
Abstract
We present a multimedia exposure intervention for specific phobias using images and videos in a specific case of claustrophobia and acrophobia. The patient was a 47-year-old woman named “Jane” (anonymized name) who was diagnosed with fear of heights (acrophobia) and fear of confined spaces and enclosed areas (claustrophobia). The procedure was a single-case A-B design with several concurrent baselines, pre-post measurements, and two follow-ups (6 and 12 months). For the assessment, there were several questionnaires on anxiety and phobias and the continuous evaluation of anxiety and heart rate during treatment assays for each session. The treatment consisted of eight sessions of progressive multimedia exposure: images, videos, and in vivo settings. The results showed a decrease in the score for pre-post questionnaires (Z = −4.196, p < .0010) and also a total decrease in anxiety in the different baselines (PND 100%). The benefits were maintained during 1 year of follow-up. After the treatment, “Jane” could be confronted with situations she previously feared, such as being on floors of different levels (up to ninth floor), in closed places, in crowded elevators, and traveling on buses and trains for long distances.
1 Theoretical and Research Bases for Treatment
Specific phobias are very frequent in the population with prevalence between 3% and 12% (Suso-Ribera et al., 2018) and higher frequency in women, except in the blood-injection-injury subtype where they have a similar presence. In particular, acrophobia (heights) and claustrophobia (closed spaces, immobilization) present prevalence values of around 5% and 7.7%, respectively (Huppert et al., 2017; Vadakkan & Siddiqui, 2020).
Specific phobias are characterized by persistent and irrational fear, producing interference in the individual’s daily functioning and avoidance and/or escape from situations or places where the phobic object actually appears or may be imagined to appear (Eaton et al., 2018; Ruiz-García & Valero-Aguayo, 2020a). In the case of (1) phobia of heights people suffer great anxiety in or avoid high places such as balconies, terraces, stairs, etc. and in (2) claustrophobia it is characteristic for people to avoid (a) closed spaces such as elevators if they are poorly lit or crowded, (b) being in rooms with the door closed (e.g., bathrooms), or (c) being in small or immobile spaces such as interventions or medical evaluations (e.g., MRI), etc.
It has been observed that 75% of people with specific phobias fear three phobic objects on average (Serrano et al., 2019) explainable by the generalization of phobias, because people would apply the same coping strategies based mainly on escape and/or avoidance to other stimuli or situations that produce fear.
From the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5; American Psychiatric Association [APA], 2013) different subtypes of specific phobias are distinguished: animal, natural environment, blood-injection-injury, situations, and others. However, although this categorization may be heuristic (i.e., mental short-cut) some doubt can be expressed regarding its validity and utility, since we could find phobias classifiable in several categories. For example, this is the case in the fear of bridges which could be a phobia of the natural environment (e.g., heights) and also a situational phobia, etc. (Ruiz-García & Valero-Aguayo, 2017).
The greatest empirical support in the treatment of specific phobias, as well as other anxiety disorders, has been in vivo exposure (Böhnlein et al., 2020; Thng et al., 2020) but this tends to generate rejection in the patients because they have to directly face the stimuli. Around 25% of patients reject in vivo exposure, and a significant churn rate tends to occur (up to 45%) (Choy et al., 2007) therefore various types of interventions and strategies have been conducted to reduce fear gradually. some examples are: imagined exposure, systematic desensitization, progressive exposure, virtual reality exposure therapy (VRET), or multimedia exposure therapy (MET) (Ruiz-García & Valero-Aguayo, 2020a) which is presented in this paper. VRET and MET provide the therapist with more control over phobic stimuli in addition to preserving the privacy and safety of patients.
In recent decades, interventions have been affected using new technologies (computers, virtual reality devices, mobile phones, tablets, etc.) and the first interventions in virtual reality (VR) were conducted in phobia of heights through gradual exposure (Rothbaum et al., 1995). Exposure through VR for specific phobias has been effective for various case types: fear of spiders, fear of flying, social anxiety and fear of public speaking, claustrophobia, fear of driving, acrophobia, fear of snakes, cockroaches and mice, dental phobia, shark phobia, etc. (da Costa et al., 2018; Kaussner et al., 2020; Malbos et al., 2020; Raghav et al., 2016, 2019; Serrano et al., 2019; Valmaggia et al., 2016). Although VR devices have decreased in price (Bun et al., 2017), to our knowledge there are no related scenarios or elaborate stimuli for all types of phobias and there is only software for more common phobias (e.g., fear of dogs, spiders, cockroaches, heights, etc.). The preparation of this material is usually expensive for a day clinic therapist, due to their lack of programing, and technology skills or the cost of hiring a professional technology designer.
Faced with this situation, we propose multimedia exposure therapy (MET) as an intermediate approach, since it is easy to (1) obtain photographic or video stimuli on the Internet or (2) use a mobile phone for the autonomous approach. For the patient exposure, the therapist would not need specific equipment because normal equipment (computer, speakers, tablet, video projector, and white wall) will provide sufficient scientific guarantees when conducting the treatment in the usual clinical context (Ruiz-García & Valero-Aguayo, 2020a, 2020b, 2021).
This type of multimedia intervention has already been successfully carried out with specific phobias for various animals (dogs, cats, spiders, wasps, bees, cockroaches, etc.), driving, heights, flying, etc. (Ruiz-García & Valero-Aguayo, 2020a, 2021) in adults and also in children and adolescents for bee and wasp phobias (Ruiz-García & Valero-Aguayo, 2020b). Other successful research proposals suggest technological means including photos and videos in the treatment of blood-injection-injury phobia, hospital environment, vomiting, etc. (Bados & Coronas, 2008; Campos et al., 2019; Capafons et al., 1997; Matthews et al., 2015; Quero et al., 2014; Vansteenwegen et al., 2007).
This type of multimedia intervention is less expensive and more accessible for any clinician in private practice with a few instruments ensuring interventions on very different types of phobias with scientific guarantees. As a demonstration of this procedure, fear of heights, confined spaces, and immobilization are presented and the multimedia intervention protocol and its effectiveness eradicate the patient’s phobias (Ruiz-García & Valero-Aguayo, 2020a, 2021).
The objectives in this clinical case MET were to: (1) reduce or eliminate avoidance or escape behaviors in present or anticipated situations related to heights, confined spaces or immobilization; (2) increase exposure these stimuli and also coping capability thus reestablishing lost functionality in daily life and future projects; and (3) verify if these changes are maintained in the medium and long term.
2 Case Introduction
“Jane” was a socially and professionally active 47-year-old woman working as a sanitation company representative and married with two minor children in a family living in the province of Malaga (Spain).
“Jane” was referred by her son’s psychologist and then treated in our psychology service after discussing her problems with heights, confined spaces, and immobilization. These problems affected her daily life (not taking elevators, avoiding medical examinations, not going to dentists, not taking buses and trains, etc.) since she avoided all these situations, or if she did engage in any of them, she endured them with a high level of anxiety and discomfort. She previously had not been in psychological or psychiatric treatment.
3 Presenting Complaints
With “Jane,” her problems included fear of confined spaces, immobilization and heights in which she presented symptoms such as palpitations and tachycardia, chest tightness, dyspnea, and a sensation of suffocation. In relation to her phobia problems, she avoided medical interventions because she suffered great discomfort and anxiety when being still as in gynecological examinations (in this case her husband had intermittently forced her to undergo this revision), check-ups with the dentist, confined spaces in public transport (buses, trains, subways, and planes), use of elevators, or entering an audiometric chamber for renewal of her driver’s license (she had to complete the test with the door fully open). “Jane” informed us that if she had to enter the MRI scanner tube, she found it unbearable and even her thoughts on the tube made her very anxious. With heights, she could not look out from upper floors or even from the third to fourth floors, and on lower floors she also presented anxiety, but she could endure this. In this particular aspect she was very worried because in a few weeks she would move to her new eighth floor apartment. She believed she would be unable to hang out clothes to dry or even look out the window. In fact, when she went to see the apartment she attempted to approach the railing of the terrace and “her heart skipped a beat.”
4 History
In the evaluation, “Jane” explained that she had always disliked heights and confined spaces and these problems had increasingly interfered in her daily life in a more serious way. Her problems worsened 10 years ago when she was 37 years old, after having suffered a severe panic attack while a doctor in the emergency room prepared a line into a vein. From that point she began almost total avoidance of situations related to medical examinations (gynecological, dentists, etc.) because she had to be immobilized and this generated high anxiety. At that time her problems with confined spaces and heights were further aggravated. “Jane” explained that a few weeks before visiting the therapist, she suffered a strong panic attack inside her vehicle with locked the doors, since she had activated the door safety control for her children. When she could not find the key to open the door and exit the vehicle she felt like she was dying.
In addition, “Jane” also reported that she had stopped traveling and taking planes, something that had usually given her pleasure, and not because she was afraid of flying but because she was in a confined space, exacerbated when wearing a seat belt.
5 Assessment
For the case evaluation, a set of instruments and devices were used to evaluate general and specific anxieties as detailed below.
Semi-structured Interview for the Behavioral Assessment of any Specific Phobia (BISP) (Ruiz-García & Valero-Aguayo, 2017, 2021). Using the BISP, Phobic aspects (characteristics of situations and stimuli), antecedent and consequent situations, history of the problem, previous treatments, and interference in daily life, and coping styles are explored.
Multimedia Behavioral Avoidance Test (MBAT) (Ruiz-García & Valero-Aguayo, 2017, 2021). The MBAT is an observational test with 10 photographic elements and 10 video elements, all adapted to the anxiety stimuli of the clinical case. The images and videos were downloaded from the Internet and some elements were taken with the research team’s smart phone camera. During the evaluation, the images were presented to the patient for a few seconds and the video fragments for 30 seconds. Before each stimulus, “Jane” reported on the degree of subjective anxiety on a 0 to 10 Likert scale (not at all - very much). In addition, the reactions and emotions that the patient had regarding each of these visual stimuli were observed. These ratings and reactions were recorded in an “exposure log” where image, rating, maximum heart rate and comments on her reactions were noted.
Clinical Digital Pulse Oximeter (MD300). This is an electronic device for clinical medical use, which is placed on a participant’s finger and facilitates measurements of heart rate and blood oxygen saturation level. In each trial in the MBAT test, the therapist recorded the maximum rate the device showed on the display when each image or video appeared.
Self-Report of Relaxation and Exposure (Ruiz-García & Valero-Aguayo, 2017, 2021). In this self-report exercise, after applying the homework assignments using paper and pencil the patient recorded the relaxation and self-exposure tests she carried out (as indicated by the therapist). In the first part, the relaxation tests using abdominal breathing were recorded, indicating the degree of relaxation achieved in each daily exercise (0–10 point Likert scale). In the second part, the patient had to record the description of the situation, time elapsed, and subjective anxiety (Likert scale 0–10) when she encountered any of the feared stimuli.
Computer, sound speakers, projector, and projector screen. The researchers used a laptop with Windows 7 as the operating system, the video and photo display software VLC Media Player, 5 W powered loudspeakers for videos with sound, and a video projector located at one end of the laboratory. At the other end there was a white 2 m × 3 m screen for projecting the images and videos.
State-Trait Anxiety Inventory (STAI) (Spielberger et al., 1986). The STAI allows an objective measure of self-assessment of both trait and state anxiety. It is made up of 40 items in total, and is a highly reliable test, with a range of α = .93 to .87.
Fear Survey Schedule III (FSS-III-122) or General Fear Inventory (Wolpe & Lang, 1964; Spanish version of the work of Carrobles et al., 1986). This is a self-report measure composed of 122 items, which refer to a wide range of fears: animal, agoraphobic, social, sexual, etc., where the degree of fear is indicated on a scale of 1 to 5. This inventory has an internal consistency of α = .97.
Fear Questionnaire (FQ) (Marks & Mathews, 1979; Spanish adaptation of the work of Mathews et al., 1986). The FQ consists of 24 items and evaluates avoidance, anxious and depressive responses, and disability, corresponding to agoraphobia, blood-injection-injury phobia, social phobia, and the main phobia where the patient requests treatment. This instrument has shown good internal consistency, Cronbach’s alpha between .83 and .86 for the total score; and between .71 and .83 in the three subscales for the clinical population.
Inadaptation Scale (IS) (Echeburúa et al., 2000). The IS evaluates the degree to which the disorder affects various areas of the individual such as studies, social life, free time, relationship with a partner, family life, and degree of global maladjustment. It consists of six items and the responses score the degree of interference (from 0 to 6), with an internal consistency of .94.
Acrophobia Questionnaire (AQ) (Cohen, 1977; Spanish version in McCabe et al., 2005). The AQ evaluates severity of anxiety and avoidance related to different situations that have to do with heights. It consists of 40 items divided into two subscales. On the one hand, there is an anxiety subscale where it is necessary to indicate the degree of anxiety, tension, or discomfort caused in the situations described, responding on a 0 to 6 point Likert-type scale (“no anxiety, calm and relaxed” - “extremely anxious”); and on the other hand, there is an avoidance subscale, where the response is coded on a 0 to 2 point Likert-type scale (“I would not try to avoid it” - “I would not bear it under any circumstances”). It has shown reliability, using the Spearman-Brown correction, of r = .82 for the anxiety scale, and of r = .70 for the avoidance scale; and good test-retest reliability (.86 and .82, respectively) after 3 months for both scales.
Questionnaire of Situations Triggers in Fear of Flying (QPVR-R is the Spanish acronym) (Bornas et al., 1999). In the QPVR-R, 31 situations related to traveling by plane are described, contemplating days before traveling while making preparations for the trip, during the flight including flight situations such as sudden descents, turbulence, fastening the seatbelt, landing, take off, accidents, and situations in the airport terminal, etc. The response coding is given on a 1 to 9 point Likert-type scale (“Minimum-Maximum”). The total questionnaire has shown Cronbach’s alpha in the general range of .87 to .93 for individuals with fear of flying.
Claustrophobia Questionnaire (CLQ) (Radomsky et al., 2001; Spanish adaptation by Martínez-Valls et al., 2003). The CLQ is a 23-item questionnaire evaluating claustrophobia, and its components of asphyxia and inability to escape (movement restriction) (McCabe et al., 2005). Responses are coded using a 0 to 4 point Likert scale from “Not at all anxious” to “Extremely anxious.” The questionnaire has shown good internal consistency for both the full scale between .88 (Cronbach alpha) and .77 (correlation between the two halves). As for the subscales, asphyxia has .83 (Cronbach alpha) and .74 (two halves correlation), and restriction has 0.84 (Cronbach alpha) and 0.77 (two halves correlation) and a high correlation with other measures of trait anxiety, vulnerability to anxiety, panic, agoraphobia, and other fears.
Elevator Phobia Questionnaire (CFAS is the Spanish acronym) (Ruiz-García & Valero-Aguayo, 2017, 2021). The scale includes 32 situations associated with elevator use. For example, type of elevator, lighting, number of people entering the elevator, floor to which the patient is headed, space inside the elevator, type of floor, anticipating the use of the elevator, etc. For each of the stimulating situations, the patient must answer questions using a 0 to 10 point Likert scale (0: absence of anxiety to 10: maximum anxiety).
6 Case Conceptualization
For the explanation of the case, a functional analysis was carried out with the hypotheses of H1: origin and H2: maintenance of the problem. “Jane” always had difficulties with confined spaces, being immobilized, and heights, but over a period of about 10 years the problems had worsened, as a result of a medical intervention where she had to remain immobile and consequently suffered a severe panic attack. After this episode, her problems have been aggravating, producing generalization to other situations in which she previously had no problems, such as flying, something she previously could do without problem. Hence, we hypothesize that she acquired that phobia with a high level of anxiety from the classical conditioning for that serious episode of panic, and subsequently the phobias have been maintained by the contingencies of escape and avoidance regarding those situations (negative reinforcement). In this way, the problems of phobias in these places and situations have never been faced, and the extinction of physiological and cognitive anxiety responses has not been permitted. Indeed, they have increased when generalized to other situations with some physical similarity such as other enclosed places, other types of transportation and other high-altitude places that she had always avoided visiting. In this way, the phobia problems of “Jane” have been maintained by continued escape and avoidance contingencies, which have not allowed the extinction of the physiological responses from the first episodes of panic attack. In this study, no other organic variables have been detected that could maintain these problems. In any case, their worsening in recent years could also be attributed to their heavy workload, in addition to family care for children with behavioral difficulties.
In the evaluation, high scores were observed in the specific instruments that evaluated the patient’s phobia problems, specifically in MBAT, FQ, CLQ, CFAS, AQ, QPVR-R, and IS. These results are related to the data collected through the behavioral interview. In the most general instruments (STAI and FSS-III-122), because the patient’s phobia problems were specific she did not present high scores (see Table 1). Thus, in the pre-treatment evaluation “Jane” obtained a mean subjective anxiety score of 9.3 in MBAT images and a very high anxiety score of 9.6 in MBAT videos. Regarding mean maximum heart rate (MHR) she obtained normal scores of 71.9 and 69.55, respectively. Regarding the evaluation with questionnaires in STAI, which determine the level of general anxiety, she obtained a score of 15 for Anxiety State (25th percentile, a low degree of anxiety) which indicates that she currently experiences some anxiety, and in Anxiety I she had a score of 29 (65th percentile, a moderately high degree of anxiety) which demonstrates that “Jane” was prone to anxiety. In the Fear Survey Schedule III (FSS-III-122) she obtained a score of 303 which is low and may indicate the presence of more specific problems. In the Fear Questionnaire (FQ) she obtained the following results in the seven different subscales: main phobia with a score of 8; total phobia: 38; Agoraphobia: 8; blood-injection-injury phobia: 20; social phobia: 20; anxiety and depression subscale: 34; degree of interference in daily life: 6. With these results, we can affirm that there are high levels of phobic anxiety and avoidance of and/or escape from situations that produce anxiety. In addition, a specific Claustrophobia Questionnaire (CLQ) was used, whereby in the Asphyxia and Restriction subscales, 33 and 25 points, respectively, were obtained with a total score of 64; the Acrophobia Questionnaire (AQ) obtained a score of 22 on the Anxiety Scale and 9 on the Avoidance Scale; in the Elevator Phobia Questionnaire (CFA) she obtained a total score of 130; and in the Questionnaire of Situations Triggers in Fear of Flying (QPVR-R) she obtained a score of 125. Finally, on the Inadaptation Scale (IS) she obtained a total score of 23, demonstrating that her problems have a high interference in her daily life. From all of the above, it can be concluded that “Jane” had a DSM-5 diagnosis of a specific phobia (APA, 2013) of heights, confined spaces, and immobilization.
Main Data from Pre, Post, and Follow-Ups 1 and 2 (6 Months and 1 Year).

So, we can conclude that “Jane” presented intense levels of anxiety and avoidance in a variety of situations. Her daily life was currently being affected, as she avoided medical check-ups involving immobilization. If she engaged in them it was with high anxiety and suffering panic attacks (dentist, blood extraction, gynecologist, etc.). She did not go to high places to look out from terraces or balconies, and she was afraid to move to her new home on the eighth floor due to extreme anxiety. She had been avoiding airplanes, buses and trains for some time because it meant confinement for long periods; and for her this was an important limitation as she always liked traveling.
7 Course of Treatment and Assessment of Progress
For the intervention of the case a behavioral-based treatment protocol using progressive multimedia exposure was applied (Ruiz-García & Valero-Aguayo, 2017, 2020a, 2021). Through this treatment it was sought to generate the necessary conditions for the desensitization of the specific phobias of “Jane.” The protocol used different intervention phases that ended in the necessary in vivo exposure to the feared stimuli. Previously, in the first evaluation session, the patient signed an informed consent and the behavioral interview for phobias was applied, followed by an MBAT adapted to the stimulation that produced fear in “Jane.” Along with the protocol, a counter conditioned response to anxiety was used, which was achieved by applying the abdominal or diaphragmatic respiration technique as a counter-conditioning to anxiety.
The phases of the progressive multimedia exposure protocol were as follows (Ruiz-García & Valero-Aguayo, 2020a, 2021): exposure using photographs, exposure using videos, and in vivo exposure using real stimuli.
Exposure Phase with Photographs
High-quality photographs were used that assembled situations and elements related to the phobic fear in the patient (confined spaces, tightly fastened vehicle belts, heights from different levels and places (apartment blocks, skyscrapers, stairwells, etc.). These showed the stimuli and feared situations in a focused way, without distractions and with varied formats. The therapist guided the breathing exercise when necessary, encouraged observing the elements presented, and gave feedback and social reinforcement for the progress and control of the situation achieved. Anxiety decreased by five points, subjective anxiety tests with photographs and videos were mixed in the same session, and maximum heart rate measurements were taken using the digital pulse oximeter.
Exposure Phase with Videos
High-quality videos specific to this patient were used and in some cases researchers produced their own videos. During the exposure each video appeared for a duration of 1 to 3 minutes and at the same time, subjective anxiety and maximum heart rate reached were recorded. As in the previous phase, the therapist guided the breathing exercise when necessary, encouraged the patient to continue exposing herself to the material, and gave social reinforcement regarding the achievements obtained.
Exposure Phase with Real Stimuli
Finally, once the anxiety scores had been reduced to between 0 and 3, the therapist facilitated or created live exposure situations such as hanging clothes in the stairwell of the building at different heights, entering the elevator, varying the number of people inside, etc. In real situations, the therapist asked the patient questions approximately every 3 minutes and recorded the anxiety assessment that “Jane” had at that time.
A total of eight sessions were held with between 50 and 60 minutes per session spread over 10 weeks, including a period without sessions for the Christmas vacation period. Two evaluation sessions (pre and post) and two follow-up sessions were also held. In each intervention session, approximately 20 items (10 photographs and 10 videos) were presented. The treatment is described below (see Table 2). The photographs and videos used gradually, represented situations in lifts (different degrees of lighting, dimensions, passengers, etc.), aircraft cabins (use of belts, turbulence, etc.), medical or clinical procedures where one person must remain still (scanner tubes, blood extraction, dentists, etc.), closes paces (people hidden in cupboards, o similar), heights from different floors and places (skyscrapers, blocks of flats, cranes, etc.). In all the multimedia sessions, a variety of photographs and videos showing these situations were presented.
Content of Treatment Sessions and Inter-Session Homework.

In the first evaluation session (pre), after the patient signed the informed consent, the behavioral interview, general and specific questionnaires were carried out. Then at a later stage a MBAT with photos and videos with the stimuli material adapted to the stimuli and situations that produced the patient’s phobia.
In the intervention period, in the first session, after returning the evaluation results, abdominal respiratory training was carried out. From the first session, abdominal breathing exercises were prescribed for home practice, twice daily, for 10 to 15 minutes, which had to be noted in the patient’s self-record of relaxation and exposures. At first there were no assigned exposure tasks and “Jane” only had to write down related situations that she experienced.
In the first, second, and third sessions, the multimedia exposure trials were carried out as previously described.
In the fourth session, the self-record was reviewed, and the progressive multimedia exposure continued and afterwards immobilization situations were recreated in vivo. To do this, the procedure was to alternate restraint of the therapist and then the patient using arm compressors (rubber bands) and the office chair. First, “Jane” tied the therapist’s arms to each armrest of the chair and her legs to each front leg of the chair. Later the therapist did exactly the same procedure to “Jane.” Both situations caused a high subjective anxiety in the patient. After the reduction of her anxiety “Jane” removed the rubber bands restraining the therapist and the same procedure was performed on her, as described. In this session, it was agreed that “Jane” would make a visit to the National Museum of Airports and Air Transport outside the session, where there was an airplane passenger cabin, and she could use a seat belt. During the self-exposure situations, while practicing the abdominal relaxation technique, he had to stay at least 5 minutes in each situation or until the anxiety level was reduced.
In the fifth session, in addition to the review of the self-record and the multimedia presentation, the exposure was repeated with the patient immobilized as in the previous session, and the therapist left the room and closed the door leaving “Jane” alone inside the room. This was repeated in several increasing time trials (1, 3, and 5 minutes). In these situations, “Jane” did not present any difficulty except after the 3-minute trial when the therapist returned to the room and “Jane” explained that in being alone, she noticed a peak of anxiety, but she was able to manage the situation without calling the therapist. In the fifth session, we recreated the situation of hanging clothes at different heights on the stairs of the building. We started from the second floor and proceeded to the eighth floor. To do this, using an elastic Octopus Strap held from rail to rail, “Jane” laid out shreds of fabric that she held with tweezers. As homework, it was agreed that she should be exposed to different heights. In addition, it was recommended that she expose herself to all occasions that could occur unintentionally and to other situations she had already been exposed to in the previous week.
In session 6 we rode the elevator and in the first rehearsals the patient was with the therapist and then alone. Once anxiety in the patient was reduced, the difficulty of the exposure was increased, and internship students were gathered at the center of the elevator until it was filled (considering the safe number of people and recommended weight). With all passengers in the elevator, we took tours of all nine floors while moving around inside the elevator, thus creating a feeling within the patient of being crammed inside the confined space. After this session the patient was recommended exposure at her home on the second floor, at her mother’s fourth floor apartment and at the Interactive Music Museum in the city where there are soundproof booths that close hermetically.
In the seventh and eighth sessions, while also maintaining a multimedia exposure at the beginning of the sessions, “Jane” again hung clothes while on the top floor, rode the elevator with many other people entering and leaving on different floors, and undertook a new immobilization test wearing the restraints and getting accustomed to being alone for up to 10 minutes of immobilization. “Jane” no longer had any problems in these rehearsals. As homework she continued with breathing exercises and exposures to situations that she had already undertaken in previous weeks. Figure 1 shows the evolution of the averages for the different types of stimuli used (photographs, videos, and in vivo).
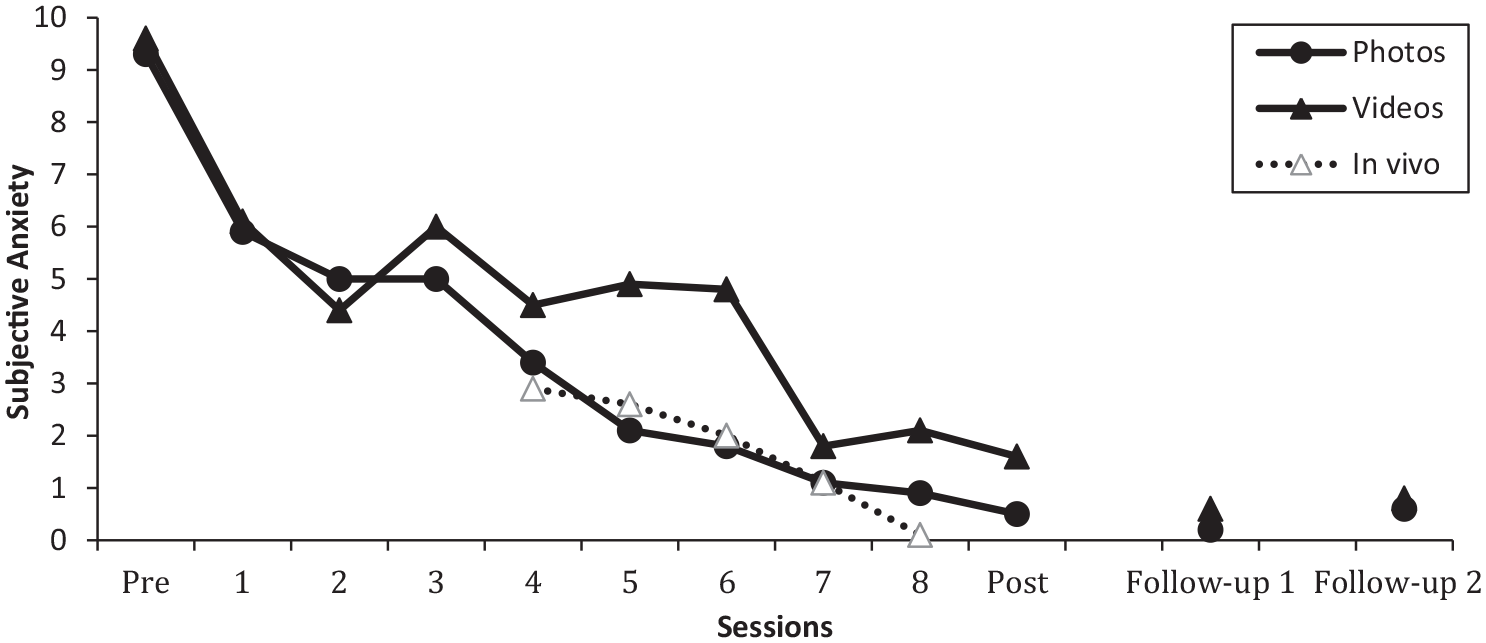
Mean of subjective anxiety per treatment session.
Before ending the intervention, the achievements and the strategies applied to prevent relapse were reviewed and the post evaluation was carried out, for which the aforementioned evaluation instruments were used. In addition, subjective anxiety and heart rate per trial were recorded in each session, as noted earlier in this paper. Figure 2 shows the degrees of anxiety that the patient registered when undertaking these tests in the situations of her daily life.
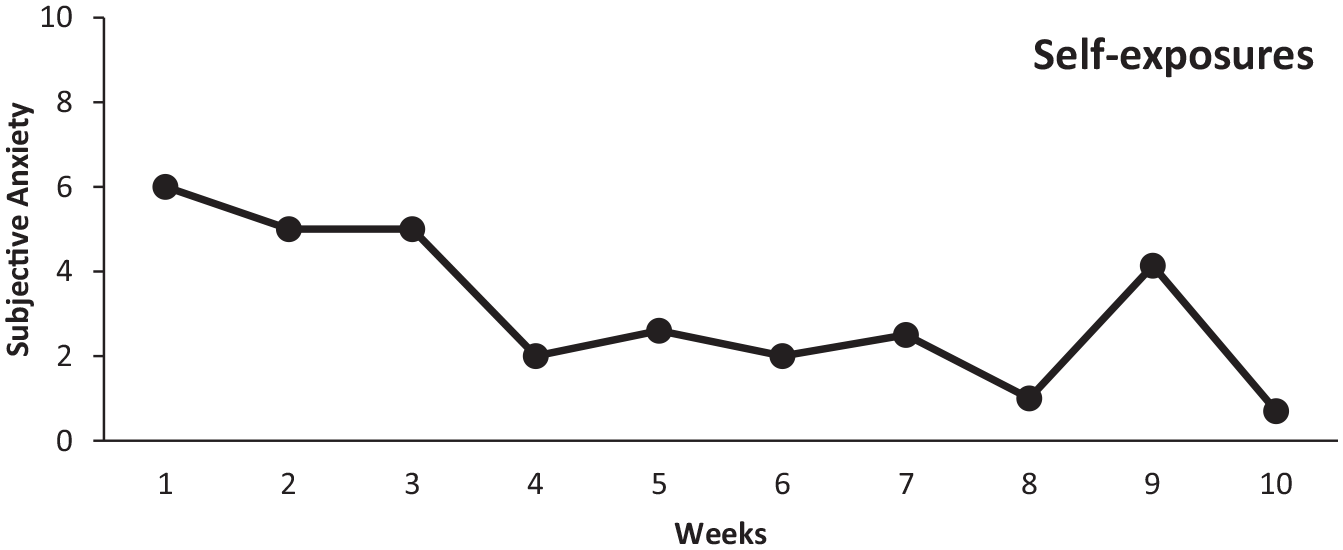
Mean of subjective anxiety per week in self-exposures.
The results of the intervention produced clinically relevant changes in the life “Jane” and at the end of the intervention, she could take elevators, stay in confined places and withstand great heights. Therefore, in addition to the objective of reducing her anxiety, it was possible to eliminate avoidance and escape regarding situations that were previously problematic for her. All of these results had a clear and positive effect on the quality of her life.
8 Complicating Factors
There were no factors that made treatment difficult. On the contrary, being a progressive exposure and at first only with images and videos, the treatment was well accepted by “Jane.” She followed procedural instructions without problems within the clinical center and also carried out the exposures and recommendations for her daily life without problems. There was only one interruption of the treatment for 2 weeks, which lengthened the process, due to the Christmas vacation period but this did not in influence the results achieved.
9 Access and Barriers to Care
It is common to find that certain objectives cannot be achieved during the intervention itself. In the case of “Jane” some medical tests such as gynecological and dental check-ups, etc., could not be performed. This was not due to a lack of interest or motivation but because of the difficulties of balancing work schedules. For “Jane” it was a great effort to attend the intervention sessions due to the level of stress and workload she had but she never missed an appointment because, according to her own explanation, “that moment was the only time of day she had to herself” and she “wanted to have the weekly session.” Those other objectives she achieved by herself in subsequent follow-ups.
10 Follow-Up
After the end of the treatment two follow-ups were carried out at 6 and 12 months where “Jane” was interviewed again and filled out the same battery of questionnaires. She explained that after these months the changes due to the intervention had been maintained, and she had continued to expose herself to various situations that for her were previously problematic but currently were not at all. During this time, she had visited her gynecologist and dentist without incidents or relevant problems. She also reported that now in her new eighth floor home she was leaning over her terrace rails enjoying sea views was hanging her clothes without problems. She used the elevator without problem to get to her apartment, and she took elevators in different buildings with and without other passengers and even filled to capacity. In addition, she has also continued to travel on buses and uses the high-speed train, which she previously would not be able to use for a long journey. In her last follow-up, she reported booking a flight to Barcelona (100 minutes of flying time) for a couple of weeks in the future. She no longer had any difficulty performing all kinds of actions indoors.
11 Treatment Implications of the Case
The case was a complete success. The life change for “Jane” was clinically and statistically significant. At the statistical level, the results were analyzed using a non-parametric Wilcoxon test where we found significant effects and the data used for their calculation are shown in Table 1. Thus, between the pre- and post-evaluations there were statistically significant changes (N = 29, Z = −4.196, p < .0001). Further, there were no statistically significant effects between post and follow-up evaluations at 6 months (N = 29, Z = −.261, p = .794); likewise, between this follow-up and the following evaluation at 12 months (N = 29, Z = −.733, p = .464). It can therefore be stated that the results were maintained over the long term up to 1 year.
In addition, a data analysis of the single-case design has been performed using the Percentage of Non-Overlapping Data (PND) (Sanz & García-Vera, 2015) that shows a 100% change between baseline diagnostics and initial treatment both in the treatment via the images and videos, which would imply maximum effectiveness of the treatment.
However, these results should be viewed with caution since it is a clinical case with a baseline and follow-up, but there is no comparison with other groups or with another form of exposure. However, this procedure has already been tested in group studies with comparisons with the group on the list of Ruiz-García and Valero-Aguayo (2020a) and also in other clinical cases with different phobias (Ruiz-García & Valero-Aguayo, 2020b, 2021). It would be an even safer step to pursue a comparison of this clinical case with other previously established treatments such as virtual reality (VR), exposure in imagination or similar, and especially to study its efficiency due to the ease of use, acceptability by the patients and cost which is assumed to be quite minor.
12 Recommendations to Clinicians and Students
This type of protocolized intervention through progressive multimedia exposure for specific phobias has yielded scientific evidence for its use by clinicians in their private clinical practice. This approach is technically simple, but with rigor it is accessible to any new or veteran therapist, since the elements to be used can be easily obtained and presented using a computer and an Internet connection. Despite its simplicity, it is necessary to possess adequate therapeutic and creativity skills to encourage and accompany the patient in confronting their phobic fears, which prevent and paralyze them or produce panic attacks. Also, the creative capacity of the clinician is needed to be able to generate different and significant situations for gradual exposure, to maximize the possibility of generalization, as well as for the final exposure to in vivo stimuli.
This type of progressive multimedia intervention can have an important day-to-day relevance for a clinician who can intervene in specific phobias using this type of protocol without large expenses related to equipment, subscriptions to software packages or great computer knowledge. Added to this is the acceptability by the patient, since it is much easier to start the treatment with exposures to photos and videos rather than starting with in vivo stimuli.
In addition, for the automatic evaluation, the research team must possess software (MBAT) that the therapist can use with his own images and videos or those media he can download from the Internet, and the patient directly indicates her responses that are registered during the treatment program. From these scores, the clinician can organize the hierarchy of stimuli necessary for progressive multimedia exposure in his specific case. Currently the research team of this paper are in possession of MBAT software with these characteristics containing specific images for blood-injection-injury phobia (Ruiz-García et al., 2019; https://www.institutoanalisisconducta.com/software).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.