
Abstract
Objective:
Telehealth can increase health care utilization for substance use disorder (SUD) and mental health (MH) services, particularly for underserved populations. We examined shifts to telehealth for SUD and MH services during the COVID-19 public health emergency and whether they occurred similarly by race, ethnicity, and population density.
Methods:
We used data from the 2021 to 2022 National Survey on Drug Use and Health, focusing on adults with an SUD and/or MH condition in the past year. Estimated prevalence of SUD and MH appointments shifting from in-person to telehealth and used adjusted logistic regression models to examine differences by race, ethnicity, and population density. Sample sizes ranged from 2,440 to 9,695 (∼11–42 million weighted), depending on condition and outcome.
Results:
Approximately 26% of adults with an SUD reported their SUD appointments shifted to telehealth, whereas 66% of adults with an MH condition reported their MH appointments shifted to telehealth. Black (59%) and Latinx (61%) adults with an MH condition were significantly less likely to report appointment shifts to telehealth than White adults (69%, p < 0.01 for both). Individuals in less populated areas were significantly less likely to report their SUD and MH appointments shifted to telehealth, compared with those in highly populated areas.
Conclusion:
Shifts to telehealth were less common for SUD than MH appointments. Rates differed by race and ethnicity. Telehealth was underutilized by those in less populated areas. Research to identify barriers for telehealth services and strategies to ensure telehealth equity in the present day are needed.
Introduction
Only about 12% of adults with a substance use disorder (SUD) and 52% of adults with a mental health (MH) condition receive treatment. 1 These gaps in care are even larger among Black and Latinx individuals and those living in rural areas throughout the United States.2,3
Telehealth can increase health care utilization for MH and SUD by addressing challenges related to travel, transportation barriers, childcare costs, and stigma.4–7 Telehealth is particularly helpful to people who are low income, living in rural areas, and members of racial and ethnic groups that are more likely to experience challenges accessing care. Yet, it has also proven to exacerbate preexisting inequities since these populations are also less likely to have access to reliable internet and technology.8,9
The COVID-19 pandemic led to fast policy changes and uptake of telehealth. Examining shifts to telehealth for MH and SUD services during the COVID-19 public health emergency (PHE) provides a unique opportunity to analyze service utilization patterns and identify inequities in use. Although the use of telehealth had been encouraged, prior to the COVID-19 PHE, telehealth use had been limited. In 2016, only 29% of psychiatrists reported working in practices that used telehealth services with patients. 10 Several factors had been identified as barriers for the provision of telehealth, including lower reimbursement, limits on types of services allowed for telehealth, costs associated with implementation, limited training, and concerns about patient privacy protection and confidentiality and related regulations.11–14 The COVID-19 pandemic led to a sharp increase in the provision and use of telehealth for MH and SUD outpatient treatment.15–17 States, health plans, and federal agencies quickly made temporary changes to regulatory requirements to increase telehealth uptake during the PHE to help maintain continuation of treatment, including easing restrictions on platforms allowed for services and increased reimbursement for telehealth services.2,12,15 Temporary provisions were extended past the end of the COVID-19 PHE, and many have become permanent. Multiple studies have cited the continued high patient satisfaction rates in the use of telehealth past the COVID-19 PHE given the low associated medical, transportation, and wage costs compared with in-person visits.18–20 Examining how common shifts to telehealth occurred during that specific time period, and for whom these shifts occurred, can identify areas where additional support is needed for accessing telehealth services by people living with MH and substance use conditions today.
Social isolation during the COVID-19 PHE exacerbated underlying MH and SUD conditions, leading to an increase in demand for health services.21–23 Yet, research suggests that the transition to telehealth for MH and SUD care may not have occurred equitably. 24 Some studies found that telehealth use for MH was lower for Black individuals and for those living in rural areas compared with White individuals and individuals living in urban areas.24,25
Yet, several gaps remain. Most studies on telehealth use for SUD and MH did not use representative samples and instead focused on limited geographic areas or on specific populations (e.g., veterans). Furthermore, studies examining the use of telehealth for SUD, and those focusing on issues of equity specifically, tend to be limited to opioid use disorder (OUD).
Using a nationally representative community sample, the objectives of this study were to (1) estimate the prevalence of SUD and MH appointment shifts from in-person to telehealth due to COVID-19 among adults with these conditions and (2) examine differences in shifts to telehealth for MH and SUD appointments by race, ethnicity, and population density. Analyzing these shifts during a time when telehealth access was expanded quickly provides a unique opportunity to help inform telehealth expansion efforts, especially for underserved populations accessing SUD and MH services.
Methods
DATA SOURCE
We used publicly available data from the 2021 and 2022 National Survey on Drug Use and Health (NSDUH). The NSDUH is a cross-sectional, nationally representative survey conducted annually by the Substance Abuse and Mental Health Services Administration (SAMHSA). The NSDUH collects information on substance use and MH, as well as the utilization of SUD and MH services among the U.S. noninstitutionalized population aged 12 or older. 26 More detailed descriptions of the NSDUH are available elsewhere.27,28
SAMPLE
We focused our analyses on adults aged 18 and older who had an SUD and/or MH condition in the past year. We classified adults as having an SUD condition if they met the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) criteria in the past year and having an MH condition if they had a severe or moderate mental illness in the past year as determined using an NSDUH-derived predictive model aligned with DSM-5 criteria.29,30
OUTCOMES
Our primary outcomes of interest were the prevalence of SUD and MH appointments that were moved to telehealth due to COVID-19. NSDUH respondents were asked “Because of the COVID-19 pandemic in the U.S., did you experience any of the following in your access to substance use treatment?”, followed by a series of questions, including “Appointments moved from in-person to telehealth?”. Similarly, respondents were asked “Because of the COVID-19 pandemic in the U.S., did you experience any of the following in your access to mental health treatment?”, followed by “Appointments moved from in-person to telehealth?”. Participants could respond “Yes,” “No,” or “Not Applicable” to each question. Participants who responded “Not Applicable” were excluded from the analyses.
INDEPENDENT VARIABLES
Our main independent variables were race and ethnicity (as one variable) and population density.
RACE AND ETHNICITY
The NSDUH first asks participants if they are of Hispanic, Latino, or Spanish origin or descent. Then, it asks individuals to identify which group(s) describes them among the following: American Indian or Alaska Native, Asian, Black or African American, Native Hawaiian or Other Pacific Islander, and/or White. Participants could choose more than one group. In the publicly available dataset, responses to the two questions were recoded into the following categories: non-Hispanic White, non-Hispanic Black/African American, non-Hispanic Native American/Alaska Native, non-Hispanic Native Hawaiian/Other Pacific Islander, non-Hispanic Asian, non-Hispanic more than one race, and Hispanic. Participants who indicated they were of Hispanic, Latino, or Spanish origin or descent were categorized as Hispanic (from here on Latinx) regardless of the response to the second question. Due to small sample sizes, we combined Native American/Alaska Native and Native Hawaiian/Other Pacific Islander (each <0.9% of adults in each of the samples) into one group.
POPULATION DENSITY
The NSDUH provides three levels of population density of participants’ residence using Core Based Statistical Area (CBSA) classifications: 30 CBSA with ≥1 million persons, CBSA with <1 million persons, and non-CBSA (rural).
COVARIATES
Covariates included self-reported health status, age group, sex, and marital status. We also used indicator variables for the following SUDs as covariates: past year alcohol use disorder, OUD, and stimulant use disorder (all based on DSM-5 criteria).
ANALYSIS
All analyses were conducted using R version 4.4.0. We conducted our analyses separately for four samples: (a) adults who had an SUD condition in the past year, with outcome data for SUD appointments shifting to telehealth (i.e., they did not respond as “not applicable”) (Sample 1, N = 7,842, excluded 11,492 responding “not applicable”); (b) adults who had a moderate or severe MH condition with outcome data for MH appointments shifting to telehealth (i.e., they did not respond as “not applicable”) (Sample 2, N = 9,695, excluded 4,726 responding “not applicable”); (c) adults with co-occurring SUD and MH conditions with SUD outcome data (Sample 3, N = 2,440, excluded 3,656 responding “not applicable”); and (d) adults with co-occurring SUD and MH conditions who had MH outcome data (Sample 4, N = 4,207, excluded 1,889 responding “not applicable”). We estimated the prevalence of shifts to telehealth using survey weights to account for the complex survey sampling design and to make nationally representative estimates. We then used weighted logistic regression models predicting that appointments were moved to telehealth including our key independent variables and covariates as predictors. Statistical significance was assessed at p < 0.05. We report predictive probabilities generated using the predictive margins method.
Results
DESCRIPTIVE STATISTICS
Table 1 displays the characteristics of the four study samples. Across all samples, most respondents were White (60.8–68.1%), followed by Latinx (14.1–18.2%) and Black (9.4–14.1%). The greatest proportion of respondents lived in CBSAs with 1+ million people (47.7–50.4%). Less than 8% of respondents in any sample lived in a rural area. Among adults with an SUD, respondents were predominantly male (60.1%), whereas among adults with an MH condition, respondents were predominantly female (63.0%). Across all samples, most respondents indicated that they had excellent, very good, or good health (63.7–76.4%) as opposed to fair or poor health.
Characteristics of Analytic Samples
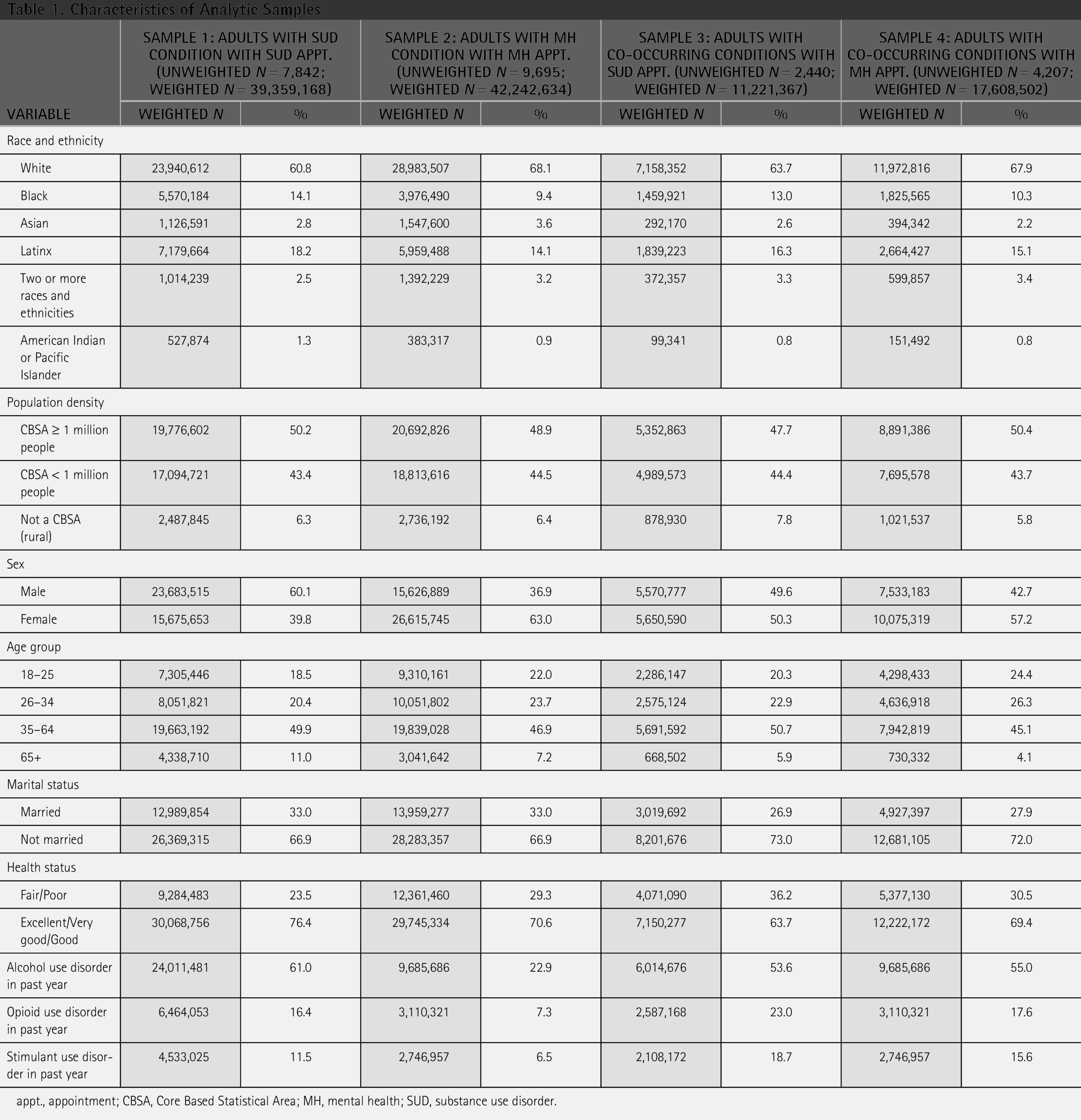
appt., appointment; CBSA, Core Based Statistical Area; MH, mental health; SUD, substance use disorder.
SHIFTS OF SUD AND MH APPOINTMENTS FROM IN-PERSON TO TELEHEALTH (UNADJUSTED RATES)
Table 2 displays the unadjusted proportions of adults who reported having an SUD or MH appointment shift to telehealth. About a quarter (26.0%) of adults with an SUD condition in the past year reported that their SUD appointments were shifted to telehealth, whereas about two-thirds of adults with a moderate or severe MH condition reported that their MH appointments were moved to telehealth (66.2%). Among adults with co-occurring conditions, 40.6% reported that their SUD appointment was moved to telehealth, and 66.7% reported that their MH appointment was moved to telehealth.
Adults Reporting MH and SUD Appointments Moved to Telehealth Due to the COVID-19 Pandemic (Weighted Proportions)
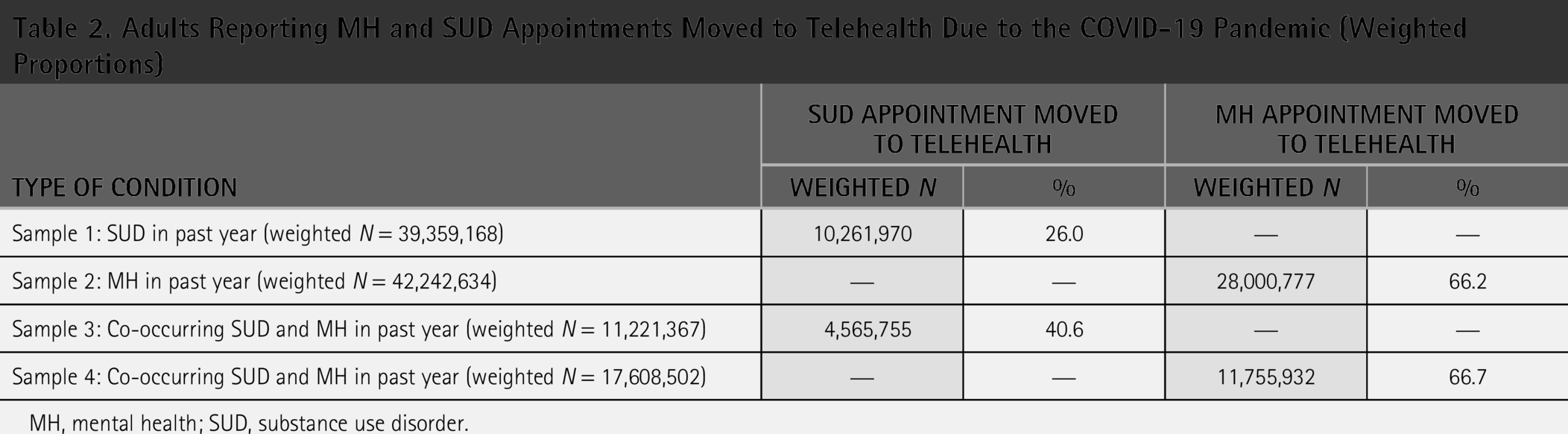
MH, mental health; SUD, substance use disorder.
MODEL RESULTS
Fig. 1 displays the estimated proportion of adults who had their SUD or MH appointments moved to telehealth by race and ethnicity. We did not find significant differences in the prevalence of SUD appointments shifting to telehealth by race and ethnicity among adults with an SUD in the last year or among adults with co-occurring disorders. Among adults with an MH condition in the past year, Black (58%, p < 0.01) and Latinx (60%, p < 0.01) individuals were significantly less likely to report MH appointment shifts to telehealth than White individuals (68%). Among adults with co-occurring conditions, Black individuals (52%, p < 0.01) were also significantly less likely to report MH appointments, shifting to telehealth than White individuals (68%).
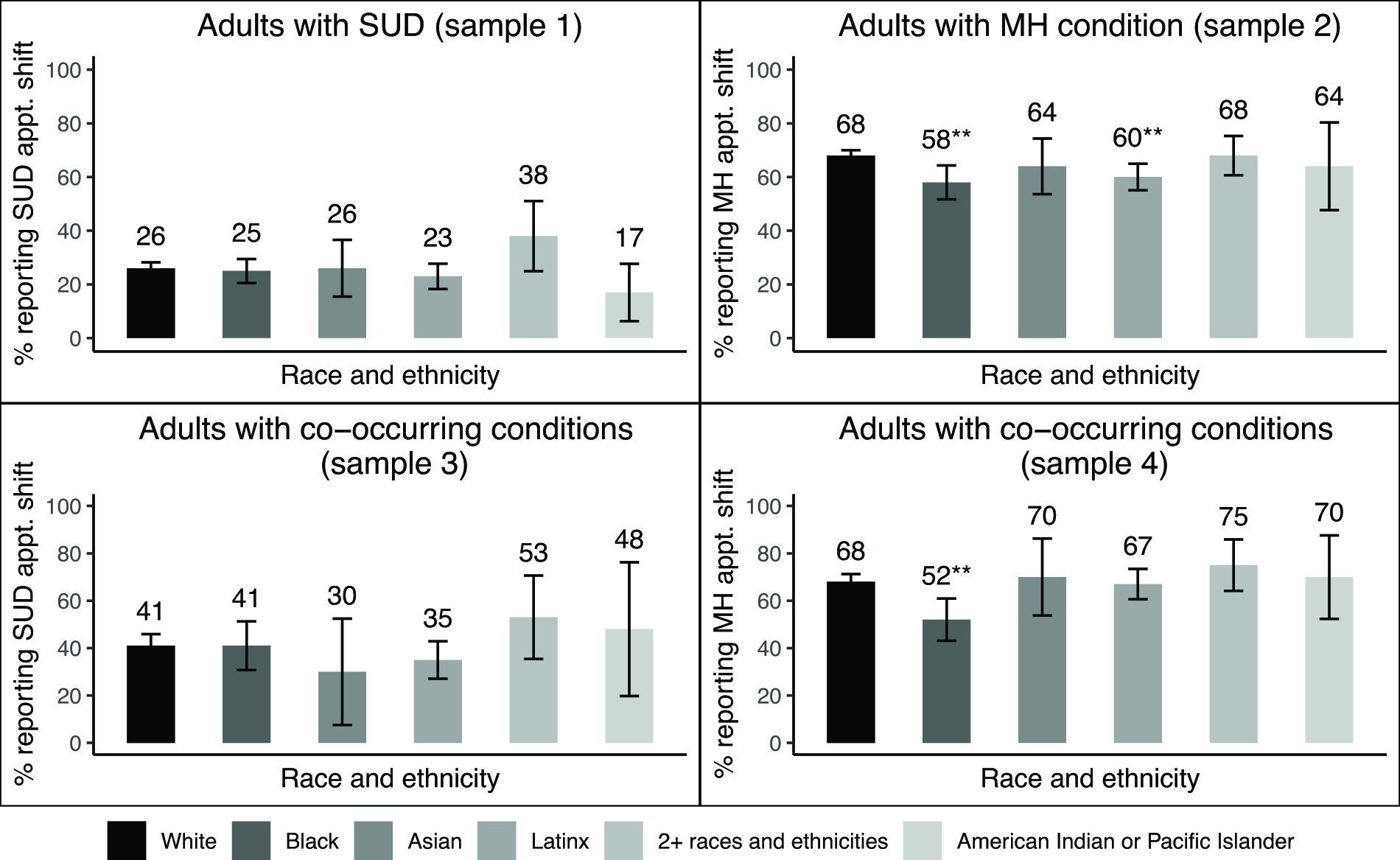
Estimated proportion of adults reporting their SUD or MH appointments moved to telehealth due to COVID-19, by race and ethnicity. Estimates are derived from logistic regression models with race and ethnicity, adjusting for population density, sex, age group, marital status, health status, and past-year alcohol use disorder, opioid use disorder, and stimulant use disorder. *p < 0.05, **p < 0.01 for differences in estimate with that of White adults.
Fig. 2 displays the estimated proportion of adults who had their SUD or MH appointment moved to telehealth by population density. Among adults with an SUD condition in the past year, individuals living in CBSAs with <1 million people (23%, p < 0.05) were significantly less likely to report SUD appointment shifts to telehealth than individuals living in CBSAs with 1+ million people (28%). Among adults with an MH condition in the past year, individuals living in CBSAs with <1 million people (62%, p < 0.01) and individuals who lived in a rural area (53%, p < 0.001) were significantly less likely to report MH appointment shifts to telehealth than individuals living in CBSAs with 1+ million people (70%). Likewise, among adults with co-occurring conditions, both individuals living in CBSAs with <1 million people (62%, p < 0.01) and individuals who did not live in a CBSA (51%, p = 0.01) were significantly less likely to report MH appointment shifts to telehealth than individuals living in CBSAs with 1+ million people (71%). We did not find any significant differences in the prevalence of SUD appointments shifted to telehealth by population density among adults with co-occurring conditions. Full models can be found in the Supplementary Appendix.
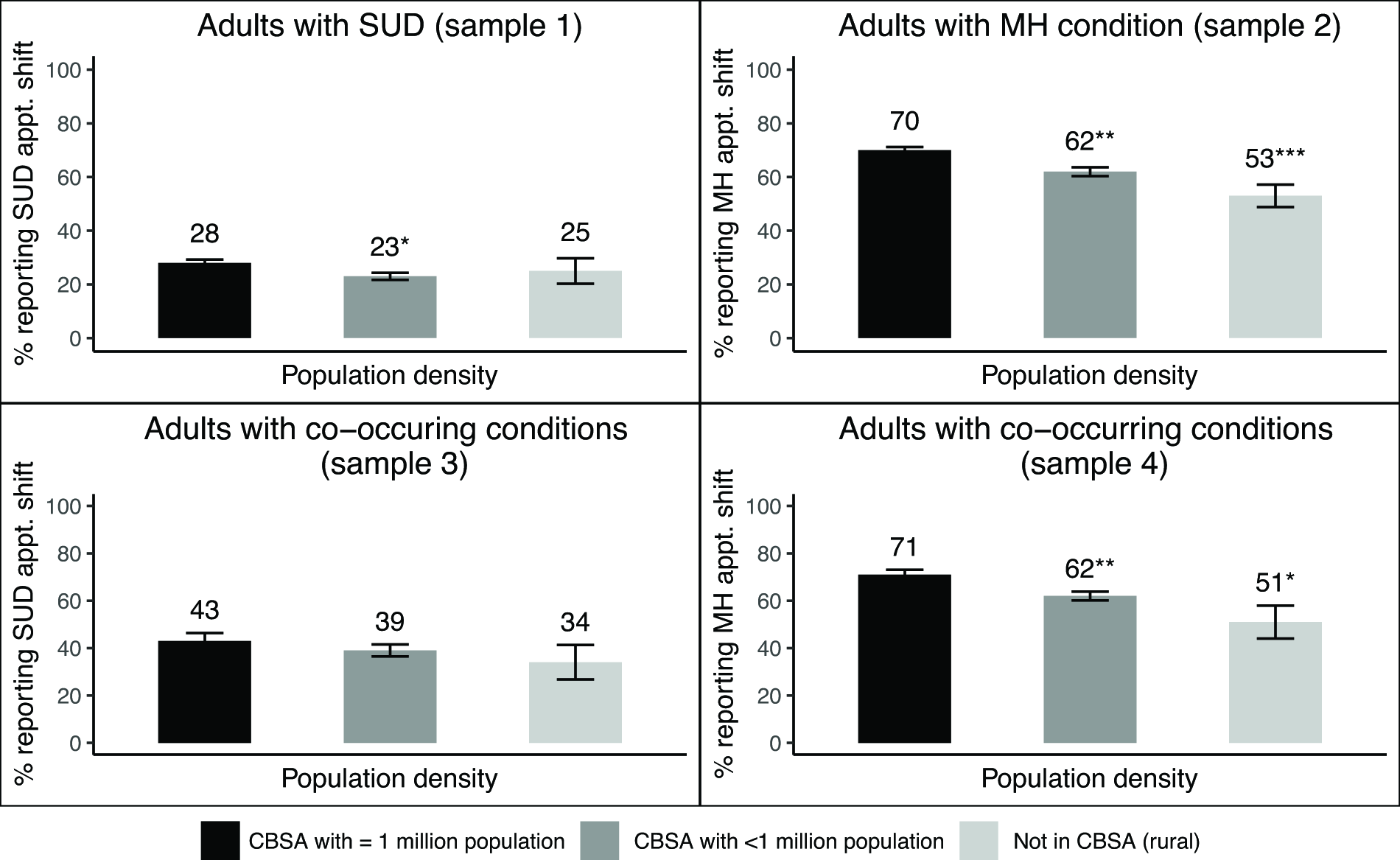
Estimated proportion of adults reporting their SUD or MH appointments moved to telehealth due to COVID-19, by population density. Estimates are derived from logistic regression models with population density, adjusting for race and ethnicity, sex, age group, marital status, health status, and past-year alcohol use disorder, opioid use disorder, and stimulant use disorder. *p < 0.05, **p < 0.01, ***p < 0.001 for differences in estimate with that of CBSA’s with >1 million population.
Discussion
Roughly one in four adults with an SUD reported shifts in their SUD appointments to telehealth. Shifts to telehealth were more common for MH appointments, with about two-thirds of adults with an MH condition reporting shifts to telehealth. Black and Latinx adults, and those living in less populated areas, were less likely to report MH appointment shifts. Patterns by race and ethnicity and population density were generally similar for those with co-occurring conditions.
Our findings are consistent with other studies that have also found lower rates of telehealth use for SUD services. Data from a large private health plan from 2010 to 2017 showed that although telehealth use for MH and SUD services increased substantially during the PHE, telehealth use for SUD accounted for only 2.6% of all telemedicine use compared with 34.5% for MH. 31 Similarly, a national study that analyzed adoption of telehealth by SUD treatment facilities from 2016 to 2019 found that although adoption of telehealth increased during the study period, less than 20% of all facilities used telehealth for SUD services. 32 Consistency in findings across multiple studies can be attributed to the many challenges faced with servicing individuals with SUD through telehealth. As opposed to MH services, SUD services often require access to daily medication for OUD and serve a population who is more likely to lack consistent access to technology, creating a new set of disparities. 33
Very little research exists on racial and ethnic differences in telehealth utilization, particularly for SUD and MH. A retrospective study analyzing telehealth visits for any health-related services among privately insured patients from March through December 2019 showed significantly lower percentage of monthly telehealth visits for Latinx patients compared with non-Latinx White patients. 34 Although some early pandemic research suggested that there were no significant racial and ethnic differences in telehealth use for MH and SUD, more recent studies have highlighted disparities for Black and Latinx individuals for both MH and SUD telehealth utilization.17,21,25,35 A cross-sectional study that examined racial and ethnic disparities in telehealth counseling among Medicaid-insured patients for SUD in a clinic in New York found that Black and Latinx patients used significantly less services than their non-Latinx White counterparts, even after adjusting for confounding factors, suggesting potential factors for inequities in use of telehealth. 36 In addition, a cohort study analyzing telehealth service expansion from 2019 to 2022 within different states found that the percentage of Black residents in a county was inversely associated with telehealth availability. 21 These findings suggest inequities in access to telehealth among underserved populations.
Research also varies regarding differences in telehealth use by population density and rurality. Higher rates of telehealth use were more commonly seen in rural areas as compared with urban areas even prior to the COVID-19 PHE. 37 Despite the belief that these trends would continue through the COVID-19 PHE and that telehealth would help expand access in rural regions, newer studies suggest that telehealth use increased more substantially in urban areas during that time.38–40 For example, a study analyzing telehealth use for MH among veterans between 2019 and 2020 found higher rates of telehealth use among rural patients prepandemic, yet higher rates of telehealth use among urban patients during the COVID-19 PHE. 39 The geographic variation in telehealth readiness seems to suggest that rural areas were not properly equipped to provide telehealth services during this time and might continue to need infrastructure support. At present, the Centers for Medicare and Medicaid published their Calendar Year 2026 Physician Fee Schedule Final Rule that includes the removal of the distinction between provisional and permanent telehealth services—making all telehealth services permanent. 41 The continued current use and permanent adoption of telehealth by federal agencies emphasizes the need for research on barriers experienced by rural populations and best practices for accessing telehealth services for MH and SUD.
It is important to note that the NSDUH did not capture reasons for why an SUD and/or MH appointment shift may have occurred. It is not clear whether the differences we found by race and ethnicity and by population density were due to patient preferences or due to inequities in the availability of or access to telehealth. Given that telehealth was more of a need rather than a preference during the COVID-19 PHE, our findings suggest that these differences highlight inequities.
Studies analyzing the shifts to telehealth during the COVID-19 PHE discovered that appointments not shifted to telehealth were more likely to result in missed appointments, which could translate into a variety of unaddressed health risks for the patient. 42 As telehealth for behavioral health care services continues to evolve and becomes permanent,41,43 it is imperative to consider how its use can be implemented equitably. Studies have shown that despite clinician reservations regarding patient rapport-building through telehealth, patients generally hold a positive view of telehealth utilization for SUD and MH treatment due to accessibility, convenience, and comfort.44,45 However, for underserved communities, documented barriers to equitable adoption of telehealth treatment include concerns with patient privacy and confidentiality, lack of technological support, and lack of culturally competent care.34,46–48 The implementation of culturally competent care for telehealth services is essential to cater to the diverse needs of different populations as it ensures more flexible scheduling and a more diverse network of local health care, psychological, social, and spiritual support for racial and ethnic minorities. 48 For those who live in rural communities, telehealth can help protect the privacy of patients by connecting them to skilled practitioners in other physical locations. 49
Limitations
This study has several limitations. First, the study relied on self-report which is subject to recall and social desirability bias, particularly when reporting substance use. 50 The NSDUH attempts to increase the accuracy of self-reported data by utilizing self-administration of sensitive questions when possible and continuous reminders of confidentiality and anonymity in data results. 27 Second, the questions used to assess shifts to telehealth were asked of all participants, without first asking whether they had had appointments for these conditions. We addressed this limitation by restricting the samples to those meeting the criteria for SUDs and/or a moderate or severe MH condition in the past year and excluding those who said the question did not apply to them. Still, our prevalence estimates may have been subject to measurement error. Third, the study’s cross-sectional nature did not follow participants to assess the reasons for not shifting to telehealth. Yet, this specific point in time offers a unique opportunity to analyze the impact of shifts to telehealth on various populations following the increase in access.
Conclusions
Our analysis of a nationally representative survey found that shifts to telehealth for SUD services did not occur as frequently as they did for MH services and that telehealth treatment uptake for MH conditions was less common for groups that were already underserved and disproportionately affected by COVID-19. As telehealth has addressed several of the barriers to care experienced by underserved communities and COVID-19 era policies have now become permanent, it is imperative that it be an option that can be offered to all. Research should seek to understand patient, provider, and policy factors associated with lower uptake of telehealth of SUD appointments and decipher strategies needed to ensure equity among underserved populations today.
Highlights
Shifts to telehealth due to COVID-19 were more common for mental health than for SUD services Black and Latinx adults were less likely to have mental health appointments moved to telehealth Shifts to telehealth were less common among people living in less populated areas
Authors’ Contributions
A.D.B.: Conceptualization, data curation, and writing—original draft; C.H.G.: Methodology and formal analysis; M.S.: Writing—review and editing; and A.A.: Methodology and writing—review and editing.
Data Availability
This study used publicly available data from the 2021 and 2022 NSDUH. The datasets are available on the SAMHSA website, https://www.samhsa.gov/data/data-we-collect/nsduh-national-survey-drug-use-and-health/datafiles.
Footnotes
Acknowledgments
The authors would like to thank Yuxin Zhao and Chelsey DuBois for their thoughtful feedback on an earlier version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
The views expressed in this article are those of the authors and not those of Booz Allen Hamilton or Boston University. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.