
Abstract
There are few proven effective treatments such as Parent–Child Interaction Therapy (PCIT) for use with deaf parents and their children, even though it is likely that the prevalence rate for disruptive behavior problems including attention deficit/hyperactivity disorder (ADHD) and oppositional defiant disorder (ODD) are similar to those reported for all U.S. children. Medication and behavioral therapy involving parents comprise the cornerstone for ADHD/ODD management, with PCIT endorsed as one of the most effective interventions available for children aged 2 to 7 years. This case study presents the implementation of PCIT with deaf parents and their 7-year-old hearing son with ADHD/ODD, with the help of a certified interpreter and readily available video technology. Findings from this case report documented PCIT as a promising treatment option for use with individuals who are deaf.
1 Theoretical and Research Basis for Treatment
Attention deficit hyperactivity disorder (ADHD) is one of the most common behavior disorders in children and adolescents, affecting more than 5 million U.S. children, with boys more than twice as likely to have ADHD as girls (Center for Disease Control and Prevention, 2010). ADHD is marked by symptoms of inattention, hyperactivity, and impulsivity, which are evident from the early childhood years and may persist into adulthood, and affect one’s ability to function in home, school, and community settings (American Psychiatric Association, 2000). The most prevalent co-occurring disorder with ADHD is oppositional defiant disorder (ODD), which appears 41% of the time (Elia, Ambrosini, & Berrettini, 2008). ODD symptoms include behaviors that are viewed as more negative, hostile, and defiant, and as such may interfere with functioning at school and disrupt family relationships (American Psychiatric Association, 2000).
Upward to 75% of those children diagnosed with ADHD receive stimulant medication treatment, especially those who also showed symptoms of ODD. Behavioral parent training interventions which help parents learn to more effectively manage their child’s behavior by promoting a positive and caring relationship and using effective discipline strategies are also effective in managing ADHD and ODD symptoms and, when combined with medication, are more effective than either medication or behavioral therapy alone (Charach et al., 2011; Gale, 2010).
Children with parents who are deaf are thought to have similar risk for ADHD/ODD as their peers with hearing parents; however, deaf parents may have reduced access to treatments on effective parenting skills, and fewer treatments have been shown to be efficacious for this population (Singleton & Tittle, 2000). This means that their children with disruptive behavior disorders including ADHD/ODD may be at a disadvantage with respect to accessing non-pharmaceutical interventions, such as parent training (Charach et al., 2011). Deaf parents are likely to be as vulnerable as hearing parents to life stressors that affect family functioning and child behavior, but have less access to empirically validated services that would benefit their entire family (Singleton & Tittle, 2000). Therefore, it becomes essential for providers to make the necessary adaptations and reduce barriers to provide effective services for deaf families.
Parent–Child Interaction Therapy (PCIT) is an evidence-based treatment for children between the ages of 2 and 7 years with disruptive behavior disorders (Bagner & Eyberg, 2007; Charach et al., 2011; Hood & Eyberg, 2003). Parents/caregivers are taught specific skills through didactic sessions and are coached in real time during play interactions with their child. PCIT emphasizes changing negative parent/child interactions by enhancing the parent/child relationship and improving child behavior management skills. Studies have documented improvement in the quality of the parent/child relationship, decrease in child behavior problems and increase in prosocial skills, development of positive discipline skills, and decrease in parenting stress as a result of PCIT intervention.
PCIT uses a two-stage approach to improve the parent/child relationship and discipline methods. These stages are referred to as Child Directed Interaction (CDI), which teaches parents to pay attention to and reinforce their child during play, and Parent Directed Interaction (PDI), which helps parents give effective commands and consistently follow a discipline sequence (Eyberg & Funderburk, 2011). Unique to PCIT is the use of the “bug-in-the-ear” technology, which enables the therapist to provide real-time coaching to the caregiver while he or she is engaging with and/or managing the child. Parents move from the CDI to the PDI stage based upon mastery of key skills, and generally lasts 12 to 20 weeks (National Child Traumatic Stress Network, 2004). Parents are taught broad classes of behavioral antecedents and response behaviors that are uniquely tailored to their ability level and child’s need (Eyberg & Funderburk, 2011). As such, the parent in PCIT becomes the agent of change, which results in more enduring and positive child outcomes (Horner, Carr, Strain, Todd, & Reed, 2002).
Parent progress is monitored at each visit following a formalized coding system called the Dyadic Parent–Child Interaction Coding System (DPICS; Eyberg, Nelson, Duke, & Boggs, 2004), while child behavior change is documented by weekly parent ratings on the Eyberg Child Behavior Inventory (ECBI; Eyberg & Pincus, 1999). Other assessment instruments such as the Achenbach Child Behavior Checklist/Teacher’s Report Form (CBCL/TRF; Achenbach & Rescorla, 2000) and Sutter-Eyberg Student Behavior Inventory (SESBI; Eyberg & Pincus, 1999) may be used as desired, but are not needed for PCIT progress monitoring. PCIT also includes a parent-report measure of consumer satisfaction called the Therapy Attitude Inventory (TAI), which may be used at post-treatment (Brestan, Jacobs, Rayfield, & Eyberg, 1999).
PCIT was initially targeted for families with children aged 2 to 7 with oppositional, defiant, and other externalizing behavior disorders, and has been successfully documented for its use with children with chronic illness (Bagner, Fernandez, & Eyberg, 2004), children with anxiety disorders (Chase & Eyberg, 2008), and very young children (Gallagher, 2003), among other clinical use. PCIT has been adapted to treat children with Asperger’s disorder (Armstrong & Kimonis, 2012), children with depression (Lenze, Pautsch, & Luby, 2011), and children with callous-unemotional traits (Kimonis & Armstrong, 2012). PCIT has been successfully implemented with mothers with ADHD (Zisser & Eyberg, 2012), mothers with mild intellectual disabilities (McDiarmid & Bagner, 2005), parents who were physical abusers (Chaffin et al., 2004), immigrant families (Pearl, 2008), families with domestic violence (Borrego, Gutow, Reicher, & Barker, 2008), and parents who are Spanish speakers (Borrego, Anhalt, Terao, Vargas, & Urquiza, 2006). However, no studies of PCIT adaptations with deaf families have been published to date.
With these issues in mind, we describe the use of PCIT with a 7-year-old hearing boy presenting with comorbid ADHD and ODD and his mother who is deaf, and communicated via American Sign Language (ASL) with her child. Taking the child and his parents’ unique circumstances into consideration, PCIT was tailored to ensure appropriateness and generalizability (Eyberg, 2005), which will be described in greater detail below, and included the support of a certified interpreter and video technology. Preintervention measures (ECBI/SESBI; CBCL/TRF) were completed by the child’s mother and his teacher 2 weeks prior to beginning therapy, and the same measures were completed 1 month after the last visit and again at 3 months follow-up. Throughout the 13 treatment sessions, progress was monitored using the DPICS coding and ECBI.
2 Case Introduction
Michael (name changed for confidentiality) was a 6-year-old hearing son of deaf parents, treated at a university medical center for ADHD by a psychiatrist fluent in ASL. While Michael responded well to stimulant medication at school, he had become increasingly more difficult for his parents to manage at home. Michael’s behaviors had escalated to include refusals, defiance, arguing, and even striking his mother. He would call his grandparents (who often cared for him) to complain about his parents and his grandparents frequently sided with Michael. Almost 7 months elapsed from the time of Michael’s referral to our PCIT clinic and beginning treatment, because his grandfather was diagnosed with cancer, and died, which added an additional stressor to this already challenging situation.
3 Presenting Complaints
Michael became more challenging for his mother to manage following the birth of her daughter, now 3 years old. During this pregnancy, mother was placed on bed rest in the hospital for 2 months, and Michael was cared for by his grandparents, who were Spanish speakers. When mother was well enough to care for Michael, he became increasingly more irritable and non-compliant. In addition, he refused sleep in his own bed, insisting that he needed to sleep with his mother, just like his baby sister. Michael became anxious and upset whenever his mother left him even for short trips to the store. He complained of headaches and stomach aches, would not eat fruit or vegetables, and refused to drink water. Michael also became increasingly sad about his grandfather’s demise, but would not open up about it to his mother. He exhibited communication challenges such as refusing to face his parents when they would redirect his behavior using ASL. Eye contact is critical in communication in the Deaf community. Michael found an effective way to avoid engaging when being redirected by refusing to make eye contact. He also would at times use very limited sign language to communicate his frustration to his parents, making communication a further challenge in this family.
4 History
Michael was born 5 weeks early, and spent 5 days in the newborn intensive care unit before he was released from the hospital. At 8 months of age, Michael was hospitalized for a collapsed lung, but has otherwise been healthy. He struggled with falling asleep independently and was described as a picky eater, who refused most vegetables and fruits. His developmental milestones were achieved on time, and he was evaluated for placement in the Gifted program at his school. Michael’s achievement in both math and reading were exceptional, but he had difficulty paying attention. At age 5, he was diagnosed with ADHD, and began taking Concerta, which seemed to help him focus his attention at school. Michael’s parents reported that he was fluent in English, Spanish (grandparents spoke Spanish), and ASL.
5 Assessment
Physical, psychological and neurological assessments, and behavior observations were conducted by a specialty team of pediatric providers, and included a physical, psychiatric, and neurological examination. These data are not presented in this article. In addition, standard behavior rating scales were obtained from his mother and classroom teacher, which are discussed in this article and shown in Table 1.
Pre-Post Assessment and 3-Months Follow-Up Results for CBCL/TRF.
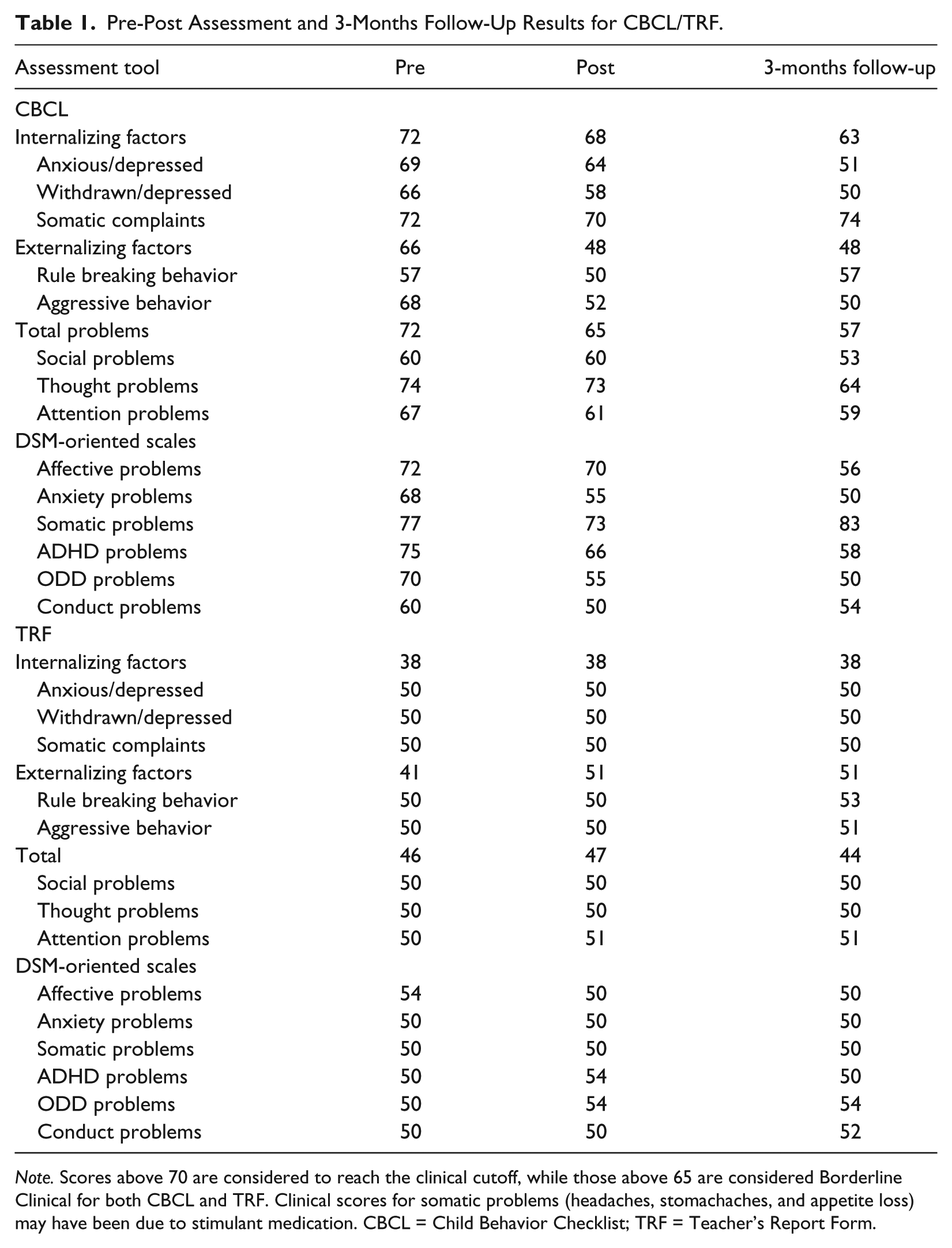
Note. Scores above 70 are considered to reach the clinical cutoff, while those above 65 are considered Borderline Clinical for both CBCL and TRF. Clinical scores for somatic problems (headaches, stomachaches, and appetite loss) may have been due to stimulant medication. CBCL = Child Behavior Checklist; TRF = Teacher’s Report Form.
Behavior rating scales completed at the beginning and conclusion of PCIT intervention and again at 3 months post-treatment follow-up included the CBCL/TRF (Achenbach & Rescorla, 2000) and the ECBI/SESBI (Eyberg & Pincus, 1999). The CBCL/TRF is a standardized assessment system that is used to measure various aspects of behavior and personality, including competencies and behavioral or emotional problems. T-scores with a mean of 50 and standard deviation of 10 are used to identify behavior problems relative to a standardization sample, and scores above 70 are considered to reflect a risk for behavioral health problems. Scores are summarized into Total Problems, Internalizing Problems, and Externalizing Problems, Syndrome Scales, and DSM-oriented Scales.
Pre-treatment CBCL ratings indicated significant risk for behavioral health problems related to affective problems, anxiety problems, pervasive developmental problems, attention deficit/hyperactivity problems, and oppositional defiant problems. Michael’s T-scores declined over course of intervention, with the biggest declines for CBCL ratings of Aggression, Attention Problems, Anxiety Problems, Oppositional Defiant Problems, and Conduct Problems. With the exception for parent ratings for Somatic problems, all of these subscales were in the non-clinical range at post-treatment, and again at 3 months follow-up. Scores from his teacher’s ratings on the TRF were non-clinical and remained consistent from pre to post-assessment, presumably because the medication was effective in controlling Michael’s ADHD symptoms during school hours.
The ECBI was used to assess the intensity of the disruptive behavior and caregiver perceptions regarding how problematic the behavior is to him or her. The ECBI was completed on a weekly basis by Michael’s mother during the course of PCIT, at 1-month post-treatment, and at 3-month follow-up. The teacher’s version of this tool, the SESBI, was used at PCIT Week 1, after Week 13 (i.e., post-treatment), and at 3 months follow-up. ECBI scores for Intensity and Problem scales are represented as T-Scores, with scores at or above 60 considered to be clinically significant. Michael’s ECBI scores declined from 82 to 45 for Intensity, and 77 to 41 for Problem, indicating significant improvement over the course of PCIT treatment and into follow-up. SESBI scores were non-significant at the onset of PCIT training and did not change. Data from the CBCL/TRF and ECBI/SESBI are summarized in Tables 1 and 2, and ECBI scores for each of the weeks in PCIT intervention are shown by Figure 1.
Pre-Post Assessment and 3-Months Follow-Up Results for ECBI and SESBI-R.
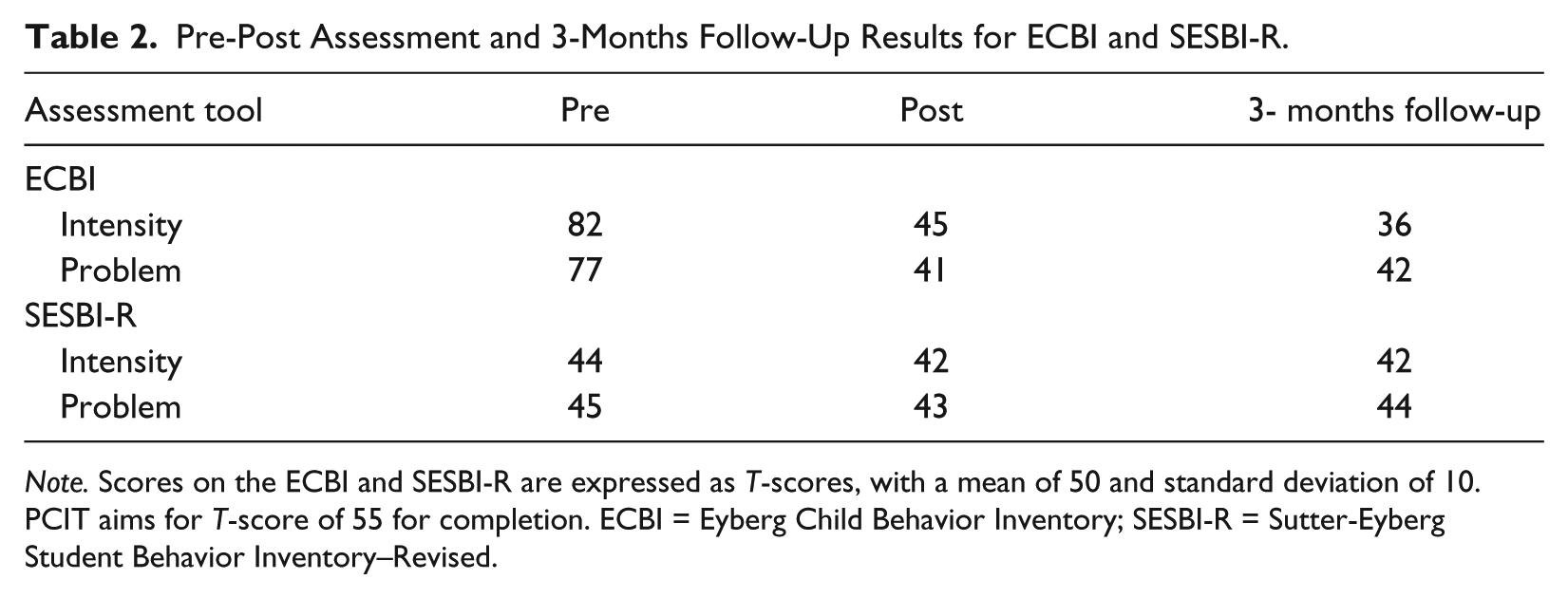
Note. Scores on the ECBI and SESBI-R are expressed as T-scores, with a mean of 50 and standard deviation of 10. PCIT aims for T-score of 55 for completion. ECBI = Eyberg Child Behavior Inventory; SESBI-R = Sutter-Eyberg Student Behavior Inventory–Revised.

Mother’s ECBI ratings for intensity and problems over the course of the intervention and at follow-up.
6 Case Conceptualization
Michael’s behavior problems were defined through developmental history, observations, interviews, and standardized behavior rating scales completed by his mother and teacher. Michael’s problem behaviors included annoying others, disobedience, hitting, destroying property, and running away. These problems occurred at home and in community settings, and he was more disobedient with his mother than with his father or other caregivers, per his mother’s report. The perceived function of his behavior was to gain mother’s attention, to access control or power, to avoid non-preferred activities, and to express his anger and/or frustration. Our goal with Michael was to teach him to obtain mother’s attention with appropriate behavior, follow adult directions, and use appropriate communication when he was upset rather than engaging in temper tantrums or hitting. Our goal with his mother was to help her learn to reinforce Michael’s appropriate behavior, ignore his inappropriate behavior when possible, and use a consistent discipline plan when needed.
PCIT was selected as the intervention plan because of the evidence for this approach in treating young children with disruptive behavior problems (Bagner & Eyberg, 2007; Eyberg, Nelson, & Boggs, 2008). Michael’s attachment to his mother appeared to be insecure, stemming from their earlier separation, daily negative interactions, and inadequate behavior management. His mother reported personal stress related to Michael’s behavior and understood the commitment that this approach would require of her which included weekly visits to our clinic and daily practice at home. However, we did not have a PCIT therapist fluent with ASL, meaning that accommodations would be needed in order for this family to access treatment. It was determined that an ASL interpreter and video technology would be the appropriate accommodation for this therapy to be utilized with a deaf parent, and services were secured from an interpreting agency.
7 Course of Treatment and Assessment of Progress
Michael and his mother were seen in weekly, 60-min sessions which were over the course of 4 months for a total of 13 sessions, of which Michael attended 11. Due to holidays and illness, there were gaps of 2 weeks between some coaching sessions. In each of these sessions, an interpreter also attended, and we utilized a readily available video communication application (VCA) downloaded onto two tablet devices during coaching sessions: One device was utilized with Michael and his mother, and the other device was kept in the observation room with the therapist and interpreter. The therapist stood next to the interpreter, who translated Michael and his mother’s communications (which included ASL, plus vocalizations), and then communicated the therapist’s feedback with ASL via the VCA. The interpreter was available for all feedback and training sessions with the mother and therapist, as well as for all feedback sessions that were held without Michael. Handouts from the PCIT manual were provided to reinforce skills.
PCIT progresses through the two distinct phases, which are divided between relationship-building skills (CDI) and positive discipline and compliance (PDI). Included in the 13 sessions were 2 sessions that his mother attended without Michael for the purposes of learning the skills involved in CDI and PDI. The first parent-only session was dedicated to rapport building, and teaching core CDI concepts and skills. Homework sessions of 5 to 10 min per day are part of this treatment, and were documented via a homework sheet handout, in which parent checks whether or not they completed 5 min of special play for each day over the course of the week. Michael’s mother returned 9 homework sheets, indicating that they had practiced special play on the average of 3.2 times per week. Handouts taken from the PCIT manual were also provided on other helpful topics, such as strategies to generate more effective praise and examples of all CDI skills; however, we did not evaluate the effectiveness of this advice.
During the first CDI phase of PCIT, parents learn to follow their child’s lead during play, and reinforce their child’s behaviors through the use of relationship-building skills. These skills are captured in an acronym: PRIDE, which stands for Praise, Reflection, Imitation, Description, and Enjoy. Parents are taught not to give commands, ask questions, or use negative talk, as those responses may reduce child compliance and self-esteem as well as prevent the child from leading the play. PRIDE skills are coded during a 5-min coding period at the beginning of each session to determine parent’s skill mastery of labeled praise, reflections, and behavior descriptions. Planned ignoring is recommended for use in response to mildly inappropriate behaviors such as whining or bossiness, while aggressive or destructive behavior results in cessation of special play for that day. Parent’s competence with using these core skills are thought to foster greater attachment and parent–child warmth, and increase child compliance (Eyberg, Boggs, & Algina, 1995).
The clinician follows the structured PCIT manual, which describes each session and coaching skills to be utilized. The goal of the sessions is to shape the parent’s verbalizations and behavior during the play with their child via the use of positive reinforcement delivered by the coach/therapist. Parent’s skill mastery is defined as 10 labeled praises, 10 behavior descriptions, and 10 reflections coded within this observation period, after which the therapy may proceed to the next phase.
During the PDI phase, parents learn to use effective discipline strategies that include effective delivery of commands, appropriate response to child compliance, and strategies to increase compliance. Parents are encouraged to gradually apply PDI skills to other situations, such as the clinic waiting room or playground, in the home, and in public settings. Coding of skills continued in the therapy sessions, and were graphed to provide the parent with feedback about their progress and skill mastery. Coaching continued, via VCA with communication between parent and therapist being facilitated by the interpreter. Due to the delay of relaying the information from the therapist to the parent via video, it was often observed that the parent self-corrected behaviors before the prompt was relayed. For example, mother might pose a question, realize it, and changed the question to a statement before the interpreter provided corrective feedback. Mastery of PDI is reached when 75% of parent’s commands are effective meaning that commands are direct, positively stated, and so on, labeled praise for compliance is provided when child complies, and the discipline sequence is followed in cases of non-compliance. As with CDI, homework and handouts from the PCIT manual were provided to enhance skill mastery.
The therapist met with Michael’s mother and interpreter, to review the skills involved with PDI. Effective commands were modeled, practiced, and reinforced by the therapist via the interpreter. A discipline protocol was introduced, which could result in time out for non-compliance, and always labeled praise for compliance. At the following session, a role-play was used to demonstrate the PDI procedure to Michael. Michael learned to comply with his mother’s effective commands quickly, and only once, needed to be in the time out chair during clinic sessions. Likewise, PDI proved to be effective with Michael when implemented at home during special play time, and later, used within his everyday routines. Each week, his mother was asked to document how well PDI worked during the week. Michael’s non-compliance at home resulted in occasional time out chair and time out room consequence, but by the third week of implementation, he complied with his mother’s commands or, at the very least, complied when given the chair warning.
8 Complicating Factors
Once treatment began, we noticed that Michael spoke very little to his mother, and when he did, whined or used minimal ASL, which made it difficult for both mother and the interpreter to understand him. When his mother was not present, Michael had no difficulty expressing himself in English. Later on in this process, his mother told us that Michael shared with her that he was embarrassed to sign in front of other people, and was sad that she was deaf.
Another challenge was the placement of the tablet device in a visual line of sight for Michael’s mother. The tablet was placed on the floor during the therapy sessions; however, as PCIT is predominantly a “play” therapy, the device was occasionally obstructed, requiring repositioning which sometimes delayed communicating the coaching statement to the mother. In addition, lighting in both rooms was occasionally an issue, though this was a bigger challenge for the interpreter, as the room behind the two-way mirror must be kept dark in order to minimize the child’s view of the therapist.
We also discovered that there were inherent differences between ASL and spoken English, which became challenging for both mother and the therapist during coaching and coding sessions. For example, in ASL, one might sign GREEN TRUCK, which can be interpreted as “That’s a green truck” or “You have a green truck.” The interpreter was able to provide information about ASL structure and grammar, which then allowed Michael’s mother and the therapist to discuss how she might be able to expand her statements to match PCIT criteria.
We were greatly concerned about the immediacy of the coaching feedback with respect to strengthening CDI skills (Cooper, Heron, & Heward, 2007), given that there would be lapse time between mother’s response and our feedback to her. However, the delay between mother’s response and our feedback via the tablet device did not seem to affect her rate of learning the CDI skills. As per PCIT recommendations, we employed a continuous reinforcement schedule and extra practice examples as needed to strengthen mother’s desired CDI skills.
Using this readily available technology enabled us to offer this innovative approach with a family who might otherwise not be able to receive the benefit of PCIT. However, technology is not without its challenges. We learned (the hard way) to have an extra tablet device and extra charging cords on hand, in case the battery wore out, as it did in the middle of one coaching session. There were occasional problems with connecting to the internet because of the firewall protection in our building, which we were able to solve with our technology support. Finally, we worried that Michael might become rough with the tablet (especially during PDI), which was his mother’s connection to the coach, but thankfully he never did, and in fact, after a few sessions, the device lost its novelty much as the Bluetooth earpieces our hearing parents use during coaching sessions. In the future, we plan to mount the tablet on a wall, to prevent any possible problems that might occur.
9 Access and Barriers to Care
There were several barriers to care, among them no trained PCIT therapist fluent in ASL in the geographical area, father’s work hours, family’s commuting distance to the clinic, and the death of Michael’s grandfather right before PCIT was to be initiated. As we did not have a trained PCIT therapist who was fluent in ASL, interpreting services would be required for each session. In addition, PCIT use has never been documented for the Deaf, and we were concerned about how necessary adaptations and the time lapse between the parent’s response and coaching support might affect outcomes. We consulted with Dr. Shelia Eyberg, founder of PCIT, for her advice and she encouraged us to proceed with this study (S. Eyberg, personnal communication, September 27, 2012).
Michael’s father wanted to participate in PCIT but only could come to two sessions due to his extended afternoon and evening work schedule as an executive chef. At those sessions, he watched Michael and his wife through the one-way mirror, but did not wish to participate in the coaching session. Michael’s mother agreed to attend all of the therapy sessions and later teach her husband the skills that she learned, and father agreed to practice the skills as often as he could, given his work schedule which meant he rarely was home when Michael was awake. The treatment team extended an offer to Michael’s father to attend a coaching sessions at a more convenient time for him, but unfortunately his work obligations were an obstacle to his consistent participation in coaching sessions. We did not have an opportunity to observe Michael’s interactions with his father.
Unfortunately, PCIT is not readily available in many rural communities, meaning that this family commuted 2 hr each way when they came for therapy sessions at the university clinic. With 4 hr spent on driving, plus an hour of PCIT treatment, Michael missed school 1 day each week. Even so, Michael and his mother came reliably to each session with the exception of one due to the child’s illness, and twice, due to holidays. We found that communication regarding change in appointment times and mode of communication was best held ahead of time, and the use of confidential email proved to be most effective in communication about rescheduled appointment date/time.
Access to care was greatly enhanced by the use of the same interpreting team throughout all of the therapy sessions. There were two interpreters on the team, one primary and one backup. This allowed the mother and primary interpreter to build an agreed upon set of signs to be used during the therapy. The second interpreter attended and observed a therapy session before interpreting a session, in order to become familiar with the setting and the terminology used. It is strongly suggested that continuity of interpreters be considered a necessity for success with this therapy, especially in light of the importance of terminology used (e.g., PRIDE skills) during PCIT.
Not only did the interpreter become more familiar with the family, treatment protocol, and technology, she was able to make suggestions that improved our service delivery to this family. For example, she helped us with room arrangement that allowed us to face and speak to the parent, while she interpreted seated behind us, to improve the interaction. She also arranged the room for the coaching sessions so that we could clearly see Michael and his mother, and so that Mother could see the tablet, without it distracting Michael too much. The interpreter also helped us understand some of similarities and differences between ASL and spoken English, so that we could adapt our training to overcome communication or cultural barriers. The interpreter’s contributions in this situation illustrate the importance of the interpreter’s role as a member of the health care team in delivering mental health services to deaf individuals.
10 Follow-up
Follow-up data were acquired at 1- and 3-month post-treatment. In addition to a parent interview, ECBI/SESBI and CBCL/TRF ratings were repeated, and are presented in Table 1. Michael’s mother and father reported sustained improvement with Michael’s behavior and compliance at home, and his behavior at school remained positive over the course of the school year. Although Michael’s teacher never endorsed challenging behavior issues, she verbally reported that Michael had gotten “better” over the year, describing him as a hard worker, but who could become easily distracted and liked to talk when others were working. She also mentioned that Michael was very well-mannered and enjoyed helping others. Michael continued to excel academically and had few behavioral issues at home or at school.
11 Treatment Implications of the Case
There are few proven effective psychotherapeutic treatments for use with deaf parents and their children. This case study described how an empirically supported intervention, PCIT, could be adapted to treat disruptive behaviors in a young hearing child with ADHD/ODD whose parents were Deaf. Given the prevalence of deaf parents with children who may have ADHD and/or other disruptive behavior disorders, and limited access to quality mental health services, efforts made to incorporate their language, cultural practices, and values into PCIT are critical (Singleton & Tittle, 2000). When it is not possible to find a trained therapist to deliver direct services to deaf individuals, the National Association for the Deaf (NAD) recommends collaboration with a qualified sign language interpreter (NAD, 2012). As with caregivers in general, PCIT can provide deaf parents with the knowledge and skills to effectively implement behavior management principles that improve relationships, parenting skills, and child behavioral functioning. Given the evidence that supports the use of behavioral interventions for children with ADHD and/or ODD and the high prevalence for this disorder, PCIT should be made available to deaf families, with a qualified sign language interpreter when needed.
12 Recommendations to Clinicians and Students
This case study supported the effectiveness of adapting PCIT for use with deaf parents and a child with ADHD/ODD. In this case, PCIT was effective in reducing disruptive behavior at home and increasing compliance with parents, and served to improve the parent–child relationship. PCIT utilizes behavioral technology to help parents pay attention to their child in a way that strengthens their relationship and builds child confidence and self-esteem. When children misbehave, parents are better able to consistently and calmly manage the misbehavior. As a result, both parent and child become more relaxed and better able to cope with the frustrations of daily life. In Michael’s case, his emotional outbursts were greatly reduced in response to his mother’s focused attention on more positive and adaptive behaviors. In addition, Michael’s mother became more attuned to Michael and his need for her positive attention. She stated in a note sent to our team “Our progress is getting so much better every day. I am spending more time with Michael after school.”
Future studies using PCIT with deaf families might wish to consider pre-intervention training in Deaf culture and the structure of ASL for the therapists involved in the interaction (Hamerdinger & Karlin, 2003). Again, we wish to emphasize the importance of interpreter continuity to the success of the interaction when the therapist is not fluent in ASL. Allotting time for the interpreter and deaf client to develop signs for stage-specific vocabulary is also critical. In addition, providing copies of all printed materials to the interpreters prior to the session allows them to be adequately prepared to have their interpretation support the therapist’s goals.
Absolutely critical to the success of this therapeutic intervention was the use of technology. Fortunately, the mother, interpreter, and therapist all had access to the same tablet device (an Apple iPad) with the same VCA (Face Time). It is expected that a variety of devices and software applications would be able to produce the same functionality.
Because there are very few published studies examining the effects of psychotherapy or parent training with individuals who are Deaf, continuing research is critical toward documenting how to best serve and support for this population. We appreciate the willingness of this family to share their story, and encourage other practitioners who work with the Deaf to consider publishing their research. Finally, we found that PCIT was an extremely beneficial intervention, when implemented by a collaborative health care team in which the interpreter was a core partner.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.