
Abstract
Clients who present to psychotherapy reporting diffuse and/or sub-clinical concerns may provide a puzzling treatment decision for providers of evidence-based practice. The current case study illustrates the implementation of an evidence-based treatment, Acceptance and Commitment Therapy (ACT), for a client diagnosed with adjustment disorder with mixed anxiety and depressive symptoms. ACT targets a dimensional, transdiagnostic construct known as psychological flexibility, currently conceptualized as involving six inter-related behavioral repertoires. The client was a Caucasian woman in her 30s who self-referred to therapy. She reported feeling anxious and depressed, especially in regard to interpersonal difficulties with her mother and her ex-husband. Fourteen sessions of an ACT protocol emphasizing a modular approach to the repertoires emphasized by the psychological flexibility model were provided. Each modular session consisted of psychoeducation, metaphors, experiential exercises, and daily practice assignments for one of the repertoires. The client completed pre-treatment, post-treatment, and 6-month follow-up outcome measures and weekly process measures to track change throughout treatment. One process measure assessed each of the six repertoires. The client’s data revealed substantial increases in psychological flexibility and decreases in psychological distress from pre- to post-treatment, which remained stable at follow-up. This case report suggests that ACT may be a desirable treatment option for clients bearing ambiguous or sub-clinical presentations, including interpersonal conflicts. The report also provides a model for monitoring change with individual psychological flexibility repertoires with respect to a modular approach to teaching those repertoires.
Keywords
1 Theoretical and Research Basis for Treatment
Ambiguous clinical presentations may present as a challenging treatment decision for practitioners who wish to provide evidence-based interventions. When symptoms cluster around specific Diagnostic and Statistical Manual of Mental Disorders (DSM) categories, choosing an empirically supported treatment package may be a relatively straightforward decision. For example, a client presenting with complaints of persistent sadness, diminished pleasure, self-criticism, and changes in weight and sleep may receive behavioral activation, a treatment option which has been shown to be helpful for mood disorders such as major depression (Cuijpers, van Straten, & Warmerdam, 2007). Alternatively, when symptoms are diffuse, non-specific, or even sub-clinical in severity, adherents to the DSM classification scheme may lack clear-cut treatment options bearing known efficacy for problems that are difficult to classify. In such cases, one possible worthwhile alternative treatment is Acceptance and Commitment Therapy (ACT; Hayes, Strosahl, & Wilson, 2012), a contextual cognitive behavior therapy designed to facilitate increases in a transdiagnostic construct known as psychological flexibility.
Psychological Flexibility
Psychological flexibility is “the ability to contact the present moment more fully as a conscious human being, and to change or persist in behavior when doing so serves valued ends” (Hayes, Luoma, Bond, Masuda, & Lillis, 2006, p. 7). More colloquially, psychological flexibility involves engaging in personally meaningful behavior while also embracing a mindful perspective on problematic thoughts and emotions. Currently, the psychological flexibility model is depicted via an organization of six interwoven behavioral repertoires (see top half of Figure 1). This “Hexaflex” (Hayes, Strosahl, Bunting, Twohig, & Wilson, 2004) displays six clinical components of flexibility, referred to as present moment awareness, defusion, self-as-context, values, acceptance, and committed action. Present moment awareness refers to the ability to bring attention to the current environment, to simply observe events, internal as well as external, that are occurring here and now. Defusion is a deliteralized, detached perspective on symbolic experiences such as memories and beliefs. Self-as-context involves a cluster of perspective-taking abilities that serve self-awareness, empathy, and even a sense of transcendence. Values are personally chosen, deeply inspiring purposes of one’s life. Acceptance involves a curious willingness with respect to undesired private experiences (e.g., unpleasant sensations, emotions, or memories). Committed action is the behavioral expression of values, or values-consistent action.
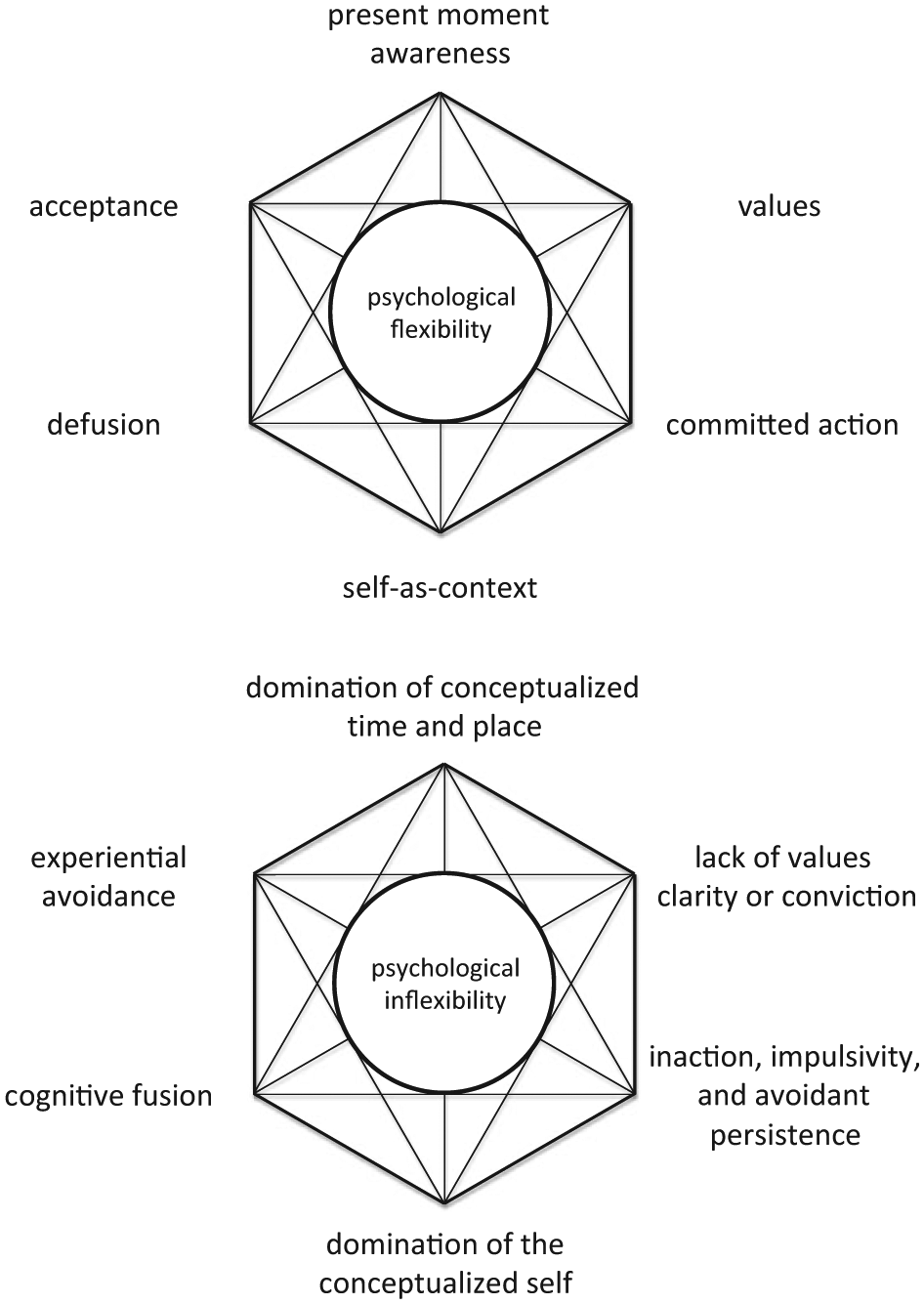
The psychological flexibility model as depicted by the Hexaflex (top) and Inflexahex (bottom) repertoires.
Psychological Inflexibility
In contrast, the psychological flexibility model views suffering as a product of inflexibility, which involves six absent or ineffective repertoires conceptualized via the “Inflexahex” (P. A. Bach & Moran, 2008; see bottom half of Figure 1). In contrast to present moment awareness, inflexibility may be characterized by a preoccupation with the past, the future, or events occurring in another place. With respect to defusion, inflexibility may involve a rigid adherence to the literal meaning of one’s thoughts and beliefs, otherwise known as fusion. In contrast to self-as-context, self-as-content entails narrow and constrained conceptualizations about self and others. Inflexibility with respect to values may be described as impoverished or incoherent repertoires with respect to identifying one’s deeply held convictions. Acceptance stands in contrast to experiential avoidance, regarded as any action intended to prevent or minimize private experiences such as unpleasant emotions and memories. An inflexible repertoire contrasting with committed action may be characterized by inaction, mindless impulsivity, or persistent situational avoidance. Thus, ACT treatment involves identifying and disrupting these classes of inflexible repertoires while developing and reinforcing more flexible repertoires.
The psychological flexibility model provides an alternative paradigm to the DSM classification system. Whereas the DSM approach to diagnosis is based on the number or severity of symptoms reported, psychological flexibility may be viewed dimensionally (Hayes, Wilson, Gifford, Follette, & Strosahl, 1996). Assessing an individual’s abilities across facets of psychological flexibility may reveal useful variations in the relative strengths and weaknesses of the six Hexaflex repertoires. Furthermore, these repertoires may be impacted by situational factors that may contribute to distress and dysfunction (e.g., relationships, employment, physical health). Such information may inform the treatment plan; relatively weak repertoires may be targeted with greater emphasis, or relatively strong repertoires may be enhanced first to facilitate subsequent interventions on weak repertoires. Clients commonly present to community mental health centers in distress and reporting few social and/or financial resources. When common life stressors co-occur with limited resources, and clients exhibit relatively inflexible repertoires in their efforts to deal with them, the resulting symptomatology may overlap with a variety of mood, anxiety, and personality disorders without meeting the criteria for any one diagnosis. When clients present with no clear basis for a DSM diagnosis but are exhibiting distress and dysfunction, the psychological flexibility model may offer a means of providing evidence-based treatment for presentations that would normally be regarded as non-specific or sub-clinical. A growing body of research provides substantial support for the relevance of the repertoires targeted by ACT.
Empirical Support for ACT
ACT seems to be a viable and effective treatment for a variety of human dilemmas, having been subjected to more than 100 randomized clinical trials for a broad range of difficulties and with a variety of populations. For example, Division 12 of the American Psychological Association lists ACT as an empirically supported treatment for chronic pain (Vowles & Thompson, 2011) and a probably efficacious treatment for depression (Zettle & Hayes, 1986), mixed anxiety (Arch et al., 2012), obsessive-compulsive disorder (Twohig et al., 2010), and psychosis (Gaudiano & Herbert, 2006). With respect to interpersonal difficulties, ACT has produced positive outcomes for stigma (Masuda et al., 2007) and borderline personality disorder (Morton, Snowdon, Gopold, & Guymer, 2012). This broad applicability seems to support the transdiagnostic assumptions of the psychological flexibility model.
Another important body of supportive evidence originates from mediational studies examining specific mechanisms of action for treatment outcomes. If the Hexaflex processes are genuinely active ingredients in psychotherapeutic change, then measures of those processes throughout treatment should predict improvements in therapy outcomes at the conclusion of treatment and beyond. As repertoires become increasingly flexible over the duration of therapy, clinical symptoms would likely decrease and quality of life increase. For example, increases in psychological flexibility have been demonstrated to mediate outcomes for psychosis (P. Bach & Hayes, 2002), chronic pain (Dahl, Wilson, & Nilsson, 2004), and depression (Zettle, Rains, & Hayes, 2011). Individual Hexaflex repertoires also have been scrutinized empirically. A recent meta-analysis containing more than 50 studies showed that clinical interventions representing most of the six components have generated considerable supportive evidence in laboratory-based treatment analogue studies (Levin, Hildebrandt, Lillis, & Hayes, 2012).
Measures of Hexaflex Components
Measures of ACT processes are relatively limited in number and under-researched compared with many clinical measures. The most prominent instrument is the Acceptance and Action Questionnaire (AAQ), currently in its second version (Bond et al., 2011). The AAQ was initially developed as a measure of experiential avoidance (Hayes, Strosahl, Wilson, et al., 2004), although it is now regarded as a measure of psychological flexibility. Some Hexaflex repertoires lack specific measures (e.g., self-as-context), whereas others have been subjected to measurement but with little data available to render solid conclusions regarding the utility of the measure (e.g., Forman et al., 2012; Wilson, Sandoz, Kitchens, & Roberts, 2010).
Although well-designed measures for each process may prove to be empirically progressive, it also may be advantageous for clinical settings to have a single, brief measure of flexibility that contains a relatively balanced approach to items from the six repertoires. Many ACT protocols are organized into sessions that focus on one process at a time over the duration of treatment. In theory, a process measure that assessed each of the six dimensions separately may be sensitive to specific treatment activities over the course of therapy. For example, scores for defusion questions of the measure could be considered before and after defusion sessions of a protocol are delivered. Changes for each pair of the flexible/inflexible repertoires depicted could be evaluated over the entire duration of treatment as well as with respect to the delivery of specific Hexaflex interventions. Such a measure was used with the client presented here. The measure was designed by a clinical psychology practicum team, supervised by the second author and administered weekly, in conjunction with a Hexaflex-based ACT protocol.
2 Case Introduction
The client, “Casey,” was a woman in her 30s. She was raised and currently residing in a rural area of the Midwestern United States. She was divorced with three young children and had recently completed graduate school. She was employed in two part-time jobs and applying for teaching positions. She self-referred for individual psychotherapy.
3 Presenting Complaints
Casey presented to the clinic following a number of significant life changes and a desire to speak with someone outside of her family and friends. She reported sadness and frustration about some of her relationships, anger and regret over some of her decisions with respect to these relationships, and stress regarding her search for employment and the financial demands of providing for her children. She said that her mother contributed to the difficulties of her relationship with her ex-husband as well as with other family members. She reported that she recently left the father of her children for the second time after a protracted history of conflict and purchased her own home. Nevertheless, contact with her ex-husband and/or her mother inevitably led to conflict. Casey revealed that interactions often would quickly escalate into heated arguments, and as a result she often felt as if her emotions were out of control. In her intake, she reported a desire to “learn how to establish relationship boundaries and [receive] help with making good social choices.”
4 History
Casey reported being married for 3½ years prior to her divorce approximately 10 years ago. She reported marrying her husband after becoming pregnant, and that the relationship was marked by frequent instances of verbal and emotional abuse. She said that her husband regularly abused alcohol and was rarely employed or contributing finances to the family. In contrast, Casey described herself as active socially and academically, which distinguished her from the rest of her family as well as her husband. She reported she returned to live with her ex-husband several years after the divorce and conceived their third child, although they never remarried. She stated that her husband and family never fully supported her academic and career aspirations, and that she had turned down enticing job offers to keep her children close to their father. After their most recent separation, she reported a relatively civil relationship with him, although she also reported continuing arguments regarding finances and child care.
Casey described a support system consisting of nearby friends and extended family members. She reported reluctance to burden her friends with disclosures about her own problems. She talked about going out for dinner and drinks with her friends weekly but also elaborated that she wished alcohol consumption did not coincide with their outings. She described a difficult relationship with her mother that sometimes impacted her relationship with other family members and her ex-husband. Casey described her mother as “stubborn” and exhibiting “borderline personality traits.” She said she requested a female therapist in hope of a better understanding of the mother–daughter relationship. She stated her mother frequently would turn family members against one another, elaborating that she believed her poor relationship with her sister was due to her mother’s influence. Casey described an incident in which her mother was planning a family outing and reassured everyone that she would make sure Casey would receive an invitation. However, Casey did not receive the invitation from her mother, and on the day of the outing her other family members concluded that Casey had refused to attend. The client revealed that over the years, her mother and sister often would side with her ex-husband on contentious issues without first listening to Casey’s perspective. Casey stated that her family believes she “over-reacts,” appears dramatic, and does not put forth adequate effort to communicate with the family.
Casey endorsed a psychiatric history. She revealed a former diagnosis of “general anxiety,” adding that she had been taking an anti-anxiety medication for the past 3 years. She reported recently reducing the dosage and a desire to eventually stop taking the medication altogether. Approximately 2 years previously, the client received Cognitive Behavioral Therapy for approximately 6 months. She described the experience as beneficial but also indicated concern that her prior experience consisted mostly of talking. She reported an interest in obtaining skills to prepare her for future crises. Casey denied any history of alcohol or substance use problems. She also denied any history or current experience with suicidal or homicidal ideation. Based on client reports during an intake interview as well as the first ACT session, she appeared to meet criteria for adjustment disorder with mixed anxiety and depressive symptoms, a relatively non-specific diagnosis with very little evidence available to guide selection of treatment (Carta, Balestrieri, Murru, & Hardoy, 2009).
5 Assessment
Casey completed a variety of measures during all sessions as well as approximately 6 months after termination. All were self-report measures presented via an online survey website. Each measure is described in further detail below.
Outcome Measures
AAQ
The AAQ-II (Bond et al., 2011) is a seven-item measure of psychological inflexibility. Respondents rate statements about their inflexibility with respect to unpleasant thoughts and emotions on a scale of 1 (never true) to 7 (always true). Higher scores indicate lower flexibility and higher inflexibility, with Bond and colleagues reporting a minimal range of scores from 24 to 28 as suggestive of a clinically significant level of inflexibility.
Outcome Questionnaire (OQ)
The OQ-45 (Lambert, Hansen, & Harmon, 2010) is a 45-item self-report measure of general psychological distress. The measure includes subscales for Symptom Distress, Interpersonal Relations, and Social Role. Respondents rate statements about these experiences by endorsing items on a scale of 0 (e.g., never) to 4 (e.g., almost always). Higher scores indicate higher distress. The administrator’s manual contains established clinical cutoff scores and reliable change intervals for each subscale as well as the total score.
Valued Time and Difficulty Questionnaire (VTDQ)
The VTDQ is a 30-item self-report measure of the importance, amount of time, and difficulty in engaging in activities oriented toward a variety of valued life domains. For example, the domain for intimate relationships includes the questions “How important is it to you to be in an intimate relationship?” “In the last week, how much time have you spent working toward or participating in an intimate relationship?” and “In the last week, how difficult was it to work toward or participate in an intimate relationship because of unpleasant thoughts, feelings, or bodily sensations?” Respondents rate their agreement with statements that refer to a scale of 0 (e.g., not at all) to 10 (e.g., completely). This measure is an adaptation of the Valued Living Questionnaire (Wilson et al., 2010). It was developed in a clinical setting by the second author and has not been the subject of a published study.
Processes Measures
Weekly Hexaflex Assessment (WHA)
The WHA is an exploratory process measure of psychological flexibility. Items refer to general examples of the 12 repertoires described by the Hexaflex and Inflexahex (see Figures 1 and 2). Instructions ask respondents to “ . . . estimate how much or how little you have done each of the following behaviors over the past week.” Respondents select a number on a scale of 0 to 10, with the following labeled numbers: 0 (not at all), 3 (sometimes), 7 (frequently), and 10 (all the time). Items were generated by the second author and a vertical team of clinical psychology students enrolled in a year-long ACT practicum. From a larger pool of items and over a series of revisions, the group refined the list to 12 items that were deemed easiest to comprehend and also specific and accurate examples of each concept. Six items refer to flexible behaviors and six refer to inflexible behaviors. For example, the item for acceptance stated “open to experiencing uncomfortable emotions, thoughts, or memories,” and the item for experiential avoidance stated, “trying to control my emotions, thoughts, or memories.” For all administrations, each inflexible item was reverse-scored and added to the complimentary flexible item, resulting in six scores with a possible range of −10 to +10, where positive values represent higher flexibility and lower inflexibility.
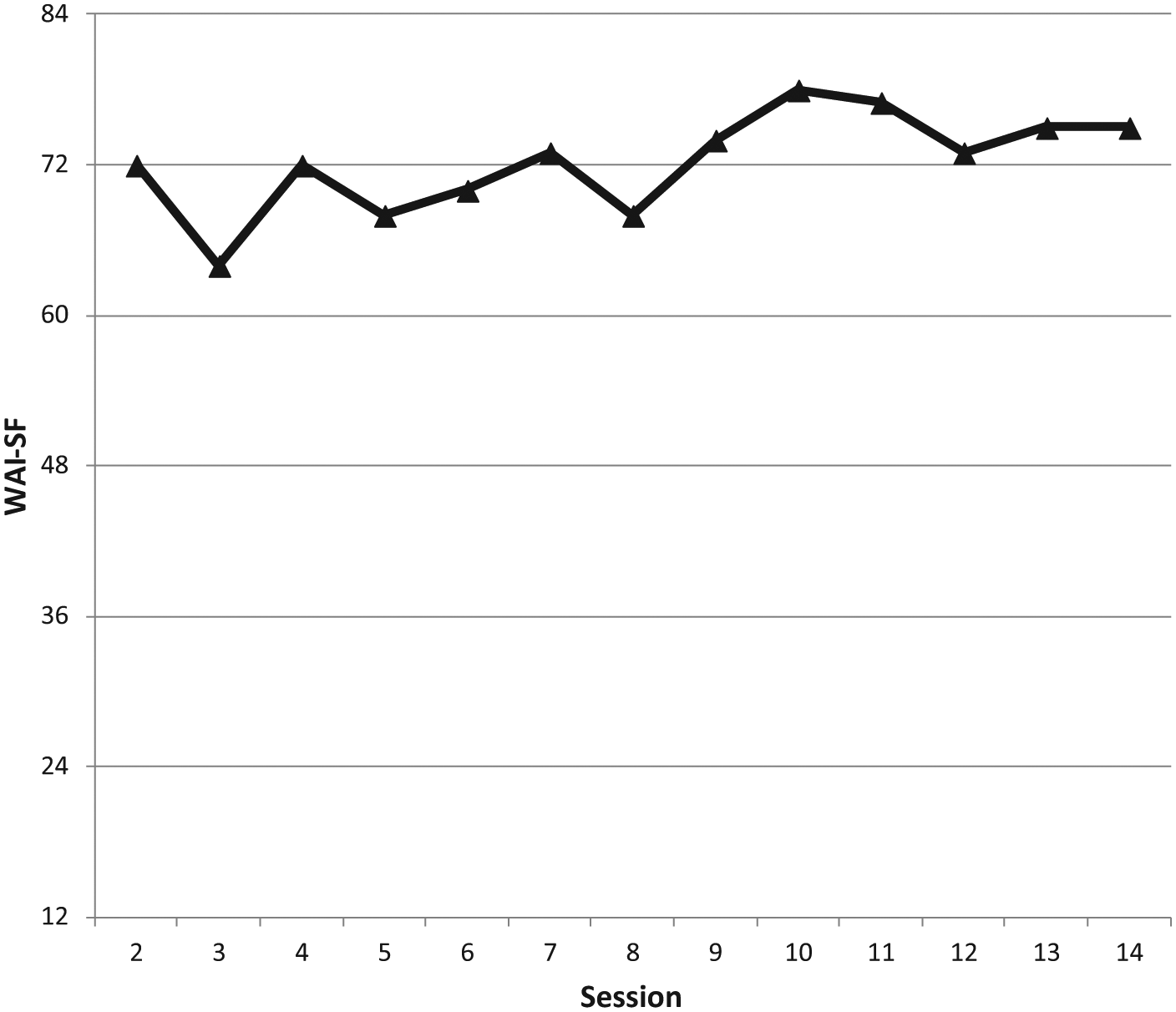
Client scores on the Working Alliance Inventory, Short Form (WAI), for Sessions 2 to 14.
Working Alliance Inventory (WAI)
The WAI (Tracey & Kokotovic, 1989) is a 12-item measure of a client’s perception of the therapeutic relationship. It contains evaluative statements about the therapist and treatment that involve a 7-point Likert-type scale ranging from 1 (never) to 7 (always).
These measures were organized into two separate packets, which were administered at different times throughout treatment. The Outcomes packet (AAQ-II, OQ-45, and VTDQ) was administered at the beginning of Sessions 1 and 14 and at the 6-month follow-up. The Processes packet (WHA and WAI) was administered during each session except the first, with the WHA administered at the beginning and the WAI at the conclusion of these sessions. These measures were scored after each session and discussed weekly during supervision meetings.
6 Case Conceptualization
Casey presented with distress largely oriented to difficult relationships in her life. As such, her feelings about them as well as the actual behaviors of her ex-husband and mother may be classified as uncontrollable experiences that she nevertheless was trying to avoid or otherwise control. Her efforts to manage these events indicated a relatively inflexible repertoire with respect to these challenges, as she also reported little confidence or success in her efforts to deal with them. Although Casey had previously received short-term psychotherapy for these conflicts, she stated that she felt as if she lacked the skills to respond adaptively to new examples when they inevitably occurred.
More specifically, Casey exhibited signs of inflexibility with respect to most of the Hexaflex components, especially those more oriented to mindfulness. Casey appeared to readily become preoccupied by her emotions and perceptions of her mother and ex-husband, to the extent that she was disconnected from the present moment. She reported feeling overwhelmed during conflict rather than being able to simply observe her reactions and the reactions of others. Casey also displayed a clear investment in unhelpful evaluations about herself and the people in her life, a marker of fusion. She reported ruminating about who was in the right and who was in the wrong regarding each instance of conflict. She revealed considerable concern regarding thoughts about being a bad person, mother, and wife for leaving her husband and pursuing a career. Furthermore, Casey demonstrated difficulties observing her thoughts, feelings, and emotions as merely psychological content that changes over time and instead experiencing the stable, unchanging perspective of self-as-context. She seemed constrained by her perceptions of herself and others, which readily led to her participating in heated arguments. Her frequent interpersonal difficulties suggested that she found it challenging to engage in perspective-taking skills with respect to self and others that could facilitate healthier patterns of social behavior. Given the ways in which her mind was interfering with her ability to navigate all the social demands of her life, training in present moment awareness, defusion, and self-as-context appeared desirable.
Regarding motivational components of the Hexaflex, Casey revealed markers for ambivalence about her values. For example, she described drinking socially to fit in despite the inconsistency between this behavior and her actual wants and preferences. She also talked about her efforts to get along with her family members even when doing so involved associating with people who were reportedly manipulative and hurtful. This suggests that Casey was prioritizing other people’s needs and emotions over her own values. Indeed, these activities were likely instances of experiential avoidance, as she primarily was working to minimize conflict and negative emotions (for her and others) rather than to build meaningful, healthy relationships. Although committed action appeared to be a relative strength for Casey, as indicated by her accomplishments as a mother, student, and employee, this repertoire was not as prominent in the difficult social circumstances she described. Additional acceptance, values clarification, and committed action training seemed merited based on her ineffective behavior with respect to friends and especially family.
7 Course of Treatment and Assessment of Progress
A psychological flexibility training protocol was provided consisting of many of the metaphors, experiential exercises, and other activities reviewed by Levin and colleagues (2012). The protocol outlines 3 introductory/preparatory sessions that precede 6 to 12 modular sessions on each of the six Hexaflex repertoires. An optional termination session concluded the protocol, resulting in a possible treatment duration of 9 to 16 sessions. The protocol was written to be adjustable in accordance with weekly supervisory meetings with the graduate student therapists administering it. Each process of the Hexaflex could be covered in 1 or 2 sessions, and the order of the processes could be varied as needed. Each modular session involved (a) a review of last week’s daily practice assignment (if needed), (b) provision of psychoeducation and a rationale for the session’s Hexaflex repertoire, (c) provision of a metaphor illustrating the repertoire, (d) engagement in an experiential exercise for the repertoire, and (e) assignment of at least one daily practice activity for the repertoire. Casey received 14 total sessions, including a termination session and 10 of 12 possible modular sessions.
Casey’s first session consisted of obtaining informed consent, completing assessment measures, introducing the ACT model, and discussing expectations for treatment. The second session primarily involved the creation of two lists. The first detailed the client’s experience with suffering (e.g., anxiety, self-doubt, anger), and the second list detailed her efforts to cope with or “solve” items from the suffering list. Her suffering list consisted of worrying about her family members and the uncertainties of her future, while her solutions list consisted of organizing (e.g., creating to-do lists) and avoiding stressful situations and people. For example, the client described frequent worries about what to say or how to behave during interactions with her mother. She said she would often consult with family members regarding the exact time to arrive and leave from family events to prevent seeing her. In the third session, Casey and the therapist created a diagram in which they listed and distinguished between controllable and uncontrollable experiences. This distinction was related back to the items on her suffering and solutions lists. She indicated that on workdays she spent approximately 25% of her day attempting to control things that were uncontrollable. In contrast, she reported spending 80% of her time attempting to control the uncontrollable on days when she was not working. As specified by the protocol, goal formulation began during the latter part of Session 3. However, due to time constraints, this had to be completed in Session 4. Casey reported goals that included fostering good friendships, finding a significant other, joining a good church, and “living in a mindful way.”
Sessions 4 to 13 were modular sessions covering each of the Hexaflex components. Present moment awareness, defusion, and self-as-context were delivered first, because they appeared to be relative weaknesses for Casey as well as similar to the psychological coping skills she requested. Casey engaged in two sessions for present moment awareness, two for defusion, and one for self-as-context, in that order. Present moment awareness was practiced in session via the Floating Leaves on a Moving Stream exercise (Hayes, 2005), which involved imagining each thought and feeling that arose being placed on a leaf and then watching the leaf float down a stream. Although this activity is commonly regarded as a defusion exercise, it was instructed and guided in a way that highlighted engaging in the present moment. A session involving a Passive Progressive Muscle Relaxation exercise (Feldman, Greeson, & Senville, 2010) was conducted as well, except with an emphasis on noticing a variety of sensations rather than reducing tension or anxiety. Defusion was taught via the Milk, Milk, Milk exercise (Hayes, Strosahl, & Wilson, 1999), which involves noticing the physical properties of saying the word “milk” while quickly repeating it out loud for approximately 30 s. The activity was also conducted with a specific word identified by Casey as problematic for her. The I Cannot Walk exercise (Kehoe, Barnes-Holmes, Barnes-Holmes, Cochrane, & Stewart, 2007), involving repetition of the statement “I cannot walk” while walking, further emphasized that words need not dictate perception or behavior. Casey engaged in only one session for self-as-context, as she identified it as similar to the other two modules and was eager to move on to a values module. The Observer Self exercise (Hayes et al., 1999) guided her imagination through a series of different personal and social experiences, with the conclusion of the activity highlighting a sense of self-awareness that is stable and consistent across the variety of experiences.
Following her training with present moment awareness, Casey reported incorporating the activity into her morning routine. After the first defusion session, she said she started examining her thoughts in a variety of different ways, including singing one thought to the tune of “When the Saints Come Marching In.” She reported experiencing greater calmness since beginning treatment. In particular, she reported that she did not get as upset with certain people as she formerly had.
Next, Casey engaged in one session for values, two for acceptance, and two for committed action. Values were addressed via a Values Card Sort exercise (Ciarrochi & Bailey, 2008), involving the categorization of a deck of cards displaying values-oriented words with respect to importance. Casey selected her eight most important cards and arranged them into a format in which “love” was in the center with the other cards surrounding it. Casey reported adequate understanding of this component, in part because she had been reading about values in some popular ACT books, so only one session addressed it. Her acceptance sessions included the Physicalizing exercise (Hayes et al., 1999), which involved imagining an unpleasant sensation as an object hovering in front of her and inspecting a variety of its sensory properties. Although typically regarded as an activity exemplifying defusion, in this case a posture for willingness was promoted during the client’s experience. The Chinese Finger Cuffs exercise (Eifert & Forsyth, 2005) was also used in an acceptance session, where it was noted that the easiest way to remove one’s fingers from this toy was by discontinuing one’s efforts to force them out. The final sessions on committed action involved values-consistent activity scheduling using the Matrix (Polk & Schoendorff, 2014) as a guide. The Matrix is a simple model of psychological flexibility that highlights the purpose of behavior (experiential avoidance vs. committed action) in conjunction with the source of influence over behavior (mental vs. physical stimulation) in any given moment.
During these later modules, Casey began describing her learned skills as a lifestyle change and repeatedly expressed her gratitude to the therapist. She provided her own flexibility metaphor based on her experience with childbirth (i.e., willing to endure the pain of childbirth for the sake of bearing a child and being a mother). She reported a greater ability to utilize ACT skills in her relationships, including with her sister and mother. She also said she was more aware of when her behavior was consistent or inconsistent with respect to her values.
Session 14 was a formal termination session during which treatment was reviewed and Casey’s future plans were discussed. She stated she was consistently more aware of the present moment. For example, she stated that instead of always looking forward to the weekend, she enjoys every day. She reported a desire to surround herself with people who live values-consistent lives. She described encouraging friends to be more present moment aware and practicing other Hexaflex skills whenever feasible. Casey said she was spending less time with friends who consumed alcohol heavily and making efforts to reconnect with family members whose relationships were strained by past conflict with her. She stated that she was more able to recognize and experience challenging thoughts and emotions, and that this diminished her emotional reactivity and improved her ability to communicate with family members. The therapist and Casey discussed how to maintain the progress she made in therapy, including the continuation of her therapy hour each week for a valued activity. Casey revealed that learning new skills, applying them to her everyday life, and reflecting on her experiences with her journal were most helpful over the duration of treatment.
Review of Outcome Measures
Table 1 shows the client’s data for the AAQ-II, the OQ-45, and the VTDQ for all three administrations (Sessions 1 and 14, and at a 6-month follow-up). Generally speaking, these scores showed improvements at post-treatment that were maintained to follow-up. Although Casey’s self-reported level of psychological distress was below an established clinical cutoff of 63 at pre-treatment, nevertheless she obtained a reliable reduction at post-treatment for her overall score. Her “Interpersonal Relations” subscale score did exceed the clinical cutoff at pre-treatment, which is consistent with her presenting complaints, but was no longer significant at post-treatment and follow-up. Her AAQ-II score was also within a range of clinical significance estimates reported by Bond and colleagues (2011) at pre-treatment but not subsequently, indicating reduced psychological inflexibility. Although the stability of her Importance score on the VTDQ was expected, the reduction for Time was not. Perhaps her tendency to overinvest in her relationships with her family at pre-treatment was reflected in her responses to this measure, and the reduction represents a more functional level of commitment for her. Curiously, her scores for the Difficulty subscale were quite low in comparison with most clients, even after a minor increase at follow-up. Given the interpersonal nature of her presenting complaints, perhaps she was responding to these items as if her difficulties were based on the people themselves rather than her thoughts and feelings about them.
Outcome Measure Scores at Pre, Post, and Follow-Up.
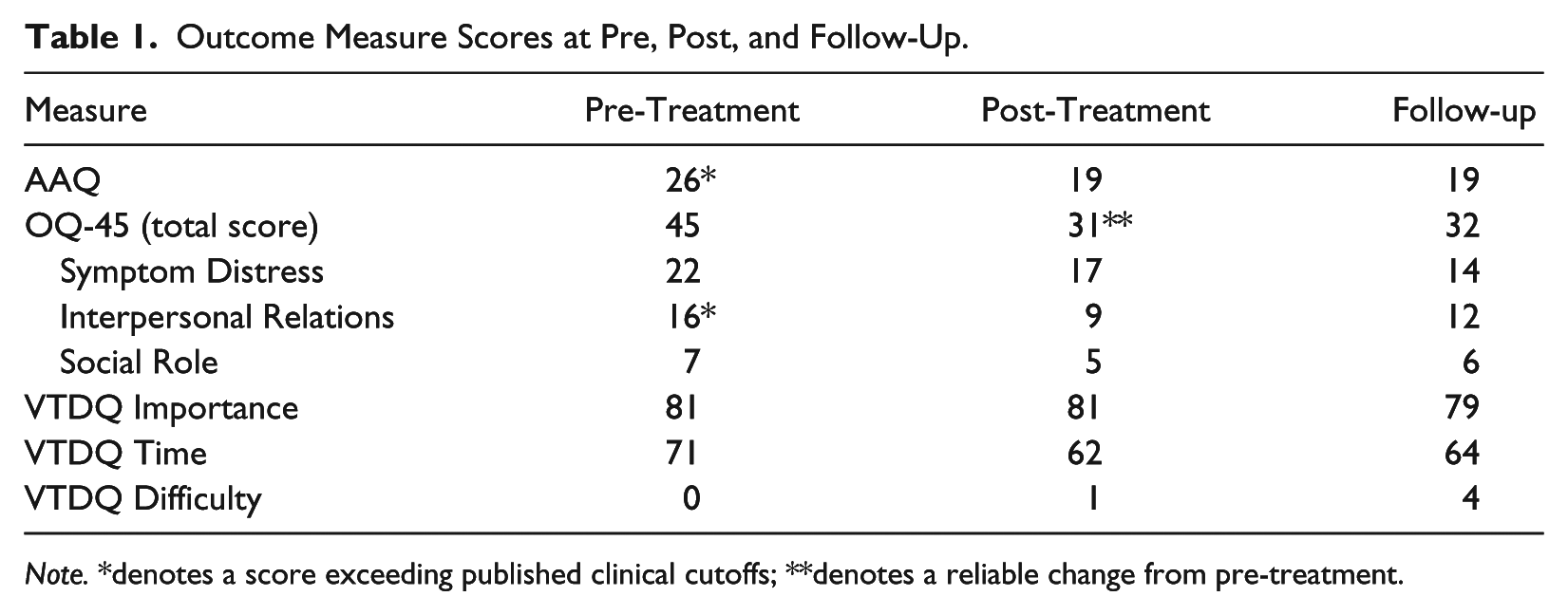
Note. *denotes a score exceeding published clinical cutoffs; **denotes a reliable change from pre-treatment.
Review of Process Measures
Figure 2 shows Casey’s WAI scores through Sessions 2 to 14. Although quite positive and relatively stable throughout, the first eight sessions appear to be slightly lower than subsequent sessions on average. Although seemingly compliant with treatment, Casey reported some concerns about therapy during some of these sessions. She expressed concern that insufficient attention was spent on the details of her arguments with family members. It appears that additional discussion about the treatment plan as well as some initial success with the skills taught in sessions preceded the small but positive shift beginning around Session 9.
Figure 3 shows Casey’s WHA scores through Sessions 2 to 14. There is a trajectory from mildly inflexible to strongly flexible repertoires over time. Although these increases occurred throughout treatment, there seem to be two occasions where increases were substantial—around Sessions 2 to 4 and Sessions 8 to 10. Some initial treatment goals were formulated in Sessions 3 and 4, which may explain some of the early increase and continuing escalation of her values and committed action scores during treatment even though these modules were not provided until the latter half of the protocol. Defusion and self-awareness scores seemed particularly responsive to delivery of their respective modules during treatment, as substantial gains were exhibited for these scores afterward. Perhaps these two modules represent activities that were the least familiar to the client and therefore most difficult to learn before direct instruction. The only repertoires that did not show increases after being covered in treatment were for willingness and committed action, which were delivered in Sessions 10 to 13 after scores were already at their peak (and presumably after some degree of indirect coverage in previous sessions as well as in books the client was reading). As with the WAI, there also appears to be a positive shift for all WHA scores after Session 8, where scores on the WAI are also somewhat higher afterward.

Client scores for each flexible/inflexible composite repertoire of the WHA for Sessions 2 to 14.
WHA scores did not always increase during treatment. Two or three sessions indicated substantial declines from previous weeks—Sessions 7, 13, and to some extent 11—that resurged in subsequent sessions. During Session 7, Casey reported feeling anxious about her planned attendance at a family member’s birthday party later in the week. Session 11 occurred a week later than usual, after canceling the previous week’s session to attend a family member’s funeral. During Session 13, she described frustration with an ongoing disagreement with her mother and ex-husband regarding child care. Perhaps these stressors contributed to the temporary declines in certain scores on the WHA during treatment.
8 Complicating Factors
With respect to treatment compliance, Casey appeared to be particularly dedicated to understanding and practicing what she learned in sessions. She took vigorous notes in her journal during every session, and reported using it to review her notes from the prior session as well as to guide her daily practice activities. Throughout treatment, Casey reported reading various ACT books, including ACT Made Simple (Harris, 2009). Thus, it is unclear how much these supplementary forms of therapy impacted the client above and beyond session activities. Nevertheless, Casey appeared to be a highly motivated and intellectually curious client who the authors perceived to be a reliable provider of valid data.
Although seemingly an “ideal” client in some ways, Casey also presented some complicating factors that required minor adjustments to her sessions. In some early sessions of the protocol, Casey periodically voiced concerns regarding the appropriateness of ACT for her problems. In particular, she reported that although the offered skills would be helpful for mildly distressed and healthy clients, she required “crisis management” to cope with her distress. She also suggested that her interpersonal difficulties should require discussing in depth her relationships with her mother and ex-husband. She said she wanted to process her feelings about these ongoing relationships during sessions. These concerns were raised through Sessions 5 and 6. The therapist and Casey agreed to briefly spend time at the beginning of each session (i.e., less than 10 min) to discuss her prior week rather than immediately beginning the module content.
9 Access and Barriers to Care
Given her responsibilities with respect to children and work, Casey presented with limited availability to meet for psychotherapy. She canceled two appointments throughout treatment due to unexpected family obligations. On one occasion, a session was scheduled a week later than usual to accommodate work-related travel. She met criteria for a substantially reduced fee for sessions based on her income and dependents.
10 Follow-Up
Casey was contacted via email approximately 6 months after treatment termination requesting she complete the outcome measures. She responded with news that her children were doing well and that she was enjoying a new job in a new town, elaborating that it was “very challenging and also very rewarding.” Casey responded to the measures very promptly.
11 Treatment Implications of the Case
It appears that teaching clients to be more psychologically flexible may be helpful for clients presenting with Adjustment Disorder symptoms. In the absence of specific and severe symptomatology that might guide selection of an empirically supported treatment, the psychological flexibility model offered an evidence-based approach that appears to have helped Casey with long-standing personal and social challenges in her life. Over the course of therapy, she exhibited significant investment in practicing the skills provided in sessions. At the end of treatment and afterward, the client reported substantial increases in psychological flexibility and decreases in psychological distress.
Although hardly to be taken as a validation of the measure, the WHA appeared to work as intended. For all six processes, scores were shown to transition over the course of treatment from relatively inflexible repertoires to flexible repertoires. Although the direction and magnitude of change varied over the course of treatment, all processes were substantially more flexible at the conclusion of therapy. These data appeared consistent with client self-reports as well as therapist observations. This case provides tentative evidence for the usefulness of assessing mechanisms of action that are specific to each of the repertoires specified in the Hexaflex.
The structured nature of the protocol and associated assessment may have enhanced therapist and client accountability. The client’s perception of therapy sessions and weekly engagement with the Hexaflex repertoires were monitored throughout treatment. Prior to moving on to the next skill, mastery of the current skill could be assessed based on the client’s weekly data. Any progress or difficulties could be identified and addressed with the client. Furthermore, working toward mastery of all modules helped to provide a sensible basis for the conclusion of treatment. At times, it can be challenging to determine the appropriate time for termination, especially if problems are difficult to classify and progress difficult to measure. However, with this ACT protocol, continuous assessment of specific repertoires that were systematically trained during modular sessions allowed for therapy to be delivered ideographically and succinctly. Perhaps this combination of elements—modular treatment components, specific process measures, and transdiagnostic target behaviors—might offer a desirable treatment strategy for other ambiguous or empirically under-addressed clinical presentations.
12 Recommendations to Clinicians and Students
Numerous clients present for treatment requesting specific tools and techniques to help them cope with their perceived problems. ACT may be a desirable treatment package for such clients, especially if the processes are presented as “life skills” or practices that are designed to help people live more effectively. This contrasts with certain common assumptions about suffering and therapy among clients, so it is often important to address these possibilities early and directly, as done in the initial three sessions of the protocol. Clients commonly request tools to get rid of problems, not enhance life. Clients who embrace the skills with an intention to minimize unpleasant thoughts, emotions, and sensations will likely be dissatisfied, as these are often additional examples of the client’s experientially avoidant repertoires on display. Alternatively, when the model elements are presented as skills that increase behavioral options in difficult circumstances and enhance engagement with life, clients will have a more workable relationship with the goals of treatment.
This clarity about the purpose of treatment also applies to individual sessions, as evidenced by the rationales provided at the outset of each modular session. Some data suggest that the combination of rationale and experiential exercise produce superior outcomes compared with either component alone (McMullen et al., 2008). Although efforts were made to clearly describe the target behavior and the value of the behavior in these rationales, at times it may be challenging to translate the repertoires into accessible examples for the client. To avoid common misperceptions or misunderstandings, the term “willingness” was used instead of “acceptance,” and “self-awareness” instead of “self-as-context.” Matching metaphors and exercises to Hexaflex concepts is not always straightforward. At times, metaphors and experiential exercises were provided that could be conceptualized via more than one Hexaflex component. To the extent possible, the protocol was populated with empirically supported metaphors and exercises that were readily distinguished as exemplifying one particular component. However, given the limited current database for these studies and the plethora of metaphors and exercises detailed in the ACT literature (e.g., Hayes et al., 1999, 2012), it seems likely that many others may effectively teach the associated repertoire and could serve as worthy substitutes. A balanced approach might involve providing an empirically supported activity for the initial session of each Hexaflex component and an ideographically chosen activity for the second session.
Strongly encouraging, supporting, and reinforcing client engagement in daily practice seems advisable for any therapy, and the emphasis on life skills in the current protocol was an attempt to promote this view with clients from the outset. Casey was a noteworthy client in this regard, as she utilized her own journal for treatment notes and read a number of popular books about ACT in conjunction with her sessions. It appeared evident that Casey adopted ACT into her everyday lifestyle, and it seems likely that this level of engagement contributed to the changes in her scores. To the extent possible, it seems important to influence clients to incorporate the skills introduced in session into their lives, and to have faith in the processes that empirical psychology has to offer.
The current case is consistent with the view that maintaining rapport and developing a justifiable rationale for the focus of treatment is important. In the current case, the client expressed some initial concerns about the focus of the treatment, stating that she needed to spend some time in sessions elaborating on interpersonal difficulties experienced in the previous week. Although such activities are not regarded as essential to the psychological flexibility model, maintaining rapport and a sense of shared purpose would be expected to facilitate progress. The therapist was able to allocate a brief period of time at the beginning of sessions for the client to update the therapist about recent relevant experiences. This seemed to provide a basis for maintaining and improving rapport as well as setting a context for the introduction of treatment components. Taking a firm but flexible approach to protocol implementation seems advisable when managing the therapeutic relationship.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.