
Abstract
To investigate the effects of direct peritoneal resuscitation with pyruvate-peritoneal dialysis solution (Pyr-PDS) of different concentrations combined with intravenous resuscitation on acid–base imbalance and intestinal ischemia reperfusion injury in rats with hemorrhagic shock. Sixty rats were randomly assigned to group SHAM, group intravenous resuscitation, and four direct peritoneal resuscitation groups combined with intravenous resuscitation: group NS, LA, PY1, and PY2, that is, normal saline, lactate-PDS (Lac-PDS), lower concentration Pyr-PDS (Pyr-PDS1), and higher concentration Pyr-PDS (Pyr-PDS2), respectively. Two hours after hemorrhagic shock and resuscitation, the pH, oxygen partial pressure, carbon dioxide partial pressure (PCO2), base excess, and bicarbonate ion concentration (HCO3−) of the arterial blood were measured. The intestinal mucosal damage index and intercellular adhesion molecule 1 (ICAM-1), tumor necrosis factor-α, interleukin-6, zonula occludens-1, claudin-1, and occludin levels in intestinal issues were detected. Two hours after resuscitation, group PY2 had higher mean arterial pressure, pH, oxygen partial pressure, and base excess and lower PCO2 of arterial blood than group PY1 (P < 0.05). Tumor necrosis factor-α and interleukin-6 levels in group PY2 were significantly lower than those in group PY1 (P < 0.05). Zonula occludens-1, claudin-1, and occludin expression levels were significantly higher in group PY2 than in group PY1 (P < 0.05). Direct peritoneal resuscitation with Pyr-PDS2 combined with intravenous resuscitation enhanced the hemodynamics, improved the acid–base balance, and alleviated intestinal ischemia reperfusion injury from hemorrhagic shock and resuscitation in rats. The mechanisms might include correction of acidosis, inhibition of inflammatory response, enhancement of systemic immune status, regulation of intestinal epithelial permeability, and maintenance of intestinal mucosal barrier function.
Impact statement
Hemorrhagic shock is a life-threatening condition after trauma or during surgery. Acid–base imbalance and intestinal ischemia reperfusion injury are two significant causes in the pathogenetic process and multiple organ dysfunction. As a result, it is urgent and necessary to find an effective method of resuscitation in order to reverse the acid–base imbalance and protect organ function. This current study confirmed the protection against hypoxic acidosis and intestinal ischemia reperfusion injury by peritoneal resuscitation with pyruvate combined with intravenous resuscitation in rats with hemorrhagic shock. And the peritoneal dialysis solution with pyruvate of high concentration plays a crucial role in the process. It provided a new idea and possible direction of fluid resuscitation for alleviating organ injuries, protecting organ functions, and improving clinical prognosis after hemorrhagic shock and resuscitation.
Keywords
Introduction
Hemorrhagic shock (HS) is a common complication in patients with severe trauma. It is a life-threatening condition and a leading cause of potentially preventable death among patients with trauma. 1 Early recognition of HS and appropriate intervention can save many lives and increase the survival rate of patients. Therefore, effective resuscitation strategies have become the key in the efforts to reduce mortality and to improve outcomes based on timely surgical hemostasis. 2
Although conventional intravenous resuscitation (VR) has advantages in improving hemodynamics, microcirculation disturbance is maintained in splanchnic organs, which could be alleviated by direct peritoneal resuscitation (DPR).3–6 Dilation of arterioles, especially in the intestine, is sustained by DPR, which reduces visceral organ ischemia and cellular hypoxia. 7 As an effective antioxidant and free radical scavenger, pyruvate protects the function of multiple splanchnic organs from HS in animals.8–11 Superior to lactate-based peritoneal dialysis solution (Lac-PDS), DPR with pyruvate-based peritoneal dialysis solution (Pyr-PDS) improves visceral vasoconstriction and hypoperfusion. 12 Sodium pyruvate in different concentrations has different outcomes on intestinal ischemia reperfusion injury (IRI) in HS rats. 13 However, it remains unknown whether Pyr-PDS with different concentrations of pyruvate has different effects on acid–base disturbance and organ injury from HS.
It has long been recognized that major trauma and shock can lead to acute systemic inflammatory response syndrome (SIRS) and multiple organ dysfunction syndrome (MODS). Gut ischemia appears to be the dominant link by which splanchnic hypoperfusion is transduced from a hemodynamic event into an immune-inflammatory event, and this is achieved via the release of biologically active factors into the mesenteric lymphatics. 14 For the distant organ injury caused by gut barrier failure, intestinal epithelium injury, and increased permeability during ischemia and reperfusion, the gut plays a significant role in the pathogenesis of acute SIRS and MODS after HS.
Therefore, a hypothesis was presented that DPR with Pyr-PDS of different concentrations combined with VR could improve acid–base disturbance, maintain homeostasis, and alleviate intestinal IRI from HS and resuscitation in rats in different degrees. In this study, the major outcomes blood pressure, blood gas analysis and pathological changes in intestinal mucosa were evaluated, and the possible mechanisms were investigated, including inflammation inhibition, immunological enhancement, and maintenance of intestinal barrier function.
Materials and methods
Materials
Sodium pyruvate, sodium lactate, glucose, and sodium pentobarbital were purchased from Sigma (St Louis, MO). Streptavidin/peroxidase (SP-9003) kit was purchased from Zymed Laboratories (San Diego, CA). Micro BCA protein assay kit, SDS-PAGE gel preparation kit, and chemiluminescence assay kit were purchased from Aspen (Johannesburg, South Africa).
Preparation of solutions
The following solutions were prepared: (1) 2.5% Glu-Lac-PDS (Lac-PDS) containing 40 mmol/L lactate, 132 mmol/L Na+, 1.75 mmol/L Ca2+, 0.25 mmol/L Mg2+, 96 mmol/L Cl−, and 2.5 g/dL glucose; (2) 2.5% Glu-Pyr-PDS (Pyr-PDS1) containing 40 mmol/L pyruvate, 132 mmol/L Na+, 1.75 mmol/L Ca2+, 0.25 mmol/L Mg2+, 96 mmol/L Cl−, and 2.5 g/dL glucose; and (3) 2.5% Glu-Pyr-PDS (Pyr-PDS2) containing 80 mmol/L pyruvate, 172 mmol/L Na+, 1.75 mmol/L Ca2+, 0.25 mmol/L Mg2+, 96 mmol/L Cl−, and 2.5 g/dL glucose. The pH was adjusted to 5.2 with HCl or NaOH. All the three PDSs were prepared fresh in the laboratory and kept in the refrigerator at 4°C, and they were warmed up to room temperature before use. High-performance liquid chromatography analysis was used to verify the stability of Pyr-PDS. 12
Animals
Sixty male Sprague-Dawley rats, weighing 200‒50 g and seven to nine weeks of age, were purchased from The Center for Animal Experiment of Wuhan University (Wuhan, China). According to the Guide for the Care and Use of Laboratory Animals (National Institutes of Health), all the animal experimental procedures were performed and approved by the Animal Experiment Committee of Wuhan University. Before the formal experiments, all the animals were acclimatized to 12-h light-dark cycles for one week with free access to food and water, and then fasted overnight and kept water-deprived from 4 h before experimentation.
Hemorrhagic shock and resuscitation protocol
The HS model of rats was induced as previously described with slight modification. 15 After allowing to breath spontaneously, the rats were anesthetized by an intraperitoneal injection with 1% sodium pentobarbital (45 mg/kg). The rats were then fixed in supine position, and the right common carotid artery was catheterized with an indwelling catheter (24 G), which was connected to a Surgivet Advisor Vital Signs (Smiths Medical, Norwell, MA) for continuous arterial blood pressure monitoring. The left femoral artery was catheterized for withdrawing blood to induce HS, and the right femoral vein was catheterized for heparinization (heparin sodium, 300 IU/kg) and fluid infusion. The surgical operation was performed in aseptic and constant temperature condition, and all the catheters and syringes were prefilled with heparin saline (100 IU/mL). To allow the rats to stabilize, no operation was performed for 15 to 30 min after surgery.
When the blood pressure stabilized, blood was withdrawn through the sterile syringe connected to the left femoral artery within 10 min to induce HS. By continuous withdrawal or reinfusion of blood as required, mean arterial pressure (MAP) was maintained at 35 ± 5 mmHg for 60 min before resuscitation. The maximum volume of blood loss was recorded. All the rats were divided into six groups (n = 10) randomly. In group SHAM, only surgical operation was performed without HS or resuscitation. After maintaining HS for 1 h, normal saline (NS) equal to twice the volume of blood loss was injected into the rats following reinfusion of the withdrawn blood in group VR; this entire procedure lasted for 30 min. At the end of the HS period, simultaneously with VR, DPR was performed in rats of the other four DPR groups. In group NS, LA, PY1, and PY2, rats were intraperitoneally infused with 20 mL of NS, Lac-PDS, Pyr-PDS1, and Pyr-PDS2, respectively, with a micro-infusion pump in the meanwhile of VR. MAP was recorded before blood withdrawal (T0); at 5, 30, and 60 min after HS (T1-3); and at 5, 30, 60, 90, and 120 min after resuscitation (T4-8) to observe the hemodynamic changes in rats.
Arterial blood sampling from animals
When resuscitation was completed, 1 mL arterial blood was taken from the left femoral artery for blood gas analysis with an ABL80 blood gas analyzer (Radiometer Medical ApS, Denmark). The pH, oxygen partial pressure (PO2), partial pressure of carbon dioxide (PCO2), base excess (BE), and bicarbonate ion concentration (HCO3−) of the arterial blood were measured to assess hypoxia and acid–base disturbance.
Intestinal tissue sampling from animals
The rats were killed humanely by exsanguination 2 h after fluid resuscitation. Sections of intestinal tissue were removed 10 cm from the ileocecal valve and rinsed with ice-cold saline. A 5-cm portion of the intestine was stored immediately in a −70°C ultra-low temperature freezer for further analyses. Another 5-cm portion of the intestinal tissue was fixed with 4% paraformaldehyde for further studies.
Evaluation of the intestinal mucosal damage index
The intestinal tissue samples fixed in 4% paraformaldehyde were made into paraffin sections. The sections were stained with hematoxylin-eosin to observe the pathological changes of the small intestinal mucosa with a light microscope. According to Chiu’s method, 16 IMDI was evaluated by three pathologists who were blinded to the groups in this study. The standards of evaluation were as follows: 0 point, normal mucosal villi; one point, development of the subepithelial space at the apex of intestinal villi, usually with capillary congestion; two points, extension of the subepithelial space, often with the epithelial layer mildly separating from lamina propria; three points, massive epithelial lifting down the sides of villi with a few tips desquamated; four points, completely denuded villi from lamina propria and exposed capillaries; and five points, digestion of lamina propria, ulceration, and hemorrhage.
Detection of intestinal intercellular adhesion molecule 1 and tumor necrosis factor-α levels
Intestinal tissue samples fixed in 4% paraformaldehyde were made into paraffin sections. ICAM-1 and TNF-α expression levels were detected using immunohistochemistry with streptavidin/peroxidase (SP-9003) kits (Zymed Laboratories) to evaluate intercellular adhesion and immune response. Image Pro Plus software was used to analyze the photographs of intestinal tissue sections and measure the average optical density in order to assess the levels of ICAM-1 and TNF-α in intestinal issue.
Detection of the expression level of interleukin-6, zonula occludens-1, claudin-1, and occludin in intestinal issue
To evaluate the intestinal mucosal barrier function and inflammatory reaction in intestinal tissue, Western blots were performed to detect IL-6, ZO-1, claudin-1, and occludin levels in intestinal issue. The proteins of the samples stored in −70°C ultra-low temperature freezer were detected as follows: extraction by cell lysis and centrifugation, concentration quantification with the BCA protein assay method, electrophoresis on an SDS-PAGE gel, transfer to a PVDF membrane, incubation with antibodies, and chemiluminescence detection. The primary antibodies were rabbit-sourced and purchased from Bioss Co. (Beijing, China), Affinity Biosciences (Cincinnati, OH, USA), and Abcam (Cambridge, UK). The dilution rate of the primary antibodies for GAPDH, IL-6, ZO-1, claudin-1, and occludin was 1:10,000, 1:500, 1:500, 1:1000, and 1:2000, respectively. The secondary antibodies were HRP-goat anti-rabbit antibodies purchased from Aspen. The dilution rate of the secondary antibodies was 1:10,000. Finally, the optical density value of the target strip was processed and analyzed with the AlphaEase software (Alpha Innotech Co., Fremont, CA).
Statistical analysis
All continuous variables were presented as mean ± standard deviation (SD). Analysis of statistical differences between the groups was performed with one-way analysis of variance (ANOVA), and multiple comparisons were analyzed with Student–Newman–Keuls test. All the data processing and analysis were completed using SPSS, version 25 software (IBM Corp., NY). P < 0.05 was considered to be statistically significant.
Results
Baseline characteristics
The age and body weight of rats in all the groups and the maximum volume of blood loss in the HS and resuscitation groups are shown in Table 1. There was no significant difference in these baseline characteristics between the groups (P > 0.05).
The age, weight, and maximum blood loss of rats in six groups (n = 10).

Note: Values are presented as the mean ± SD of 10 animals.
Map
The MAP at different time points (T0-T8) is shown in Table 2. Compared with T0, MAP at T1, T2, and T3 was significantly lower in the HS and resuscitation groups (P < 0.05), which confirmed that the HS model of rat was successfully established. At T4 and T5, there was no significant difference in MAP between groups LA, PY1, and PY2 (P > 0.05). At T6, T7, and T8, group PY2 had significantly higher MAP than groups LA and PY1 (P < 0.05).
The effect of Pyr-PDS on MAP of rats at different time points (T0-T8) (n = 10).
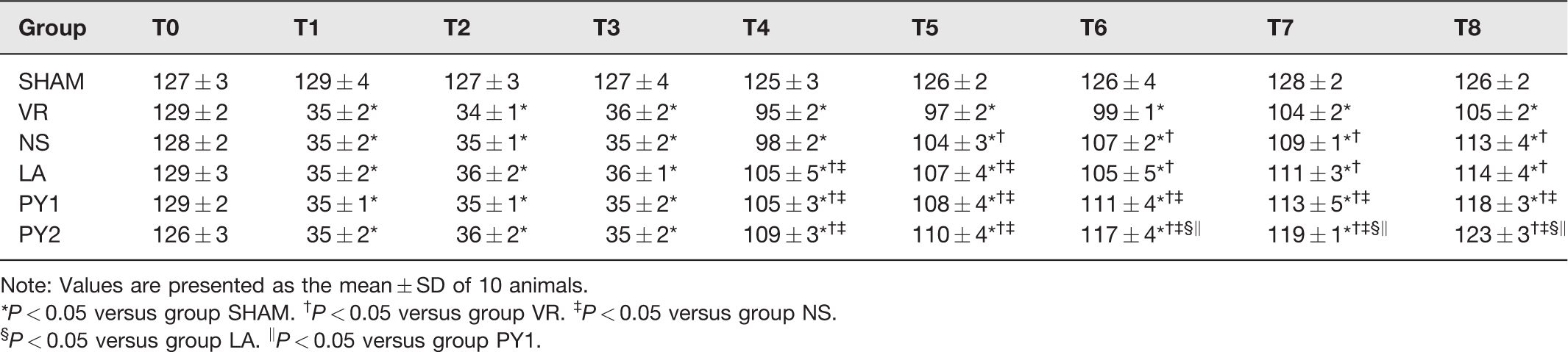
Note: Values are presented as the mean ± SD of 10 animals.
*P < 0.05 versus group SHAM. †P < 0.05 versus group VR. ‡P < 0.05 versus group NS.
§P < 0.05 versus group LA. ‖P < 0.05 versus group PY1.
pH, PO2, PCO2, BE, and HCO3− levels of the arterial blood
The pH, PO2, PCO2, BE, and HCO3− levels of the arterial blood at 2 h after resuscitation are shown in Table 3. In groups PY1 and PY2, the pH, PO2, and HCO3− levels were significantly higher than those in group LA (P < 0.05). In group PY2, the pH, PO2, and BE levels were significantly higher than those in group PY1 (P < 0.05). Group PY2 had higher HCO3− than group PY1, but the difference was not significant (P > 0.05). Compared with group LA, PCO2 was significantly lower in groups PY1 and PY2 (P < 0.05), and PCO2 in group PY2 was significantly lower than that in group PY1 (P < 0.05).
The effect of Pyr-PDS on arterial blood gas at 2 h after resuscitation in rats (n = 10).
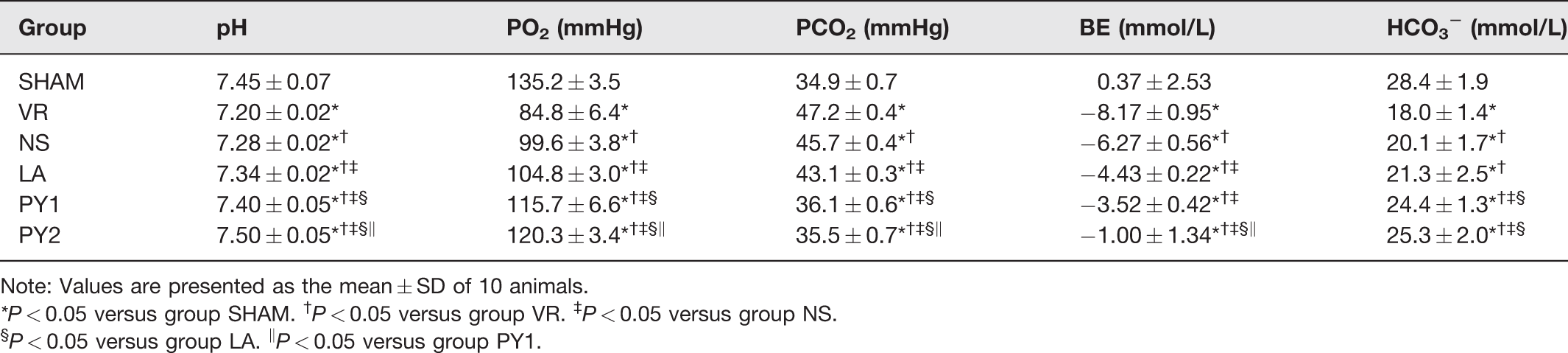
Note: Values are presented as the mean ± SD of 10 animals.
*P < 0.05 versus group SHAM. †P < 0.05 versus group VR. ‡P < 0.05 versus group NS.
§P < 0.05 versus group LA. ‖P < 0.05 versus group PY1.
Pathological changes in intestinal mucosa
By using a light microscope, the pathological changes of intestinal mucosa were observed at 2 h after resuscitation (Figure 1). In groups SHAM, PY1, and PY2, the epithelial structure of the intestinal mucosa was approximately integrated without any obvious damage, and there was an infiltration of few neutrophils and lymphocytes in groups PY1 and PY2. In groups VR and NS, there was significant widening of the subepithelial space at the top of the villi, shedding of massive epithelium down the sides of the villi with a few tips desquamated, partial disintegration of lamina propria, and infiltration of a large number of lymphocytes and neutrophils. The pathological injuries of intestinal mucosa were alleviated in group LA as compared to those in groups VR and NS. The subepithelial space was widened to a certain extent in the villi tips, and the epithelial layer was mildly separated from lamina propria with denudation of few tips. The intestinal mucosa was infiltrated with many lymphocytes and neutrophils.
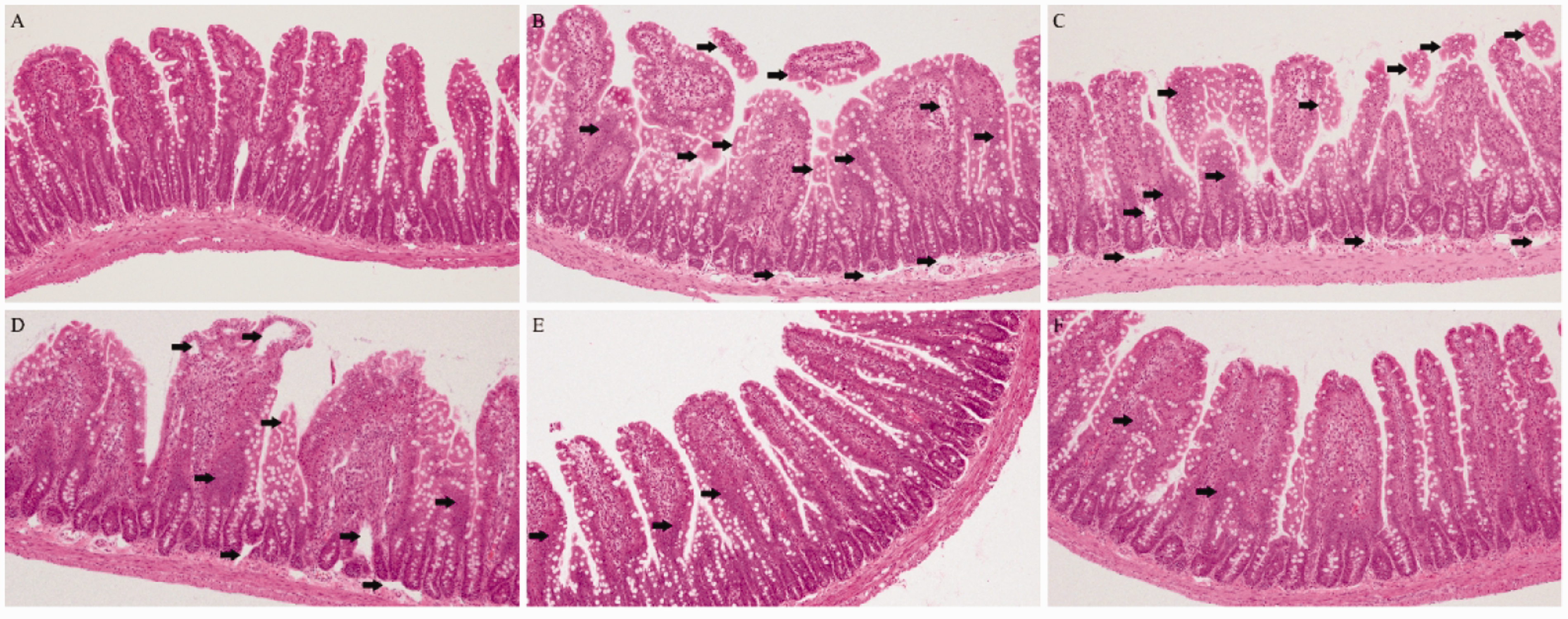
The effect of Pyr-PDS on morphological changes in the intestinal mucosa of rats (n = 10). Photomicrographs of hematoxylin-eosin-stained sections of the small intestine of rats at 2 h after resuscitation (original magnification, ×100 for the six panels). (a) Group SHAM. (b) Group VR. (c) Group NS. (d) Group LA. (e) Group PY1. (f) Group PY2. In (b) and (c), the arrows highlight the shedding of massive epithelium down the sides of villi with a few tips desquamated, partial disintegration of lamina propria, and infiltration of a large number of lymphocytes and neutrophils. In (d), the arrows highlight the widened subepithelial space in the villi tips, mild separation of the epidermis, and lamina propria with denudation of few tips, and infiltration of many lymphocytes and neutrophils. In (e) and (f), the arrows highlight the infiltration of few neutrophils and lymphocytes. (A color version of this figure is available in the online journal.)
IMDI
Table 4 presents the IMDI, which demonstrated pathological changes in the intestinal mucosa of the rats. Two hours after fluid resuscitation, no statistically significant difference in IMDI was observed between groups PY1, PY2, and SHAM (P > 0.05). Groups PY1 and PY2 showed significantly lower IMDI than group LA (P < 0.05). Moreover, group PY2 had lower IMDI than group PY2, but the difference was not significant (P > 0.05).
The effects of Pyr-PDS on IMDI, expression levels of ICAM-1, TNF-α, and IL-6 in intestinal tissue at 2 h after resuscitation in rats (n = 10).
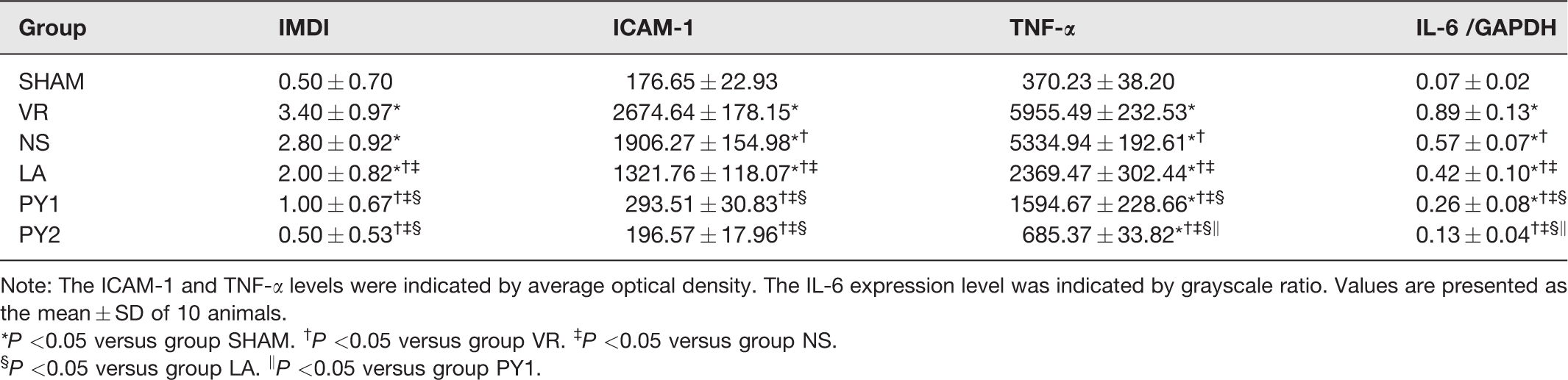
Note: The ICAM-1 and TNF-α levels were indicated by average optical density. The IL-6 expression level was indicated by grayscale ratio. Values are presented as the mean ± SD of 10 animals.
*P <0.05 versus group SHAM. †P <0.05 versus group VR. ‡P <0.05 versus group NS.
§P <0.05 versus group LA. ‖P <0.05 versus group PY1.
ICAM-1, TNF-α, and IL-6 levels in intestinal tissue
Immunohistochemical staining of ICAM-1 in the sections of the small intestinal mucosa at 2 h after resuscitation is shown in Figure 2. ICAM-1 levels were significantly decreased in groups LA, PY1, and PY2 as compared to those in groups VR and NS (P < 0.05) (Table 4), and groups PY1 and PY2 had significantly lower ICAM-1 levels than group LA (P < 0.05). The ICAM-1 level was lower in group PY2 than in group PY1, but the difference was not significant (P > 0.05).
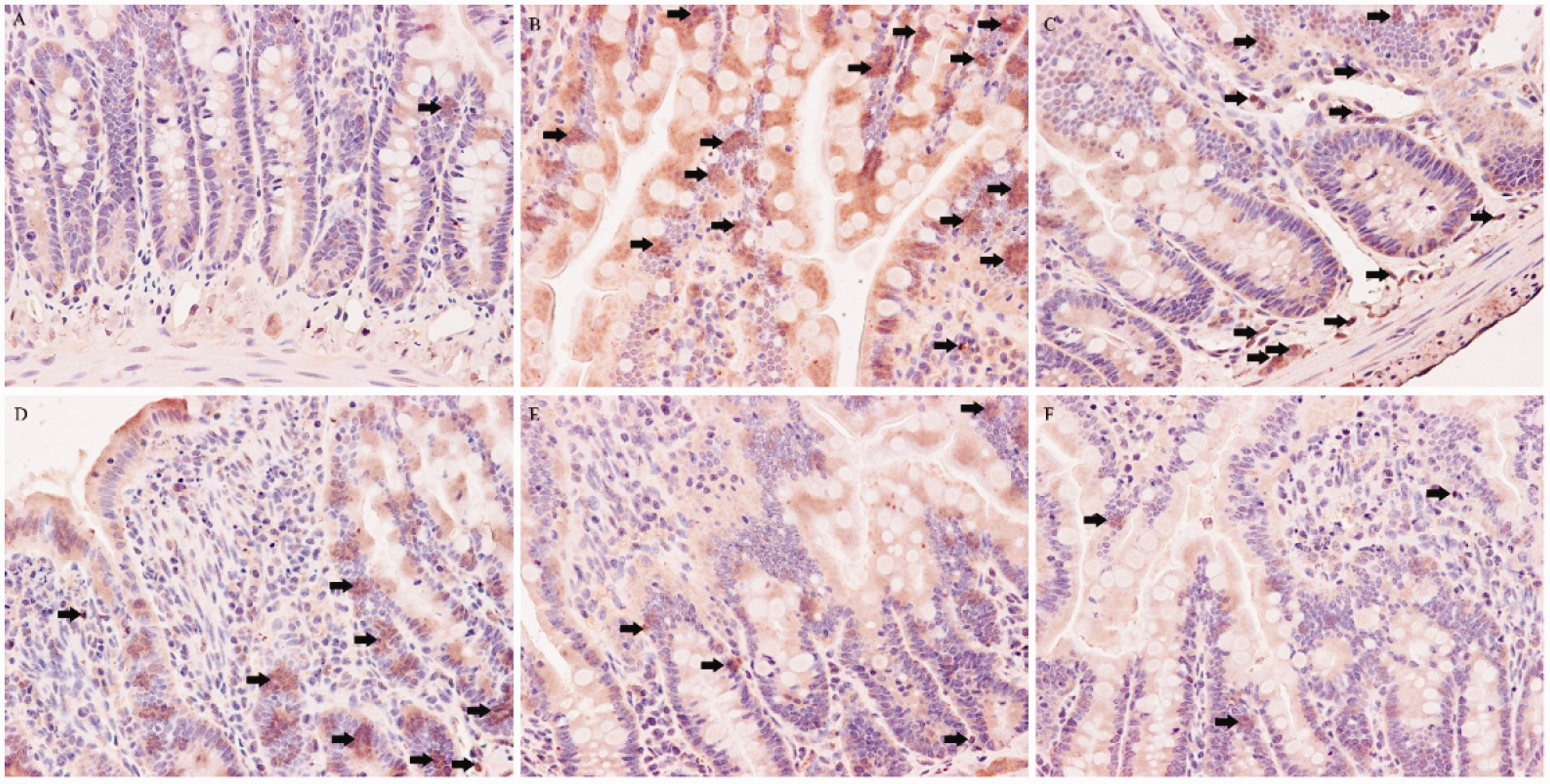
Immunohistochemical staining of ICAM-1 in the sections of the intestinal mucosa of rats at 2 h after resuscitation (n = 10) (original magnification, ×400 for the six panels). (a) Group SHAM. (b) Group VR. (c) Group NS. (d) Group LA. (e) Group PY1. (f) Group PY2. The arrows highlight the expression of intestinal ICAM-1. (A color version of this figure is available in the online journal.)
Immunohistochemical staining of TNF-α in the sections of the small intestinal mucosa of rats at 2 h after resuscitation is shown in Figure 3. Compared with groups VR and NS, TNF-α levels were significantly lower in groups LA, PY1, and PY2 (P < 0.05) (Table 4). Groups PY1 and PY2 showed significantly lower TNF-α levels than group LA (P < 0.05), and TNF-α level in group PY2 showed a significant decrease relative to that of group PY1 (P < 0.05).
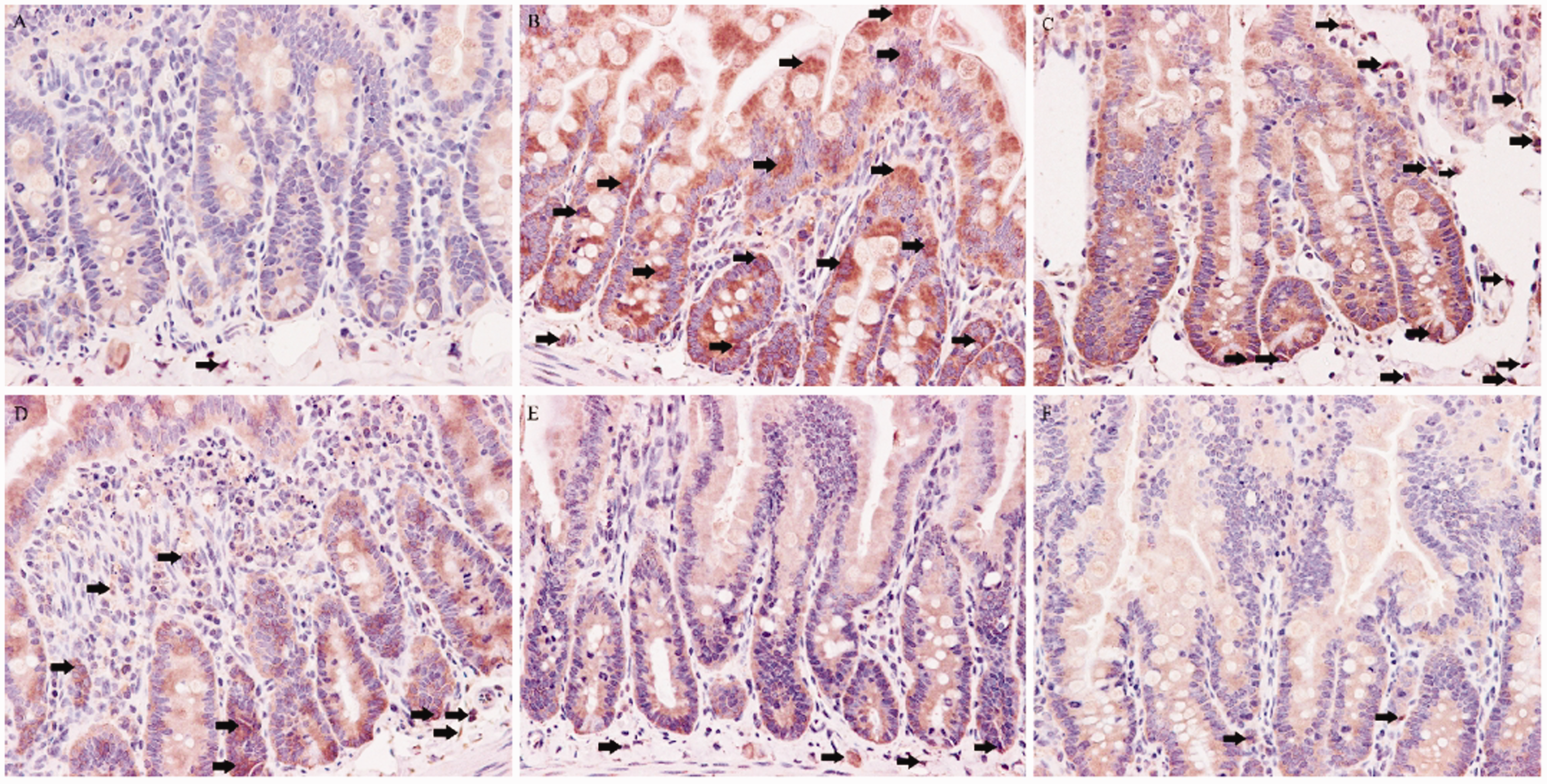
Immunohistochemical staining of TNF-α in the sections of the intestinal mucosa of rats at 2 h after resuscitation (n = 10) (original magnification, ×400 for the six panels). (a) Group SHAM. (b) Group VR. (c) Group NS. (d) Group LA. (e) Group PY1. (f) Group PY2. The arrows highlight the expression of intestinal TNF-α. (A color version of this figure is available in the online journal.)
The grayscale values of the expression levels of IL-6 determined by Western blot analysis at 2 h after HS and resuscitation in rats are presented in Figure 4. Groups LA, PY1, and PY2 had significantly lower IL-6 levels than groups VR and NS (P < 0.05) (Table 4). The IL-6 levels in groups PY1 and PY2 were significantly lower than that in group LA (P < 0.05), and group PY2 showed a significant decrease in IL-6 level as compared to that in group PY1 (P < 0.05).
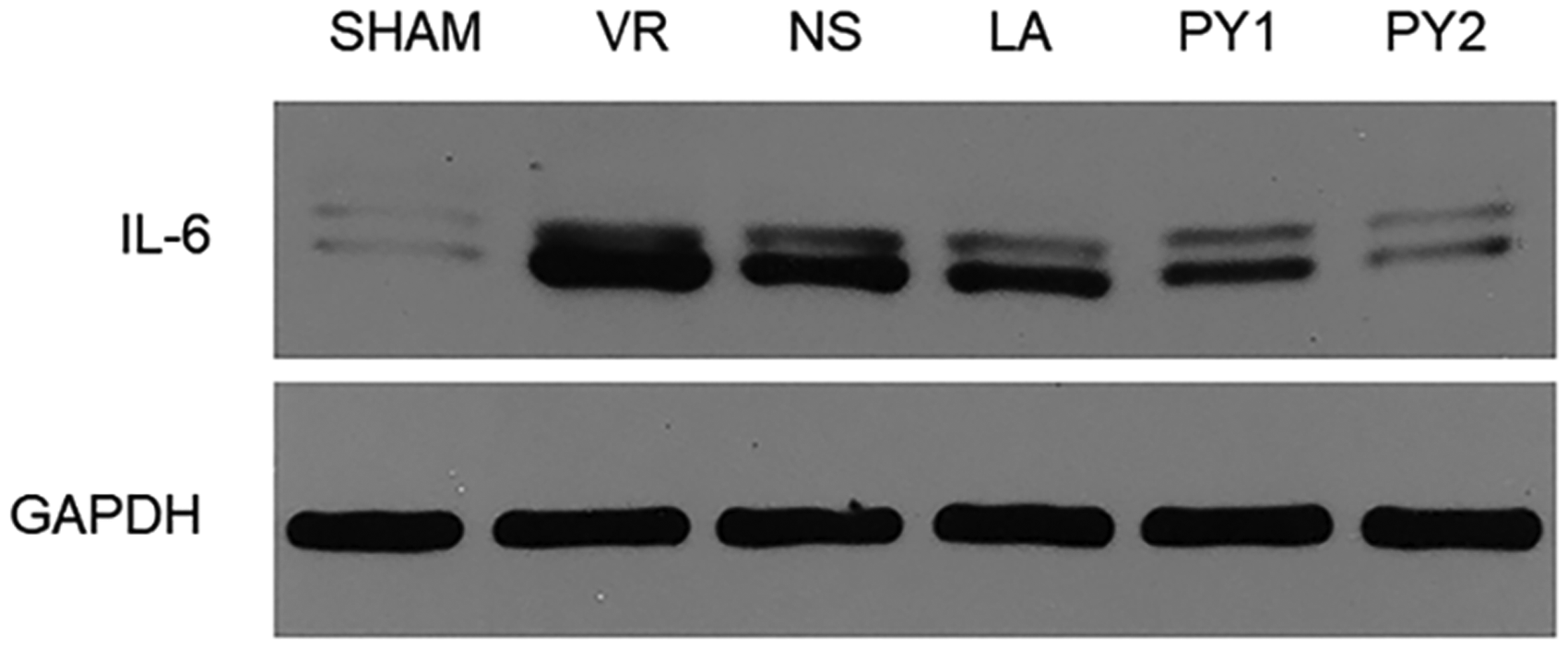
Effects of Pyr-PDS on the expression of IL-6 in the intestinal tissue as represented by grayscale value and determined by Western blot analysis at 2 h after HS and resuscitation in rats (n = 10).
ZO-1, claudin-1, and occludin levels in intestinal tissue
The grayscale images of the tight junction proteins ZO-1, claudin-1, and occludin at 2 h after resuscitation are shown in Figure 5. The expression levels of these proteins were significantly lower in the five HS and resuscitation groups than in group SHAM (P < 0.05) (Figure 6.). Compared to groups VR and NS, groups LA, PY1, and PY2 had significantly higher levels of ZO-1, claudin-1, and occludin (P < 0.05). In groups PY1 and PY2, the expression levels of ZO-1, claudin-1, and occludin were significantly higher than those in group LA (P < 0.05), and group PY2 showed a higher level of these proteins than group PY1 (P < 0.05).
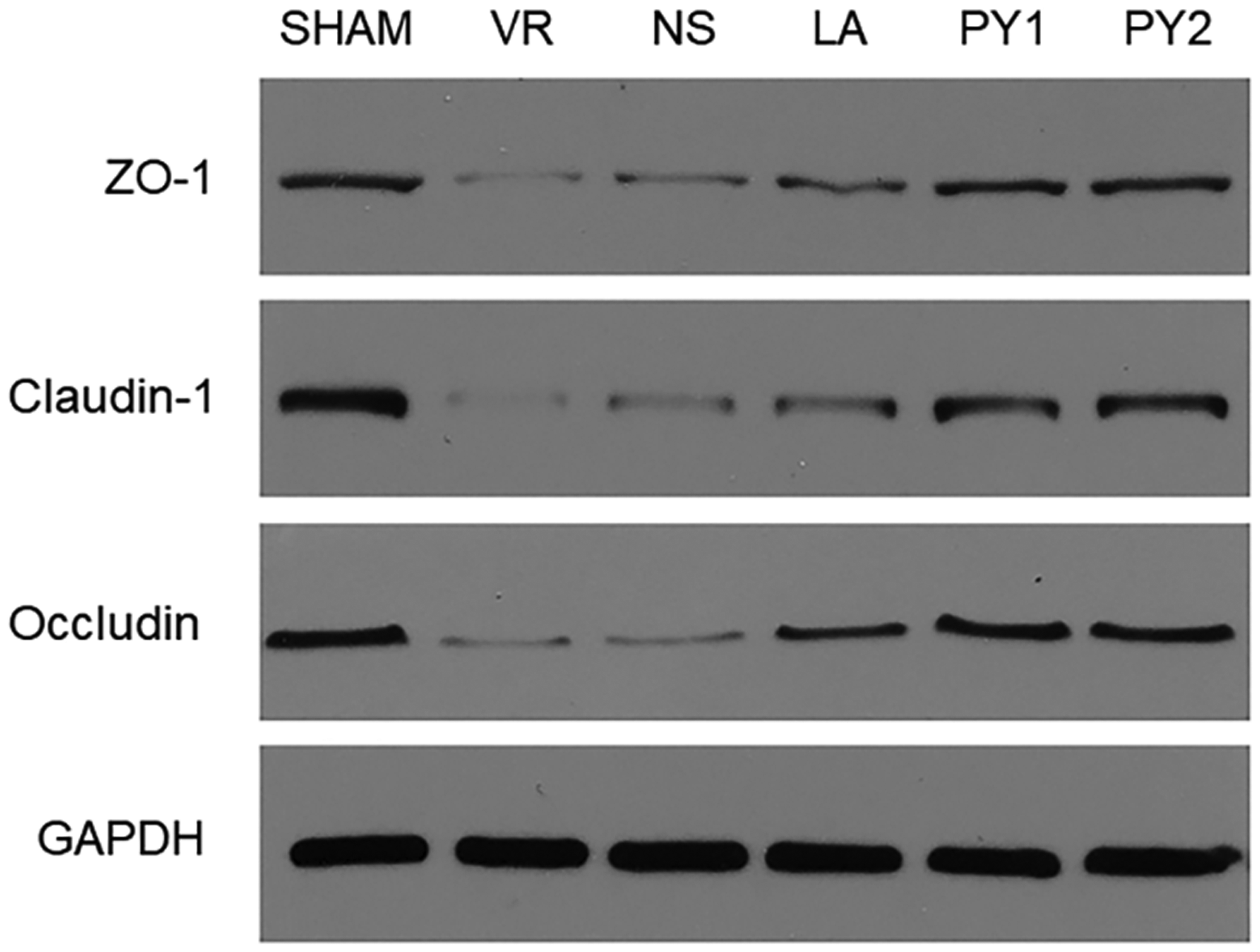
Effects of Pyr-PDS on the expression of tight junction proteins ZO-1, claudin-1, and occludin as represented by grayscale value and determined by Western blot analysis at 2 h after HS and resuscitation in rats (n = 10).
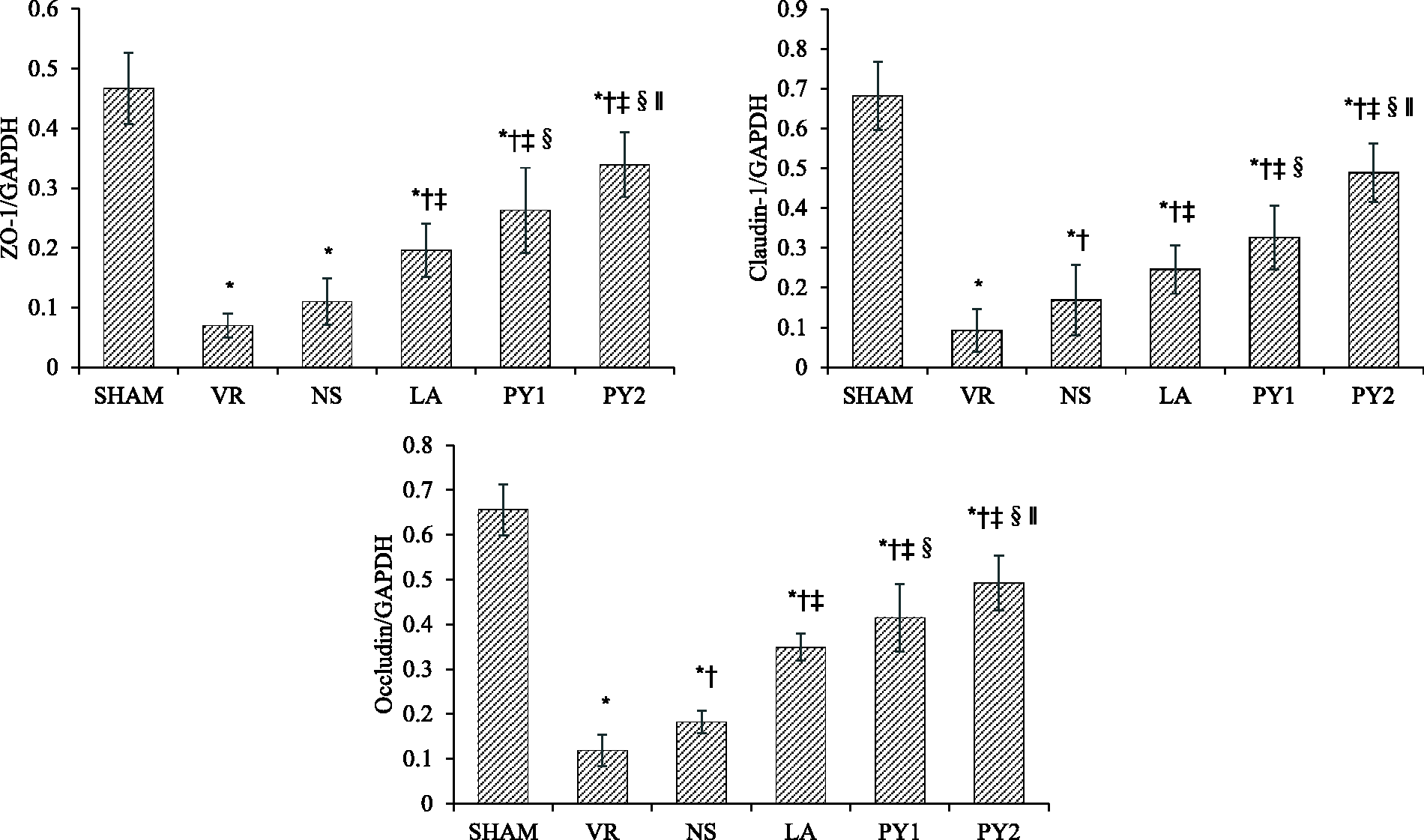
Effects of Pyr-PDS on the expression of tight junction proteins ZO-1, claudin-1, and occludin as represented by the grayscale ratio at 2 h after HS and resuscitation in rats (n = 10). Data are expressed as mean ± SD. *P < 0.05 versus group SHAM. †P < 0.05 versus group VR. ‡P < 0.05 versus group NS. §P < 0.05 versus group LA. ‖P < 0.05 versus group PY1.
Discussion
As an important substrate in the tricarboxylic acid cycle and a pivotal intermediate in glycolysis, pyruvate is an effective antioxidant and oxygen-free radical scavenger.8–10 Hypertonic sodium pyruvate provides a significant protection against oxidative stress and inflammatory response to alleviate liver injury. 17 DPR has significant therapeutic potential for improving intestinal permeability, inflammatory response, mesenteric perfusion, and intestinal IRI.18,19
Effects of Pyr-PDS with different concentrations on hemodynamics and acid–base balance in rats
MAP indicates the status of blood circulation and perfusion and reflects the hemodynamics during HS and resuscitation in vivo. In this study, there was no significant difference in MAP between groups LA, PY1, and PY2 within 1 h after resuscitation. However, from 1 h after resuscitation to the end, the MAP in group PY2 was significantly higher than that in groups LA and PY1. This finding demonstrated that Pyr-PDS with higher pyruvate concentration was superior in improving blood circulation and organ reperfusion from 1 h after resuscitation to the end.
The arterial blood gas analysis showed that Pyr-PDS had an advantage over Lac-PDS in correcting acid–base disturbance caused by HS and resuscitation. Furthermore, Pyr-PDS2 with higher pyruvate concentration was superior to Pyr-PDS1 in alleviating hypoxic acidosis and maintaining homeostasis. This finding also confirmed the effective alkalinization of Pyr-PDS2. However, the pH value in group PY2 was slightly high, which was possibly because of the alkalinization of pyruvate and the compensated hyperventilation of the rats. Pyr-PDS2 with high pyruvate concentration lowered arterial blood PCO2 significantly than Pyr-PDS1. Although there was no CO2 retention in group LA, this finding indicated that there might be compensatory hyperventilation following metabolic acidosis.
Effects of Pyr-PDS with different pyruvate concentrations on intestinal pathological injury
After HS, ischemia and hypoxia of the intestinal mucosa, swelling of the intestinal epithelium, and increase in intestinal mucosal permeability occurred in vivo. When fluid resuscitation is performed, the primary intestinal diseases are worsened to secondary processes, namely IRI. 20 In the present study, the pathological injuries in the intestinal mucosa were alleviated in groups PY1 and PY2 as compared to that in group LA. This result demonstrated that Pyr-PDS was superior to Lac-PDS in protection against intestinal IRI from HS and resuscitation in rats. The IMDI in group PY2 was lower than that in group PY1, but without statistical significance; this finding indicated Pyr-PDS with both higher and lower pyruvate concentrations improved intestinal injury effectively.
Effects of Pyr-PDS with different pyruvate concentrations on intestinal inflammation and immunity
Even though the blood pressure is restored after HS and resuscitation, the activation of inflammatory cells could be triggered by cytokines and mediums from ischemic or injured vascular endothelium. 21 Evidence suggests that neutrophils are accumulated and activated in the early stage of shock by the mediation of ICAM-1, leading to injuries of intestinal epithelial cells and increase in intestinal permeability.22,23 Inflammatory reaction could be induced by TNF-α through the expression of ICAM-1. 24 TNF-α is an early key mediator in the induction of SIRS and MODS, and it forms a network together with IL-6, a common inflammatory cytokine in the regulation of immune responses. This study showed that Pyr-PDS had a significant advantage over Lac-PDS in terms of reducing these three inflammatory mediators. This result demonstrated that DPR with Pyr-PDS was superior in inhibiting inflammation by alleviating the activation and interaction of endothelium and neutrophils. Although group PY2 had a nonsignificant lower ICAM-1 level than group PY1, the TNF-α and IL-6 levels were significantly lower in group PY2 than in group PY1. This result showed that Pyr-PDS2 with higher pyruvate concentration afforded a better protection on intestinal immune status after HS and resuscitation in rats than Pyr-PDS1.
Effects of Pyr-PDS with different pyruvate concentrations on intestinal barrier function
Intestinal bacterial translocation and endotoxin release are attributed to impaired intestinal barrier function after HS and resuscitation. 14 Signals that can reach the periphery could be produced by most components of the intestinal barrier. 25 As a semipermeable barrier, the intestinal mucosa composed of epithelial cells with intercellular junctions selectively allows inflow of nutrients and electrolytes while keeping potentially harmful substances out. To maintain the normal intestinal barrier function, various elements participate in the defensive system to keep epithelial barrier integrated. 26
The dysfunction of the intestinal barrier is closely associated with impairment of tight junctions mediated by special proteins such as ZO, claudin, and occludin. As members of the junctional adhesion molecule family, ZO proteins interact with the actin cytoskeleton to maintain the tight junction structure and regulate intestinal barrier integrity. 27 Proteins of the claudin family that comprises at least 20 members are considered to be significant barrier proteins.28,29 Occludin was discovered as the first integral membrane tight junction protein and plays a crucial role in tight junction function because of its close association with other junction proteins.30,31 Changes in the expression of these proteins are associated with the epithelial barrier dysfunction, leading to an increase in intestinal permeability. 32 In this study, the expression levels of ZO-1, claudin-1, and occludin in intestinal mucosa were higher in group PY than in group LA, and group PY2 had significantly higher levels of these three tight junction proteins than group PY1. This finding demonstrated that Pyr-PDS was superior to Lac-PDS in maintaining tight junction integrity in endothelial cells, and Pyr-PDS2 with higher pyruvate concentration afforded a better protection to intestinal epithelial tight junction than Pyr-PDS1 with lower pyruvate concentration. This finding indicated that Pyr-PDS with higher pyruvate concentration had an advantage in regulating the intestinal mucosal barrier function and alleviating intestinal injury from HS and resuscitation in rats.
According to this study, DPR combined with VR showed better protective effects on the vital signs, acid–base balance, and multiorgan failure of rats than conventional VR, probably for the reasons of homeostasis correction, inflammation inhibition, immune enhancement, and maintenance of intestinal barrier function.
Combined with VR, DPR is performed by infusion of PDS into the abdomen. Accompanying dilation of arterioles in the abdominal viscera alleviates the cellular hypoxia and organ ischemia, especially in the intestine. It has been demonstrated in animal studies that DPR combined with VR after HS can reduce organ edema and serum inflammatory mediators when compared with VR. 7 Furthermore, human studies have shown numerous benefits of DPR. After damage control surgery for HS or sepsis, DPR indicated faster closure of abdomen, increased rate of primary fascial closure, and lower rate of abdominal complications. 33 Additionally, DPR following abdominal catastrophes and sepsis have shown decreased ventilator days and length of stay in ICU. 34 Therefore, DPR combined with VR produced a promising result in treatment of patients with trauma or sepsis.
Clinical significance
The present study confirmed the protection provided by DPR with Pyr-PDS combined with VR against hypoxic acidosis and intestinal injury from HS, and showed the advantage of Pyr-PDS2 with higher pyruvate concentration over Lac-PDS and Pyr-PDS1. The superiority of Pyr-PDS might be relevant to the protection of the intestinal immunologic function and barrier function, which might have significant effects on other remote organs, including the liver and kidney. 12 All these discoveries provide a new idea and direction for fluid resuscitation for alleviating organ injuries, protecting organ functions, and improving clinical prognosis after HS and resuscitation. Nevertheless, further basic and clinical investigation is warranted, and more evidence needs to be collected.
Limitations
In the present study, only two concentrations of Pyr-PDS were experimentally investigated. The 40 mmol/L concentration was a regular concentration of pyruvate in PDS, similar to that in Lac-PDS used in clinics. The 80 mmol/L pyruvate concentration was used to evaluate the effect of PDS with higher pyruvate concentration in DPR. Protection against intestinal IRI by pyruvate infusion could be achieved at doses with negligible sodium overload. Systemic effects are apparent only at a dose of more than 250 mg sodium pyruvate/kg. 35 Furthermore, DPR with hypertonic fluids following VR alleviates visceral hypoperfusion and enhances organ function from HS in rats. 12 Therefore, we used only these two groups for basic comparison. However, because of the high concentration of sodium and hyperosmolarity of the fluid, there was a limitation on the resuscitation time to avoid water and electrolyte imbalance and accumulation of metabolites.
Conclusions
In the present study, both the hemodynamics stability and acid–base balance in rats were improved, and the intestinal IRI from HS and resuscitation was significantly alleviated by DPR with Pyr-PDS combined with VR. Pyr-PDS with higher pyruvate concentration provided a better protection to HS rats. The possible mechanisms of this effect might include correction of homeostasis, inhibition of inflammatory response, enhancement of systemic immune status, regulation of intestinal epithelial permeability, and maintenance of intestinal mucosal barrier function.
Footnotes
ACKNOWLEDGMENTS
The authors thank The Ohio State University, Wexner Medical Center for the language editing of the manuscript. The authors thank Jia-He Lin, MD, from Pinggu Hospital, Beijing Friendship Hospital, Capital Medical University at Beijing for her writing assistance in this article.
Authors’ contributions
All authors participated in the design, interpretation of the studies and analysis of the data and review of the manuscript. Jing-Jing Zhang was involved in study design and drafting, data analysis, and manuscript writing; Hui-Qin Shen conducted animal experiments, index detection, and data interpretation; Jiang-Tao Deng, Lin-Lin Jiang, Qiong-Yue Zhang, and Ying Xiong participated in sample collection and detection; Zong-Ze Zhang assisted in animal experiments; and Yan-Lin Wang assisted in study design and manuscript revision and made the final decision of submission for publication. All authors have approved the final article.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
This research is currently supported by the National Natural Science Foundation of China (NSFC) (#81601678).