
Abstract
This case study presents the treatment of a 23-year-old single White male with a specific phobia of swallowing and choking on pills. He presented for treatment as part of a larger treatment study for specific phobia and met criteria for a specific phobia, other type (swallowing pills), and social phobia. Treatment of the specific phobia involved One-Session Treatment and was conducted per Zlomke and Davis and Davis, Ollendick, and Öst. A posttreatment assessment 3 weeks after treatment and an 8-week follow-up assessment revealed significant improvements. At both assessments following treatment, clinician severity ratings on the Anxiety Disorders Inverview Schedule—Client (ADIS-IV) decreased, indicating no significant impairment, and the ADIS-IVs at those time periods indicated he no longer met criteria for a specific phobia. Improvements were also seen in the client’s self-reported fear, on his ratings of catastrophic cognitions, on a behavioral avoidance task, and in the comorbid social phobia symptoms.
1 Theoretical and Research Basis for Treatment
This case study is of the treatment of a specific phobia of swallowing pills in a young man. Specific phobia of choking is characterized by an extreme fear of ingesting or swallowing certain foods, liquids, or pills (McNally, 1994); it is qualified in the “other” type in the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000). The age of onset for choking phobia varies from childhood to older adulthood, and although the prevalence of choking phobia is unknown, specific phobias have a lifetime prevalence of 7% to 11% (DSM-IV-TR; American Psychiatric Association, 2000). Behavioral and cognitive–behavioral treatments have the most empirical support for choking phobia (Bailly, 2005).
One such cognitive–behavioral therapy (CBT) for specific phobia that has amassed a considerable evidence base over the past several decades is One-Session Treatment (OST; Davis, Ollendick, & Öst, 2012; Öst, 1989, 1997). OST is a very brief evidence-based treatment for a variety of specific phobias that occurs in one 3-hr massed exposure session. This treatment approach makes use of a combination of techniques including participant modeling, reinforcement, and cognitive challenges, all within the context of a larger graduated exposure hierarchy. To date, OST has also reached probably efficacious status for treating specific phobias in adults based on the available literature (Davis, Ollendick, et al., 2012; Zlomke & Davis, 2008). Studies on OST have occasionally mentioned less common phobias including those of vomiting, choking, or swallowing (e.g., Davis, Ollendick, et al., 2012; Ollendick et al., 2009) but have not clearly described how OST might be carried out with these other-type phobias. Similarly, recent reviews and descriptions of how to perform the treatment have not included specific examples of how to treat this particular type of specific phobia (e.g., Davis, Ollendick, & Öst, 2009; Zlomke & Davis, 2008). As a result, the following case study provides an opportunity to describe the various techniques utilized in OST and their application to the specific phobia of swallowing pills.
2 Case Presentation
“John” (pseudonym) was a 23-year-old White male who worked part-time, making approximately US$15,000 annually. He was also taking night classes at a local community college. He reported no previous inpatient or outpatient treatment for mental health concerns. John also reported having never been prescribed any psychotropic medications and reported no prior or current serious health complaints. He reported his marital status as engaged to be married. He presented as reasonably well-groomed, slightly fatigued, shy, and anxious.
3 Presenting Complaints
John entered the clinic for treatment as part of his interest in a larger University IRB-approved study offering free treatment for specific phobias. His primary complaint was a significant fear of swallowing pills since childhood. John reported that he would become anxious during any attempts to swallow oral medication and that he would take liquid/chewable forms of child medications when ill if they were available. Specifically, he avoided taking pills if at all possible, and if he was faced with taking a pill, he reported that his “throat closes up,” his muscles tense, he feels “on edge,” and he feels his heart pounding and blood rushing. In these situations, John reported that he had not generally been able to successfully swallow the pill and instead would chew it up, crush capsules in his mouth, or get so anxious that he would hold them in his mouth until they dissolve (in these instances he reported he had “gotten used to the taste”). John reported that these sensations and anxious responses had gotten so bad that they generalized to being triggered by the sight of pill bottles as well.
In addition, John reported experiencing significant symptoms of social anxiety for the past 5 years. In particular he reported fears of public speaking, speaking in classes, and talking to unfamiliar people. He actively avoided these situations and worried that he might embarrass himself or do or say things to make others have a bad impression of him. His symptoms reportedly “weighed on [his] mind” and he often thought about getting treatment for it because symptoms had progressed to the point that thinking about it had reportedly caused him to have panic attacks. No other significant symptoms of psychopathology were reported.
4 History
John reported that throughout his childhood and early adult life, he had rarely been able to successfully swallow a pill (i.e., he only recounted two successful instances in his lifetime). He stated that he became anxious every time he attempted to swallow a pill on his own or at the prompting of family members. Historically, he reported a fear of pills that has existed for more than 15 years and developed from an initial bad experience. John vaguely recalled having accidently swallowed a piece of hard candy whole as a child that led him to have a sensation of choking and a bout of coughing even though he did not actually report choking on the candy. Subsequently, his family had resorted at times to forcing him to take medication in pill form unsuccessfully, thereby further exacerbating his fear and worry. During one such incident, several family members were reported to have forced him into a chair and force-fed him several aspirins. He reportedly did not swallow the first pill, thereby allowing it to instead dissolve in his mouth, but he reported “accidentally” swallowing the second pill causing him greater anxiety.
5 Assessment
Following his completion of an informed consent, John was assessed for symptoms of psychopathology, particularly those related to anxiety and specific fears, using the Anxiety Disorders Interview Schedule—Client (ADIS-IV; Brown, DiNardo, & Barlow, 1994). The ADIS-IV is a widely used, semi-structured diagnostic interview that assesses for the presence of a variety of anxiety, mood, and other disorders. A detailed assessment of symptoms, fear, avoidance, and distress are obtained, along with patients’ ratings of interference with daily life on a 0-to-8 scale. Clinicians assign a clinician severity rating (CSR) from 0 to 8, with a CSR of 4 and above indicating clinical levels of impairment or a “diagnosable” disorder and 3 and below indicating subclinical to more normative levels of symptoms. The measure has been shown to have very good interrater reliability for the anxiety disorders. In this case study, the ADIS-IV was conducted at each time period by a trained examiner who was blind to whether the participant had a specific phobia and to whether treatment had been conducted (as per the larger, phobia treatment study). Examiner training and supervision was as follows. Doctoral students in an APA-accredited clinical psychology program served as examiners. All examiners initially attended a 2- to 3-hr training on the use of the ADIS-IV conducted by the first author. Those in training then observed and simultaneously scored at least two live ADIS-IV interviews conducted by a trained examiner. Following that observation, examiners-in-training had their initial interviews (2 or more) observed and approved by a trained examiner prior to their seeing study participants. Finally, all examiners and trainees enrolled in an anxiety practicum for at least 2 semesters and attended weekly staffing/supervision meetings. Interrater reliability for the primary and/or treated specific phobia in this lab as a part of the overall project was 100%.
John also completed the Motivation for Fear—adult (MOTIF; Davis, 2006a; Nebel-Schwalm & Davis, 2011) and the Fear Survey Schedule–II (FSS-II; Geer, 1965) to further measure his fears. The MOTIF is a functional assessment instrument designed to examine the potential functions of fear and phobia in adults. This instrument is still under development, but findings using the preliminary scoring and factors suggested by Nebel-Schwalm and Davis (2011) indicated John’s phobia was maintained by escape and distress. Escape contains items indicating attempts to escape the situation and also his receiving negative reinforcement for escape (e.g., “How often do you appear to feel better after successfully leaving or avoiding the feared situation?”). Distress is indicative of the degree of fear experienced and also difficulty coping alone with that fear (e.g., “How often do you have difficulty calming down by yourself during or after being afraid?”). The items of the FSS-II include animals, objects, or situations that could evoke fear. The FSS-II comprises 51 items that measure fear responses; participants rate their fear levels from 1 to 7, and scores range from 51 to 357. The sum is taken for a total score with higher numbers indicating more fear. The FSS-II has been shown to have excellent internal consistency (r = .94 using Kuder–Richardson Formula 20) and has been validated against other measures (Geer, 1965; Liddell & Hart, 1992). It has also frequently been used in young adults, similar to John (Liddell & Hart, 1992; Reuther, Davis, Grills-Taquechel, & Zlomke, 2011), and the instrument’s internal consistency with this age range has been found to be quite high (e.g., α = .97; Munson, Davis, Grills-Taquechel, & Zlomke, 2010).
In addition, John participated in a behavioral avoidance task (BAT). As part of the larger phobia study, all participants were given a 10-step in vivo BAT, which was standardized for each feared stimulus. In this instance, a BAT room was preset with a glass of water and a vitamin tablet on a small table on the side of the room opposite the door. The BAT involved requesting John to open the door to the room, walk to the other side, pick up the vitamin and swallow it using the glass of water. Low demand instructions were used, and John was instructed that he did not have to proceed further than he wanted with the BAT (or even enter the BAT room). Avoidance behavior was observed and rated on a scale from 0 (does not agree to proceed with BAT) to 10 (completes terminal step) for all BATs based on the last step completed. Subjective units of distress (SUDs) were taken on a scale from 0 to 8 (0 being no fear at all, 8 being very, very much) immediately before the BAT and at the last step completed during the BAT (while John was still in that last step). This range of SUDs was chosen to capitalize on research participants’ familiarity with the ADIS-IV and the use of the fear thermometer that accompanies that interview (Davis et al., 2013).
Finally, a functional assessment worksheet for OST (FAW; Davis, 2006b; Davis, Ollendick, et al., 2012) was completed with John to collect detailed information about his specific fear of swallowing pills including stimulus characteristics and possible maintaining variables. The FAW is a 4-page semi-structured interview designed to probe and collect information important for the planning and execution of the OST. The FAW has three broad sections that probe the individual’s catastrophic cognitions, assist in the creation of a fear hierarchy, and obtain relevant information about the individual’s unique phobia symptoms and history (i.e., this section is broken into “etiology/maintaining variables,” “client’s previous exposures,” “client’s response when exposed,” and “important stimulus characteristics” (Davis, 2006a). In addition to providing important information for designing the OST, the FAW also includes cognitive rating scales adapted with permission from those reported in Ollendick et al. (2009).
6 Case Conceptualization
Based on the results of the assessment, John qualified for a diagnosis of specific phobia—other type (choking/swallowing pills). John’s phobia was determined to be significantly distressing to him and to interfere with his daily functioning by impairing his ability to take oral medication when necessary. He was observed to be unable to complete the action of swallowing a pill, despite his best attempts. Other than social phobia, John did not meet criteria for any other psychiatric diagnoses nor did he exhibit any medical complications that would be prohibitive of an exposure-based treatment. Catastrophic thoughts identified as part of the FAW included not being able to swallow the pill, the pill getting stuck in his throat, and choking on the pill.
John’s specific phobia is best conceptualized according to Öst’s (2012) cognitive–behavioral model for the maintenance of specific phobias. In this model, specific phobias are maintained by (a) a strong conviction in the catastrophic beliefs and (b) autonomic arousal that combine to maintain specific phobia psychopathology. These factors then lead to escape or safety behavior, which prevents disconfirming exposures and leads the individual to conclude that the catastrophic belief is justified, given avoidance prevented or attenuated the feared catastrophe (Öst, 2012). Based on John’s history and catastrophic cognitions, it was believed that his early experience with choking on a piece of candy had become generalized to other similar food/pill items. His hazy recollection of a learning history was not unexpected given the myriad experiences that can culminate into a clinical phobia (Nebel-Schwalm & Davis, 2013). Over time, it became apparent that his catastrophic cognitions (i.e., being unable to swallow a pill, if he did attempt to swallow it would get stuck, and if it did get stuck he would choke) remained largely unchallenged by him avoiding opportunities to swallow pills. Furthermore, consistent with Öst’s (2012) model, John’s catastrophic cognitions likely interacted with physiological sensations of fear prompted by various experiences with eating, swallowing, coughing, and choking through the typical course of consuming edibles. Finally, his cognitions and fear of pills, in particular, were likely exacerbated by familial practices. His view of pills specifically as something to be feared and physiologically arousing was reinforced by the repeated episodes of physical restraint and force-feeding him pills through the years. Therefore, pills in particular became stimuli associated with catastrophic thinking, low self-efficacy, physiological arousal, and avoidance in concert with a history of somewhat traumatic restraint when forced to consume pills.
John presented as highly motivated and eager to be able to swallow oral medication and no longer need to use children’s medication when ill. Given the empirical support for exposure-ased CBT for specific phobia (Bailly, 2005; Davis, Jenkins, & Rudy, 2012), the straightforward nature of John’s case, and his strong desire to overcome his fear and subsequent heightened motivation for treatment, OST was thought to be an appropriate choice of treatment for his fear of swallowing pills, and so he continued in the study to the treatment portion. Completion of OST would allow John to receive exposure-based CBT for his fear and include providing him with psychoeducation, addressing his catastrophic cognitions, and gradually exposing him to the process of swallowing pills in a single, massed, 3-hr session format. As aforementioned, OST has been found to be an evidence-based treatment choice and probably efficacious for the treatment of specific phobias in adults (Davis, Jenkins, et al., 2012; Zlomke & Davis, 2008).
7 Course of Treatment and Assessment of Progress
Per Öst’s (1989, 1997) protocols and as further described by Zlomke and Davis (2008), treatment for John’s specific fear of swallowing pills was administered in one 3-hr session. Treatment progress was assessed using the previously mentioned measures (i.e., ADIS-IV, FSS-II, BAT, and FAW) administered at a pretreatment assessment, posttreatment assessment (3 weeks following treatment), and a follow-up assessment (8 weeks following treatment). At pretreatment, John met criteria for a specific phobia of swallowing pills (ADIS-IV CSR = 6) and for social phobia (ADIS-IV CSR = 5) given the symptoms and impairment he described. He was only able to complete 70% of the total steps of a low-demand pill BAT (approached the pill but did not pick it up or swallow it). His SUDs were low at the step he stopped (a 2 on a scale of 0-8), likely indicating he decided to stop the BAT as his approach and distress increased so as not to experience significant distress. In addition, before beginning treatment, John was asked to rate his identified catastrophic cognitions as to the certainty of each one occurring on a scale from 0 (not at all certain) to 8 (very certain that the thought would come true). He rated his certainty of not being able to swallow the pill at a 7, his certainty of the pill getting stuck and creating an uncomfortable feeling at a 6, and his certainty of choking on the pill at a 3.
The 3-hr OST session began with the clinician providing psychoeducation about the physiology of swallowing, followed by exposures moving up the hierarchy created by John and the clinician during the functional assessment session (guided by the FAW). With each exposure, participant modeling was used in which the therapist demonstrated each step of the fear hierarchy and then participated with the client in that step of the hierarchy. Items on the hierarchy included Mini M&Ms, Tic-Tac’s, small empty pill capsules, medium “typically sized” empty pill capsules, and large “horse pill” empty pill capsules. John was asked to attempt each step with the clinician after the step was demonstrated. The clinician and John did not move to the next step until mastery of the current step had been achieved (i.e., successful completion of the step without the presence of significant anxiety).
At the beginning of the session, psychoeducation about pill swallowing focused on emphasizing that it is an automatic process for which the body is prepared and discussing the body’s natural protective mechanisms against choking. This education lasted approximately 20 min, and John started to think of swallowing pills as having the same physiology as swallowing food; although he was still very anxious to begin the exposures. Exposures began with the therapist and client swallowing the easiest items (mini M&M candies). John perceived these to be easiest because they were round. He considered the round candies as a more natural shape to swallow, because they were soft and would dissolve if he was unsuccessful in his attempt to swallow them. Because he was not worried about this candy getting stuck in his throat, he was able to challenge his first cognition (i.e., not being able to swallow the pill) without the other catastrophic cognitions (i.e., the pill getting stuck and choking on the pill). The therapist and John took the longest amount of time on this food item (approximately 1 hr).
Once success had been achieved at the first step of the hierarchy (successively swallowing at least five mini M&M candies whole), the client moved up to more anxiety-provoking foods (e.g., foods/edibles of larger size, oblong shape). He perceived the next step up (Tic-Tac’s) to be more anxiety-provoking because the candy was oblong and hard and would not melt quickly. Therefore, he was able to challenge his second two catastrophic cognitions (i.e., the pill would get stuck in his throat, and he would choke on the pill). Because of his increased anxiety, John drank much more water when he was initially trying to swallow Tic-Tac’s. However, he was able to successfully swallow the candy on approximately his second or third attempt. During the first several attempts, he tried several times but ate the candy instead. After swallowing several Tic-Tac’s in a row, John became much more confident in his ability to swallow pills and was able to progress through the rest of the hierarchy items fairly quickly (small, medium, and even large empty pill capsules). This relatively faster progression may have been due to him successfully challenging his catastrophic cognitions. John was able to successfully swallow several large “horse pill” empty pill capsules. At the end of the treatment session, John was able to complete all of the items on his hierarchy. He reported no longer having anxiety before, during, or after attempting to swallow a pill, including the largest pill size presented.
8 Complicating Factors
One unanticipated consequence of choosing the OST modality for treatment was the large amount of water consumption that was necessary within the 3-hr span. Often, many attempts are necessary to complete or master a single step of the fear hierarchy, requiring several cups of water be consumed for each step. Consequently, the feeling of fullness can be prohibitive to continuing on with the next step without breaks (for the client and the clinician who is modeling each step). Clinicians must also be mindful of the slight potential of water intoxication should an excessive amount be consumed. It is recommended that clinicians vary the types of liquid consumed (e.g., water, milk, coke, juice) according to participant preference to help with this problem. Depending on the participant, it may also be important to consider the type of drink as it relates to their fear of swallowing pills because some participants may feel more anxious about using certain types of liquids. Along the lines of these safety recommendations, it is also important to confirm that the pills and edibles to be used during exposure are inert and/or the patient does not have any allergies or prohibitive medical conditions that need to be taken into consideration (in this case he did not).
Furthermore, it should be anticipated that the hardest step will be the initial swallowing of the object (even the smallest size) without any chewing. This was the case in this instance as well. This step may take some time, and depending on the time spent on the step, the ability to complete the hierarchy in its entirety may not be possible (though this was not the case with John who completed his entire hierarchy). In such circumstances, it should be the goal of the clinician to move up the hierarchy as far as possible, while maintaining the gradual pace necessary to ensure that mastery has occurred at each step. Along these lines, successful outcomes in OST have not been tied to completing a particular percentage of the hierarchy, though successful completion of much of the exposure would be anticipated (Davis, Ollendick, et al., 2012).
9 Access and Barriers to Care
John sought treatment through participation in our larger treatment study on the use of OST for specific phobias. Because he had reliable, adequate transportation and the assessments and treatment were offered at no cost, there were no access or barrier issues in this case. Even so, a general issue is the ability of OST for the general public outside of this university setting. The OST treatment manual was only just published in 2012 (Davis, Ollendick, et al., 2012), and training opportunities to learn how to adequately administer the massed treatment are still limited. Overall, OST is still not widely practiced, even though it has been shown to be very effective.
10 Follow-Up
Two follow-up assessments were conducted to assess John’s level of functioning and results of treatment. A posttreatment assessment was conducted 3 weeks after the completion of the OST session. In addition, a treatment follow-up was completed 8 weeks after the completion of the OST session. According to the readministration of the specific phobia section of the ADIS-IV, John no longer met criteria for a specific phobia of choking or swallowing pills (CSR = 2) at posttreatment or at follow-up (CSR = 2; see Figure 1). Interestingly, he also no longer met criteria for social phobia at posttreatment (CSR = 3) or at follow-up (CSR = 1) sessions. In both the assessments after treatment, John was able to complete 100% of the steps of the BAT (i.e., swallowing a pill) with little anxiety (see Figure 3). In addition, his total score on the FSS-II decreased from pre- to posttreatment and follow-up assessments (see Figure 2). Furthermore, his ratings of certainty regarding his catastrophic cognitions decreased as follows: Certainty of not being able to swallow the pill decreased from 7 at pretreatment, to 3 at posttreatment, and 2 at follow-up; certainty of the pill getting stuck and creating an uncomfortable feeling decreased from 6 at pretreatment, to 2 at posttreatment, and 4 at follow-up; certainty of choking on the pill decreased from 3 at pretreatment to 1 at posttreatment and follow-up. John’s SUDs showed no change at post (still a 2) and only a slight decrease at follow-up (a 1); however, he completed all steps of the BAT at these follow-up appointments and did not attempt to swallow the pill at the pretreatment assessment. Overall, John no longer reported anxiety related to choking when swallowing pills and reached his goal of being able to take oral medication as necessary.
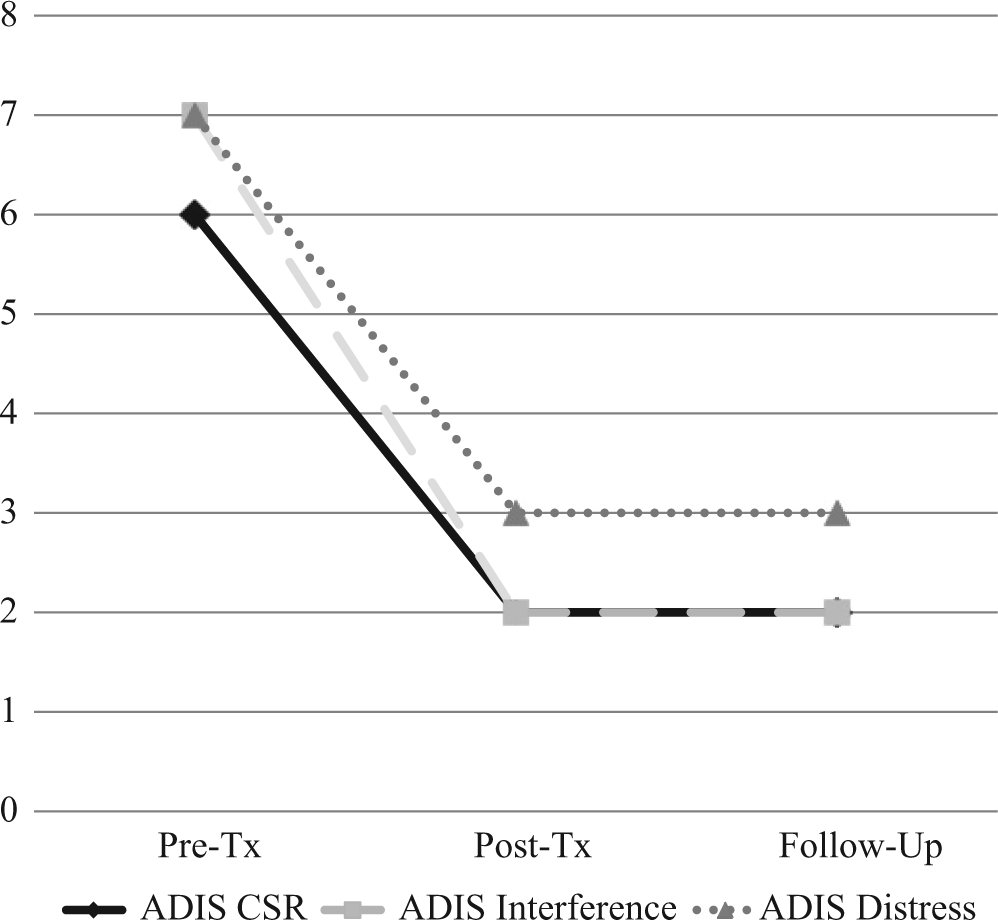
ADIS-IV clinician severity rating (CSR) outcomes.
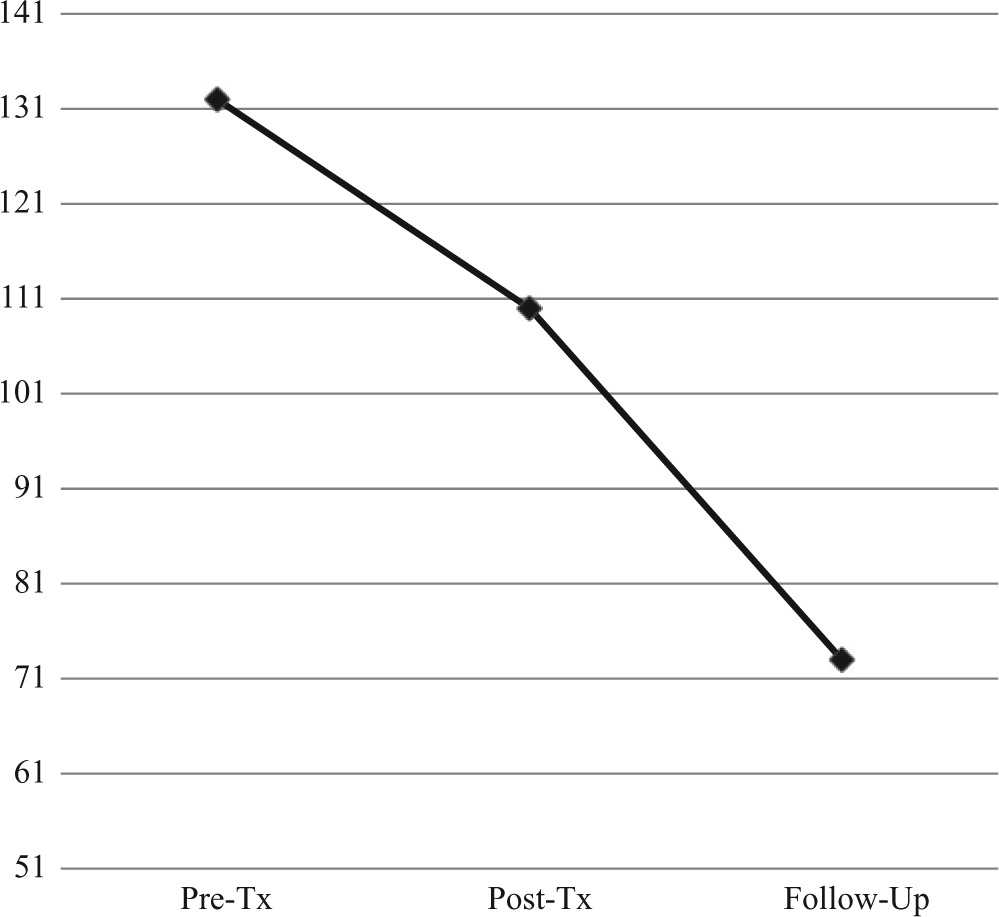
Fear survey schedule–II (FSS-II) outcomes.

Behavioral avoidance task (BAT) outcomes.
11 Treatment Implications of the Case
John greatly improved following OST for his specific phobia of choking and swallowing pills. According to clinician-administered interviews, a BAT, and self-report measures, he no longer met criteria for a specific phobia, and he reported that he no longer feared swallowing pills. These gains were seen at the posttreatment and 8-week follow-up assessments. However, his SUDs were low throughout and exhibited little change. He had the same level of distress posttreatment that he reported before treatment when he could not complete the BAT. It may have been that his overall anxiety sensitivity had not yet changed subsequent to the treatment given the brief timeline of assessments. In other words, individuals with significant fears have been found to have an increased sensitivity and aversion to physiological experiences (Reuther et al., 2011). John may have been stopping his exposure on the BAT at the onset of these sensations. Similar relationships between BAT progress and SUDs have been described (Davis, 2013; Ollendick, Lewis, Cowart, & Davis, 2012). Even so, we would expect him to further solidify his treatment gains in time. Although the follow-up period for this study was relatively short, past research on OST for the types of specific phobia other than choking has shown maintenance of treatment gains at six months and 1 year following treatment (Ollendick et al., 2009; Öst et al., 2001).
Given the gains seen in this individual case, OST appears to be an effective option for treating specific phobia, other type, of swallowing pills. This treatment also has great appeal in that pill-swallowing phobia usually does not begin to interfere until one needs to take a medication in pill form, making the haste of receiving treatment all the more important. This treatment approach is also beneficial as the specific phobia of choking has onset in childhood and adulthood, and the literature has supported it as appropriate for both age groups.
In addition, this case also provides some replication in an adult of an OST phenomenon documented more thoroughly in children—treatment generalization beyond the targeted specific phobia. Ollendick, Öst, Reuterskiöld, and Costa (2010) found that comorbid disorders in 100 youth treated with OST did not affect treatment outcome. More interestingly, however, was that OST for the targeted phobia was associated with a generalization of treatment effects to other phobias and anxiety disorders (i.e., statistically significant decreases in CSRs for those disorders). Such a generalization appears to have been the case here as well. John’s CSRs for his diagnosis of social phobia decreased from pre- to posttreatment and even more at follow-up, thereby giving the appearance of a response to the OST. Such a response is not necessarily unexpected as the OST teaches a client to break down and gradually confront anxiety-provoking situations and also to learn how to expose oneself and better handle anxiety. This may have been what transpired in this case. Specifically, OST provides a very structured and straightforward approach to learning how to do exposures for anxiety-provoking stimuli. In addition, it theoretically increases a patient’s sense of self-efficacy for the treated stimulus, and possibly for performing small, manageable self-exposures (Davis, Ollendick, et al., 2012). While we do not have direct knowledge of or evidence for self-exposures for social anxiety or more global changes in self-efficacy in the current case, these would be likely possibilities for the generalization effects observed.
12 Recommendations to Clinicians and Students
This case presentation has provided support for the use of OST with adults who have a specific phobia of swallowing pills, as well as tentative evidence of the generalization of OST effects to a comorbid anxiety disorder in an adult. OST has demonstrated efficacy across a number of specific phobias; however, this is the first detailed description of its use with a problematic fear of swallowing pills. Importantly, this brief, intensive intervention offers a rather immediate, quick, and effective intervention for a specific phobia that often prevents clients from receiving medical care (i.e., a quick resolution to a client’s fear to allow for important medical treatment).
This lone case study, however, should be interpreted with caution, as it did not make use of a single-subject design capable of confirming treatment effects. Even so, the bulk of the research on the use of OST across a host of phobias would seemingly suggest the intervention’s utility (cf., Davis, Jenkins, et al., 2012). As well, the effects of treatment seemed to last at least 2 months after the massed exposure, and similar studies have documented the long-term benefits of OST. As a result, whereas a great deal more study is needed to justify OST as an efficacious treatment for pill and swallowing phobia in particular, its evidence base across numerous phobias to date would suggest no reason to believe that it would not be effective in other instances of specific phobias of swallowing pills. Future research, however, will be necessary to determine the mediators and moderators of OST outcome, as well as any limitations in its use for particular fears.
From a clinical training perspective, OST offers a unique opportunity to train clinicians and students in an evidence-based intervention that incorporates many, if not most, of the techniques used in the treatment of other anxiety disorders. As a result, OST has been suggested to be “A Model CBT Protocol” (Albano, 2009, p. 359). Moreover, it has been argued that,
If training begins with OST for phobias, then I would argue that subsequent training for anxiety and mood disorders can flow rapidly by focusing on unique elements of the protocol or specific developmental adaptations. In considering training costs plus the costs of therapy, OST is likely to prove the most cost efficient model that exists in contemporary CBT.” (Albano, 2009, p. 359).
In addition to this high praise, tools for practitioners, students, and those training others in the use of OST exist in the recent comprehensive edited volume on the topic (Davis, Ollendick, et al., 2012). As a result, and though more study is always useful, OST offers promise as a treatment for a wide range of specific phobias and as a key treatment to be learned by those just beginning to practice cognitive–behavioral techniques.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by grants from the Council on Research at Louisiana State University and from the College of Humanities and Social Sciences. Their support is gratefully acknowledged.