
Abstract
Deaf and hard of hearing (DHH) children are an exceptional needs population with unique mental health concerns requiring specialized intervention. However, psychological interventions aimed at treating these children are limited. Parent–Child Interaction Therapy (PCIT) is an empirically established therapeutic modality for the treatment of children with behavioral and emotional difficulties. This case study describes how PCIT was adapted to effectively intervene in assisting a deaf mother improve parent–child communication, bonding, and her hard-of-hearing son’s behavior. Readers will learn how PCIT was adapted and implemented with a DHH family, including the use of sign language interpreters within the model, translating PCIT behavioral coaching to American Sign Language, and an overall broadened understanding of mental health treatment with the DHH population. The effect of treatment on the child and parent who participated is also discussed.
1 Theoretical and Research Basis for Treatment
The effect of deafness or hearing loss on emotional and behavioral development is significant. Given that hearing loss in children often translates into delayed language development, deaf and hard of hearing (DHH) children are at a higher risk of developing psychological conditions (Hintermair, 2006; Hogan, Shipley, Strazdins, Purcell, & Baker, 2011). In addition, compared with hearing children, some estimate the rate of emotional disturbance and behavioral problems in deaf children is two times higher (Stevenson et al., 2011), while others found the incidence to be five times larger (Vogel-Walcutt, Schatschneider, & Bowers, 2011).
Despite the increased need for mental health services among DHH children, when a group of medically oriented providers were surveyed about their ability to make mental health referrals for DHH children, only 29% of the respondents reported that they could find services available in American Sign Language (ASL; Montoya, Giardino, & Leventhal, 2010). When informants were further asked about community-based treatments (CBTs) versus home-based treatments (HBTs), only 39% of CBTs provided DHH children access and an even fewer percent (22.7%) of HBTs offered services (Montoya et al., 2010). Regarding the use of sign language interpreters, the same researchers found that most practitioners reported evaluating DHH children (84.5%), but only half reported using professionally trained sign language interpreters (Montoya et al., 2010).
Behavioral problems among deaf children may result from poor parent–child communication, as well as DHH children’s decreased causal thinking skills, and decreased ability to learn new behaviors and regulate their emotions (Quittner et al., 2010). Quittner et al. (2010) argued that if a parent with a child who has unique communication needs does not adopt new communication strategies, it can lead to difficult parent–child interchanges and negatively affect parenting duties. Therefore, a key issue for parents of deaf children seeking to modify their child’s behavior is the ability to effectively communicate with their child and implement new communication strategies.
For hearing and deaf parents of deaf children, parental stress is greater compared with hearing children (Hintermair, 2006; Quittner et al., 2010). One perspective is that parenting stress may be heightened due to incongruence between parent expectations for typical child development and the deaf child’s actual ability and greater need for parental support (Quittner et al., 2010). For deaf parents, unique types of quality attention to their deaf child’s needs are essential to the child’s development of effective communication skills and improved responsiveness to their environment (Sanford Koester & Lahti-Harper, 2010). In evaluating desirable intuitive parenting abilities, Sanford Koester and Lahti-Harper (2010) learned that hearing mothers improved their interactions with their infants by increasing variations in pitch and melodic speech. Similarly, deaf parents enhanced their signs by increasing physical proximity and using strong facial expressions such as increased eyebrow lift, and opening of the eyes and mouth more widely (Sanford Koester & Lahti-Harper, 2010).
Counseling and therapy are generally not trusted within the DHH community, primarily due to unsatisfactory results in treatment. As such, strength-based, results-driven, and wellness models are recommendable (Peters, 2007). For DHH patients, identifying and working with a clinician who has respect for deafness as a unique culture and does not view their communication difference as a deficit is of great importance. Therapies such as dialectical behavior therapy, solution-focused brief therapy, constructionist therapy, and cognitive-behavioral therapy are among the interventions that have been adapted for treating DHH individuals (Fellinger, Holzinger, & Pollard, 2012). In a survey of 456 caregivers of deaf children, parents reported a preference for clinicians who specialized in DHH, appreciated receiving internet resources, and valued opportunities for contact with other parents including those of children with and without hearing loss (Jackson, 2011). Moreover, DHH persons value treatment facility efforts to offer an ASL-fluent practitioner, or an interpreter who is specialized in translating for the specified setting (Fellinger et al., 2012).
Parent–Child Interaction Therapy (PCIT)
PCIT is a manualized parent training coaching model developed by Sheila Eyberg (2005). Parents are coached on effective ways to interact with their child by a therapist who is behind a one-way mirror in an observation room and provides live parent coaching through a bug-in-the-ear device (McNeil & Hembree-Kigin, 2010). Eyberg explains that PCIT has core defining principles that should be maintained with all adaptations and describes these core elements as Baumrind’s authoritative parenting paradigm, along with coaching that uses operant conditioning techniques aimed at addressing the function of behaviors. Moreover, PCIT is distinct from other parent training and family therapy models in that it applies live parent coaching with the child present (Timmer, Urquiza, Zebell, & McGrath, 2005).
PCIT’s effectiveness has been evaluated in a large number of studies, including pre–post treatment comparisons, single-subject studies, program evaluations, and randomized controlled trials that have resulted in its designation as an evidence-based treatment (Lyon & Budd, 2010; Substance Abuse and Mental Health Services Administration [SAMHSA], 2009; Zisser & Eyberg, 2010).
PCIT has two treatment phases. In the first, child-directed interaction (CDI), the parent and child increase attunement and attachment via the application of PCIT relationship enhancement strategies (McNeil & Hembree-Kigin, 2010). In CDI, parents develop competency in the ability to praise, reflect, imitate, describe, and display enthusiasm and enjoyment (PRIDE skills) while following their child’s lead in play (McNeil & Hembree-Kigin, 2010). During the live coaching session, the therapist, who is in another room behind a one-way mirror, directs the parent to initiate play and follow the child’s lead. Meanwhile, the therapist codes the parent’s application of the PRIDE skills. Throughout the course of treatment, one of the goals is to achieve mastery of the PRIDE skills, with special emphasis on attaining 10 praises, 10 descriptions, and 10 reflections (10-10-10 skills) within the 5 min of coding. The coach additionally guides the parent to abstain from critical comments and excessive questions that can be intrusive to the play and possibly result in child disruptive behaviors (these are sometimes described as “don’t behaviors”). Consistent application of these skills is believed to be at the core of enhancing the parent–child relationship.
The second phase is the parent-directed intervention phase (PDI), which is aimed at improving the child’s behavioral compliance (McNeil & Hembree-Kigin, 2010). During this stage of treatment, the therapist teaches the parent compliance sequences that, among other skills, include the parent stating clear and direct commands, demonstrating rule setting, implementing of time-out, and removing privileges (Dombrowski, Timmer, Blacker, & Urquiza, 2005; McNeil & Hembree-Kigin, 2010). In a typical PDI session, the parent is coached to continue application of the CDI (i.e., PRIDE) skills with consistency toward reinforcing desired behaviors. In this phase, the parent is also taught how to state direct commands of increasing difficulty, which heightens the likelihood that the child will noncomply and then allows the parent the opportunity to implement a timeout sequence or a removal of privilege with the real-time support of the clinician. Together, child lead (CDI) and parent lead (PDI) interactions where nurturance and firm limits occur can be “calibrated”/individually modified and applied to intervene in changing child behaviors, including adaptation to special populations (Eyberg, 2005, p. 198).
Research shows that equipping parents with behavioral strategies empowers them to serve as change agents in reducing their child’s behavior problems and can serve to improve positive parenting approaches (Timmer et al., 2011). Given that parental stress is especially high for parents of DHH children, empowering these parents with PCIT behavioral strategies is a crucial objective.
Total PCIT treatment length is approximately 15 to 20 weeks of 1-hr sessions (SAMHSA, 2009); however, because PCIT uses a skill building approach to determine completion of treatment, parent and child “graduation” is dependent on mastery of parenting skills (i.e., PRIDE, compliance sequences) and improvement of the child’s initial problem behaviors (McNeil & Hembree-Kigin, 2010).
Eyberg (2005) states that the essential elements necessary for effective nurture (CDI) and limit setting (PDI) interactions can be adapted in the treatment of special populations. Furthermore, changes to PCIT must take into account differences in culture, that is, the culture of the special population (Eyberg, 2005). McNeil and Hembree-Kigin (2010) suggested that future PCIT research expand on current findings that the treatment is helpful for children of diverse behavioral and mental health need. Because DHH children are susceptible to delays in development and behavioral disruption, research in this area is pertinent. This case study represents a starting point for evaluating the application of PCIT with DHH families.
Eyberg (2005) further explained that PCIT treatment adaptation refers to “changes in the structure . . . ” (p. 200). PCIT was developed and has been studied for use in hearing parents and hearing children, and was not designed with DHH families in mind. As such, adapting the model to these families presented logistical and clinical challenges. These involved eliminating direct coaching to the parent and instead using a sign language interpreter in the treatment room, which required re-organization of the therapeutic space and special consideration for therapeutic phenomena that might occur involving the interpreter.
Planning Interpreting and PCIT Coaching
Sheppard (2011) conducted a study comparing interpreters who were specially trained to interpret for research with nonresearch trained community interpreters and found that interpreters who were additionally trained by the researcher to perform the unique tasks of the experiment facilitated increased accuracy and quality of data collection. By extension, clinicians intending to obtain essential information for diagnostic and treatment planning purposes should also provide their interpreters with setting and task specific training to reduce chances of miscommunication. Within the context of PCIT, this is of particular importance because PCIT’s effectiveness depends on following the treatment protocol with fidelity. Specifically, as outlined previously, one of the goals of PCIT is to assist parents in achieving mastery of the relationship enhancement skills, PRIDE, and compliance strategies while the clinician codes the caregiver’s verbalizations. In the case of DHH families, the interpreter’s role is crucial to translating to sign and to voicing parent signs in a manner that can be coded by the hearing clinician using the Dyadic Parent–Child Interaction Coding System–Third Edition (DPICS-III; Eyberg, Nelson, Duke, & Boggs, 2005).
In an article on conducting psychotherapy with deaf patients, de Bruin and Brugmans (2006) recommend that interpreters and therapists discuss their roles before treatment and agree on how they will collaborate. In preparation for a session, it is helpful for practitioners to communicate the goal of the session to the interpreter, driving home the main ideas and concepts that should be learned (Wolbers, Dimling, Lawson, & Golos, 2012). Pre- and post-session meetings between the interpreter and the therapist are vital for establishing session expectations (de Bruin & Brugmans, 2006). A pre-session meeting with the interpreter can assist in planning out the therapy hour so that there is smooth communication. Similarly a post-session meeting can help the therapist and interpreter coordinate their understanding of the technical and emotional aspects of the interpreted dialogue (Williams & Abeles, 2004).
In family therapy, the positioning of the interpreter is of great importance as it has the potential to influence the family dynamic (de Bruin & Brugmans, 2006). For example, de Bruins and Brugmans (2006) explain that when working to steer or influence the family system (e.g., reassign roles, shift power, align), the therapist may strategically position herself in the therapeutic space. However, when an interpreter is present, the organization is generally intended to facilitate communication between signing members and hearing members of the session. Having an interpreter in the room during therapy can therefore add another component to the clinical planning of therapeutic interventions.
When multiple family members require facilitated communication by the interpreter, it may be challenging for the therapist to determine which deaf person is speaking. This becomes especially challenging in PCIT because the therapist is not in the room, making it harder to discriminate between speakers, particularly when the therapist is looking down to code parent communication voiced by the interpreter onto the coding sheet. Clinically, the therapists may also lose some of the benefit obtained from observing gestures or other communication cues that may be more readily apparent if they were in the room (e.g., eye contact, hand motions).
Criteria and Selection of Interpreters
Translating from English to ASL is unlike translating from one spoken language to another spoken language. Translation to ASL entails conversion from a speech code to a visual code (Sheppard, 2011). Consequently, selecting a qualified interpreter who can effectively make this transfer is an important prerequisite to providing treatment. The process of deciding whether an interpreter meets criteria to provide quality interpreting can be challenging for individual service agencies because of their inexperience. For this reason, independent certification and accrediting bodies are valuable. Hitch (2005) states that because language is so essential to the learning process, certified interpreters are recommended in environments where important information is being conveyed due to the potential effect on comprehension. Undoubtedly mental health settings fit this description. In addition, certified interpreters who are independent contractors, or contract through an interpreting agency, have the benefit of providing unbiased interpreting because they are not affiliated with the employing institution and have already had their interpreting skills verified by an external body (Hitch, 2005).
In the United States, there are two interpreter-accrediting entities, The National Association of the Deaf (NAD) and The Registry of Interpreters for the Deaf (RID). NAD has five levels of interpreter certification. Levels I to III interpreters require supervision during interpreting, whereas those certified at Levels IV and V can interpret independently (Hitch, 2005). Similarly, RID awards an endorsement called a Certification in Interpreting (CI) that requires interpreters to pass a written and performance examination (Hitch, 2005). Interpreters with a CI can interpret without supervision. In this case study, all sessions were conducted using a certified interpreter contracted through an interpreting agency. 1
Confidentiality and Cultural Competence
Confidentiality is a right assigned to all mental health consumers and an ethical obligation for practitioners. Within the DHH population, issues surrounding confidentiality are compounded due to the use of interpreters. Clinicians should address confidentiality as it pertains to the use of interpreters and clarify the role of the interpreter to the patient and caregiver as a facilitator of communication and not as someone with whom they should independently explore clinical concerns (Peters, 2007).
Deaf Culture
Cultural diversity is not exclusive to race and ethnicity; it also includes cultural deafness where members communicate visually (Sheppard, 2011). Effective treatment of children who are DHH requires that therapists have an understanding and sensitivity toward deaf culture (Peters, 2007). Therapists should be aware of the differences in nonverbal communication between deaf and hearing persons. Moreover, while a cultural match between the therapist and patient is preferred (Williams & Abeles, 2004), given that ASL-fluent clinicians are sparse, culturally sensitive and affirming therapists who are willing to treat this unique population are needed.
Murray, Klinger, and McKinnon (2007) conducted a study where they qualitatively assessed the perceptions of individuals who defined themselves as culturally deaf when participating in deaf and hearing communities. They distinguished cultural deafness and medical deafness explaining that medical deafness relates to audiological “status,” whereas cultural deafness is defined by participation in the deaf community. Audiological deafness is often spelled with a small “d,” and cultural deafness is spelled with a capital “D.” Identification with one group or another varies between DHH persons and families. Murray et al. state that identification in either group is largely dependent on social engagement with hearing, deaf, or both hearing and deaf persons. Because of this continuum of identification with deaf culture and hearing culture, individuals may be more or less accepting of interventions that were originally developed for the hearing. In other words, because the belief that one’s cultural views and values are being respected is an important ingredient to therapeutic engagement, it may be that DHH persons who identify as culturally deaf disagree and/or do not perceive that interventions designed for the hearing could be adequately applied to treat those who are DHH. It is also possible that they may have a preference and or a greater acceptance to interventions that were specifically designed with their culture and language in mind.
In the Deaf culture, attention is gained in ways that may be considered rude among hearing people (Williams & Abeles, 2004). For instance, a deaf person might wave, flick lights on and off, or tap on the shoulder to obtain other’s attention. Sign language communication also involves exaggerated facial expressions, body and hand movements, closer physical proximity, and increased eye contact (Peters, 2007). These differences in interaction may produce discomfort for hearing practitioners and may be wrongly interpreted. For instance, parent gestures aimed at getting the child’s attention can be interpreted by the hearing therapist as a way of interrupting the child or leading the interaction instead of following.
The preceding section presented an empirical review of the literature that establishes the need for increased access to mental health services for children and families who are DHH. Currently, there are few ASL-fluent mental health clinicians and as such the use of interpreters is discussed as one way of increasing access. The responsible selection and use of interpreters, and how they may be used in the context of PCIT is presented. The section also provides an overview of PCIT and the stages of treatment. Finally, cultural and linguistic considerations pertaining to the application of PCIT to DHH are discussed.
2 Case Introduction
In the following description regarding participants, names of the family members are changed to protect their confidentiality. Both parents whose child is described in this case study consented to the sharing and writing of their story for the purpose of educating clinicians and increasing access to DHH families.
A mother and father brought their 9-year-old son “Sam G.” for a mental health assessment intake. Sam is a Latino male who at the time of intake was in the fourth grade. During the assessment clinical interviews, his parents initially reported that Sam was very inattentive, unable to complete tasks, required spoon feeding, could not tie his shoe laces, needed help getting dressed for school, was forgetful, ignored parent directions, and had problems getting along with his siblings and school peers. They also reported that while Sam was always active and inattentive, it was at the beginning of second grade (2 years prior to intake) that he became more aggressive with siblings and peers, became very disruptive during instruction—interfering with others’ learning and his own—and would have tantrums before school that would cause him to miss the school bus. A thorough clinical assessment that included several clinical interviews with Sam, his parents, and educators; behavioral observations in multiple settings; and parent completed rating scales (see below Section 5 “Assessment”) lead to the determination that Sam met criteria for a diagnosis of attention deficit hyperactivity disorder–combined type (ADHD-CT). The possibility of a learning disability was ruled out as his teachers reported that despite disruptive behaviors during instruction, Sam demonstrated grade-level academic performance on classroom tests and benchmark testing (i.e., standardized academic assessments administered by the school district). Sam’s ADHD-CT was characterized by hyperactivity including running and out of seat behavior six times daily, distractibility and inattention eight times daily, talking in class four times daily, playing during instruction three times daily, interrupting three times daily, and noncompliance with teacher directives four times daily. At home, Sam had a challenging time following routines such as attending and completing his homework five times weekly, he resisted showers and had to be told that it was time for his shower five times daily and to brush his teeth two times daily, and to get in bed at his designated sleep time three times daily. Sam’s symptoms and behaviors impaired his ability to perform to academic potential as he struggled with task and homework completion, and his noncompliance at home disrupted his sleep and wake times, which frequently caused him to miss the school bus and made him tardy for class.
All clinical services were conducted at Child Guidance Center, Inc., in Orange County California. The Child Guidance Center is a nonprofit community mental health agency that provides comprehensive outpatient mental health services to children and adolescents birth to 21 and their caregivers. The author, an experienced PCIT therapist and a licensed child psychologist, conducted all of the described assessment and intervention activities.
3 Presenting Complaints
At intake Mr. and Mrs. G. expressed concern about Sam’s school behaviors and worried that if he continued misbehaving and disrupting instruction then he would be removed from his school, which would be a problem as very few schools have a DHH program. They also shared that school staff required them to attend meetings to discuss Sam’s behaviors and this placed a strain on the family because only Mr. G. drove and would need to take off from work to attend meetings. The parents also related that it worried them that Sam’s younger siblings would begin imitating his disrespectful behaviors that included ignoring and protesting parent directives, and having tantrums in the grocery store when his parents did not purchase what he wanted.
4 History
Mrs. G. related that she learned she was pregnant 3 months into the pregnancy and received adequate pre-natal care. Sam was the product of a full-term, uncomplicated labor and cesarean delivery. Mother and baby were discharged 3 days post delivery and both were in good health. Sam was initially diagnosed as deaf, but later doctors realized that he had some hearing and subsequently fitted him for hearing devices. His parents reported that Sam began using his voice at about 1 year old when he started receiving speech therapy. His mother noted that he began using sign language in the home around the same time. Sam is reported to have reached all other developmental milestones within normal limits. With regard to the onset of ADHD-CT behaviors, his parents reported that Sam was always an active, distractible, and “stubborn” boy; however, they did not perceive this as a problem until the second grade when they began receiving behavioral referrals from school staff. The behavior referrals alarmed Mr. and Mrs. G. as it revealed that his behaviors were becoming a significant problem at school.
5 Assessment
The child in this study was assessed for PCIT following standard protocol, which involves administration of pre-treatment standardized assessments of child behavioral problems and parental stress, and a coded observation of the quality of the parent–child relationship. The 15-min observation (i.e., 5-5-5 playtime observation) consisted of all three components of the baseline observation protocol; 5 min of child-directed play, 5 min of parent-directed play, and 5 min of cleanup. During the first 5 min of the observation the parent–child interactions were evaluated and coded using the DPICS-III (Eyberg et al., 2005).
The parent also completed the Achenbach Child Behavior Checklist (CBCL 6-18; Achenbach & Rescora, 2001), Parenting Stress Index–Short Form (PSI-SF; Abidin, 1995), and the Eyberg Child Behavior Inventory (ECBI; Eyberg & Pincus, 1999) to clinically assess suitability for PCIT treatment. However, because the parent in this case study was deaf and related that she could not read English, the measures were administered via interpreter. Moreover, because the rating scales were not normed on deaf persons, standardized scores on these measures may not be reliable indicators of functioning or progress. Typically when parent measures cannot be depended on, teacher forms such as the Teacher Report Form of the Achenbach System (Achenbach & Rescora, 2001) and the Sutter-Eyberg Student Behavior Inventory (Eyberg & Pincus, 1999) are alternatively administered. However, in this case, the parent did not grant an exchange of information consent for the administration of teacher-rated measures.
A baseline observation was conducted using the DPICS-III (Eyberg et al., 2005). The DPICS-III was used to measure parenting abilities at pre- and post treatment. The pre-treatment baseline observation and coding revealed an absence of interactive dialogue during play and no parental application of behavior modification techniques. The child was engaged in solitary play and was not observed to invite nor include his mother in the play. He was observed to ignore parent directives when given a command to transition or cleanup, was often out of his seat, and was observed whining and protesting prior to complying. The mother applied the directed prompt to allow the child to select toys; however, she did not demonstrate the ability to follow his lead and instead was observed to sit in her chair and from a distance appeared to visually track her son’s behaviors without joining him. Following the observation, the mother shared that her son was much better behaved and cooperative during observation than he usually was at home.
The outcome of pre-treatment assessment yielded the following findings. Based on the DPICS coding and looking only at the core 10-10-10 skills, Mrs. G demonstrated two labeled praises, one reflection, one behavioral description, and a total of seven don’t behaviors (questions, commands, negative talk). On the PSI-SF, she self-rated Defensive Responding in the 15th percentile, which indicates a valid protocol; Parental Distress in the 7th percentile, Parent–Child Dysfunctional Interaction in the >99th percentile, Difficult Child in the 90th percentile, and Total Stress in the 89th percentile. On the Eyberg Child Behavior Checklist (ECBI), intensity was rated as T = 72 and number of problems was reported as T = 72. On the Achenbach CBCL Summary domains, Mrs. G’s responses yielded an Internalizing score of T = 68, Externalizing T = 80, and a Total Score T = 76.
After a thorough mental health assessment that included the above approaches and additional sessions where clinical interviews were conducted with both parents and the child, PCIT treatment was recommended. A treatment plan was jointly designed to decrease noncompliant and disruptive behaviors at home and school, and to improve parent–child and sibling relationships.
Formative assessment of treatment effect was conducted using a weekly check-in where the parent was asked to rate problem behaviors on a 5-point Likert-type scale, rate the degree of change or behavioral improvement compared with the previous week, and relate which PCIT skills were rehearsed and used with relative ease, and which ones were more challenging to apply. In addition, to prepare the parent for the session, she was asked to attend to positive behaviors in her child and share three good things he did that week. Following the check-in, a weekly observation was conducted using the DPICS-III system. In accord with treatment protocol, this family completed both phases of PCIT treatment: CDI and PDI. They completed 17 treatment sessions in total. The post-treatment assessment also included a 5-5-5 playtime observation and DPICS coding, administration of rating scales to obtain clinical information, and parent clinical interview.
6 Case Conceptualization
Following the determination that Sam met criteria for a diagnosis of ADHD-CT, his family and the psychologist (author) working with the family considered treatment options to address the disruptive, hyperactive, impulsive, inattentive, and noncompliant behaviors that had been identified as the primary areas of concern. His parents agreed that PCIT would be the most appropriate intervention because they felt that Mrs. G. needed hands-on practice to learn how to manage their son’s behaviors. Sam’s parents also agreed to a psychiatric assessment to evaluate whether he would benefit from medication, and while the psychiatrist did recommend beginning a trial of medication, Mr. and Mrs. G felt strongly that they preferred to begin with an intensive behavioral intervention such as PCIT and reassess the need for medication sometime in the future.
As highlighted previously, many of the standard aspects of PCIT were followed in treating this family. This section will exclusively detail the adaptations that were made to accommodate for differences in the communication modality. It is important to point out that PCIT treatment of DHH children requires more than is described in these sections on adaptation. Effective provision of PCIT requires extensive training, supervision, and practice coaching live cases.
Before conducting any sessions, careful consideration was given to room and seating arrangement to ensure effective coaching. In addition, sessions were video recorded so as to facilitate coding after the session and to modify and improve the treatment approaches. As such, the placement of the camera was critical. In our clinic, the camera was pre-installed and could not be moved—we therefore arranged the room with the fixed location of the camera in mind. Given our treatment room setup, we decided to sit the child and parent across from each other instead of next to one another as is typically done. The interpreter was positioned behind the child and slightly to the right to additionally see and voice the child’s communication. The bug-in-the-ear device used for live coaching was placed in the interpreter’s ear.
Adaptations to the CDI
Prior to conducting the didactic training with the parent, training was scheduled with the interpreter to introduce all the concepts of PCIT and provide detailed explanation of the goals of CDI. The interpreter was provided with all written materials, including rating scales and parent handouts so she would know what information the parent was to receive. We believed that teaching the interpreter core concepts served to communicate the spirit and purpose of PCIT, and eased the work of translating the information to ASL. Moreover, in our clinic, we sometimes use a PCIT didactic video that demonstrates the skills using parent and child examples. In this case, the video proved to be especially helpful as the family was already accustomed to a visual learning modality, and seemed to benefit from the additional visual demonstration of the strategies. Moreover, because interpreter preparation is such an important component to coaching, we used the same two interpreters for the family discussed in this study.
As the grammatical structure of ASL and English are different, parents were taught to sign using exact English signing. In other words, instead of using signs that conveyed a complete English sentence, the parent was taught to sign each word individually. For instance, when describing play, instead of signing “building tower” the parent was coached to sign “I see you building the tower,” “it looks like you are building a tower,” or “it seems like you are building a tower.” Similarly for praises, the parent was coached to specify whom the praise was for beyond providing a labeled praise. For example, instead of signing “good job in seat/chair,” the parent was coached to sign “I like the way you are sitting in your chair.” The use of a noun was an important additional element as it made the signed dialogue explicitly about the child and eliminated any confusion that the parent was merely describing the toys or play in general. It is important to point out that coaching the parent to use a specific code of communication is not unique to coaching DHH families. Hearing families are also taught a new mode of communication consisting of application of certain words and sentence structures intended to facilitate the application of PRIDE, which is a central set of strategies that are used to enhance the parent–child relationship. In fact, in our practice, parents often comment that applying the PCIT skills is like learning a whole new language for communicating with their child and requires them to exert greater conscious effort in choosing their words. And, as stated earlier, changes to PCIT should retain the central elements of the model (Eyberg, 2005), which include skilled parent verbiage that communicates tuned attending and reinforces desirable behaviors displayed by the child.
As we determined that shaping was particularly helpful in teaching the deaf child desired behaviors in a concrete and observable manner, we implemented play rules at the beginning of each session. Most sessions we maintained two basic rules: stay in your seat and keep the toys on the table. At each session, in addition to stating these two rules, the parent was coached to demonstrate the active ignore procedure to the child by standing up and sitting one seat over (empty seat next to the parent). The parent was instructed to sign “if you get out of your seat, I will stand up, sit here and play by myself, but when you are back in your seat then I can sit here (directly in front of the child) and play with you.” In other words, the parent was initially seated in front of the child and when actively ignoring moved sideways to the empty seat beside so that they were no longer in front of the child.
Adaptations to the PDI
For the parent-directed phase of PCIT, the aspects that remained the same include teaching “BE DIRECT” skills and compliance strategies. The acronym BE DIRECT stands for Be specific, Every command positively stated, Developmentally appropriate, Individual rather than compound commands, Respectful and polite, Essential commands only, Carefully timed explanations, and Tone of voice is neutral. The compliance strategies in turn consisted of timeout and removal of privileges sequences. Overall, the goal of coaching during this phase is to instruct the caregiver on strategies for giving clear and direct commands followed by praise for compliance, and teaching of compliance strategies for when the child does not comply with the command.
In PCIT, there are two commonly used time-out procedures (i.e., 3 minutes + 5 seconds of silence with an “if you don’t” warning, and the two-choice time-out). The family in this case study was taught the two-choice time-out procedure accompanied by a visual 5-second count before and after the two choices. We found that an additional benefit of the visual count was that it made the amount of elapsed time between command, choice, and consequence more obvious.
Emphasis was placed on commands given using a neutral tone—as in neutral body language, signs, and gestures. This skill proved to be of special importance for the deaf family because all the affect is communicated visually. The parent was taught to give single step directions and to state commands positively (e.g., please walk), instead of negatively (e.g., don’t run).
This phase also included use of pre-viewing and teaching of skills. Specifically, videos for Be Direct skills and Compliance Strategies were used with the interpreter and the parent.
In PCIT, “Mr. Bear” or another stuffed animal is often used to demonstrate PDI skills such as the direct command compliance sequence, and to demonstrate contingencies for going to time-out. Mr. Bear was also helpful in demonstrating use of choice making, mindfulness, and shaping strategies such as the use of “when-then.” In our work with this deaf family, we found that using Mr. Bear as a model was of greater help than the didactic followed by rehearsal alone. Mr. Bear served to concretely demonstrate the compliance and time-out sequences in the child’s primary learning modality. Whereas in hearing families Mr. Bear can be used to reinforce skills/behaviors, for deaf children Mr. Bear functions as a primary visual learning tool. Analogous to the treatment of hearing children, reinforcement occurs through repeated practice of the direct command and time-out procedure following each demonstration of noncompliance.
For the time-out procedure, we found that the two-choice timeout was more visual and communicated more clearly the result of the choice to comply and noncomply. Similarly, the two-choice removal of privilege also facilitated clear visual distinction between options. Presenting the child with the available choices also reduced the possibility that the child would infer incorrectly or fail to associate unwanted behaviors with the consequence. As in typical PCIT, once our parent was able to effectively use a counting/systemized time-out procedure, we then taught and rehearsed an automatic time-out for specific rule-breaking behavior. An automatic timeout is distinct in that when a child breaks a rule, the parent implements the timeout without warning and does not offer the child an opportunity to make a choice to comply—as the child has already made a choice not to comply with a pre-established rule.
7 Course of Treatment and Assessment of Progress
During the course of CDI, the mother was highly motivated to do homework and to practice PRIDE skills for 5 min daily with her son. She additionally cooperated with rehearsals and role-plays conducted during the session check-in. The mother first mastered use of behavioral descriptions and signing with enthusiasm, followed by imitation and reflection, and finally, labeled praise. In our experience treating many hearing families, we have found that behavioral descriptions are also typically mastered first. Given that this was one of our first DHH PCIT cases, it is hard to know whether this trend would hold true for other DHH parents. This parent’s experience revealed greater facility in recognizing her child’s actions and describing his behaviors with specific detail. Over the course of treatment, we saw a typical trend of skills development; that is, we observed an increase in the positive PCIT skills (i.e., praise, reflection, description) and a decrease in negative communication approaches (i.e., questions, excess commands, and critical statements; see Figure 1).
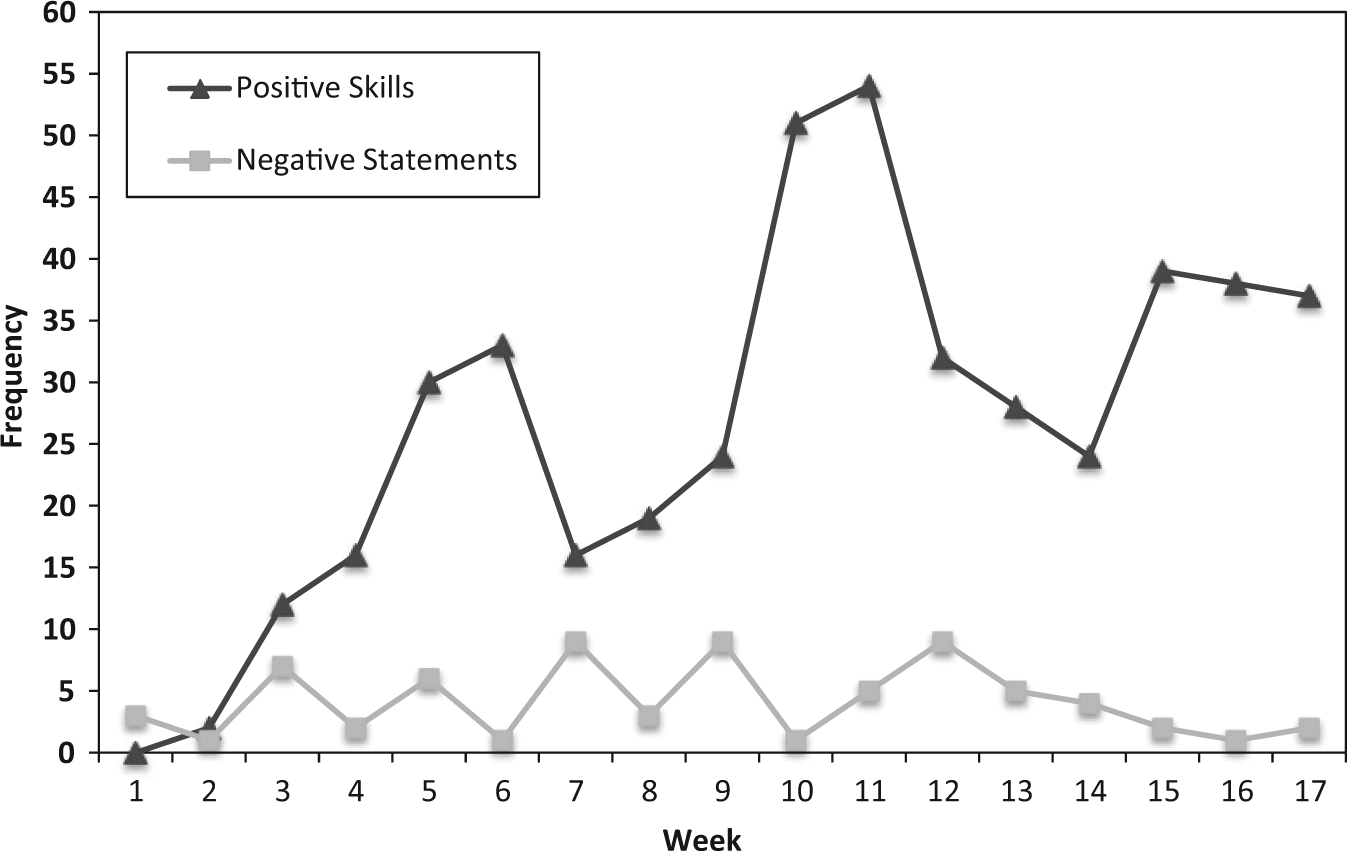
Weekly positive skills and negative statements.
Similar to hearing families, as the mother increased the frequency and quality of PCIT skills, her child demonstrated greater engagement in play and improved behavioral cooperation. Specifically, unlike in the beginning of therapy where the child played on his own and did not include his mother, by midpoint of treatment, the child was eagerly sharing about his play and involving his mother in the play and story sequences that he developed during the session. In turn, we observed the mother’s sense of reciprocal interaction also increase—she too demonstrated greater spontaneous interest in her child’s play and required less and less directive coaching to do so. In addition, by treatment midpoint, as the mother had consistently reinforced sitting in his chair, sharing toys, keeping the toys on the table, playing gently, and helping with cleanup, the child was conditioned and demonstrated these behaviors without prompting, but because he received positive attention for displaying these behaviors.
Once in PDI, the mother continued to apply relationship enhancement skills in session and for homework, while also adding new PDI compliance strategies. She shared with us that when she and the father introduced house rules to Sam, he smirked in surprise but was attentive. The mother was also able to learn and practice the time-out sequence during the didactic; she cooperated in rehearsing the sequence with Mr. Bear, and practiced time-out before session during the check-in with the interpreter and the therapist. Once in the session, she effectively modeled the time-out sequence with Mr. Bear and then subsequently applied it with her son. She grasped and applied single step, clear, and direct commands with relative ease. Once mastered in session, the mother implemented time-out in the home. She was also taught how to remove privileges in session by taking away prizes Sam had the opportunity to earn during each session. Similarly, once mastery was achieved at the clinic, the parent was asked to apply this skill at home independently and report back on what worked and what challenges she confronted. At check-ins and check-outs, the therapist and parent would then troubleshoot how to tweak anything that the mother may have been doing that was different from the protocol and therefore decreasing the strategies’ effect. Mastery of these skills allowed the mother to manage Sam’s behaviors not only in the home but also in the community, such as grocery shopping.
8 Complicating Factors
One of the main complicating factors in this case was the change in communication modality used for PCIT. Typically, PCIT coaching is accomplished through direct coaching in the parent’s ear. In this case, coaching was through a sign language interpreter and as such we had to consider potential therapeutic effects. Specifically, while the interpreter may aim to function as a facilitator of communication and avoid inserting their reactions and experience into the interaction, the impact of a third person in the room does influence the mood of the communication (Brunson & Lawrence, 2002). In a mental health environment, interpreters cannot perform the role of impartial or neutral conduits because they do influence the dynamic of the therapeutic relationship. Interpreters translate the cultural context for therapists, and in so doing can be more accurately described as “clinical collaborators” rather than simply interpreters (de Bruin & Brugmans, 2006).
Brunson and Lawrence (2002) conducted an investigation where they demonstrated that a triadic effect (i.e., therapist-interpreter-patient) is at work during therapeutic sessions. They describe the triadic effect as the resulting experience that occurs when communication flows from a therapist or patient through an interpreter. Their investigation revealed that as a result of the triadic effect, mood states in the interpreter were found to shift the mood of the deaf patient. Their study identified that a negative mood in the interpreter negatively affected the deaf patient’s mood. Similar to the experience of counselors, interpreters can be affected by therapeutic phenomena and may have counter transference feelings (Williams & Abeles, 2004). In fact, the triadic flow of communication makes it so that the interpreter is perfectly positioned in the transference crossfire. This is problematic because, among other reasons, while a therapist may be adequately trained and skilled at responding to transference and counter transference, interpreters are typically not, thus making them easy targets to the effects of transference phenomena (de Bruin & Brugmans, 2006).
Selection, training, and clinical collaboration with sign language interpreters are therefore essential prerequisites to planning for and implementing PCIT treatment. Readers should refer to the above sections on planning interpreting and PCIT coaching, and criteria and selection of interpreters.
9 Access and Barriers to Care
For the population that we serve, some of the common barriers to care include lack of transportation, economic factors (e.g., money for gas or public transit fares), housing, childcare for nontreated siblings, parent employment and their resulting availability to attend family sessions, the patient’s school schedule, and other less tangible factors that make families resistant to engage in treatment. DHH families have additional barriers to care that often include lack of an ASL-fluent practitioner, a trained ASL interpreter in the area where they live and are seeking services, and limited practitioner understanding of the Deaf culture.
The family in the present case study was offered access to PCIT treatment using an ASL interpreter. Issues pertaining to transportation and childcare were not a concern as the family owned a car and reported sufficient financial resources to allow participation in treatment. Sam’s mother is a homemaker and was able to attend treatment without conflicts with her employment schedule. The family was offered an appointment after school hours and the providing clinic’s childcare staff cared for the siblings while the mother was in the PCIT session with Sam.
10 Follow-Up
In contrast with her pre-treatment performance, Mrs. G appeared warmer and more focused on her child post treatment. For example, during the behavioral observation, she gave 10 labeled praises, 7 reflections, and 16 behavioral descriptions, and only 2 “don’t” behaviors. In spite of improved parenting skills, Mrs. G reported inconsistent improvements in child behavior problems and parenting stress on standardized assessments. She explained that because her husband had returned to work and her stress was much higher managing all the children, her stress levels had increased. Specifically, parental distress fell in the 95th percentile, Parent–Child Dysfunctional Interaction in the 93rd percentile, Difficult Child in the 84th percentile, and Total Stress fell in the 95th percentile. Similarly, the ECBI post scores were intensity T = 72 and number of problems T = 71.
Interestingly, Mrs. G’s description of the severity of the child’s symptoms on the Achenbach CBCL revealed significant improvements (similar to those observed in session); Internalizing T = 48, Externalizing T = 50, and Total Score T = 47. While the ECBI focuses on ordinary, difficult-to-manage behaviors (e.g., dawdling, fighting with siblings) that make home life stressful, the CBCL contains about three times as many symptoms of different disorders. It is possible that, overall, symptoms related to the child’s more severe mental health problems diminished as his mother’s parenting skills increased, while the fewer behaviors associated with family stressors and sibling relationships remained challenging.
11 Treatment Implications of the Case
The purpose of this case study was to demonstrate how PCIT, an established evidence-based treatment, could be adapted to help DHH families improve their parent–child relationships and behavior. It also explained how sign language interpreters could be used to bridge the communication between the hearing therapist and the DHH family in treatment. The interpreters used should be fluent in ASL, preferably with certified skills, as this proved beneficial to facilitating the treatment. Moreover, introducing the interpreter to PCIT and preparing them for the unique aspects of the modality such as the bug-in-the-ear and live coaching of disruptive behaviors is also important. Much was also learned about how the PCIT treatment room could be organized to place the interpreter in the room while also promoting fluid coaching through the therapist behind the one-way mirror.
The effect on the child and the mother in this case was positive and reported by both parents as helpful in teaching them parenting skills and improving their child’s behaviors. Specifically, the mother reported feeling more prepared to manage her son’s behaviors and expressed that she valued learning how to play with her child in a way that was fun and taught him new behaviors. The father, though not directly involved in PCIT treatment, also shared that he noted more cooperative and obedient behaviors in Sam toward him and the mother.
Sam for his part was observed to be very compliant, cooperative, and eager to earn praise and positive attention by the end of treatment. In comparison with his baseline behaviors in the clinic and at home, he displayed greater engagement and communication with his mother, and stopped displaying the initial presenting problems that involved tantrums, talking back, and disobedience toward his parents. In addition, his parents reported that his behavior at school was also improved as they noted that Sam no longer received behavioral referrals.
In the future, the next challenges for clinicians and researchers pertain to access for populations that have historically not participated in the initial stages of dissemination of empirically supported treatments. Usually, access for diverse populations is postponed until later stages of evaluation and dissemination. Our findings demonstrate that DHH providers (hearing and ASL fluent) should be attempting, identifying techniques, testing them out, and working through strategies for application of language-loaded clinical treatment models with DHH patients.
We learned that DHH may truly only be a difference and not a disability in terms of utilizing PCIT intervention. Across hearing and DHH parents similarities included the ability to attend to positive behaviors and bring attention to them with words/signs that serve to reinforce and increase specified behaviors. Moreover, application with this DHH family taught us that stating clear commands and having predictable responses for noncompliance works to shape child behaviors not only in auditory languages, but visual languages like ASL too.
We also came to appreciate how verbally loaded our interventions are and how much hearing and verbal communication is used as the primary mechanism of change. Our experience taught us that hearing and verbal communication are not the sole instrument by which change interventions can be implemented; with some basic DHH-oriented modifications PCIT, and we suspect other evidence-based approaches, can be applied to improve child functioning and parenting skills in DHH families.
Clinically, while we dared to attempt PCIT with this family, we were really concerned that due to the extra step of interpreting, coaching would be delayed, and take too long to allow for real in-the-moment coaching. Especially given that live coaching with parent and child present is one of the key distinguishing features of PCIT. We learned that to increase flow, preparation is essential. Moreover, the PCIT didactic process took a little longer and involved more rehearsal before entering into live coaching. Once a coaching synchrony was achieved between the coach, interpreter, and the parent, an equally fluid coaching flow occurred. In fact, the coaching flow with the interpreter still allowed for good in vivo pacing and timing, and for effective parent feedback and correction.
Theoretically speaking, we affirmed with yet another diverse population that the core PCIT principles outlined by Eyberg of nurture and consistent limit setting hold true—even when the mode of communication is entirely visual. Our experience provides further evidence that PCIT is such a robust treatment for externalizing behaviors that the coaching mode can be changed from verbal to nonverbal with improvement still measurable qualitatively and quantitatively.
Be it only one example requiring replication, the deaf parent in this study showed that differences in language were differences in language, but not differences in key parenting approaches that work to modify child behaviors. In sum, this case study provides one example of how PCIT was effectively used to improve parenting self-efficacy, child behaviors, and parent–child interaction in a DHH family.
12 Recommendations to Clinicians and Students
This article is a first step in identifying ways to adapt an intervention from the hearing population to the DHH population. It highlights the effect of PCIT on one family with a deaf mother and a hard of hearing child. As many more deaf children have hearing parents, perhaps the approaches would need different modifications if the parents were hearing. This study involved a mother and it is possible that coaching of fathers who are DHH or have a DHH child would yield different results. While our experience working with interpreters in PCIT was positive, to our knowledge no studies have evaluated the effect of interpreters on PCIT. In addition, it is possible that ASL-proficient PCIT therapists/coaches would prove more effective and/or efficient in the treatment of this population. Moreover, a DHH and ASL-fluent therapist may be more culturally congruent and sensitive to the clinical needs of DHH persons. This said, given the overall shortage of ASL-fluent mental health providers, effective use of interpreters would likely result in more service access for DHH families.
Future research can evaluate more case studies with families of diverse hearing status (e.g., hearing mother, DHH child, or hard of hearing parent and a hearing child), and evaluate application of PCIT in larger samples of DHH dyads, thereby further assessing the efficacy of PCIT for treating DHH children and their caregivers. An interesting and valuable course of inquiring may be evaluating the transfer of hearing interventions to the DHH community and how such attempts are viewed and received by the DHH community. Finally, more research is needed assessing the application of other evidence-based mental health modalities in the treatment of underserved populations like DHH.
Footnotes
Acknowledgements
This work is a product of the support of many. I am abundantly grateful to the family in the study; Susan G. Timmer, PhD, for her mentorship and research expertise; Nancy Zebell, PhD, for outstanding training and guidance in PCIT; Tay Sandoz, PsyD, for his insightful clinical direction and supervision; Lori Pack, LCSW, for her leadership and vision for PCIT; to my group of clinical and research interns for joining me on each project and task; and to sign language interpreters for their invaluable work. A very special thanks to Patrick Brice, PhD, at Gallaudet University for his expert feedback on all things DHH. To my husband George Shinn III for his incessant love and support, thank you.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.