
Abstract
Atopic dermatitis (AD) and allergic contact dermatitis (ACD) is a common allergic inflammatory skin disease caused by a combination of eczematous, scratching, pruritus and cutaneous sensitization with allergens. The aim of our study was to examine whether rutin, a predominant flavonoid having anti-inflammatory and antioxidative potential, modulates AD and ACD symptoms. We established an atopic dermatitis model in BALB/c mice by repeated local exposure of house dust mite (Dermatophagoides farinae) extract (DFE) and 2,4-dinitrochlorobenzene (DNCB) to the ears. In addition, 2,4-dinitroflourobenzene-sensitized a local lymph node assay was used for the ACD model. Repeated alternative treatment of DFE/DNCB caused AD symptoms. Topical application of rutin reduced AD based on ear thickness and histopathological analysis, in addition to serum IgE levels. Rutin inhibited mast cell infiltration into the ear and serum histamine level. Rutin suppressed DFE/DNCB-induced expression of interleukin (IL)-4, IL-5, IL-13, IL-31, IL-32 and interferon (INF)-γ in the tissue. In addition, rutin suppressed ACD based on ear thickness and lymphocyte proliferation, serum IgG2a levels, and expression of INF-γ, IL-4, IL-5, IL-10, IL-17 and tumour necrosis factor-α in ACD ears. This study demonstrates that rutin inhibits AD and ACD, suggesting that rutin might be a candidate for the treatment of allergic skin diseases.
Introduction
Atopic dermatitis (AD) is a chronic relapsing skin disorder with allergic inflammation and intense pruritus. AD is aggravated by various environment factors and allergens, especially house dust mites. House dust mites have been identified as causative agents affecting skin barrier function and immunological responses. In addition, AD is a chronic inflammatory skin disease with specific immune and inflammatory mechanisms. 1,2
T lymphocytes play an important role in the pathogenesis of AD with marked infiltration of activated CD4+ and CD8+ memory T-cells in the skin. 3 AD is characterized by an imbalance between Th1 and Th2 by the presence of a specific immunoglobulin (Ig) E response in association with Th2 immune responses. 4 Important roles of Th1 and Th2 cytokines in the skin inflammatory response have been confirmed in experimental models of allergen-induced allergic skin inflammation in mice with targeted deletions of these cytokines. 3 Among cytokines produced by Th2, interleukin (IL)-4, IL-5, IL-9 and IL-13 are known to be important in stimulating Th1 immune responses. IL-31 is a recently described T-cell-derived cytokine mainly produced by Th2 and related to the IL-6 cytokine family according to its structure. IL-32 induces tumour necrosis factor (TNF)-α, IL-8, and macrophage inflammatory proteins. 5,6 Mast cells play an important role in the pathogenesis of AD. Mast cells regulate inflammation and eosinophil activation by the secretion of multiple mediators. 7,8 Mast cell-derived histamine and other inflammatory mediators contribute to itching and inflammation in AD. 9
Allergic contact dermatitis (ACD) is a chronic T-cell-mediated disease caused by repeated skin exposure to contact allergens. ACD is characterized by redness, papule and vesicles, followed by scaling and dryness. 10,11 Many of the commercial formulations for the treatment of ACD is available in gel, cream, lotion or ointment but have achieved limited success. 12
Many therapeutic trials have been performed to modulate allergic skin diseases with limited success. These include prevention of Th2 responses, enhancement of Th1 responses and decrease of IgE concentration. Topical glucocorticoids are important and effective remedies for treatment of allergic skin diseases. However, it is well known that prolonged use of high dose of glucocorticoids causes a variety of side-effects. In chronic AD lesions, both Th1 and Th2 immune responses are significantly increased. Thus, different causes of allergic skin diseases could be treated by varying therapeutic strategies. Rutin is a diglycoside of quercetin, which is the predominant flavonol type of flavonoid. Rutin can be found in asparagus, tomato, orange and apple peels. It was reported that rutin has several pharmacological effects, such as antioxidative, antiplatelet and blood vessel-protective activities. 13–15 Some flavonoids, including quercetin, kaempferol, fisetin and rutin were previously shown to inhibit IgE and histamine in human mast cells. 16 However, the effect of rutin on AD and ACD has not been elucidated yet. In this study, we examined the effect of rutin on AD using the BALB/c mice model. In addition, we examined the effect of rutin on ACD using local lymph node assay (LLNA).
Materials and methods
Animals
Six-week-old female BALB/c J mice were purchased from SLC Inc (Hamamatsu, Japan). The animals were housed with 5–10 mice per cage in a laminar air flow room maintained at a temperature of 22 ± 2°C with a relative humidity of 55 ± 5% throughout the study. The care and treatment of the mice were in accordance with the guidelines established by the Public Health Service Policy on the Humane Care and Use of Laboratory Animals and were approved by the Institutional Animal Care and Use Committee.
Drugs and chemicals
Rutin was purchased from Sigma (St Louis, MO, USA). Dermatophagoides farinae extract (DFE, Greer Laboratories, Lenoir, NC, USA) was used as an antigen. All other reagents were purchased from Sigma unless otherwise stated. DFE was dissolved in phosphate-buffered saline (PBS) containing 0.5% Tween 20. 2,4-Dinitrochlorobenzene (DNCB, 1%) was dissolved in an acetone/olive oil (1:3) solution.
Induction of AD in the mouse ear
Induction of AD using DFE and DNCB was performed as previously described.
17
A schematic experimental procedure is described in Figure 1a. Mice (n = 5) were divided into four groups, and the surfaces of both ear lobes were stripped five times with surgical tape (Nichiban, Tokyo, Japan). After stripping, 20 μL of DNCB (1%) was painted on each ear and then 20 μL of DFE (10 mg/mL) four days later. Treatment of DFE/DNCB was repeated once a week alternatively for four weeks. Two weeks after the first induction, tail bleeding was performed to check the serum IgE level. After confirming an atopic condition by IgE level, ears were treated with rutin (1 or 5 μg/ear) by painting until the end of four weeks induction. Ear thicknesses and clinical scores were measured 24 h after DFE or DNCB application with a dial thickness gauge (Kori Seiki Mfg, Co, Tokyo, Japan).
Experimental design and ear thickness in AD mice. (a) Experimental design for the induction of AD. After seven days of first boosting with 1% DNCB (20 μL/ear), DFE (10 mg/mL, 20 μL/ear) and DNCB were applied to both ears once a week alternatively for four weeks (n = 5). After one week of induction, rutin (1 and 5 μg/ear) was treated every day for three weeks (n = 5). (b) Effect of rutin on ear thickness. Ear thickness was measured 24 h after DFE or DNCB application with a dial thickness gauge. Data are presented as mean ± SD of five determinations. ***P < 0.001; **P < 0.01; *P < 0.05 significantly lower than AD. AD, atopic dermatitis; DNCB, 2,4-dinitrochlorobenzene; DFE, Dermatophagoides farinae extract
At days 14 and 28, blood samples were collected by orbital puncture. Plasma was stored at −70°C for further analysis. After blood collection, ears were removed and used for histopathological analysis. The serum IgE and IgG2a levels were measured using ELISA kit (Bethyl Laboratories, Inc, Montgomery, TX, USA) according to the manufacturer's instructions. The DFE-specific IgE level was indicated by OD value. The mean absorbance of an antigen-coated well minus the mean absorbance of a non-coated well was used as the OD value of the antigen and mite extract.
Histological observation
The ears were fixed with 10% formaldehyde and embedded in paraffin. Thin 5 μm sections were stained with haematoxylin and eosin. Infiltrated lymphocytes, thickening of the epidermis and fibrosis in the dermis were observed by microscope. For measurement of mast cell infiltration, skin sections were stained with toluidine blue, and the number of mast cells in five sites chosen at random was counted. Eosinophils cells were counted blinded in 10 high-power fields at a magnification of ×400. Dermal thickness was analysed in hematoylin and eosin-stained sections viewed under a magnification of ×100. Thickness was measured in five randomly selected fields from each sample.
Realtime polymerase chain reaction
Quantitative realtime polymerase chain reaction (PCR) was carried out using the Thermal Cycler Dice TP850 (Takarabio Inc, Shiga, Japan) according to the manufacturer's protocol. Total RNA was isolated from superficial cervicel, axillary of each group. Briefly, 2 μL of cDNA (100 ng), 1 μL of sense and antisense primer solution (0.4 μmol/L), 12.5 μL of SYBR Premix Ex Taq (Takarabio Inc) and 9.5 μL of dH2O were mixed together to obtain a final 25 μL reaction mixture in each reaction tube. The conditions for PCR were similar to ones previously described 18,19 except for the primer of IL-17 (F 5′ TCC CTC TGT GAT CTG GGA AG 3′, R 5′ CTC GAC CCT GAA AGT GAA GG 3′) and IL-32 (F 5′ GCC CAA GAT CGT CAA AAA GA 3′, R 5′ ATT GTG GAC CAG GAA CTT GC 3′). The amplification conditions were 10 s at 95°C, 40 cycles of five seconds at 95°C and 30 s at 60°C, 15 s at 95°C, 30 s at 60°C, and 15 s at 95°C. The normalization and quantification of mRNA expression was performed using the TP850 software supplied by the manufacturer.
Histamine assay
The histamine content was measured by the o-phthaldialdehyde spectrofluorometric procedure as previously described.
20
The blood from the mice was centrifuged at 400
Induction of ACD in the mouse ear
The murine LLNA is recognized by the United States Interagency coordinating Committee on the Validation of Alternative Methods (ICCVAM) as a stand-alone method for hazard identification of contact hypersensitivity. 21 Induction of ACD using 0.15% 2,4-dinitroflourobenzene (DNFB) was performed as previously described. 22 Female BALB/c mice (8 weeks old) were allocated randomly to dose and control groups for each group (n = 5). A 25 μL aliquot of test solution or solvent only (4:1, acetone: olive oil, AOO) was applied daily to the dorsum of both ears of each mouse for three consecutive days (days 1–3). For the co-treatment of DNFB with either 5 or 20 μg/ear of rutin, rutin groups were treated two hours before DNFB treatment on days 1–3. The mice were rested on days 4 and 5. On day 4, 24 h after the last treatment, measurements of ear thickness were made to assess treatment-induced irritancy. For the LLNA, ³H-methyl thymidine (³H-TdR, 20 μCi/animal) was injected via the tail vein into all test and control mice. At five hours after the injection, the mice were euthanized, and the auricular lymph nodes were placed in PBS. Single-cell suspensions of lymph node in 5 mL of PBS were prepared by passage through sterile 70 μm nylon cell strainers (Falcon, Bedford, MA, USA). The lymph node cell suspension was washed twice with PBS, and the cell pellet was incubated in 5 mL of 5% trichloroacetic acid at 4°C for 18 h. Each cell pellet was resuspended in 1 mL of trichloroacetic acid and transferred to 5 mL of scintillation fluid. Incorporation of ³H-TdR was measured with a liquid scintillation counter as disintegrations per minute for each mouse.
Statistical analysis
Statistical analyses were performed using Prism 5 (GraphPad Software, San Diego, CA, USA). Treatment effects were analysed using one-way analysis of variance followed by Dunnett's test. A value of P < 0.05 was used to indicate statistically significant differences.
Results
Clinical symptoms at the inflamed site
To validate the ability of rutin on AD, rutin was painted on the ears of mice with DFE/DNCB every day during a three-week period (Figure 1a). DFE/DNCB treatment for four weeks elicited severe AD. During the induction period, we measured ear swelling after 24 h of each induction. The tendency of ear swelling of each group was similar until two weeks. After three weeks of AD induction, rutin (1 and 5 μg/ear)-treated groups showed a significant improvement of ear thickness (Figure 1b).
Histopathological observation and serum IgE
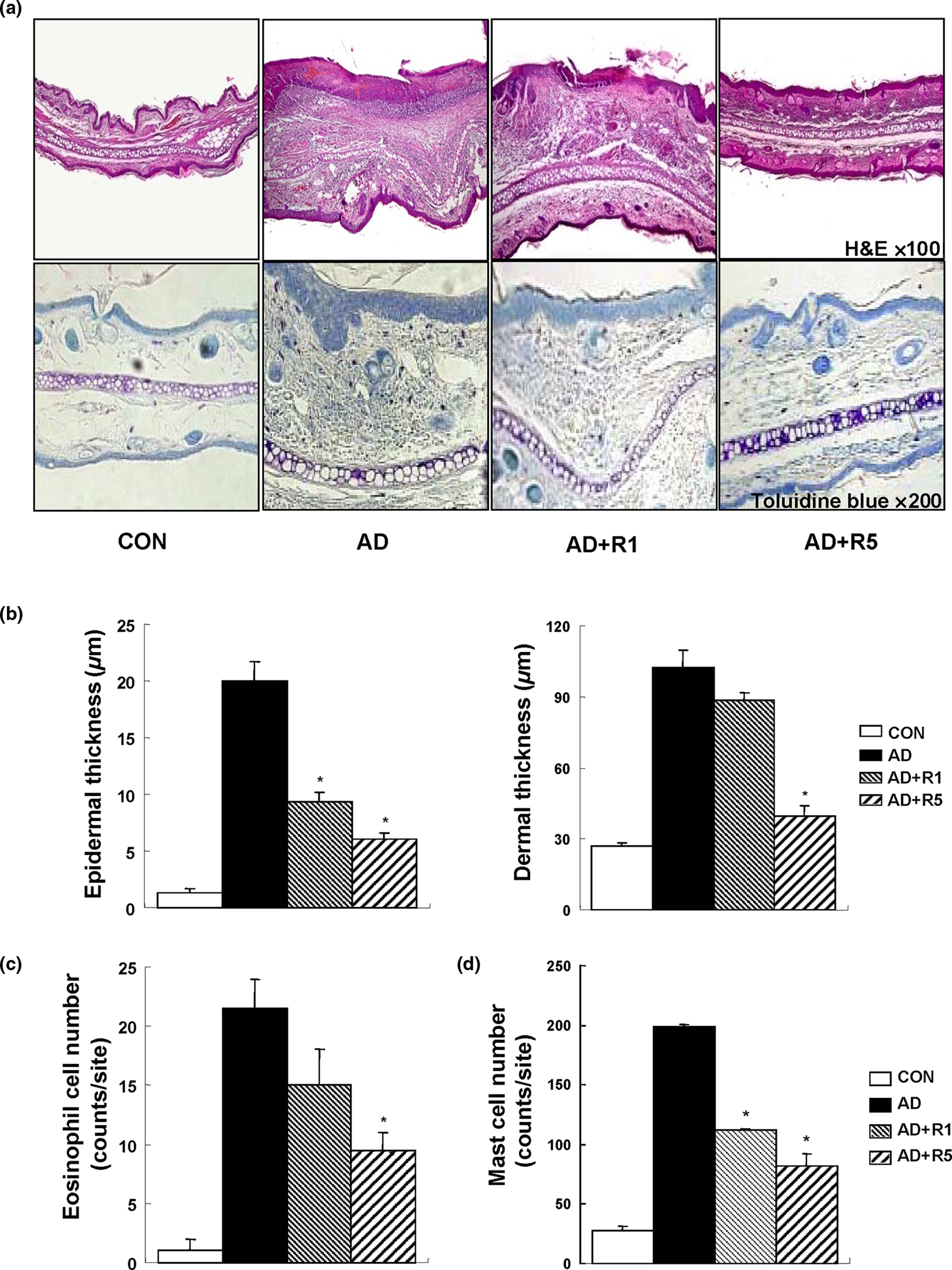
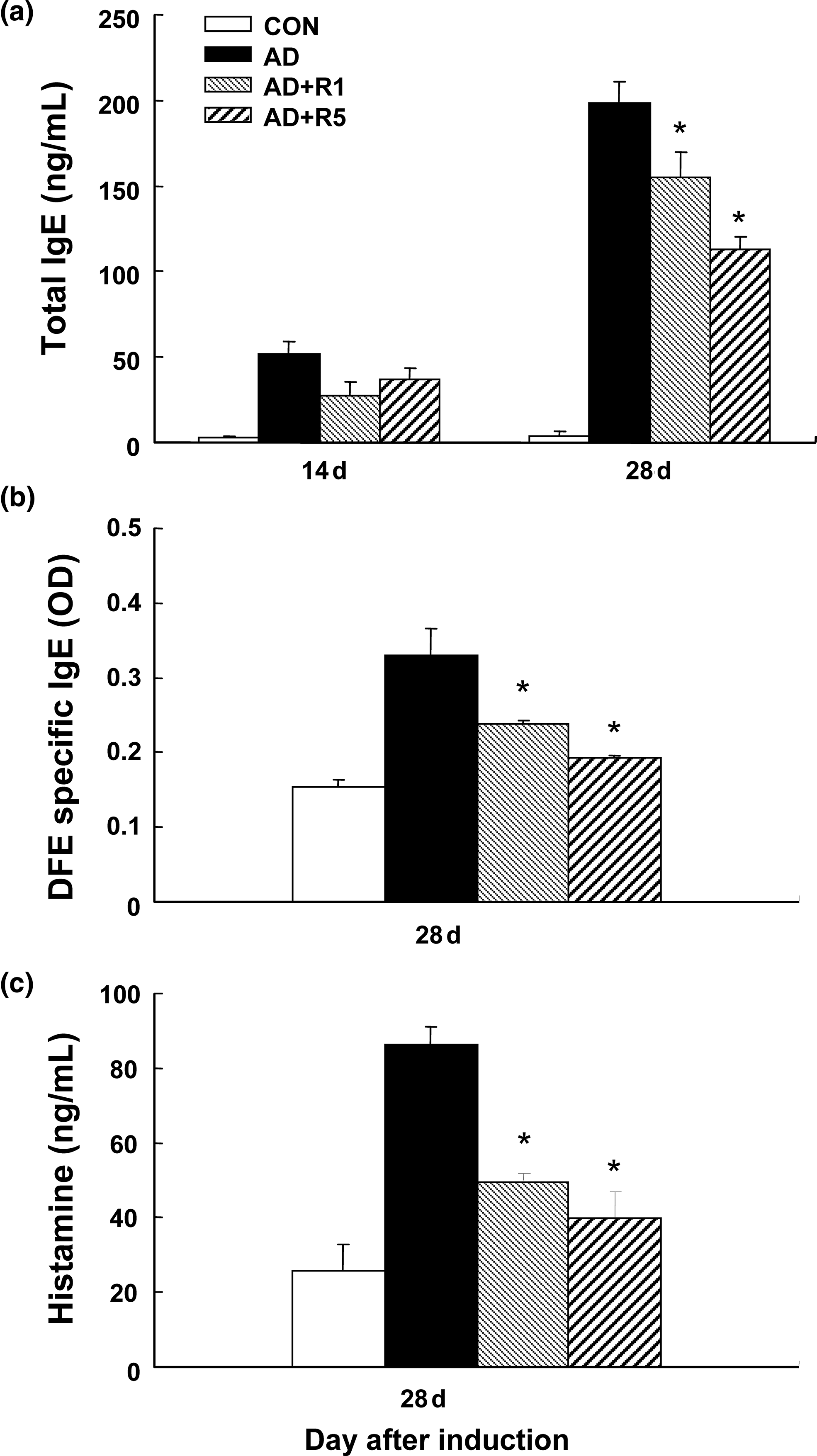
Microscopic analysis of the skin showed many alterations. These features, including hyperkeratosis, large ulcers, and acute inflammatory cell infiltration, were observed (Figure 2a). Compared with AD mice, rutin significantly reduced DFE/DNCB-induced epidermal and dermal thickness (Figure 2b), infiltration of eosinophils (Figure 2c). Chronic AD is associated with hyperproduction of IgE. We examined serum levels of total and DFE-specific IgE. Compared with the AD group, total IgE and DFE-specific IgE (Figures 3a and b) were significantly reduced in the serum of the rutin-treated (1 and 5 μg/ear) groups.
Histological analysis in AD mice. (a) Representative photomicrographs of ear sections were stained with hematoxylin and eosin (original magnification, ×100) or toluidine blue (original magnification, ×200). (b) Epidermal and dermal thickness. (c) Numbers of eosinophils. (d) Numbers of mast cells. Data are presented as mean ± SD of five determinations. *P < 0.05 significantly lower than AD. AD, atopic dermatitis (A color version of this figure is available in the online Journal) Serum IgE and histamine levels in AD mice. (a) The blood samples of vehicle, DFE/DNCB plus vehicle and DFE/DNCB plus rutin (1 and 5 μg/ear) groups were collected by orbital puncture on 28 d, and serum level of total IgE was quantified by ELISA. (b) The DFE mite specific IgE levels were measured on day 28. (c) Serum histamine levels were measured on day 28. Data are presented as mean ± SD of triplicate determinations. *P < 0.05 significantly lower than AD. AD, atopic dermatitis; DNCB, 2,4-dinitrochlorobenzene; DFE, Dermatophagoides farinae extract
Serum histamine and mast cell infiltration in the inflamed ear
Next, to understand the inhibitory mechanism of rutin, we measured a representative symptom-inducing substance, histamine. 17 Rutin inhibited the enhanced level of histamine induced by DFE/DNCB (Figure 3c). To further investigate, we assessed the effects of rutin on the infiltration of mast cells, an important effector cell and source of histamine involved in AD, into the ears. As shown in Figures 2a and d, rutin-treated group showed significantly decreased infiltration of mast cells.
Cytokine mRNA expression
We examined the effect of rutin on the inflammatory cytokines related to AD. The mRNA levels of IL-4, IL-5, IL-13, IL-31, IL-32, and INF-γ in the ear tissue were quantitatively measured by realtime PCR. Compared with the AD group, rutin significantly decreased mRNA levels of IL-4, IL-5, IL-13, IL-31 and IL-32 (Figure 4). These results suggest that rutin inhibits expression of Th2 cytokines in AD. Unexpectedly, rutin decreased the mRNA level of INF-γ, the known Th1 cytokine. This result suggests that rutin also play a suppressive role in chronic skin inflammation elicited by AD.
Expression of cytokines in the ear. The ears were excised, and total RNA was isolated. Quantitative realtime PCR was performed as described in Materials and methods. Data are presented as mean ± SD of five determinations. *P < 0.05 significantly lower than AD. AD, atopic dermatitis; PCR, polymerase chain reaction; IL, interleukin; INF-γ, interferon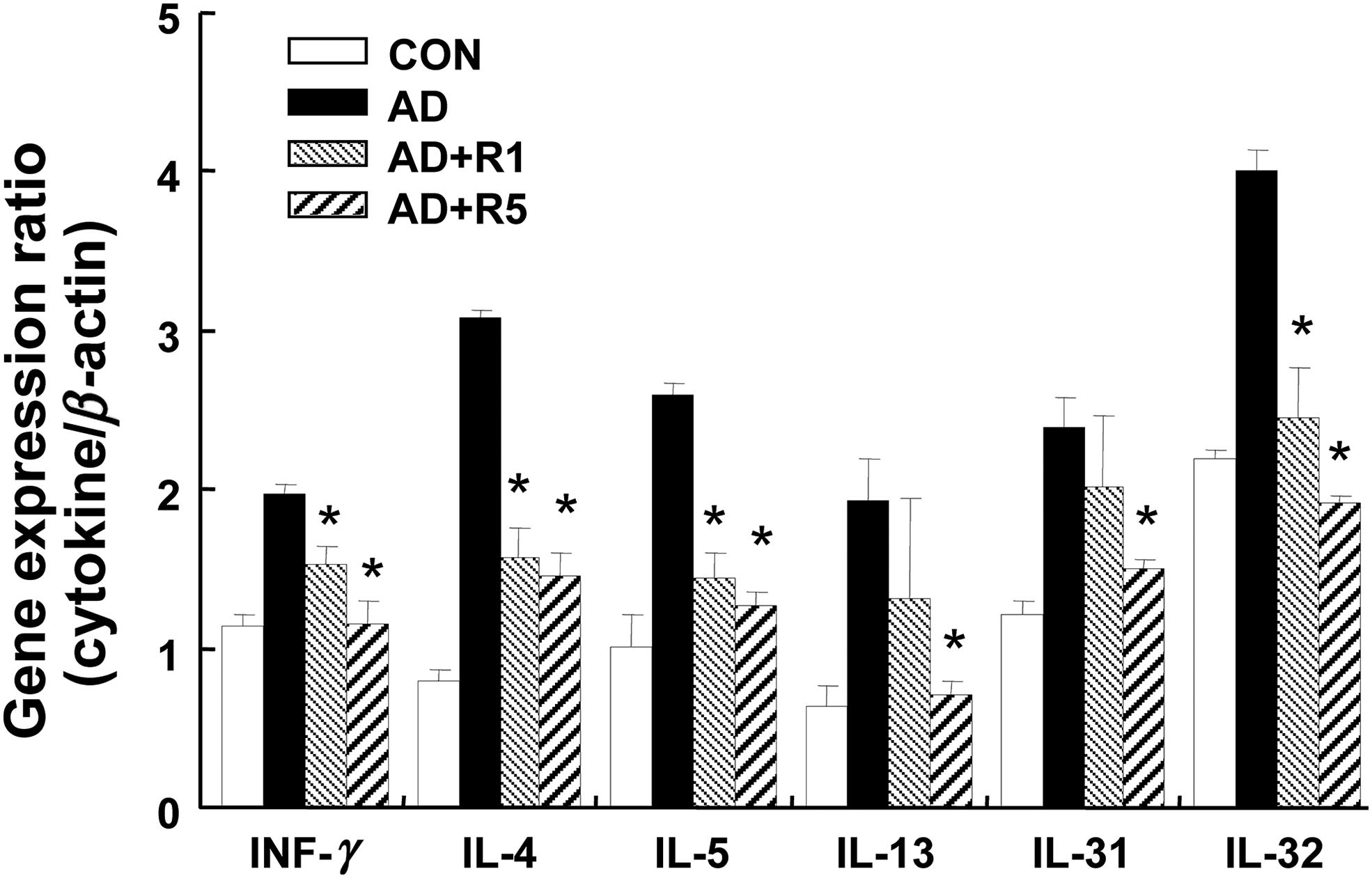
Allergic contact dermatitis
We tested the effect of rutin on the ACD using a LLNA. In the LLNA, ear swelling and lymphocyte proliferation in draining lymph nodes are used as a measure for the immune response to an applied allergen.
22,23
A schematic experimental procedure of ACD is shown in Figure 5a. LLNA was induced by the contact dermatitis sensitizer, DNFB. In spite of no changes of body weight in all groups (data not shown), significant changes have been seen in ear thickness (Figure 5b). From day 2, DNFB induced increase of ear thickness. Rutin showed significant reduction of ear thickness after three days of treatment.
Effect of rutin in ACD mice. (a) Experimental design for the sensitization of ACD. Mice (n = 5) were treated with the test article, vehicle (acetone/olive oil), positive control (0.15% DNFB, 25 μL/ear) and rutin (5, 20 μg/ear). On day 6, mice were euthanized, and the auricular lymph nodes were removed. (b) Effect of rutin on ear thickness in ACD mice. Vehicle and rutin were pretreated for two hours before DNFB. Ear thickness was measured 24 h after DNFB application with a dial thickness gauge. Data are presented as mean ± SD of five determinations. ***P < 0.001; **P < 0.01; *P < 0.05 significantly lower than ACD. DNCB, 2,4-dinitrochlorobenzene; ACD, allergic contact dermatitis; ³H-TdR, ³H-methyl thymidine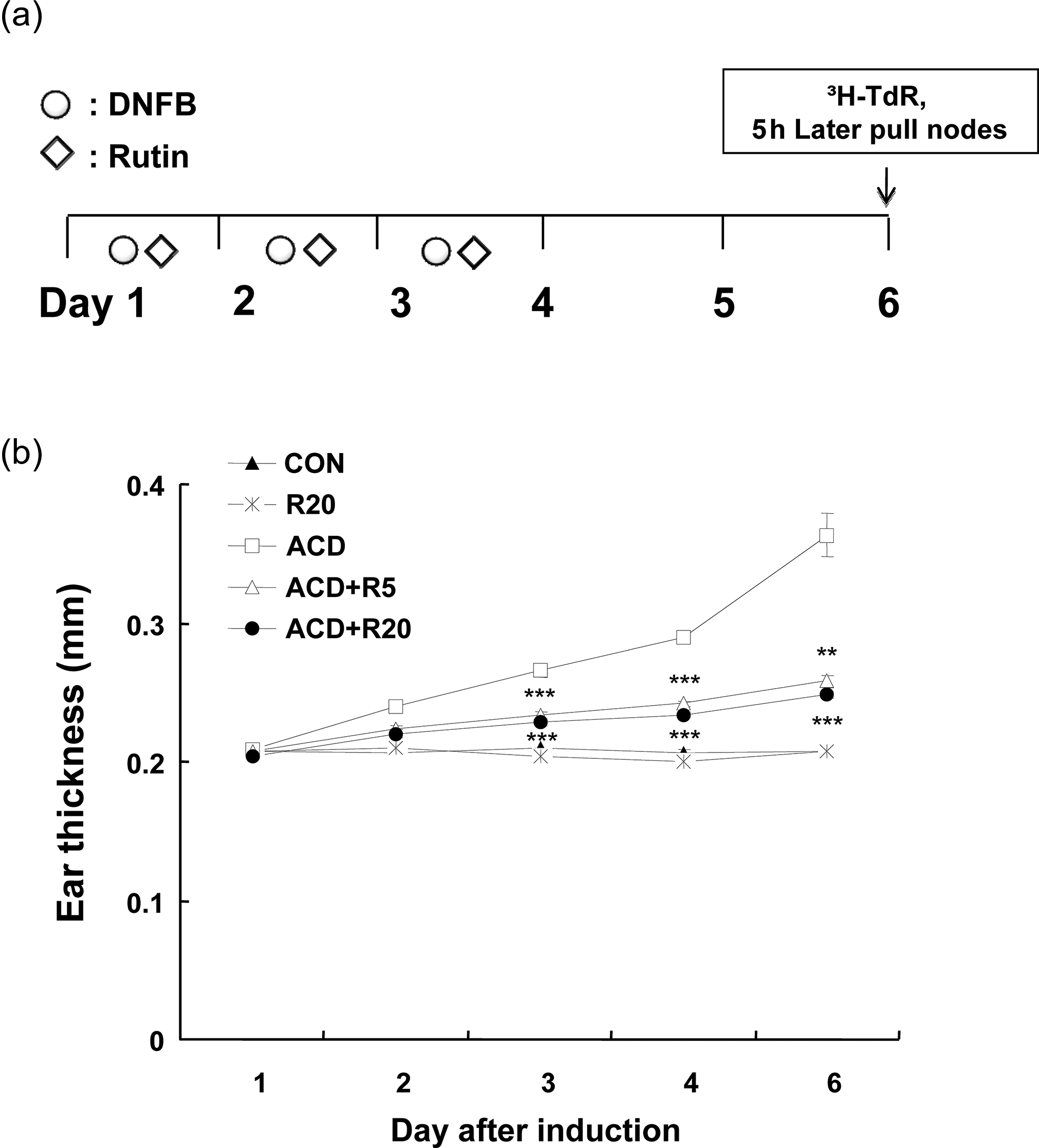
It was reported that topical exposure of 0.15% DNFB to mouse ears increases the cell number of auricular draining lymph nodes.
24
In our results, treatment of 0.15% DNFB induced proliferation of draining lymph node cells. Dermal application of rutin significantly diminished DNFB-induced lymphocyte proliferation (Figure 6a). Production of INF-γ, IL-2, TNF-α and IL-12 resulting from the activation of Th1 cells and secretion of IgG2a by B cells isotype switching are the typical character of ACD.
25
The total serum IgG2a level was significantly increased by repeated challenge, and this increased IgG2a level was also reduced by rutin (Figure 6b).
Effect of rutin in ACD mice. (a) Mice were injected intravenously with 20 μCi 3H-thymidine in 250 μL PBS, on day 6. After five hours, the lymph nodes were excised. Lymph node cells were lysed and incubated overnight in 5% trichloroacetic acid, and cpm were measured by liquid scintillation spectrophotometry. (b) The IgG2a level was measured at six days. Data are presented as mean ± SD of five determinations. (c) Effect of rutin on the expression of cytokines in ACD mice. The ears were excised and total RNA was isolated. Quantitative realtime PCR was performed as described in Materials and methods. Data are presented as mean ± SD of five determinations. *P < 0.05 significantly lower than ACD. ACD, allergic contact dermatitis; PBS, phosphate-buffered saline; IL, interleukin; INF-γ, interferon; TNF-α, tumor necrosis factor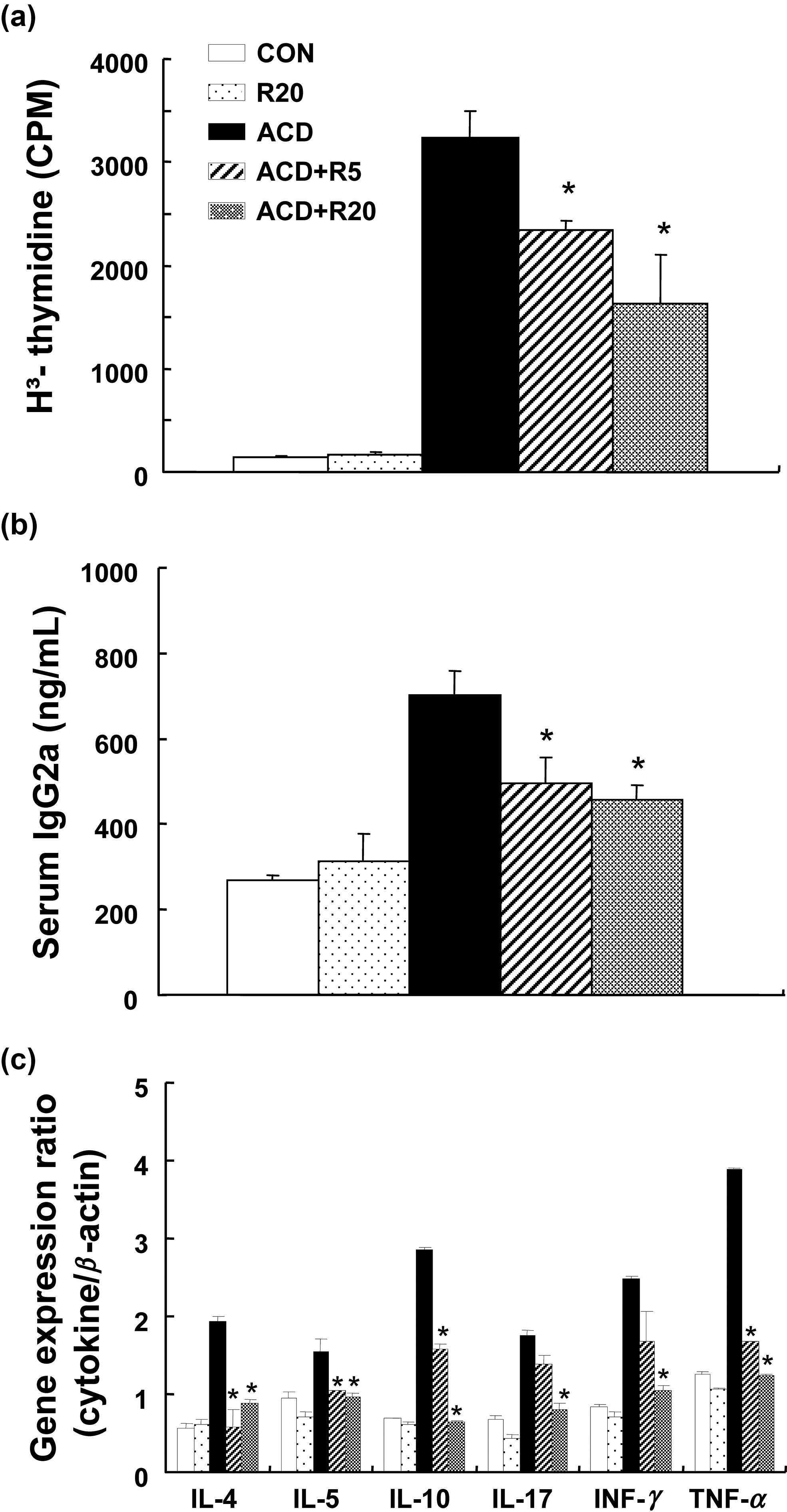
Next, we confirmed the effects of rutin on the inflammatory cytokines related to ACD. The expression levels of mRNA for IL-4, IL-5, IL-10, IL-17, INF-γ and TNF-α in the ears of mice were determined by quantitative realtime PCR. After induction of ACD, a significant elevation in the expression of IL-4, IL-5, IL-10, IL-17, INF-γ and TNF-α in ear tissue was observed (Figure 6c). Compared with the ACD group, rutin-treated groups showed significant decreases in all types of cytokines. These data indicate that rutin can reduce the expression of inflammatory cytokines in ACD.
Discussion
In the present report, we demonstrate that rutin inhibits DFE/DNCB-induced AD and DNFB-induced ACD. Skin lesions have been described very often in allergic skin inflammation-sensitized mice. Most previous reports on the development of allergic dermatitis skin lesions in mice revealed that skin inflammation is characterized by increased numbers of mast cells and eosinophils, and dermal and epidermal infiltrates. 26,27 In our results, rutin mitigated typical and histological changes, such as severe ear thickness, inflammatory cell infiltration, ulcers, dermal and epidermal thickness and epidermal hyperplasia. Rutin also significantly reduced the number of eosinophils, mast cells and serum histamine release. Mast cells are a derived source of Th2 cytokines, as well as inflammatory mediators. In addition, mast cells secrete multiple mediators affecting eosinophils, including IL-4, IL-5, IL-13 and eotaxins. 7,8 These results suggest that the inhibition of mast cell activation is another mechanism through which rutin improves inflammatory responses in the allergic dermatitis.
Th2 cell activation evokes expression of IL-4, IL-5 and IL-13 which regulating IgE class-switch. 3 We showed that rutin decreased IL-4, IL-5 and IL-13, which play important roles on isotype switching into IgE. Therefore, our results suggest that rutin can reduce serum IgE and antigen-specific IgE by suppressing the Th2 response. IL-31, which is produced by Th2 cells, has been reported to induce severe itching and dermatitis in transgenic mice and was recently proposed to promote pruritius in patients with AD. 26,28 IL-32 is a proinflammatory cytokine that was initially detected in IL-2-activated T-cells and natural killer cells. 29 Our result showed that rutin inhibited not only the expression of IL-4, IL-5 and IL-13 but also the expression of IL-31 and IL-32. These data suggest that IL-31 and IL-32 is also a target of rutin in AD.
Acute lesions display a Th2 phenotype with elevated levels of IL-4, IL-5 and IL-13; the chronic phase is dominated by the Th1 cytokine, INF-γ. 3 As described in our histological result (Figure 2a), DFE/DNCB-induced AD model showed infiltration of chronic inflammatory cells. Interestingly, the elevated expression of INF-γ was significantly reduced by rutin. Our results suggest that rutin suppresses both Th1 and Th2 immune responses. Thus, such bidirectional effects of rutin may be more beneficial from the view point of the treatment of AD. 30,31
We also confirmed the beneficial effect of rutin in ACD model. We focused on the immune response of a contact allergen and used a LLNA for its detection. LLNA is based on an increase of cellular proliferation, indicating the induction of an immune response. This assay measures the proliferation response of draining lymph node cells induced by repeated topical application of the test allergens. 23 These observations show that repeated application of DNFB induced ACD, which was characterized by significant skin swelling throughout the experimental period. In our result, rutin significantly inhibited the ear thickness and proliferation of lymph node cells. These data suggest that rutin inhibits outward contact sensitizer-induced proliferation of lymph node cells. Rutin might be useful in the treatment of lymph node cell-mediated allergic responses.
ACD is a dendritic cell-dependent and T-cell-mediated immune response elicited by epicutaneous sensitization with haptens. 32 Haptens can directly stimulate keratinocytes present in the epidermis of the skin to release inflammatory mediators. 23 Generally, contact allergens have been associated with increases in the Th1 cytokines, INF-γ and TNF-α. 23 TNF-α is an essential mediator of ACD. TNF-α expression is increased after challenge with haptens and administration of anti-TNF-α antibody abrogates ACD in mice. 33 Recently, in an ACD model, allergen sensitization induced the development of CD8+ T-cells that produce IFN-γ and IL-17 which are both required for eliciting an immune response. 3,34 We demonstrated that application of rutin prevented the development of ACD in mice by the reduction of Th1 cytokines (TNF-α and IFN-γ) and Th17 (IL-17). The increased IgG2a response in ACD mice might be due to an absence of the regulatory effect of IFN-γ on IgG2a-producing B-cells. In our ACD model, Th2 cytokines (IL-4, IL-5 and IL-10) were also elevated. DNFB, a strong contact sensitizer, is known to induce mixed Th1/Th2 responses. 35 We found that rutin inhibited all the Th1 (IFN-γ), Th2 (IL-4, IL-5 and IL-10) cytokines, and Th17 (IL-17) cytokines with the reduction of IgG2a in ACD model. Therefore, our results suggest that rutin suppresses Th1, Th2 and Th17 response.
Rutin is an important antioxidant with pharmacological benefits, including anticancer, anti-inflammatory and myocardial/renal protective effects. 13,14 Recently, a clinical application of rutin was reported. In the combination therapy of various drugs with rutin, as a food supplement, for 40 d in glaucoma patients, rutin further decreases the intraocular pressure by 20% of the initial value. 36 Author concluded that rutin can act in synergy with pharmacological treatments, and contribute to the control of intraocular pressure. Due to the low elimination rate and maintenance of high plasma concentration with a regular supply of ruin in the diet, 37 application of rutin as a pharmacological drugs or food supplement will be promising. In conclusion, according to the results of our AD and ACD models, we identified rutin as a possible therapeutic agent for AD and ACD. Although too early to draw any definitive conclusions, our data imply that rutin may be therapeutically useful in allergic response, at least in certain settings such as Th1/Th2 imbalance diseases as a pharmacological agent or food supplement.
Footnotes
ACKNOWLEDGEMENTS
This study was supported by a grant of the Korea Healthcare technology R&D Project, Ministry for Health, Welfare & Family Affairs, Republic of Korea (A111375).