
Abstract
Youth with autism spectrum disorder (ASD) may have difficulties with compliance, impulsivity, and attention, which can affect daily adaptive functioning leading to disruptions in family social interactions, communication skills, academic achievement, and engagement in the community. Although previous research has identified behavioral treatments such as applied behavior analysis (ABA) therapy for youth with ASD, it is important to explore more interventions that can be effective in decreasing problematic behaviors while also building positive social skill development. This case study illustrates the effectiveness of Parent–Child Interaction Therapy (PCIT) to address behavioral problems in a 7-year-old boy with high-functioning ASD (HF-ASD) and comorbid ADHD. Overall, the results demonstrated a decrease in child challenging behaviors and an increase in child compliance. In addition, the child’s mother increased her use of positive parenting skills and effective commands. This study provides additional support for PCIT for children with ASD, but was not without challenges. These challenges, characteristic of families affected by ASD, and treatment implications for clinicians working with this population are discussed.
1 Theoretical and Research Basis for Treatment
According to the Centers for Disease Control (2012), approximately one in 68 children have an autism spectrum disorder (ASD). Over the past decade, ASD diagnoses have increased by more than 100%, from one in 150 in 2002 to one in 68 in 2012 (Centers for Disease Control and Prevention, 2012). ASD is characterized by deficits in social communication skills and the presence of restricted and repetitive behaviors. Youth with ASD, in some cases, may view things as more “black and white,” which impairs flexible thinking across contexts; they also may have a hard time taking other people’s perspectives, reading social cues, and engaging in age-appropriate social behaviors (Pratt, Hopf, & Larriba-Quest, 2017). In contrast, youth with ASD may also exhibit a range of strengths like strong rote memory skills, rule-based thinking, and strong visual-processing skills especially for details (Commons et al., 2017). Although ASD can be reliably diagnosed by age 2 years, most children are diagnosed closer to age 4 years (Christensen et al., 2016). Early diagnosis is critical to accessing early intervention services that may mitigate the core social deficits of ASD, improve daily adaptive functioning, and support the development of positive interpersonal relationships.
In addition to the presence of atypical social communication skills, youth with ASD may also present with disruptive behaviors. Youth with ASD may have difficulties with compliance, impulsivity, and attention. If these difficulties are too severe they may meet criteria for a comorbid disorder like oppositional defiant disorder (ODD) and/or attention-deficit/hyperactivity disorder (ADHD). In fact, among children with ASD, about 50% to 70% have comorbid ADHD (Antshel, Zhang-James, Wagner, Ledesma, & Faraone, 2016) and 13% to 27% meet criteria for ODD (Gadow, DeVincent, Pomeroy, & Azizian, 2004, 2005). For example, Armstrong and Kimonis (2013) completed a cases study on a 5-year-old patient with Asperger’s disorder, currently referred to mild- to high-functioning ASD (HF-ASD). This patient not only had a diagnosis of ASD but he also met the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) criteria for ODD and/or ADHD. Similar to many characteristics listed above, this patient had difficulty facing new situations, transitions, or changes and often demonstrated aggressive and noncompliant behaviors. This in turn made it difficult for the parent to manage the patient’s behavior at home and out in public. The presence of comorbid psychiatric problems has a profound negative impact on daily adaptive functioning leading to disruptions in family social interactions, communication skills, academic achievement, and engagement in the community (Hartley, Sikora, & Mccoy, 2008; Malhi & Singhi, 2015).
Parent–Child Interaction Therapy (PCIT) is an evidence-based behavioral therapy intervention for youth with externalizing disorders ages 2 to 8 years (Eyberg, Boggs, & Algina, 1995). PCIT has also proven effective with subpopulations of youth who have experienced childhood maltreatment (Bjørseth & Wichstrøm, 2016) and ADHD (Antshel et al., 2016), and more recently, there is a growing body of research to support its use with children with ASD (Agazzi, Tan, & Tan, 2013; Agazzi, Tan, Ogg, Armstrong, & Kirby, 2017; Allen, Harrington, & Cooke, 2011; Armstrong, DeLoatche, Preece, & Agazzi, 2015; Hatamzadeh, Pouretemad, & Hassanabadi, 2010; Masse, McNeil, Wagner, & Quetsch, 2016; Solomon, Ono, Timmer, & Goodlin-Jones, 2008). Some of the components of PCIT include relationship building, which is fostered during the first half of treatment called child-directed interaction (CDI), and compliance training, which is conducted during the second half of treatment called parent-directed interaction (PDI). In addition, parents are also taught skills such as planned ignoring and differential attention for appropriate behavior. During CDI, caregivers learn positive parenting strategies and communication skills that increase warmth in parent–child interactions and improve child attention and social behaviors (e.g., taking turns, playing cooperatively, sharing), while decreasing problematic attention-seeking behaviors (e.g., whining, rough play; Eyberg et al., 1995). Given the disrupted social interactions and challenging behaviors associated with ASD, PCIT may be a viable treatment for these youth. While the evidence to support PCIT for families with ASD is in its infancy, initial findings from case studies and small pilot trials suggest that PCIT does reduce challenging behaviors of children with ASD while also increasing effective parenting skills and reducing parenting stress (Agazzi et al., 2013; Agazzi et al., 2017; Armstrong et al., 2015; Ginn, Clionsky, Eyberg, Warner-Metzger, & Abner, 2015; Jeter, Zlomke, Shawler, & Sullivan, 2017; Lesack, Bearss, Celano, & Sharp, 2014; Masse et al., 2016).
2 Case Introduction
The aim of this study is to discuss and illustrate the effectiveness of PCIT to address behavioral problems in a 7-year-old boy with HF-ASD and comorbid ADHD. Jason was a 7-year-old boy with ASD who was referred to a university pediatric clinic to receive behavioral therapy. Prior to entering therapy, Jason was diagnosed by a university pediatric psychologist with ASD, ADHD, ODD, transient tic disorder, and persistent disorder of initiating or maintaining sleep. Jason’s mother reported that he had restricted interests (e.g., math and space), rigid thinking, sensitivity to sounds, and different textures, and was argumentative. Jason’s mother also reported sleep difficulties, indicating that it often took him at least an hour to fall asleep at night.
3 Presenting Complaints
Jason’s mother’s primary area of concern related to Jason’s inability to regulate his behavior at home and at school. At home, Jason’s mother reported difficulty with following directions, staying focused, and talking too much. Jason’s mother was frustrated with his poor focus during homework routines and described him as distracted and having trouble completing assignments. She also endorsed concerns for speech articulation and described Jason as difficult to understand at times. In addition, mother reported sensitivity to sudden or loud environmental noises like fire alarms, toilets flushing, and fireworks and indicated that Jason had to covers his ears in the presence of such sounds. Finally, Jason also had light sensitivity and sometimes insisted on turning off lights in the home so he could play in the dark.
While at school, previous teachers reported Jason required frequent adult prompting and redirection to stay seated, participate in instruction, and begin and finish assignments. He frequently called out or interrupted others during instruction. Jason’s previous teacher endorsed concerns with excess energy and excitement, which often led to off-task behaviors like walking around the classroom or physical movement such as using his body to act out stories during circle time, and occasionally flapping his hands and arms. The teacher reported repeatedly redirecting Jason during academic instruction. The teacher also reported difficulty with following directions, staying seated, staying on-task, and talking too much. Jason’s mother reported similar concerns during homework routines.
4 History
Jason was born full term and adopted at birth. Jason stayed in the neonatal intensive care unit (NICU) for a few days at birth due to suspected sepsis. He also had a heart murmur in early childhood that had resolved. His biological parents’ medical history was unknown. Jason’s adoptive parents reported that Jason achieved early childhood milestones on time or ahead of time. He learned to read and tell time by age 3. Jason was diagnosed with ADHD in 2015 and, since then, has been prescribed a variety of medications, including Metadate CD (10 mg and 15 mg), Adderall, and Vyvanse. At the time of PCIT treatment, Jason was taking Metadate CD again, and his dose had recently been increased to 20 mg. Per parent report, medication was working well, and there were no significant side effects. In the school setting, Jason received academic supports through enrichment services and speech therapy through an Education Plan for giftedness and an Individualized Education Plan (IEP) for speech impairment. In addition, he had a functional behavioral assessment (FBA) after his first-grade teacher reported ongoing problematic defiant, hyperactive, and inattentive symptoms. Although Jason had some behavioral difficulties in the past at school, he reported liking his school and having many friends.
5 Assessment
A comprehensive assessment was conducted by a multidisciplinary team, including a psychiatric nurse practitioner, psychiatrist, and pediatric psychologist. Jason’s height and weight were within normal limits for his age and gender and he had a healthy body mass index (BMI; 14.39 kg/m²). The psychiatrist and the nurse practitioner conducted several assessments, which indicated that Jason met diagnostic criteria for ADHD-Combined Type and presented with symptoms of irritability. Speech sound disorder and stuttering were also noted. The Social Responsiveness Scale was completed to screen for ASD. Jason received a T-score of 60, which fell into the clinical range (60-75) for exhibiting symptoms for ASD. Based on these results, Jason was referred to a pediatric psychologist for a full psychological evaluation to rule out ASD. The psychological evaluation included behavior-rating scales, completed by mother and teacher; an IQ assessment; a sleep assessment; and a semi-structured autism evaluation. Jason achieved a Full Scale IQ score of 123 on the Wechsler Intelligence Scale for Children–Fifth Edition (WISC-V; Wechsler, 2003), placing him in the Superior range (94th percentile). Jason’s mother and teacher completed the Achenbach Child Behavior Checklist (CBCL/Teacher Report Form [TRF]; Achenbach & Rescorla, 2001). Jason’s mother rated him in the Borderline to Clinically Significant range on the total, internalizing, and externalizing problems scales. Jason’s teacher rated him in the normal range across the same scales. The Adaptive Behavior Assessment System–Second Edition (ABAS-II; Harrison & Oakland, 2003) was also completed by the mother and the teacher and both raters reported scores within the average to above-average range across the conceptual, social, and practical domains. The NICHQ Vanderbilt Assessment Scales were completed by mother and teacher. Mother’s ratings met diagnostic criteria for ADHD, hyperactive/impulsive type (ADHD-H/I). Jason’s teacher did not indicate any significant concerns. Finally, to assess for symptoms of ASD, Jason’s mother completed the Autism Spectrum Rating Scales (ASRS), and Jason was administered the Autism Diagnostic Observation Schedule–Second Edition (ADOS-2). Jason had elevated scores on the ASRS in peer socialization and social/emotional reciprocity; he still met the ADOS-2 clinical cut-off for symptoms of ASD.
6 Case Conceptualization
Based on the current comprehensive multidisciplinary assessment and psychological evaluation, it appeared that Jason engaged in most of his challenging behaviors in the home setting. Indeed, a comparison of parent and teacher ratings on standardized assessments suggested many problems in the home setting while teacher ratings were within normal limits. A few factors likely explain the contrast in ratings. First, at the time of this evaluation, Jason had recently started a new dose of Metadate CD (20 mg), and parent reported noticeable improvements in attention compared with previous doses and other medications. This may have affected his ability to focus and remain on task in the classroom. In addition, Jason had a positive behavior intervention plan (PBIP) in place in the classroom, and this plan likely provided his teacher with effective strategies to regulate his behavior in the classroom. This is important to note because Jason’s mother was not implementing any type of behavior supports at home prior to treatment. She reported feeling “unequipped with knowledge of effective behaviors strategies” and clinical observations revealed that she lacked the ability to engage in age-appropriate play and to create warm social interactions with her son. In addition, she reported that her advanced age (late 50s) and numerous health problems (see “Complicating Factors” section) made it difficult for to find the energy and interest to engage in appropriate play with Jason. Although attentive, Jason’s mother looked physically uncomfortable when sitting on the floor with him and she also appeared lethargic in some sessions, moving and responding slowly during play. The therapists were able move Jason to the table. These skills deficits had interfered with her ability to create warm, playful interaction with Jason and likely affected Jason’s willingness to comply in the home. For these reasons, PCIT was recommended as this treatment was designed to foster and restore positive child–parent relationships along with building child compliance (Eyberg et al., 1995). Jason’s mother agreed to participate in PCIT and reported commitment to completing treatment.
7 Course of Treatment and Assessment of Progress
Over the course of 15 weekly sessions, treatment was provided utilizing the manualized PCIT protocol (Eyberg & Pincus, 1999). Symptoms of noncompliance and ASD-related behaviors were addressed through differential attention for prosocial behaviors (e.g., eye contact, age-appropriate behaviors) and planned ignoring for mild inappropriate behavior (e.g., repeatedly asking, “what time is it?”). Each session lasted about 1 hr, with two of the sessions being “teach sessions” during which Jason’s mother was taught the core skills of CDI and PDI without Jason present. The CDI teach session involved teaching Jason’s mother how to follow his lead during “special play time” while also attending to his positive behaviors through the use of behavior descriptions (e.g., “you stacked the blocks”), verbal reflections (e.g., “you said this is fun!”), and labeled praises for appropriate behavior (e.g., “I like the way you are playing so gently with the toys” and “thank you for making eye contact with me”). Jason’s mother was taught to avoid giving commands, criticisms, and asking questions during special playtime because these actions can take away from the child’s lead. Throughout treatment, Jason’s mother was instructed to practice the core CDI skills at home daily during 5 min of special playtime. When Jason engaged in minor inappropriate behaviors such as excessive talking or engaged in restricted interests (e.g., holding a stuffed animal in hand and using it to talk to others), his mother was instructed to implement planned ignoring for these behaviors (e.g., turn her body slightly away from him) while also being on the look-out for positive opposite behaviors that she could praise (e.g., I like how you’re sitting nicely in your chair).
The therapists used the PCIT manual to coach the mother through a bug-in-ear technology. This wireless headset provided two-way communication between the parent and the therapist. The therapists watched the parent–child dyad through a video monitor. At the start of each CDI session, mothers’ skills were coded using the Dyadic Parent-Child Interaction Coding System–Fourth Edition (DPICS; Eyberg, Ginn, Bhuiyan, & Boggs, 2014) for the first 5 min. The DPICS assessed the quality of caregiver–child interactions and was used to depict parent progress in mastery of CDI and PDI skills. This enabled the parent to practice their CDI skills while the therapist refrained from providing any feedback. Once the mother achieved CDI mastery by providing 10 behavioral descriptions, 10 reflections, and 10 labeled praises within the 5-min observation, she advanced to the PDI phase. Jason’s mother’s progress toward CDI mastery skills is shown in Figure 1. Upon treatment initiation, Jason and his mother had trouble interacting and playing together. His mother appeared to be uncomfortable during play in both CDI 1 and CDI 2. She had difficulty engaging with Jason and mirroring his type of play, one reason being that Jason’s play was very repetitive in nature. The therapist provided feedback to help the mother engage with Jason at his play level. While caregiver was encouraged to meet Jason at his level initially, even when play was repetitive, over time, we encouraged mother to expand her statements to include a wider range of toys and topics. During CDI 3 and CDI 4, Jason’s interactions with his mother became more playful and his mother became more engaged. She had increased her number of reflections and behavior descriptions, which visibly affected her play relationship with Jason. However, as Jason’s mother progressed throughout the first phase of treatment, she consistently demonstrated lower scores on labeled praises in comparison with reflections and behavior descriptions (see Figure 1); therefore, the therapist chose to provide specific coaching in increasing labeled praises during CDI 5 and CDI 6.

Mother’s progress in mastering PCIT CDI skills.
After 5 weeks of hard work, Jason’s mother met mastery criteria during the CDI 6 session and was ready to transition to PDI. Toward the end of this phase in treatment, there was a noticeable difference in the interactions between Jason and his mother. As previously noted, some youth with ASD prefer to play alone rather than play with another person. Through participation in PCIT play sessions, Jason learned to value the presence of a playmate. Due to mother’s increased engagement during these individual sessions, Jason began to look forward to playing “with” her rather than just playing near her. Thus, PCIT sessions had a positive impact on Jason’s prosocial play skills, despite his ASD.
Following CDI, the PDI phase of treatment consisted of teaching Jason’s mother effective discipline strategies such as giving effective commands and following through with praise for compliance or implementing a time-out procedure for noncompliance. Effective commands are specific, direct statements that make it evident that the child is being instructed to do something rather than being asked. They are stated in a positive manner so that the child is being told what to do rather than what not to do. In addition, they are developmentally appropriate so that the child is able to understand what is expected of them and consequently to comply. In the PDI teach session, the therapists demonstrated how to give effective commands and how to implement the time-out sequence for noncompliance prior to allowing Jason’s mother to role-play and receive feedback. During the first PDI coach session, the therapists taught Jason the consequences of noncompliance (e.g., time-out procedure), by role-playing with a teddy bear as recommended in the PCIT manual. Throughout PDI sessions, Jason’s mother struggled with formulating direct commands. For example, she frequently gave commands in the form of a question, “Would you please hand me the red Lego” and “Will you come sit next to me?” Despite repeated prompting and six sessions of PDI coaching, Jason’s mother was unable to fully meet the PDI mastery criteria goals of using effective direct commands at least 75% of the time, achieving 100% child compliance, and 100% correct follow-through to commands. In PDI 7, she met mastery criteria for direct commands (e.g., 88% accuracy) but Jason only complied to 69% of direct commands and her follow-through accuracy was only 56%.
The Eyberg Child Behavior Inventory (ECBI; Eyberg & Pincus, 1999) was used to assess Jason’s behavior at home over the course of treatment. His mother completed it each week upon arrival to each therapy session. The 36-question inventory contains a 7-point intensity scale and a yes-or-no problem scale and has demonstrated a reliable and valid measure of response to intervention for PCIT. Raw scores were summed and converted to T-scores. A T-score of 60 or higher is considered “clinical,” and parents must rate their child with a T-score of 55 or lower prior to discharge. In a restandardization study (Eyberg & Pincus, 1999), the average internal consistency of the coefficients was .95 for the intensity scale and .93 for the problem scale. These strong coefficients of internal consistency are found across major demographic subgroups as well as clinical samples. Finally, the ECBI has demonstrated excellent convergent and discriminant validity when compared with gold-standard assessments of behavior (e.g., high correlation with the CBCL, and ability to discriminate between conduct disorder and nonreferred samples). In addition, the ECBI measure has been shown to be consistent within the ASD population. Jeter et al. (2017) demonstrated that the factors of emotional reactivity, conduct problems, defiant behavior, and attention problems identified among the ASD sample align closely with the factors identified among typically developing youth. By PDI 7, Jason had ECBI scores of 55 on the problem scale and 45 on the intensity scale (see Figure 2). Due to low ECBI scores in Figure 2, the therapist decided to discharge Jason from treatment at this session.
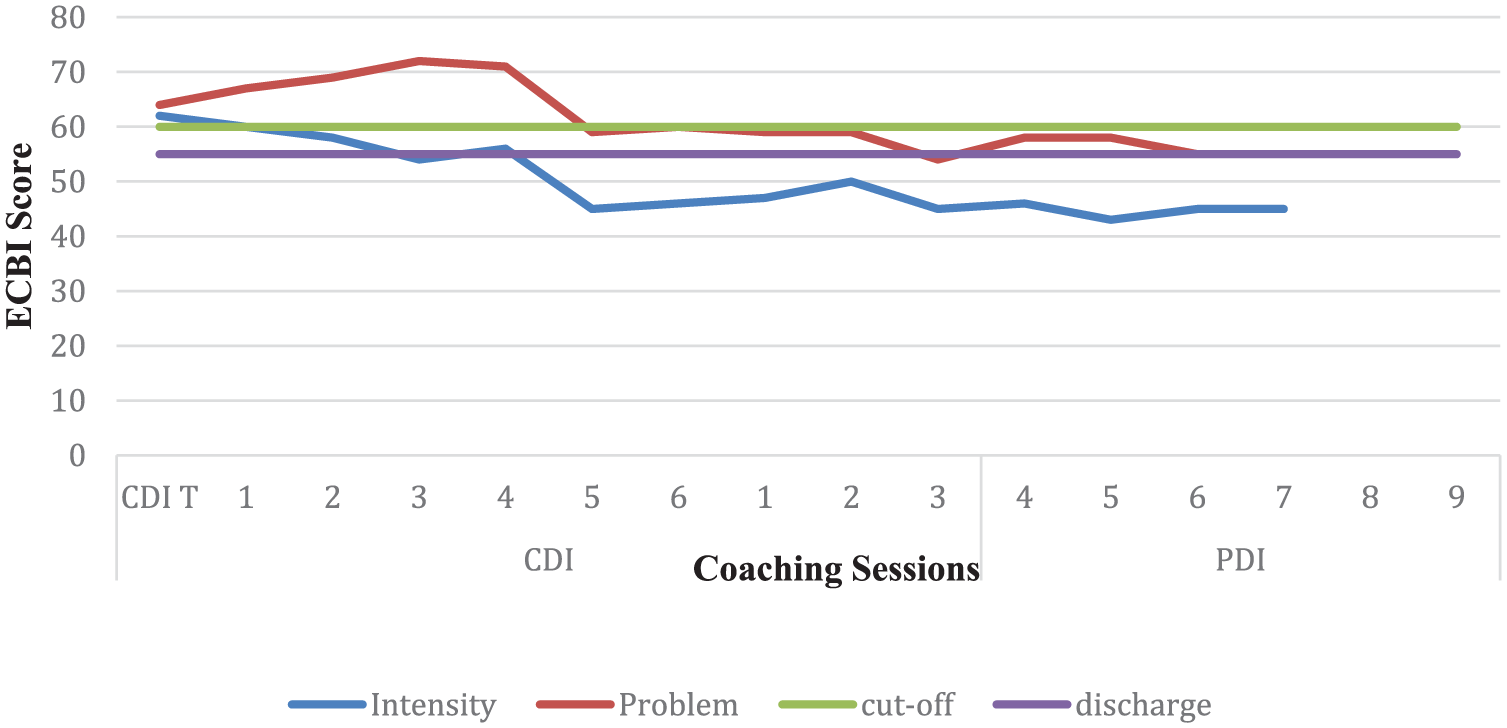
Mother’s ECBI ratings throughout treatment.
8 Complicating Factors
During the course of treatment, there were some complicating factors that interfered with treatment progress. First, Jason’s strong interests and repetitive behaviors, characteristic symptoms of ASD, made it difficult for his mother to engage in play with him. For example, Jason had the tendency to repetitively touch or move objects, which, in many cases, made it difficult for his mother to engage in direct play with him. When he was moving objects around, she could describe his behaviors, but at some point, it became important to ignore repetitive movements when they directly interfered with joint play. Jason brought a stuffed animal to sessions early in treatment, and it tended to overshadow the play with his mother, as he would pick up the animal and hold it limiting his use of both hands to engage in building or play with his mother. He would also use the stuffed animal to talk to his mother, which was not age-appropriate and greatly annoyed his mother. In this case, we discussed with mother why she allowed Jason to take the animal in public, and she said, it was something that Jason insisted on carrying throughout the day. Eventually, with mother’s support, we decided to not allow the stuffed animal into the therapy room. As such, Jason’s attention was redirected to objects in the playroom. If Jason became fixated on an object early in session, the therapists would coach mother to use enthusiasm and creative play with toys to capture Jason’s interest. Once he engaged, we then coached mother to use her CDI skills to keep Jason engaged in functional play with her.
In addition, there were complicating factors related to Jason’s mother and her overall presentation. In comparison with other parents who typically participate in PCIT, Jason’s mother was much older in age (e.g., late 50s). She repeatedly reported ongoing health issues concerning her back and neck, which definitely impeded her ability to play. She also suffered from headaches that affected her energy level. Although the relationship between parental age and child response has not been studied directly as it relates to PCIT, we hypothesized that Jason’s mother’s age and health status did have some impact on her enthusiasm and ability to play during the sessions. For example, during the first several sessions of CDI, Jason’s mother had a hard time imitating the type of play that he was doing. Instead of mimicking his play, she just sat next to him and watched him play. Therapists had to provide extensive coaching support to get mother to engage in very minimal play activity. Even so, Jason’s mother was rarely enthusiastic and energetic.
In addition, Jason’s mother rarely completed her homework assignments, during CDI and PDI. This limited her practice with skills outside of treatment and affected her ability to meet full mastery criteria for PDI, as well as maintain high levels of CDI skill fluency over the course of treatment. In fact, even during treatment sessions, there were times when Jason’s mother appeared tired and distracted by the presence of neck/back or head pain, which affected her interest in play and her ability to be enthusiastic and playful.
Finally, another complicating factor that interfered with generalization of new skills to the home setting was our inability to get Jason’s father engaged in treatment. Jason’s father declined participation in treatment in the clinic and was not interested in learning strategies at home from his wife, despite his wife’s commitment to treatment. In fact, Jason’s mother reported that her husband did not assist with any of the physical activities involved in Jason’s daily care and he would not participate in any therapy recommendations. We offered handouts for her to share with her husband if he should become interested but neither she nor we were able to garner father’s support for treatment. This may have affected mother’s ability to practice in the home setting, if her husband was not supportive of any new information or interventions. We encouraged mother to continue to practice her skills at home whenever possible as she was committed to attending therapy sessions as demonstrated by weekly attendance, on-time arrival, patience with the time it took her to learn the new skills, and alert focus during sessions.
9 Access and Barriers to Care
There were no pressing barriers to care. Jason and his mother were present at all sessions except for one, due to illness. Jason’s family had health insurance to cover the cost of treatment and our clinic was located close enough to home that transportation was easy and minimized absences from school.
10 Follow-Up
We were unable to follow up with the family because they declined.
11 Treatment Implications of the Case
This article describes the use of PCIT to treat disruptive behaviors in a 7-year-old boy with ASD. Our treatment focused on Jason’s difficulties with noncompliance and repetitive behaviors. Throughout the treatment, his mother was taught to use positive reinforcement for appropriate behavior and differential attention to shape desired behaviors. For example, mother was instructed to ignore repetitive comments (e.g., excessive questioning or whining) and to praise positive social behaviors (e.g., eye contact, big boy voice). This is important to note because Jason’s mother would often become sidetracked by his restricted interests (e.g., toy teddy bear) and repetitive questioning (repeatedly asking, “what time is it?”), overlooking opportunities to provide positive reinforcement for prosocial behaviors that he was exhibiting (making eye contact, offering a toy to mother). As Jason’s mother mastered the CDI skills, Jason became more interested in engaging in age-appropriate play, talk, and reciprocal social interactions. At the same time, parent rated Jason’s disruptive behaviors as decreasing steadily over the course of treatment. Although Jason’s mother never met the complete mastery criteria for discharge from treatment, Jason’s reductions in disruptive behavior ratings (e.g., ECBI scores) coupled with the progress mother had made over the course of treatment allowed us to make a practical decision to end treatment. Jason’s mother’s health issues seemed to be increasing and she was eager to complete treatment.
12 Recommendations to Clinicians and Students
Clinicians will find that PCIT offers a structured approach to treating disruptive behaviors among children with ASD. This case study documents the utility of PCIT for teaching a caregiver how to apply behavioral principles consistently to achieve behavior change. Although children with ASD bring additional complexities to the clinical setting in the form of restricted interests and repetitive behaviors, our experience has been similar to others in that these behaviors can be easily addressed during CDI through behavioral principles (Masse et al., 2016). Clinicians must consider ways to capitalize on each child’s unique attributes in the process of working with the parent–child dyad. For example, while Jason tended to perseverate on repetitive questions and playing with a bear early in treatment, this provided us with ample opportunity to coach the parent through planned ignoring and to teach her to apply differential attention to appropriate behaviors. As such, Jason’s mother learned to pay attention to some of his more positive social traits like sitting in his chair, using an inside voice, and making eye contact with his mother, all the while ignoring his play with a teddy bear. Similarly, when Jason made a break in repetitive statements, we coached his mother to say, “Thank you so much for allowing me to share my thoughts.” Therapists may be challenged by the presence of repetitive behaviors and restricted interests but these behaviors create new opportunities for coaching and caregiver learning.
Clinicians may also consider the utility of combining visual supports with PCIT for children with ASD. Armstrong et al. (2015) used visual supports to augment learning in a young child with ASD and found visuals were useful for teaching routines and behavioral expectations. Jason struggled with homework and bedtime routines as well as requesting help when needed and likely would have benefited from visual schedules that listed the steps of routines and behavioral expectations. Although we suggested the use of visual supports and provided literature on how to make them, Jason’s mother did not engage in this recommendation. Clinicians may need to go the extra step and help the caregiver create such tools at the end of a therapy session. Visual supports can help children remain on task while also relieving authority figures from repeatedly giving commands and can be easily implemented at home, in the community, and at school.
In terms of schools, while our client seemed to be functioning fairly well in the academic setting, this may not be the case for all children. Clinicians may consider recommending PCIT’s sister treatment for the classroom, Teacher–Child Interaction Therapy (TCIT). This therapy is a school-based intervention that implements the behavioral techniques of PCIT to assist teachers with managing disruptive student behaviors in the classrooms (McIntosh, Rizza, & Bliss, 2000). TCIT is effective for decreasing challenging and aggressive behaviors while improving overall student compliance (McIntosh et al., 2000).
There are several limitations that should be mentioned. First, Jason had recently undergone a medication change right before he entered the course of treatment. Due to this change, we cannot be certain that Jason’s behavioral changes can be attributed solely to the PCIT intervention. In addition, many of the assessment tools that were completed as a part of the multidisciplinary evaluation were not readministered post treatment. This is important to note because having these data would have aided in providing additional evidence for treatment effectiveness. Last, another limitation was that Jason’s mother did not fully meet mastery criteria during PDI. Although she did give effective direct commands 88% of the time (e.g., 75% is mastery criteria), she did not follow through correctly 75% of the time (she achieved 56% accuracy). Despite this, the therapists decided to discharge Jason based on his ECBI scores and his mother’s satisfaction with Jason’s marked behavioral improvements.
Overall, this case study provides evidence for the effectiveness of PCIT in treating a young boy with ASD and comorbid ADHD. This treatment provided Jason’s mother with positive behavior strategies to improve her relationship with her son and address compliance issues within the home setting. Although this treatment was successful with this patient, further research on PCIT and its effectiveness with the ASD population is still needed. Case studies like this one enable practitioners to share their experiences tailoring treatment to meet the unique needs of children and families affected by ASD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.