite J.F.’s low scores, there were significant differences in percentage of accuracy across phonemes, F(2, 165) = 12.401, p < .0001. This was attributed to the improvement in the target /l/ phoneme used in the initial position in words during post hoc analyses and analyses of means. The effect of condition alone was not significant, F(3, 165) = .151, p = .929. Any trends of accuracy of productions across conditions are more visible when looking at the graph of mean percentage accurate over sessions, particularly when considering the increased accuracy of /θ/ production following the initiation of FONEMZ. There was also no significant interaction of phoneme by condition, F(6, 165) = 1.216, p = .301. This was likely due to the high variability across conditions and low scores over sessions.
Selected results of J.F.’s follow-up assessment appear in Appendix A. He received a score of 75 on the AAPS-3, demonstrating improvement from his pre-treatment score of 67.5. The associated diagnostic category of “severe deficiency in articulation” improved to “moderate deficiency.” J.F. also demonstrated improvement on three of the seven PALS-PreK subtests, most noticeably in the area of Beginning Sound Awareness.
A.F.’s Results
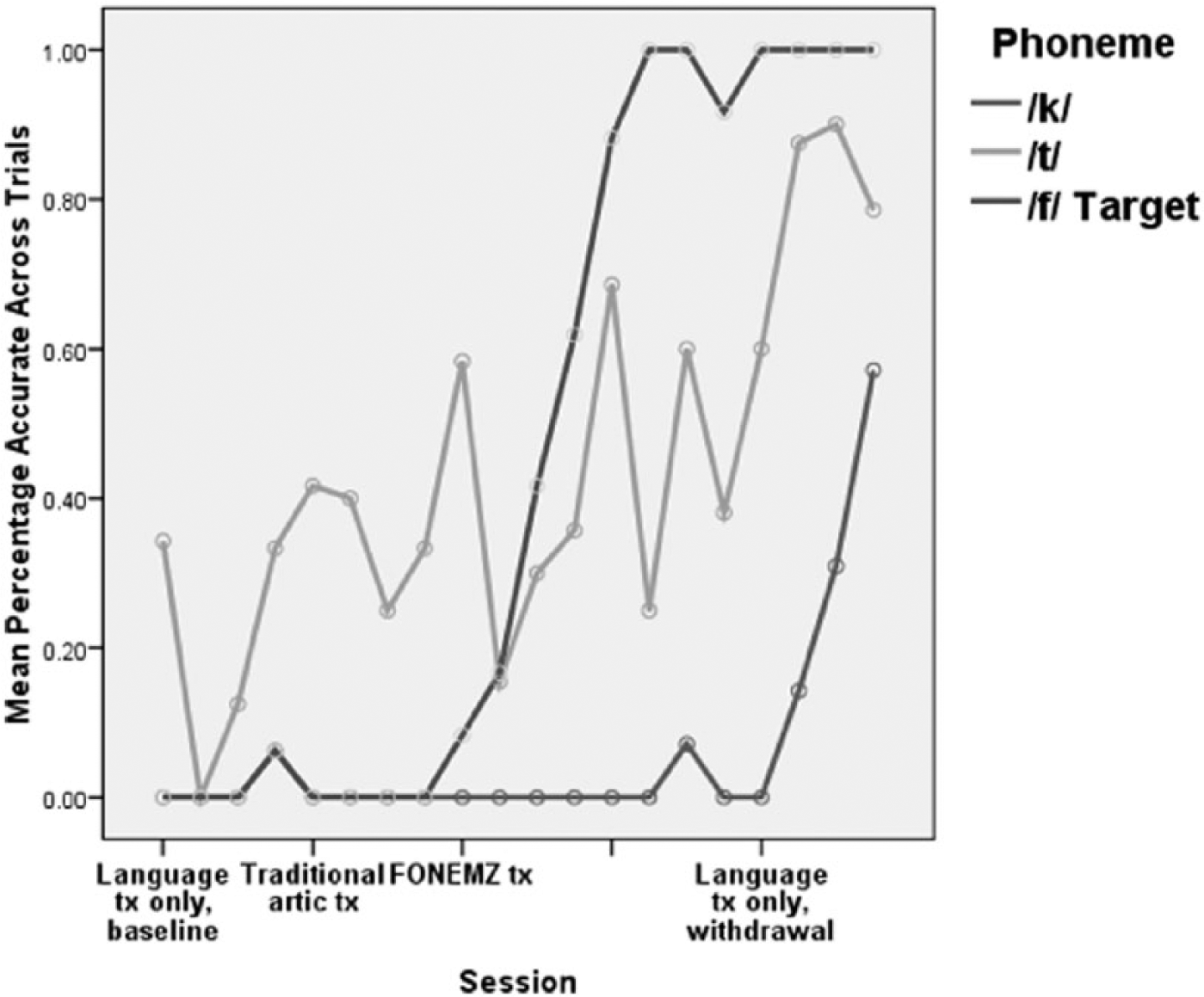
The results of A.F.’s probes by session are highlighted in Figure 2. During the baseline period, A.F.’s accurate productions of the target phoneme /f/ and a non-target phoneme /k/ were extremely low, ranging from 0% accuracy on both phonemes in the first three sessions to approximately 8% accuracy on both phonemes in the fourth session. His accuracy of production of the non-target error phoneme /t/ was extremely variable, ranging from 0% to over 40% across these sessions. During the period of traditional articulation therapy, A.F. achieved 0% accuracy of production on the /f, k/ phonemes across all four sessions. His accuracy of production of the non-target phoneme /t/ varied, ranging from 25% to 60%. On the first day of FONEMZ therapy, A.F. generated volitional productions of non-target vowels and consonants with the second presentation of the associated FONEMZ symbols. Because he could independently differentiate and retain these FONEMZ symbols and their associated sounds, the target FONEMZ symbol for /f/ was introduced. His accuracy of production of the target phoneme improved markedly during the first six FONEMZ sessions, ultimately reaching 100%. His accuracy of production of the /k/ remained at 0% during this period and his accuracy of production of /t/ continued to be highly variable. During the period of withdrawal of therapy, A.F. continued to achieve 100% accuracy of production on the target phoneme /f/. His performance on the non-target phonemes also improved, characterized by a sharp increase in the accuracy of production of the /k/ phoneme, ultimately reaching 60% during the last session. His accuracy of production of /t/ also improved, reaching 90% accuracy in the second to last session.
A.F.’s correct productions as generated by SPSS.
An identical SPSS (IBM, 2012) univariate ANOVA was also conducted on the results of A.F.’s probes. Significant differences in percentage of accurate phoneme production were noted, F(2, 168) = 67.424, p < .0001. This was attributed to the improved production of the target phoneme /f/ and the non-target phoneme /t/ during the study. The effect of number of therapy condition was also significant, F(3, 168) = 55.849, p < .0001, and was characterized by more correct productions following the introduction of FONEMZ. Most noteworthy, however, was the significant interaction of phoneme by condition, F(6, 168) = 11.458, p < .0001. Post hoc analyses and analyses of means suggested that the FONEMZ sessions had a significant effect on accuracy of productions, particularly for the target phoneme /f/ and the non-target phoneme /t/. It was also noted that A.F. demonstrated a visible increase in accuracy of the non-target phoneme /k/ during the period of withdrawal from therapy, but this was not considered to be a major contributing factor to statistical significance as it occurred late in the study and only impacted A.F.’s scores in three sessions.
Selected results of A.F.’s follow-up assessment appear in Appendix B. He received a score of 79.5 (moderate deficiency in articulation) on the AAPS-3, which demonstrated an improvement from his previous score of 64 (severe deficiency in articulation). A.F. demonstrated noticeable improvement on the PALS-PreK, scoring at or above the range for early reading success in the categories of Upper-Case Recognition, Lower-Case Recognition, Beginning Sound Awareness, Print and Word Awareness, and Rhyme Awareness.
Discussion
This study provides some preliminary support to the hypothesis that multimodal approaches, particularly those that support sound–symbol development through the visual modality, are effective in facilitating change in the articulation, phonological awareness, phonics, and overall pre-literacy skills of young children. In this study, one such multimodal phonological approach to speech sound correction appeared to be more effective than traditional articulation therapy in teaching two participants with severe articulation disorders and low phonological awareness to produce a target phoneme with a greater frequency of accuracy. Furthermore, the approach appeared to promote the development of language-based literacy skills for each of two distinct client profiles: one with delayed language abilities (J.F.) and one with average to above-average language abilities (A.F.).
Research Question 1
The two participants responded somewhat differently to the study. J.F. demonstrated variable performance on all three phonemes during the baseline and traditional articulation therapy periods. His accuracy of production of the target phoneme began an upward trend after introduction of the associated FONEMZ symbol, which was not introduced until the third day of the FONEMZ phase. This improvement suggested that he responded better to the multimodal approach. When therapy was withdrawn, an overall decrease in correct productions was noted. Overall, J.F.’s articulation improvement was characterized as relatively slow, continuing to progress over time.
A.F.’s accuracy of production of the target phoneme improved significantly over the course of the study. Statistical analyses indicated that the FONEMZ sessions had the most effect on the accuracy of the target /f/ and the non-target phoneme /t/. Furthermore, during the course of the FONEMZ therapy, it was noted that A.F. began to generalize his knowledge to both non-target phonemes, as demonstrated by his improved production of both target and non-target phonemes during the period of articulation therapy withdrawal. It was noted that A.F. produced the words containing the target phoneme with 100% accuracy on the sixth day of the FONEMZ therapy. He continued to produce all five words with greater than 80% accuracy through the final day of FONEMZ therapy. The target phoneme /f/ was used in all eight sessions of FONEMZ therapy due to the structure of the study. Comparison with an ACBA design would strengthen the current findings, because it could be hypothesized that the traditional articulation therapy prepared participants for success with the FONEMZ approach.
Research Question 2
Both students demonstrated improvement in language-based pre-literacy skills based on pre- and post-testing. Three of J.F.’s PALS-PreK scores, although still below the range indicated for early reading success, improved: Beginning Sound Awareness, a phonemic awareness skill, increased from 0 to 4 over the course of the 20 session study and improvements were noted in the areas of both upper- and lower-case letter recognition. All of A.F.’s subtest scores on the PALS-PreK improved noticeably, and he scored at or above the range for early reading success in five categories. He demonstrated a marked increase in his beginning sound awareness (100%), which is a skill specifically targeted by the FONEMZ approach. It is hypothesized that these improvements may have occurred because the participants, through exposure to this multimodal approach, began to integrate sound–symbol association and articulation to acquire the phonemic awareness and self-awareness skills necessary to identify individual phonemes and change their productions. The fact that A.F. did this so rapidly, whereas J.F. showed slow progress, correlates with existing research that indicates that children with only phonological disorders have better outcomes than children with phonological disorders and additional language problems (Lewis et al., 2000). This analysis is limited, however, due to the study design. It must be noted that once a child enters into any form of speech or language production therapy, the phonological system may be stimulated at a metalinguistic level. A replication of this study, including phonological awareness and language-based literacy skill probes, would strengthen the current findings.
Clinical Implications and Future Directions
This study concurs with the work of both Roberts (2005) and Kamhi (2006) and highlights the interrelatedness and reciprocity between articulation and phonemic awareness training. The multimodal approach used in this study, with its unique visual components, appeared to be more beneficial than traditional articulation therapy in the treatment of speech sound disorders. Both participants learned to manipulate the FONEMZ symbol that corresponded with their target phoneme, while simultaneously learning to produce that phoneme with increased accuracy and improved phonological awareness skills. A.F., who did not demonstrate concomitant receptive and expressive language difficulties, further demonstrated improved literacy skills across a spectrum of subtests designed to measure reading readiness in the area of decoding. The positive results of this study bode well for both participants’ potential acquisition of decoding skills. This is important, because A.F. and J.F. represent two distinct student profiles commonly seen on speech-language pathologist (SLP) caseloads: students having phonological disorders with and without concomitant language disorders. J.F.’s concomitant language and phonological disorders and his slow progress in acquiring phonological awareness skills match the findings of Ehri et al. (2001), which indicate that children with lower language skills make slower progress in phonemic awareness. Ukrainetz, Ross, and Harm (2009) maintain that it is such children who can benefit most from explicit phonological awareness intervention. It appears that a multimodal approach, such as FONEMZ, has the potential to strengthen phonological awareness and set the stage for phonics by providing meaningful contrasts between phonemes in a developing phonological system. Strengthening these links to early literacy will promote successful decoding when reading. This may allow for more time and energy to be focused on reading comprehension for both student types, but particularly for those with other linguistic deficits.
According to the National Center for Education Statistics (2012), up to 60% of children and youth receiving Special Education Services in the United States in 2009–2010 had been diagnosed with specific learning disabilities or speech and language impairments. Continued research is needed relating to practical methodology that professionals can use in the prevention and treatment of language-based reading deficits. This study contributes to the research base in this area. Replication of this study across additional participants, settings, facilitators, research designs, and/or investigators with phonological awareness and pre-literacy probes is necessary to further validate the effectiveness of the FONEMZ approach. Examination of both the FONEMZ and other approaches emphasizing visual symbols and orthography, including efficacy studies comparing them with less visual, but equally phonologically rich approaches (e.g., phonological processes approaches) to speech sound correction, would also be useful.
Footnotes
Appendix A
J.F.’s Pre-and Post-Treatment Scores on the PALS-Pre K.
| Section | Pre-score | Post-score | Range—Early reading success |
|---|---|---|---|
| Upper-Case Recognition | 0 | 1 | 12–21 |
| Lower-Case Recognition | 0 | 1 | 9–17 |
| Letter Sounds | 0 | 0 | 4–8 |
| Beginning Sound Awareness | 0 | 4 | 5–8 |
| Print and Word Awareness | 0 | 0 | 7–9 |
| Rhyme Awareness | 0 | 0 | 5–7 |
| Nursery Rhyme Awareness | 0 | 0 | 6–10 |
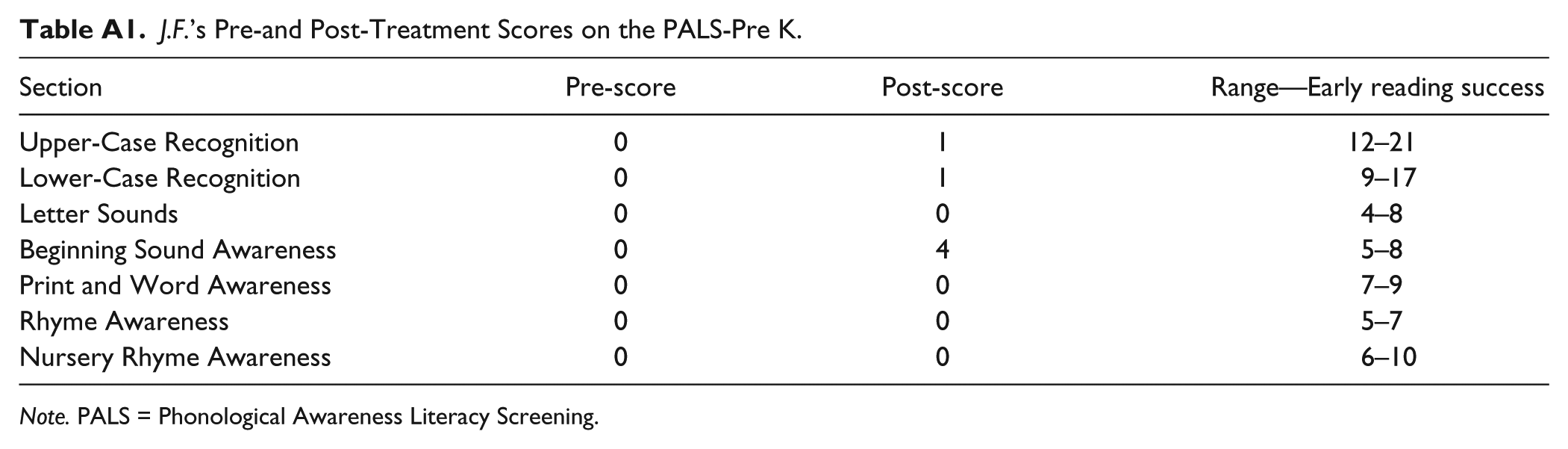
Note. PALS = Phonological Awareness Literacy Screening.
Appendix B
A.F.’s Pre-and Post-Treatment Scores on the PALS-Pre K.
| Section | Pre score | Post score | Range—Early reading success |
|---|---|---|---|
| Upper-Case Recognition | 6 | 23 | 12–21 |
| Lower-Case Recognition | 8 | 20 | 9–17 |
| Letter Sounds | 2 | 3 | 4–8 |
| Beginning Sound Awareness | 5 | 10 | 5–8 |
| Print and Word Awareness | 4 | 7 | 7–9 |
| Rhyme Awareness | 7 | 7 | 5–7 |
| Nursery Rhyme Awareness | 3 | 4 | 6–10 |
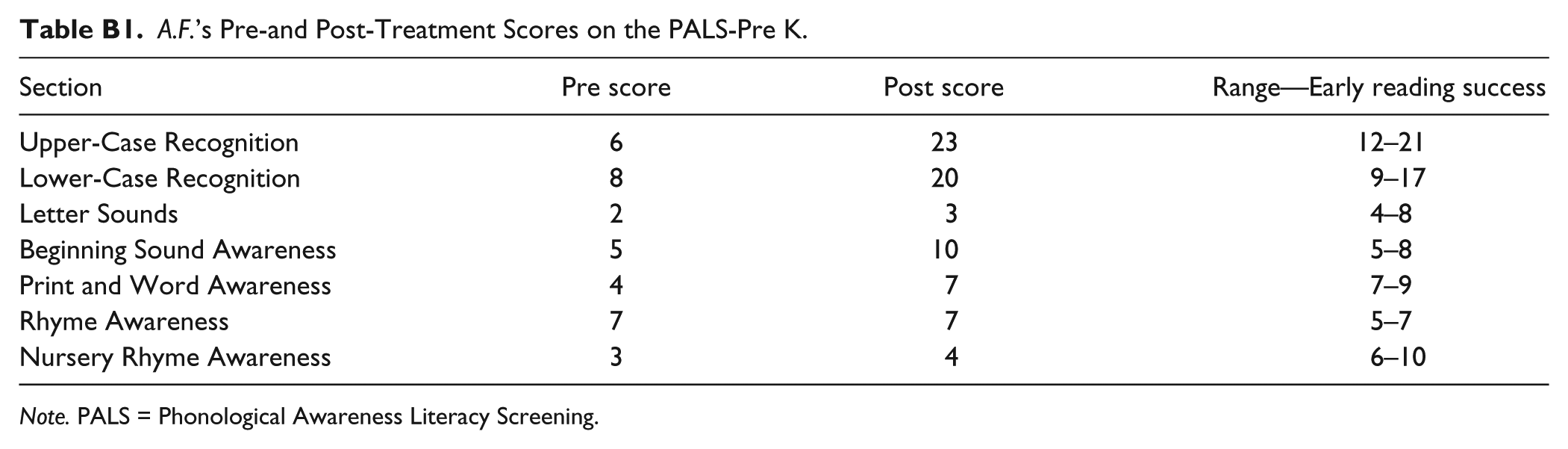
Note. PALS = Phonological Awareness Literacy Screening.
Authors’ Note
This work was accomplished with the cooperation of Laureen O’Hanlon, PhD; Sandy Kaul, MA; Robert Pieretti, PhD; Razi Zarchy, MS; Melisa McCampbell, MS; Kelly Dodge, MS; Lori Nelson, BS; and Susan Guthrie, BS.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sandy Kaul is the developer of the FONEMZ program used as a multimodal approach in this study. Ms. Kaul receives financial compensation from the sale of the program. Dr. Pieretti does not receive financial compensation from the sale of the FONEMZ program. He is a frequent speaker on topics related to language and literacy and has co-authored books on these topics. He does receive financial compensation in the form of book royalties and, occasionally, speaker honoraria.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.