
Abstract
The personality characteristics of the speech-language pathologists (SLPs) may impact their success with each client they see, specifically in stuttering therapy. This initial study explores a general personality profile of SLPs who work in the area of stuttering compared with SLPs who do not. Personality dimensions were measured by the NEO Five-Factor Inventory (NEO-FFI). An occupational questionnaire was also administered. Results from 142 respondents were available for the analysis. Results indicated a significant interaction of group affiliation and patterns of NEO-FFI personality dimensions. SLPs who work with persons who stutter (PWS) were characterized by lower levels of Neuroticism. Lower Neuroticism levels, which are associated with elevated resilience to anxiety, may be a personality trait of SLPs who choose to work with PWS. Possibly, the SLPs’ resilience may facilitate a better therapeutic alliance with stuttering clients. We discuss the importance of the personality dimensions of the SLPs in the SLPs’ career education.
The personality profile of speech–language pathologists (SLPs), and, specifically, their compatibility to the personality profile of their clients, may play an important role in the therapeutic interaction (Werbart, Hägertz, & Ölander, 2018). Particularly, patient–therapist personality matching may play an essential role in the unique and complex specialization of stuttering therapy. Although the research indicates that the SLPs’ personality traits may affect the therapeutic relationship and outcomes, this topic has not been studied yet. Indeed, clinical research on stuttering has focused mainly on the person who stutters (PWS). Special attention has been directed toward evaluating measurement techniques, seeking risk factors of persistency, and suggesting treatment programs (Ajdacic-Gross et al., 2010; Bloodstein & Bernstein-Ratner, 2008). Several studies have attempted to evaluate personality profiles of PWS (Seery, Watkins, Mangelsdorf, & Shigeto, 2007; Treon, Dempster, & Blaesing, 2006), with the purpose of predicting treatment outcome and improving its effectiveness (Ying, Yu, & Baokun, 2003). Iverach et al. (2010) explored the personality characteristics of adults who stutter using the NEO Five-Factor Inventory (NEO-FFI; Costa & McCrae, 1995) and compared them with normative data. Results revealed significant group differences. Specifically, adults who stutter were characterized by significantly higher Neuroticism score, associated with the presence of anxiety, mood swings, and emotional instability. Similar results have been reported by Jafari, Shahbodaghi, Ashayeri, Keyhani, and Baziyar (2014), who investigated personality traits using the same personality inventory in a sample of adults who stutter and a control group, age and gender matched, and found that males who stutter were characterized by high levels of Neuroticism. Taken together, these studies suggest that PWS exhibit higher Neuroticism scores when compared with controls.
SLPs who treat PWS have received less attention, and little is known about personality traits that characterize SLPs who work in the area of stuttering. Mostly, research focused on the career conflicts and difficulties associated with treating PWS. Early research has indicated that many SLPs do not feel comfortable with their ability to diagnose and treat fluency disorders (Yaruss, 1999) ranking stuttering last when asked about the types of speech–language disorders they prefer to treat (St. Louis & Durrenberger, 1993). To the best of our knowledge, the question of what communication disorders do SLPs prefer to manage has not been further studied. More recent texts have focused on clinicians’ discomfort with stuttering, providing several possible explanations for this finding. First, stuttering is considered an enigmatic and complex disorder, whose etiology yet remains unclear (Guitar, 2013). In addition, it is highly variable among and within individuals. These factors may imply a high level of uncertainty about the adequacy of treatment programs for clients who stutter (Tellis, Bressler, & Emerick, 2008; Yaruss, 1999). Second, insufficient clinical training in fluency disorders (e.g., Kelly et al., 1997; Manning & Quesal, 2016; Yaruss, 1999) and low availability of supervision may cause SLPs to feel incapable of treating clients who stutter (Tellis & Tellis, 2003). Yaruss and Quesal (2002) conducted an extensive survey of 159 graduate training programs in fluency disorders accredited by the American Speech-Language-Hearing Association (ASHA), and found that about one-quarter of programs allow students to graduate without coursework in fluency disorders and nearly two-thirds allow students to graduate without clinical practicum experiences in this area. Recently, Manning and DiLollo (2017) addressed the quality of academic and clinical preparation in fluency disorders and posited that “. . . the time devoted to any one disorder area has been reduced, and this is especially true in the area of fluency disorders” (p. 8).
In addition to these factors, as stuttering is a low-incidence clinical population (~1%), there are too few opportunities to treat individuals who stutter (within graduate training programs). Besides the low incidence of stuttering, it is estimated that only a fraction (~10%) of these individuals actually seek out therapy (Plexico, Manning, & DiLollo, 2010). Tellis et al. (2008) performed a survey of 255 school SLPs regarding knowledge of and skill levels with assessing and treating stuttering. The results indicate that, on average, the respondents had only treated 12 children who stuttered throughout their careers and averaged two children who stuttered on their caseloads per year (the average years of experience reported by the respondents was about 16, and the average years of experience working with children who stutter was about 11).
Furthermore, the literature suggests that personality influences career choice and that individuals with certain personality traits are drawn to or better suited to certain health professions or specialization (Bean & Holcombe, 1993; Hanson & Chater, 1983; Holland, 1985; Ozer & Benet-Martinez, 2006). The wide range of specialty areas within speech–language pathology allows for divergent clinical practice activities and relationships and, thus, the expression of different personality characteristics among clinicians. Accordingly, it can be hypothesized that SLPs who choose to treat PWS may be characterized by specific personality characteristics. The literature on personality dimensions of SLPs who work with PWS is scarce. The goal of this study, a first of its kind, was to examine whether a specific constellation of personality dimensions (as measured by the NEO-FFI; Costa & McCrae, 1995) characterizes SLPs who work in the area of stuttering, compared with those who do not. Uncovering such a specific constellation of personality traits may refine our understanding of overt and covert processes that may affect SLPs who treat stuttering.
The Complexity of Stuttering and Stuttering Therapy
Various surveys over the last decades demonstrate that many SLPs prefer treating clients with any other communication disorder than stuttering (e.g., Kelly et al., 1997; St. Louis & Durrenberger, 1993), and are not comfortable assessing and treating PWS (Tellis et al., 2008; Tellis & Tellis, 2003).
One possible explanation for these findings may be the nature of stuttering and stuttering therapy. Stuttering emerges from a complex interaction of many factors (Packman, 2012). It has been considered a multidimensional phenomenon, including overt symptoms (i.e., speech disfluencies, physical concomitants), as well as covert symptoms, for example, anxiety (Menzies, Onslow, & Packman, 1999). Anxiety has been considered one of the most frequent psychological concomitants to stuttering, affecting daily life and coping with stuttering (e.g., Craig, Hancock, Tran, & Craig, 2003; Craig & Tran, 2014; Ezrati-Vinacour & Levin, 2004).
The complexity of stuttering, which includes emotional and social dimensions, creates important implications for clinical practice. Providing stuttering therapy requires both a high level of knowledge and expertise regarding speech-restructuring strategies, and professional tools to recognize and address the underlying psychological aspects related to the experience of stuttering (Yairi & Seery, 2011). Therefore, a recommended therapeutic approach typically combines speech-restructuring strategies and interventions that address the cognitive and emotional aspects of stuttering (e.g., Iverach et al., 2009). In recent years, many stuttering therapists address cognitive and emotional features by employing counseling skills (Boyle, 2015; Ginsberg & Wexler, 2000; Lieberman, 2018) and incorporating elements from cognitive–behavioral therapy (e.g., Menzies et al., 2008) into their treatment methodology. In addition, several researchers have emphasized the importance of establishing a meaningful therapeutic alliance with the client who stutters, which, in turn, may contribute to the success of therapy (Herder, Howard, Nye, & Vanryckeghem, 2006; Manning & DiLollo, 2007).
Within psychotherapy research, the pertinent literature indicates that patient–therapist personality matching plays an essential role in the therapeutic relationship, and may account for therapy outcome (Werbart et al., 2018). However, in the area of stuttering therapy, the contribution of the patient–therapist personality dimensions to the therapeutic relationship and outcomes has not been studied.
The Five-Factor Model: Personality Traits of PWS
The term “personality” describes the complex of characteristics that distinguishes an individual. This term usually refers to a persistent style of thinking, feeling, and behaving that portrays an individual (Costa & McCrae, 1995). One of the most accepted means to evaluate personality differences is the NEO-FFI. This tool is widely used for comprehensive personality assessment (yet it can also be utilized for screening purposes). It is based on the Five-Factor Model (FFM; or the “Big Five”) of personality (Costa & McCrae, 1995; Sleep, Hyatt, Lamkin, Maples-Keller, & Miller, 2017). According to this model, an individual’s personality can be evaluated by five basic dimensions: Neuroticism (N)—the tendency to experience anxiety and negative emotions; Extraversion (E)—the tendency toward positive emotions and sociability; Openness to experience (O)—an appreciation for art and reception of novelty; Agreeableness (A)—a tendency toward cooperation; and Conscientiousness (C)—a bias toward organization and perseverance. This common assessment tool is also referred to as NEO Personality Inventory (NEO PI; Costa & McCrae, 1992b; DeYoung, Carey, Krueger, & Ross, 2016; Helle & Mullins-Sweatt, 2019).
The Neuroticism dimension has been postulated to “represent the individual’s tendency to experience psychological distress” (Costa & McCrae, 1992b, p. 5), with higher levels of Neuroticism reflecting a higher vulnerability to stress, depression, low self-esteem, and anxiety (Beheshti, 2014, Bienvenu et al., 2004). The latter is of special interest in discussing personality dimensions of PWS. The presence of anxiety among PWS has been investigated repeatedly over the years. Recently, a meta-analysis concluded that PWS have substantially elevated levels of trait and social anxiety (Craig & Tran, 2014). Neuroticism is robustly associated with Diagnostic and Statistical Manual of Mental Disorders (DSM) Axis I psychopathology including anxiety and mood disorders (Ormel et al., 2013). A high-level Neuroticism does not necessarily indicate on the existence of a mental disorder and does not constitute a psychopathological disorder by itself, but rather implies on personality characteristics. Accordingly, “high” or “low” levels of this trait are based on statistical rather than clinical criteria. Neuroticism has been previously associated with a predisposition to anxiety, that is, high levels of anxiety-related traits (Griffith et al., 2010, Uliaszek et al., 2009; Uliaszek et al., 2010). Note that the precise nature of the relationship between anxiety and stuttering has not been fully established. Conceivably, the anxiety is a consequence (rather than a cause) of stuttering, resulting from repeated negative experiences associated with stuttering across the lifetime (Craig & Tran, 2014). The elevated anxiety levels are not surprising given the difficulties PWS experience when dealing with the physical symptoms and negative social consequences of stuttering (Craig et al., 2003).
A review of the relevant literature reveals a well-established association between Neuroticism, as measured by the NEO-FFI, and speech fluency disorders (Gawda, 2007). Typically, PWS score significantly higher than controls in Neuroticism items (Bleek, Montag, Faber, & Reuter, 2011, Iverach et al., 2010; Jafari et al., 2014). Bleek et al. (2012) report a strong positive correlation between levels of Neuroticism and adverse impact of stuttering on a person’s life.
As stuttering therapy is a complex process, the personality dimensions of the therapist and their compatibility to those of the client may play an important role in the therapeutic interaction (for a related association in the area of psychotherapy, see Werbart et al., 2018). Presumably, the match (or the relationship) between the personality characteristics of the PWS (their high levels of Neuroticism, in particular) and the SLPs who treat them may positively affect the course of therapy, specifically the SLPs’ ability to cope with the clients’ anxiety (e.g., Wiseman & Tishby, 2014). Possibly, the SLPs’ capability to engage with the PWS’ high anxiety levels may be reflected by the low Neuroticism levels of the SLPs themselves. The personality profiles of therapists in general and SLPs in particular will be discussed in the following sections.
Personality Traits of Therapeutic Professionals
It has been suggested that a person seeks a profession or an occupation that would benefit and satisfy his personal needs (Holland, 1985; Ozer & Benet-Martinez, 2006), and that is in congruence with one’s personality characteristics (Bean & Holcombe, 1993; Hanson & Chater, 1983). Indeed, repeated evidence has suggested that different personality types are associated with different professions or vocational choices (e.g., Kaufman, Pumaccahua, & Holt, 2013; Rubinstein, 2005).
Several studies have explored personality characteristics of individuals in the therapeutic and rehabilitation professions. Eley, Eley, Bertello, and Rogers-Clark (2012) investigated the relationship between personality traits and the reasons for choosing a career in nursing. The authors found that the need and enjoyment of caring for others was the principal reason for entering that profession. Leonard (2015) suggested that the “enjoyment of caring” is a prevalent trait in all helping professionals, including SLPs. This need to care for others in a vocational environment correlates with Holland’s theory of Vocational Personalities in Work Environments (1959, in Holland, 1985) which indicates that those who have personality traits and interests that correspond with a helping profession tend to choose a career falling in Holland’s category of a Supportive Environment (e.g., teachers, counselors, or therapists).
Attempting to describe a typical “occupational personality” using the NEO-FFI is a rather complicated task, as personality is defined by a constellation of traits, and each trait consists of many more specific facets. Nonetheless, the literature suggests that low Neuroticism is associated with emotional stability, calmness, relaxation, and comfortableness, all of which are important traits for therapists. In a related study, Ackerman and Hilsenroth (2003) identified therapist characteristics that were associated with a good therapeutic alliance, for example, flexibility, honesty, respectfulness, trustworthiness, confidence, interest, alertness, friendliness, warmth, and openness; many of these traits are related to low Neuroticism scores (Herder et al., 2006; Manning & DiLollo, 2007). Therefore, it is reasonable to posit that therapeutic professionals are generally characterized by relatively low Neuroticism levels.
Note, however, that in the case of the health professions (e.g., nursing and physical therapy) different specializations in the same profession are associated with different personality characteristics (Cross & Kelly, 1983; Rovezzi-Carroll & Leavitt, 1984). For example, McPhail (2002) found different personality clusters among nurses of four different domains: direct care, administration, teaching, and research. Borges and Savickas (2002) suggested an association between a few personality factors and particular medical specialties, and advised that medical students consider their own personality when choosing a specialty.
SLPs’ Personality Traits
The literature on personality traits of SLPs is relatively limited. Baggs (2013) evaluated the personality of SLP students (using the Keirsey Temperament Sorter II) and reported that the majority of participants showed a Sensing-Judging (SJ) temperament, described as rational, practical, traditional, perceptive to the needs of others, and finding enjoyment in helping others. Recently, Schurr (2018) evaluated a large sample of SLPs across the United States (using an assessment similar to that of the Myers–Briggs Type Indicator) and found that the most common personality types in the sample were as follows:
ESFJ (Extrovert-Sensing-Feeling-Judging)—a personality type characterized as being helpful, warm, and cooperative. ESFJs are described as having multiple interests, a strong reliance on facts, warmth, and sympathy. They are joyful, enjoy being with others, and value unity and agreement (McCaulley & Martin, 1995);
ISFJ (Introvert-Sensing-Feeling-Judging)—characterized as being conscientious, loyal, and dedicated. This personality type is characteristically found to service others and be warm and empathetic. ISFJs are considered to be good listeners, dedicated to work, committed, and hardworking.
Interestingly, Baggs (2013) reported a high variability in personality types among SLP students. Although such a sample of undergraduates differs in many aspects from an SLPs’ sample, a similar variability was found by Craig and Sleight (1990) within a group of SLPs, using the Myers–Briggs Type Indicator. Schurr (2018) who used a similar tool also found a wide range of personality types in each of the possible work settings (health care, education, private practice, tele-practice, and college/university settings), showing variation of personalities in the profession. Leonard, Plexico, and Plumb (2019) examined the relationship between personality and specialty choices within the field of speech–language pathology and found high variability in the scores. The authors concluded that this may indicate that the field of speech–language pathology allows many personality types to succeed within it.
This variability in personality types of SLPs may be related to different specialties within the profession; an SLP typically does not practice in all areas of clinical service delivery, but in areas in which they are competent, based on their education, training, interest, and experience (American Speech-Language-Hearing Association, 2016) and based on their work setting. Therefore, the SLP’s personality may have a role in choosing areas of professional practice. As suggested by Leonard et al. (2019), “we hypothesized that personality could also be used to separate SLP specialty choices.”
Within the specialization of fluency disorders, to the best of our knowledge, no studies have been conducted to evaluate personality profiles of SLPs who work with PWS. With the accumulating evidence of an association between the therapist’s personality and therapy outcomes, it is of clinical importance to explore whether SLPs who work in the area of stuttering are characterized by a specific constellation of personality traits.
This Study
The purpose of this study was to compare the personality dimensions of two groups of SLPs, those who work with PWS (SLP-S) and those who do not work in this area (SLP-NS). Based on the theoretical and empirical literature reviewed above, we expected to find a significant difference between the NEO-FFI profiles of these two groups. Specifically, as previous research has associated low levels of Neuroticism with positive therapeutic relationship, we aimed to examine whether lower Neuroticism levels characterize SLP-S relative to SLP-NS. Besides (low) Neuroticism, the literature does not indicate any other NEO personality dimension that characterizes SLPs as a group, or into specific subgroups. Accordingly, we hypothesized no group differences in other personality dimensions between the two SLP subgroups.
Our sample of participants included 142 Israeli SLPs who work in the field of speech and language disorders. Importantly, in Israel, the training programs in speech–language pathology include academic and clinical education both in audiology, as well as in speech and language pathology (communication disorders). Typically, these programs provide one mandatory course in fluency disorders, followed by a practical workshop. Upon graduating and receiving a clinical certification (by the Ministry of Health), the SLPs choose their place of work, and hence their caseloads. Based on a research published in 2016 by The Administration of Strategic and Economic Planning, Ministry of Health, Israel, and the Israeli Central Bureau of Statistics, about 38% of Israeli SLPs work in the education system (kindergartens and schools in regular and special education). The majority of the other SLPs work in the health system (public, geriatric, and rehabilitation hospitals, mental health institutions, children’s rehabilitation day care centers, and community health services clinics). Clearly, some of the SLPs work in more than one work setting, and most SLPs treat more than a single communication disorder (articulation, voice, language, fluency, etc.). Especially in the health system, the SLPs can (partially) control their caseloads. For example, a clinician who chooses not to engage in a particular disorder (due to his or her personal preferences, experience, or professional knowledge) will not be forced to work with patients with this disorder (patients will be referred to other therapists). In the education system, the SLPs are limited in their ability to control their caseloads. However, generally they provide services in communication and language disorders (rather than fluency disorders; see The Pedagogical Administration, Israeli Ministry of Education).
Method
Participants
After receiving approval from the institutional ethics committee, and obtaining informed consent electronically from all participants, a total of 142 Israeli SLPs participated in this study. To be included in the survey, all participants reported themselves as clinically practicing SLPs who work in the field of speech and language disorders. Fifty-five respondents were assigned to the SLP-S group (about 40%), and 87 participants were assigned to the SLP-NS group (about 60%). Table 1 provides data on years of experience, additional fields of expertise, and participants’ age groups.
SLP Characteristics.
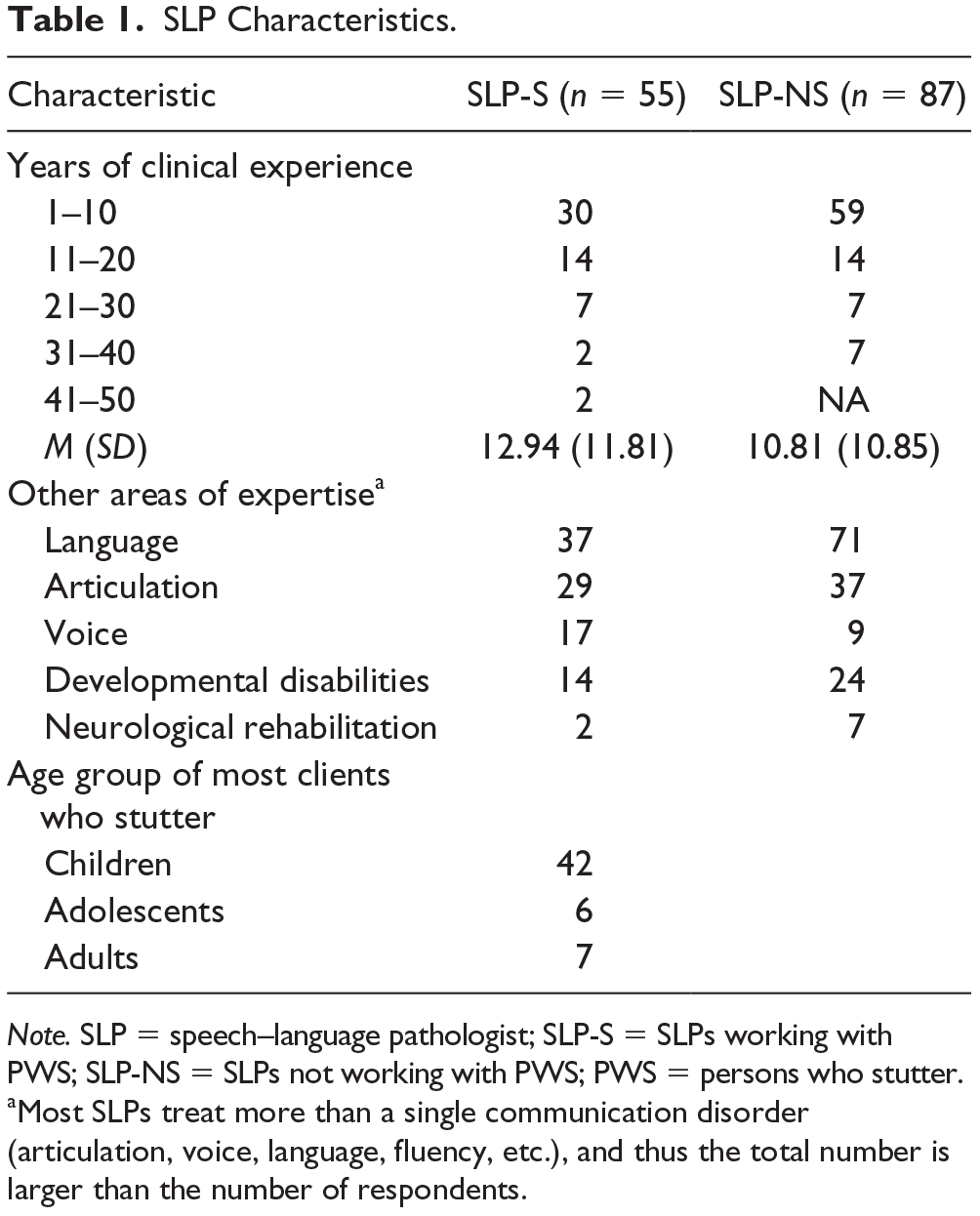
Note. SLP = speech–language pathologist; SLP-S = SLPs working with PWS; SLP-NS = SLPs not working with PWS; PWS = persons who stutter.
Most SLPs treat more than a single communication disorder (articulation, voice, language, fluency, etc.), and thus the total number is larger than the number of respondents.
Data Collection
Participants were recruited by publishing a Call for Participation in national SLP associations via social media (Facebook) and e-mail lists (contact lists of the Israeli Speech, Hearing and Language Association). Participants were informed that the aim of the study was to investigate personality characteristics of SLPs (the comparison between SLP-S and SLP-NS was not mentioned). SLPs who volunteered to participate in the survey entered an online platform and filled in questionnaires anonymously.
Research Tools
All 142 SLPs were surveyed by means of two question-naires.
An occupational (clinical practice) questionnaire
This specially designed ad hoc web questionnaire asked about SLP choice of working with PWS, desire to continue doing so, and satisfaction level from working with these clients. It included questions regarding relevant occupational information (e.g., clinical experience—number of years working as SLP), work setting and clientele, age range of clients, and basic attitudes toward stuttering therapy. Note that we designed a relatively short questionnaire, to improve overall response rate. SLPs who reported working with clients who stutter answered a total of 12 questions, six more than SLPs who answered they do not work with PWS (see Appendix).
Personality dimensions
The NEO-FFI is frequently used for a brief assessment of personality dimensions and is probably the most widely used test based on the FFM of personality (Costa & McCrae, 1992b, 1995); it includes 60 items (statements describing a behavior or a thought), 12 items for each of the five personality dimensions: Neuroticism, Extraversion, Openness, Agreeableness, and Conscientiousness. Responses to each item are rated on a 5-point Likert-type scale ranging from “strongly agree” to “strongly disagree.” Each dimension is scored by summing each of its 12 items. A relatively high test–retest reliability, ranging from .86 to .91 for the five scales (2-week test–retest reliability, Robins, Fraley, Roberts, & Trzesniewski, 2001; 3-month test–retest reliability, McCrae & Costa, 1983; for test–retest reliability for more than 6 years, see Costa & McCrae, 1992a), as well as acceptable to good internal consistency (Cronbach’s alpha ranges from .68 to .85; Sherry, Hewitt, Flett, Lee-Baggley, & Hall, 2007) and validity (in particular, correlation with peer adjective factors ranging from .29 to .43; McCrae & Costa, 2004), were reported. We used the Hebrew version of the NEO-FFI (Rubinstein, 2005).
Data Analysis
Data were analyzed using SPSS statistical software (version 24; IBM Corporation, Armonk, NY). Independent t tests were used to test group (those who practice/do not practice stuttering therapy) differences in clinical experience. A repeated-measures analysis of variance (ANOVA) with group (practice/do not practice stuttering therapy) as a between-subject factor and the five NEO-FFI personality dimensions (Neuroticism, Extraversion, Openness, Agreeableness, and Conscientiousness) as a within-subject factor was conducted. The analysis was conducted twice; with and without clinical experience (number of years working as an SLP) as a covariate. Greenhouse–Geisser corrections were applied as necessary for violations of sphericity, and partial eta squared served as an estimate for effect size of the ANOVA. Post hoc contrast analysis was used to examine interaction effects for NEO-FFI ratings.
Results
Analyzing the clinical practice questionnaire revealed that the great majority (about 90%) of the SLP-S group affiliation reported choosing this specific specialization and wishing to continue to work with PWS. Most of these SLP-S (86%) reported high levels of satisfaction working with PWS (answered positively in response to the question “Do you enjoy treating clients with stuttering?”). A lesser percentage (74%) answered positively to the question “Do you feel you have enough professional knowledge to work in the area of stuttering?” This result is in line with previous reports that some SLPs feel overwhelmed and uncomfortable when treating clients who stutter, and feel incapable of providing such treatment (e.g., Tellis & Tellis, 2003). About 34% of the SLP-NS reported that they would like to work with this population. No significant differences in the number of years of clinical experience were observed between SLP-S and SLP-NS, t(136) = 0.96, p > .05.
Means and standard deviations for the five personality dimensions of the NEO-FFI for the SLPs are presented in Figure 1. Data show that the SLP-S group is characterized by lower Neuroticism scores and higher Extraversion scores relative to the SLP-NS group.

NEO-FFI scores among SLPs who treat stuttering (SLP-S) compared with those who do not (SLP-NS).
A repeated-measures ANOVA indicated a significant interaction between group affiliation and NEO personality dimensions, F(2.89, 405.68) = 4.21, p < .01,
Discussion
Stuttering therapy is a complex process, as it comprises various dimensions, from speech modification to emotional and cognitive change. Many treatment programs for PWS are designed to teach the client specific skills or behaviors that lead to improved oral communication. At the same time, addressing the social and psychological difficulties of PWS, to increase participation in social activities and improve quality of life, is an additional necessary aspect of treatment. SLPs who treat PWS frequently need to provide a safe, supportive environment for their clients, who are often characterized by high levels of either social or speaking-related anxiety (Iverach et al., 2010).
Given the special features of stuttering therapy and the unique personality characteristics of PWS (i.e., high levels of Neuroticism, as measured by the NEO-FFI; Gawda, 2007; Iverach et al., 2010; Jafari et al., 2014), this study examined whether SLP-S are characterized by a different constellation of personality dimensions than SLP-NS. Specifically, we aimed to find out whether the NEO-FFI personality dimension of Neuroticism would distinguish between the two SLP subgroups; in accordance with the literature, we expected SLP-S to score lower on Neuroticism compared with SLP-NS.
Our findings revealed a significant interaction between group affiliation and Neuroticism scores. Post hoc analysis indicated that SLP-S are characterized by a personality constellation that includes lower Neuroticism scores compared with SLP-NS. The data also indicated that SLP-S are characterized by higher Extraversion scores relative to SLP-NS, though this effect was only marginally significant.
Personality Dimensions of SLPs
Several studies have identified specific personality characteristics among the therapeutic and rehabilitation professions (Eley et al., 2012; Leonard, 2015). Yet, no study to date has examined SLPs’ personality characteristics in the context of stuttering therapy. The current results indicate that the subgroup of SLP-S (about 40% of the participants) was characterized by lower Neuroticism scores relative to the SLP-NS group. The interaction of group and Extraversion was marginally significant.
Neuroticism
Relatively low Neuroticism may be an important characteristic of SLP-S. Low Neuroticism has been associated with more emotional stability, calmness, and resilience to anxiety and depression (DeNeve & Cooper, 1998). In this study, the subgroup of SLP-S who were characterized by lower Neuroticism may be more able to mitigate the high anxiety levels usually exhibited by PWS, relative to the subgroup of SLP-NS.
Neuroticism levels may also be related to the therapeutic/working alliance, which was previously acknowledged as an important factor in stuttering therapy (Herder et al., 2006; Manning & DiLollo, 2007). In an extensive literature review that examined therapist personal attributes that negatively influence the therapeutic alliance, Ackerman and Hilsenroth (2001) found that therapist tenseness is related to lower alliance with the patients. This conclusion was supported by other research findings indicating that lower levels of Neuroticism (i.e., less tenseness) among psychotherapy trainees were associated with higher ratings on a measure of “working alliance” (made by the trainees; Chapman, Talbot, Tatman, & Britton, 2009). Thus, it is possible that SLPs with low Neuroticism are more confident and competent in their ability to establish, and therefore perceive more positively, the working alliance with their clients. Further studies may directly evaluate the association between Neuroticism and the therapeutic/working alliance of SLPs and their clients. Note, in this study, that the SLPs’ sample was unique in that they could choose their clientele while the situation is typically different (as many SLPs work with those on their caseload). Future studies may assess the personality traits and the therapeutic alliance within the latter group.
Extraversion
In this study, the SLP-S group was characterized by higher Extraversion scores relative to the SLP-NS group (this difference was marginally significant). Extraversion is characterized by affiliation (i.e., enjoying close interpersonal bonds, being warm and affectionate) and agency (i.e., being socially dominant, enjoying leadership roles; Depue & Collins, 1999), as well as the tendency toward sociability. Previous studies have indicated that Extraversion is negatively correlated with anxiety (Zugliani, Martin-Santos, Nardi, & Freire, 2017); as such, it is reasonable to posit that SLPs with high Extraversion levels would also feel more comfortable in treating PWS who, as previously discussed, tend to exhibit high levels of anxiety. This greater comfort or compatibility may result in a higher inclination to work in the area of stuttering.
Caveats and Future Research
This study was an initial but preliminary exploration of this topic. As such, it has several limitations. First, in spite of the frequent use of the NEO for clinical and research purposes, some authors have criticized it for not controlling for social desirability bias. Widiger (1992) argued that test developers cannot assume participants will be honest, especially in settings where it benefits respondents to present themselves in a better light (e.g., personnel settings). However, because in this study an Internet anonymous questionnaire was used and the respondents were unaware of the study goals, we may assume that their answers were sincere. Note that the possible effects of social desirability would have been observed in both groups, whereas our findings indicate group differences. Hence, we assume that the current findings cannot be explained solely by social desirability.
Second, the results of this study support the possibility that the SLP-S group is characterized by low Neuroticism and possibly more suited to work with PWS. However, the study was not designed to evaluate potential causes for this finding. Indeed, the group differences may stem from several other factors. For example, as about half of our participants reported at least 10 years of clinical experience, we cannot rule out the possibility that their low Neuroticism reflects the impact of working with PWS. Namely, the low Neuroticism levels are the result of their adaptation to the continuous exposure of working with clients that are characterized by high levels of anxiety. Alternatively, as suggested by an anonymous reviewer, perhaps the fact that they have more years of clinical experience leads to greater therapeutic competence overall and to increased success with their clients. As these experienced SLPs master the interpersonal qualities inherent in stuttering therapy, they cope better with its challenges. Importantly, the findings of this study, that is, the association between SLPs’ personality profiles and their career choices, are limited in referring directly the question of causality. Future studies should address this issue.
Another limitation of the study concerns the fact that all of the participants are Israeli SLPs, which may affect how work settings are selected. As noted above, the field of speech–language pathology in Israel is different than that in Europe and the United States in several ways, including the training programs (academic coursework and clinical preparation), the type of workplaces, and the degree of control on caseload. Further studies may assess personality profiles of SLPs in other countries.
In addition, some limitations relate to the occupational (clinical practice) questionnaire used, which did not include information regarding the place of employment for the respondents (work setting), the degree to which they control their caseloads, and the age of caseload. Based on a research conducted by the Israeli Ministry of Health (The Administration of Strategic and Economic Planning, Ministry of Health, Israel, and the Israeli Central Bureau of Statistics, 2016), and assuming that the sample of SLPs in this study was representative, we can estimate that about 40% work in the education system, and the remaining respondents work in the health system. In most of these clinics (public as well as private), the SLP can control the caseload and choose the patients (pediatric vs. adult) and the type of disorders to treat. Future studies may directly assess these occupational issues, as well as the age of the caseload that the SLP most often treat, and the estimated success by client’s age. It may be also interesting to ask the SLPs if there are certain types of clients they do best with (and why) and to assess types of client problem areas (by the etiology, impacted behaviors, or the degree and type of support clients require from their clinician).
Finally, we note that the results were not analyzed for gender differences (we did not obtain SLP gender in the questionnaire). As the field of speech–language therapy is female dominated (Bergey, 2019), we assume that the proportion of males within the sample may not have been large enough to impact the results. In addition, the results were not analyzed for age main effects or interaction. Further studies may address this issue.
Conclusions and Applied Implications
This study revealed preliminary insights into the personality dimensions of two groups of SLPs, those who treat (SLP-S) and those who do not treat (SLP-NS) stuttering. The major result indicated an interaction between group affiliation and one NEO-FFI personality dimension—Neuroticism. A significantly lower level of Neuroticism was found in the SLP-S group. Presumably, SLPs who work with PWS are frequently exposed to high levels of clients’ anxiety and, as a group, may be characterized with higher resilience to anxiety, as expressed by lower Neuroticism scores. In addition, a subthreshold significant interaction of group affiliation and Extraversion was observed.
The current results provide preliminary insights regarding the personality traits of SLPs, and in particular those who work with PWS. Advancing the conceptualization of the relationships between SLP-S and their clients may have implications for clinical training, improving therapy outcomes.
Footnotes
Appendix
Acknowledgements
The authors would like to thank Shiran Swery and Ester Fainsod for collecting data for this study. They would also like to acknowledge the thorough editorial review provided by Shira Chana Bienstock.
Authors’ Note
Dr. Debora Freud is currently a post-doctoral fellow at the Department of Communication Disorders, the Stanley Steyer School of Health Professions, Sackler Faculty of Medicine, Tel Aviv University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.