
Abstract
Heart failure (HF) is often associated with compromised physical capacity in patients. However, it is unclear if established HF markers correlate with the physical performance of patients with congestive HF (CHF). We assessed the left ventricular end-systolic dimension (LVESD) and ejection fraction (LVEF) and, physical performance parameters, including short physical performance battery (SPPB), gait speed (GS), and handgrip strength (HGS) in 80 patients with CHF along with 59 healthy controls. Furthermore, levels of plasma HF markers galectin-3 and heart-specific fatty acid binding protein (H-FABP) were measured in relation to the severity of HF and physical performance. Irrespective of etiology, significantly greater LVESD and lower LVEF were observed in HF patients versus controls. As expected, the levels of HF markers galectin-3 and H-FABP were upregulated in the CHF patients which were accompanied by significantly elevated levels of plasma zonulin and inflammatory marker C-reactive protein (CRP). The SPPB scores, GS, and HGS were significantly lower in the ischemic and non-ischemic HF patients than controls. The level of galectin-3 was inversely correlated with SPPB scores (r2 = 0.089, P = 0.01) and HGS (r2 = 0.078, P = 0.01). Similarly, H-FABP levels were also inversely correlated with SPPB scores (r2 = 0.06, P = 0.03) and HGS (r2 = 0.109, P = 0.004) in the patients with CHF. Taken together, CHF adversely affects physical performance, and galectin-3 and H-FABP may serve as biomarkers of physical disability in patients with CHF. The robust correlations of galectin-3 and H-FABP with the physical performance parameters and CRP in CHF patients suggest that the poor physical performance may partly be caused due to systemic inflammation.
Impact Statement
Congestive heart failure (CHF) is often associated with poor physical performance of patients. Here we show, for the first time, an association of the HF markers with the parameters of physical performance in patients with CHF. The short physical performance battery (SPPB), gait speed, and handgrip strength (HGS) parameters were severely reduced in patients with CHF. A negative correlation of plasma galectin-3 and heart-specific fatty acid binding protein (H-FABP) levels with SPPB scores and HGS and positive correlations with C-reactive protein (CRP) levels in patients with CHF suggest that systemic inflammation may play a role in the poor physical performance of CHF patients.
Introduction
Congestive heart failure (CHF) is the leading cause of hospitalization in the older population globally and is associated with increased morbidity, mortality, and compromised quality of life. 1 CHF is primarily an age-related disease, and a progressive increase in its prevalence is reported due to the aging of the global population.1,2
The reduced cardiac pumping in CHF patients causes compromised blood supply to multiple body organs. Among them, skeletal muscle is specifically affected, resulting in muscle weakness and wasting. These findings compound the age-related muscle loss, termed sarcopenia, 3 which leads to reduced functional capacity and progressively dependent lifestyle.4,5 Stressors such as pressure overload and myocardial infarction (MI)–induced cardiac remodeling and contractile dysfunction consequently lead to muscle weakness and wasting, reduced aerobic capacity, and reduced capacity to perform activities of daily living.6,7 An interface between aerobic capacity and severity of CHF is recognized, so that the patients with advanced CHF have reduced aerobic capacity and vice versa. 8 CHF patients with reduced aerobic capacity also exhibit poor prognosis and reduced long-term survival. In addition, muscle wasting in CHF patients is also associated with reduced life expectancy. 9
These findings necessitate the proper characterization of physical capacity and muscle health in CHF patients. Several functional tests are available to evaluate physical performance in the older population. Among them, the SPPB may be of primary relevance. 10 SPPB is a composite test that assesses gait speed, balance, and chair sit-to-stand test. The relevance of these tests to the severity and prognosis of CHF has previously been recognized. 8 For example, reduced gait speed in CHF patients is associated with increased hospitalization and mortality. 11 Similarly, patients with reduced balance and low SPPB scores show worse prognosis than patients with good functional performance. 12 Thus, the SPPB evaluation of CHF patients may have prognostic and therapeutic relevance in clinical settings. However, it may not be possible to perform SPPB in patients with arthritis, neurological deficit, and/or poor compliance, warranting the necessity for a bedside assessment tool of functional capacity.
Plasma biomarkers, including inflammatory, growth factors, and cardiac injury markers, may be ideal candidates for assessment of functional capacity and muscle wasting in CHF. Several potential candidates have been described in the literature.13 –17 Galectin-3 is a member of the lectin family and is released by cardiac macrophages in the extracellular spaces. 18 Accumulating evidence indicates an association of plasma galectin-3 with a variety of clinical conditions including HF.19 –21 Specifically, galectin-3 is shown to regulate several processes in the cardiac tissues, including fibrosis, heightened inflammation, ventricular remodeling, and cellular proliferation. 18 In addition, an association between plasma galectin-3 and frailty has been described in CHF patients, indicating a potential relevance of galectin-3 to functional capacity in CHF. 22 However, the association of galectin-3 with SPPB and muscle strength in CHF remains elusive.
Heart-type fatty acid binding protein (H-FABP) is released in circulation following cardiac injury and has been used as a diagnostic marker of acute MI. 23 In addition, several studies indicate the prognostic potential of H-FABP in long-term survival following MI.23 –25 Recent evidence also indicates a role for H-FABP in age-related muscle loss, termed sarcopenia, which is the primary driver of reduced functional capacity in the older population. 26 These findings indicate the diagnostic potential of H-FABP to reduced functional capacity in CHF patients. However, no previous study has investigated the associations of H-FABP with SPPB in CHF patients.
The present study has several aims. First, to identify the potential associations of plasma galectin-3 and H-FABP levels with handgrip strength (HGS) in CHF patients. Second, to examine whether plasma galectin-3 and H-FABP can diagnose muscle weakness and wasting as critical contributors to functional compromise in CHF. Third, to assess the diagnostic potential of plasma galectin-3 and H-FABP in CHF. We hypothesized that plasma galectin-3 and H-FABP may be useful biomarkers of reduced functional capacity and cardiac dysfunction in CHF patients.
Materials and methods
Study design and participants
Healthy controls (age = 55–73 years, n = 59) and patients with ischemic (age = 56–74 years, n = 56) and non-ischemic (age = 57–71 years, n = 24) HF were recruited from Hayatabad Medical Complex, Peshawar, Pakistan, after obtaining the written informed consent from all study participants. The ethical approval for the study was obtained from the local ethics committee. Only the patients diagnosed with HF and presented with left ventricular ejection fraction (LVEF) < 50% were included. Patients reporting with a history of unstable angina, renal failure, heart transplantation, major surgeries, and prolonged bed rest within the past two months were excluded from the study. The anthropometric measurements were collected from the clinical records and routine assessment at the time of admission. All participants were Caucasian men of Pashtun or Punjabi ethnicities. This study was conducted following the Declaration of Helsinki. 27
Transthoracic echocardiography
A two-dimensional (2D) M-mode echocardiography was performed following standard guidelines of the American Society of echocardiography. 28 Briefly, the LV chamber dimension was measured through an echocardiography system using a 3 MHz phased probe (Apollo i700, Canon Medical Systems, Beijing, China), and cardiac contractile function and other parameters were calculated accordingly. An M-mode tracing was recorded in a parasternal long-axis view for the measurement of left ventricular chamber diameter, interventricular septal (IVS) thickness, left ventricular posterior wall (LVPW) thickness. The LV contractile function, including fractional shorting (LVFS) and LVEF, was automatically calculated by the system.
HGS and SPPB measurements
HGS was measured with a digital handgrip dynamometer (CAMRY, South El Monte, CA, USA) as described before. 29 Briefly, three attempts were performed by the participants to maximally squeeze the dynamometer with their dominant hands in a supine position. The highest of the three values was recorded for further analysis as described previously. 30 SPPB included the assessment of walking speed, balance, and chair sit-to-stand (STS) tests. Each test was given a score ranging from zero (worst performers) to four (best performers), and the cumulative score was used for analysis, as described elsewhere. 5
Sample preparation and measurement of plasma biomarkers
The blood sample was collected from patients and healthy controls in an appropriate anticoagulant as described previously. 31 Platelet-poor plasma was prepared following the protocol reported previously. 32 Plasma samples were analyzed using ELISA kits for Galectin-3 (Cat # ab269555, Abcam, Cambridge, UK), H-FABP (Cat # ab243682, Abcam, Cambridge, UK), and C-reactive protein (CRP) (R&D Systems, Minneapolis, MN, USA) levels, following the manual instruction.
Statistical analysis
Anthropometric measurements of the participants were presented using mean and standard error means as data met the assumption for normality. We used a one-way analysis of variance to compare the healthy controls with the two categories of CHF patients. The relationship between variables was analyzed by simple regression analysis. The areas under curve (AUCs) were calculated using receiver operating characteristics (ROCs) analysis to test the sensitivity and specificity of plasma galectin-3 and H-FABP levels in predicting CHF. Data were analyzed using GraphPad Prism 6, and the P value < 0.05 was statistically significant.
Results
Patient’s phenotypic and clinical presentation
A significant number of CHF patients (26 of 80) had one or more comorbidities, including hypertension, diabetes mellitus, and hypercholesterolemia. The body mass index (BMI) was significantly higher in ischemic (28.2 ± 1.6 kg/m2) and non-ischemic patients (27.9 ± 1.6 kg/m2) in comparison to healthy controls (26.3 ± 2.3 kg/m2) (Figure 1(A)). HF patients in both ischemic and non-ischemic groups were on standard treatment for CHF, including β-blockers, angiotensin receptor blockers (ARBs), angiotensin receptor neprilysin inhibitors (ARNIs), angiotensin-converting enzymes inhibitors (ACEIs), diuretics, and statins. The echocardiographic assessment of CHF patients showed a significantly greater left ventricular end-systolic dimension (LVESD) in both the ischemic (46.4 ± 6.1 mm) and non-ischemic (45.9 ± 5.7 mm) patients compared to healthy controls (34.8 ± 2.2 mm) (Figure 1(B)). Consistently, increased chamber dilatation was reflected by the cardiac contractile dysfunction as the percentage of LVEF was significantly lower in both ischemic (40.0 ± 3.3 %) and non-ischemic patients (40.1 ± 3.2 %) versus healthy controls (60.2 ± 3.6%) (Figure 1(C)).
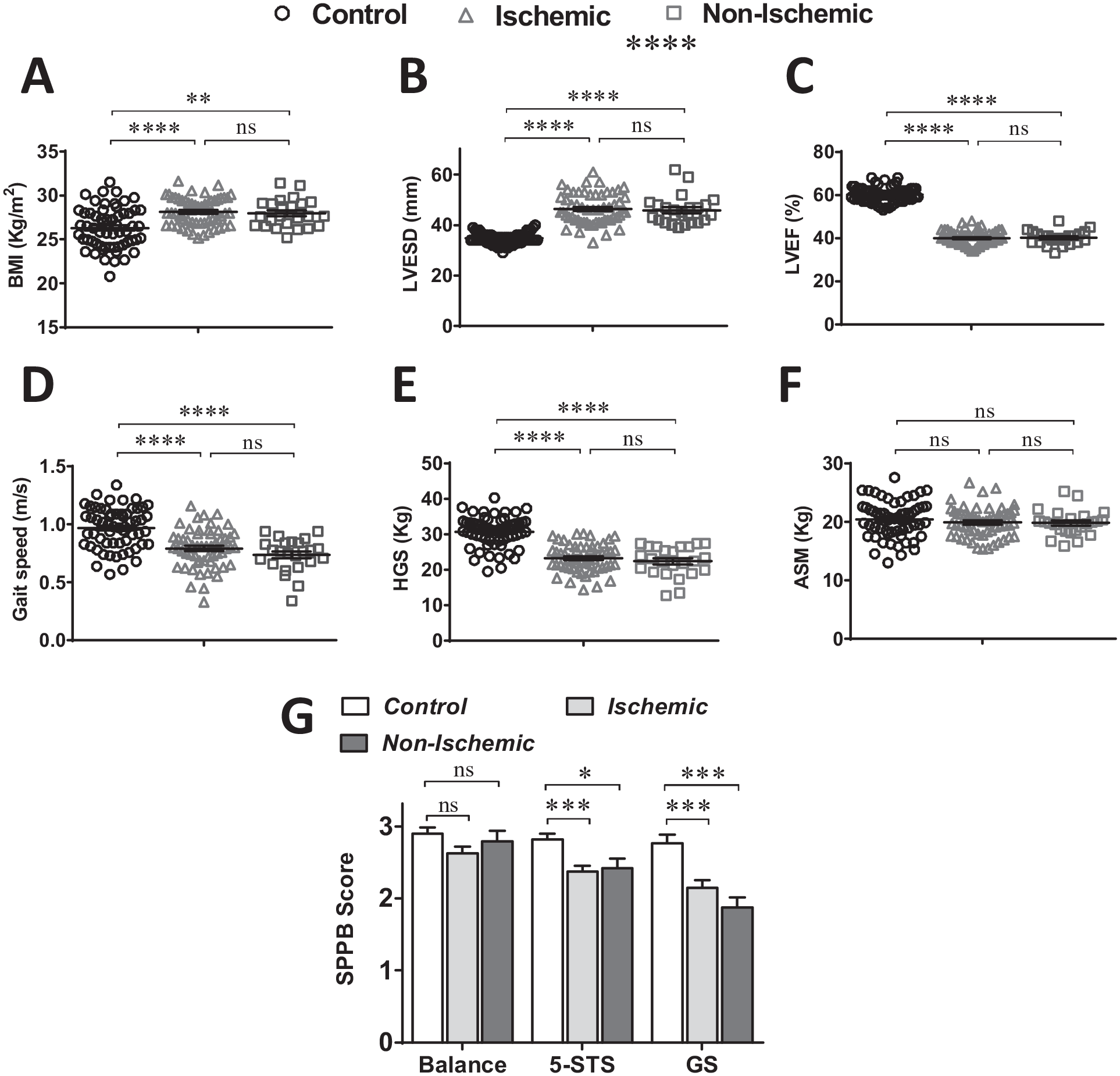
The scatter plots show (A) basic metabolic index (BMI), (B) left ventricular end-systolic dimension (LVESD), (C) left ventricular ejection fraction (LVEF), (D) gait speed, (E) handgrip strength (HGS), (F) appendicular skeletal mass (ASM), and (G) short physical performance battery (SPPB) scores for balance, five times chair sit-to-stand test (5-STS), and gait speed in controls and patients with ischemic and non-ischemic CHF. A one-way ANOVA followed by Tukey’s post hoc test was performed to compare the groups. *P < 0.05, **P < 0.01, ****P < 0.0001.
Physical performance of HF patients
The physical assessment showed a significantly compromised gait speed in the CHF patients, which was comparable between ischemic and non-ischemic patients (Figure 1(D)). Consistent with gait speed, the HGS was significantly lower in both the CHF patient groups compared to healthy controls (Figure 1(E)) though the appendicular skeletal mass (ASM) was comparable (Figure 1(F)). The SPPB score for balance was comparable between HF patients and controls; however, the score was severely reduced in the HF patients for five times STS (5-STS) and gait speed (Figure 1(G)). These observations strongly suggest that HF has a significant adverse impact on patient’s physical performance.
HF markers galectin-3 and H-FABP correlate with the physical performance of HF patients
Next, we assessed the level of different HF markers galectin-3, H-FABP, and CRP in both ischemic and non-ischemic HF patients and correlated them with their physical performance. As expected, the level of galectin-3 was highly upregulated (P < 0.01) in the ischemic HF patients. Conversely, the levels were unchanged in the non-ischemic patients versus controls (Figure 2(A)). Unlike galectin-3, the level of H-FABP was profoundly elevated in both ischemic (P < 0.0001) and non-ischemic (P < 0.001) HF patients than controls (Figure 2(B)). Similarly, the level of CRP was significantly higher in both ischemic (P < 0.0001) and non-ischemic (P < 0.0001) HF patients than controls (Figure 2(C)). Since plasma galectin-3 expression is associated with the intestinal inflammation, 33 we assessed the level of plasma zonulin, a regulator of the intestinal barrier, in the HF patients. A significantly elevated level of plasma zonulin was observed in the ischemic (P < 0.0001) and non-ischemic (P < 0.01) patients compared to controls (Figure 2(D)).
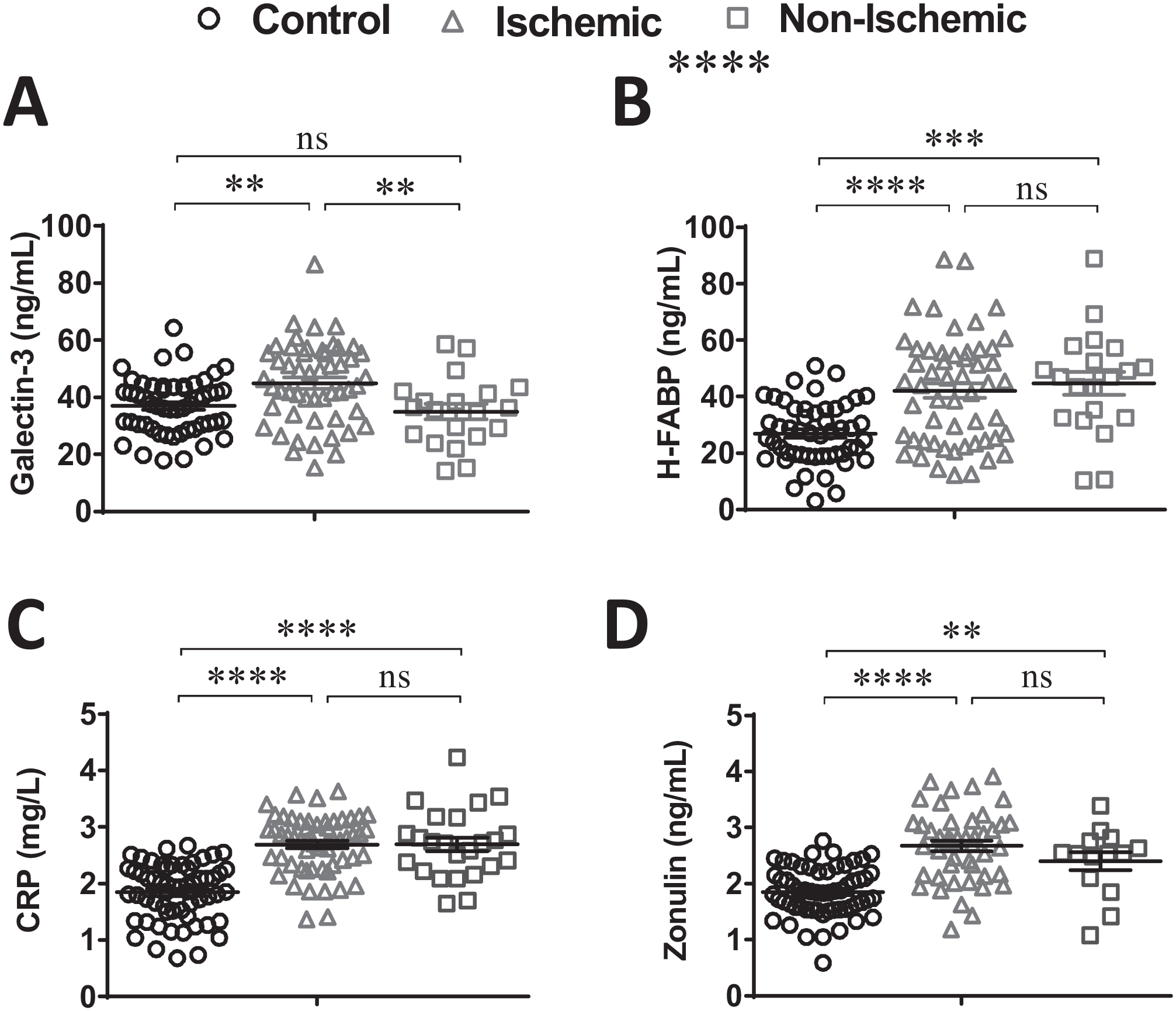
The plots show the level of (A) galectin-3, (B) heart-specific fatty acid binding protein (H-FABP), (C) C-reactive protein (CRP), and (D) zonulin in healthy controls and patients with ischemic and non-ischemic CHF. A one-way ANOVA followed by Tukey’s post hoc test was performed to compare the groups. **P < 0.01, ***P < 0.001, ****P < 0.0001.
Further analysis revealed a significant inverse correlation of galectin-3 with cardiac contractile function LVEF (r2 = 0.22, P < 0.0001) and a positive correlation with cardiac hypertrophy parameter LVPW thickness (r2 = 0.08, P = 0.01) (Figure 3(A) to (C)). Only a trend of positive correlation was observed between plasma galectin-3 and zonulin (Supplemental Figure 1(A)); however, CRP level was positively correlated (r2 = 0.09, P = 0.01) with the level of galectin-3 in the HF patients (Figure 3(D)). The physical performance parameters including SPPB (balance), SPPB (5-STS), and HGS were inversely correlated with the level of plasma galectin-3 (Figure 3(E) to (H)). However, there was no association between galectin-3 and gait speed (Figure 3(I)).
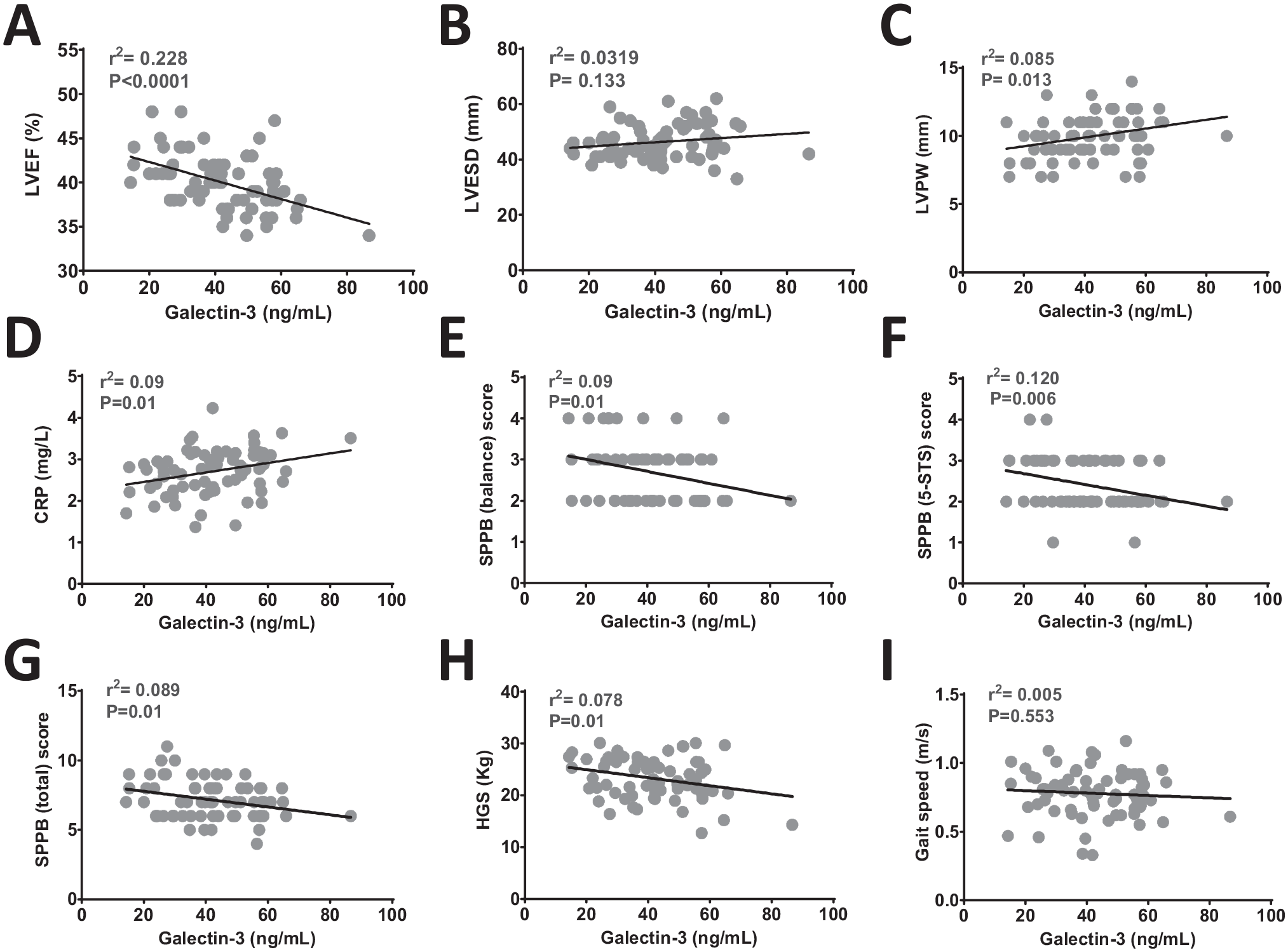
The correlation analysis of (A) LVEF, (B) LVESD, (C) LVPW thickness, (D) CRP, (E) SPPB (balance), (F) SPPB (5-STS), (G) SPPB (total), (H) HGS, and (I) gait speed with plasma galectin-3 in patients with CHF.
Next, the potential correlation of cardiac and physical performance parameters with H-FABP was assessed. Similar to galectin-3, H-FABP was inversely correlated with the LVEF (r2 = 0.10, P = 0.004), and a positive correlation was observed with LVPW thickness (r2 = 0.20, P < 0.0001) (Figure 4(A) to (C)). There was no association observed between H-FABP and zonulin (Supplemental Figure 1(B)) though the inflammatory marker CRP displayed a significant positive correlation with H-FABP (r2 = 0.13, P = 0.001) in the HF patients (Figure 4(D)). A strong inverse correlation (r2 = 0.11, P = 0.003) was observed between H-FABP and SPPB (balance) (Figure 4(E)). Interestingly, SPPB (5-STS) displayed no correlation with the levels of plasma H-FABP though the SPPB (total) was found negatively correlated (r2 = 0.06, P = 0.03) in these patients (Figure 4(F) and (G)). Consistently, H-FABP was inversely correlated with HGS; however, no association was established with the gait speed of HF patients (Figure 4(H) and (I)).
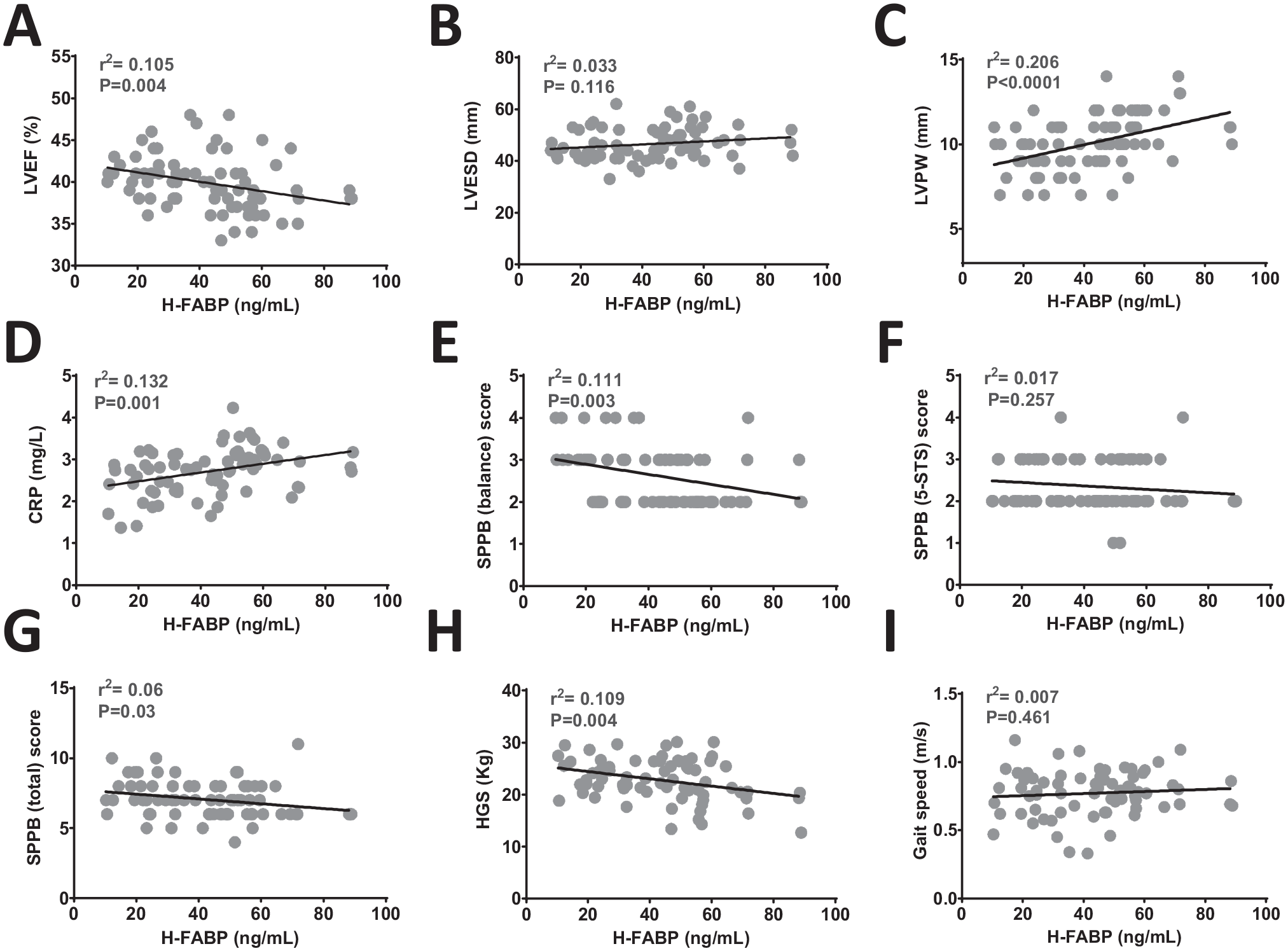
The correlation analysis of (A) LVEF, (B) LVESD, (C) LVPW thickness, (D) CRP, (E) SPPB (balance), (F) SPPB (5-STS), (G) SPPB (total), (H) HGS, and (I) gait speed with plasma H-FABP in patients with CHF.
Further investigation was performed to assess the diagnostic potential of galectin-3 and H-FABP by generating the ROC curves. The sensitivity and specificity of plasma galectin-3 and H-FABP in the diagnosis of HF showed the importance of these markers. A significantly higher ROC curve was observed for galectin-3 (AUC = 0.609, 95% confidence interval [CI] = 0.511–0.707, P = 0.03) (Figure 5(A)) and H-FABP (AUC = 0.752, 95% CI = 0.669–0.835, P < 0.001) (Figure 5(B)) in patients with HF.
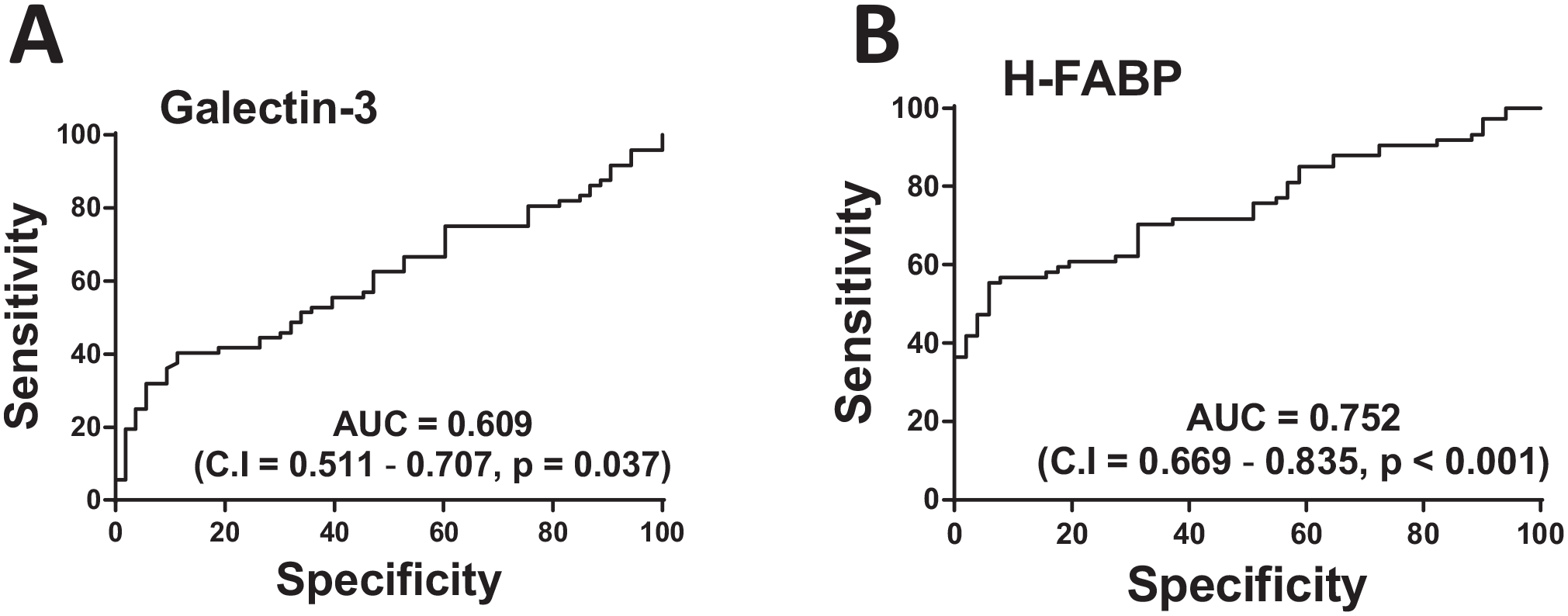
The receiver operating characteristic (ROC) curves for prediction of HF based on plasma (A) galectin-3 and (B) H-FABP in patients with CHF.
Discussion
Patients with CHF present a compromised functional capacity, including exercise intolerance, fatigue, and shortness of breath, 34 which has been associated with their prognosis. 8 Here, we show, for the first time, an association of HF markers with the functional disability of patients with CHF. Elevated levels of plasma H-FABP and galectin-3 were observed in only patients with ischemic HF but not in non-ischemic patients with HF. The physical capacity parameters, including SPPB scores, gait speed, and HGS, were significantly compromised in both the ischemic and non-ischemic HF patients. Both the assessed HF markers galectin-3 and H-FABP exhibited strong correlations with the physical performance parameters.
Pathogenesis and poor outcomes of a variety of cardiovascular diseases, including HF, have been associated with the elevated level of plasma galectin-3.19,35 Moreover, galectin-3 also plays a role in regulating immunity and inflammation. 36 Aldosterone induces the expression of galectin-3, which ultimately promotes tissue fibrosis, inflammation, and organ damage, including HF development.21,37 We observed an elevated level of plasma galectin-3, particularly in ischemic HF patients, and aldosterone may have an association with elevated levels of galectin-3 and inflammation induction in our ischemic cohort. Interestingly, the level of galectin-3 in patients with non-ischemic HF was comparable to healthy controls. These observations indicate that galectin-3 may play a more crucial role in ischemic than non-ischemic cardiac diseases. In complete agreement, studies have reported a profound induction of galectin-3 expression in acute and chronic MI, which is linked with cardiac inflammation, cardiomyopathy, and ultimately cardiac fibrosis post-MI.35,38 In contrast to ischemic cardiac disease, a study employing a mouse model has demonstrated that galectin-3 plays minimal roles in pressure overload–induced fibrotic cardiomyopathy. 39 Galectin-3-deficient mice showed no effect on pressure overload–induced survival, systolic and diastolic dysfunction, cardiac fibrosis, and hypertrophy. However, another study reported that pharmacological inhibition and genetic ablation of galectin-3 limit pressure overload–induced HF progression by attenuating cardiac remodeling and dysfunction largely through limiting cardiac fibrosis. 40 Our findings are consistent with MI studies where we only found induction of galectin-3 in the ischemic but not in non-ischemic HF patients. Inflammation is generally more aggressive in ischemic versus non-ischemic cardiac diseases and, as reported previously, 41 galectin-3 may induce systemic inflammation in HF patients, which may be one of the potential causes of the compromised physical performance of HF patients. It was strongly supported by a positive correlation between plasma CRP and galectin-3 and between galectin-3 and different parameters of physical performance in patients with HF.
The sensitivity of the plasma H-FABP for HF diagnosis was found to be superior to traditionally used markers, including cardiac troponin-I (cTn-I) and creatine kinase-MB (CK-MB) postacute MI. 42 Studies have reported H-FABP as a reliable marker, particularly for ischemic cardiac diseases42 –44; however, it is unclear if H-FABP can serve as a marker for non-ischemic CHF. We observed that H-FABP was upregulated equally both in ischemic and non-ischemic HF patients, which suggests its predictive potential in hypertension-induced HF and dilatative cardiac remodeling. Importantly, we identified an inverse correlation of H-FABP with contractile function but no associations with the remodeling parameter (LVESD), which indicates that it may serve as a better marker for contractile dysfunction but not to predict adverse cardiac remodeling.
There was no direct association of H-FABP with inflammatory disorders reported. However, studies have linked the level of adipocyte-FABP (A-FABP) with inflammation conditions. A-FABP was found associated with the expression of Toll-like receptors, macrophage activation, synthesis, and release of pro-inflammatory cytokines interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α), which induces inflammation and sepsis. 45 Consistent with these observations for A-FABP, our study, for the first time, reveals a strong positive correlation between H-FABP and CRP in patients with CHF. Inflammatory markers IL-6, CRP, and IL-1RA have previously been reported to show a strong association with compromised physical performance and muscle strength in the elderly population. 46 More specifically, a recent study has established an association of elevated CRP levels with poor physical performance; however, IL-10 and TNF-α levels did not show a prominent association with poor physical performance. 47 Importantly, the anti-inflammatory dietary intervention can improve physical performance in athletes. 48 In complete agreement, we identified significant inverse correlations of H-FABP with physical performance indicator SPPB (balance) and HGS in patients with chronic HF. These findings indicate that the induction of H-FABP in HF patients may adversely affect the physical performance of HF patients partly through inducing the inflammatory reaction.
The monocentric nature of our study and the recruitment of exclusively male population from the same ethnic background is the major strength. It minimizes the possibility of race, culture, gender, and assessment techniques–related variability. However, the exclusion of female patients may also be a limitation, as the gender-specific differences may exist between the association of plasma zonulin and echocardiography parameters. Also, we did not take patients’ history of inflammatory diseases which itself may affect the level of plasma CRP.
Taken together, here we report a strong association of galectin-3 and H-FABP with cardiac hypertrophy (LVPW thickness) and contractile dysfunction (LVEF) in patients with CHF. The physical performance parameters SPPB scores, gait speed, and HGS were significantly compromised and found to be associated with the levels of plasma galectin-3 and H-FABP in CHF. Moreover, a robust association of plasma CRP with galectin-3 and H-FABP suggests the induction of systemic inflammation in CHF patients which may play roles in the development of physical disability. Targeting inflammatory pathways may potentially help preserve or improve the physical performance of patients with CHF.
Supplemental Material
sj-pdf-1-ebm-10.1177_15353702231151980 – Supplemental material for Plasma Galectin-3 and H-FABP correlate with poor physical performance in patients with congestive heart failure
Supplemental material, sj-pdf-1-ebm-10.1177_15353702231151980 for Plasma Galectin-3 and H-FABP correlate with poor physical performance in patients with congestive heart failure by Firdos Ahmad, Asima Karim, Javaidullah Khan and Rizwan Qaisar in Experimental Biology and Medicine
Footnotes
Authors’ Contributions
Conceptualization: RQ and FA; Data curation: RQ, AK, JK, and FA; Formal analysis: RQ and FA; Funding acquisition: RQ and FA; Investigation: RQ, AK, JK, and FA; Methodology: AK and JK; Project administration: RQ, AK, JK, and FA; Resources: RQ, AK, JK, and FA; Supervision: AK and JK; Validation: RQ, AK, JK, and FA; Writing – original draft: FA and RQ; Writing – review & editing: FA and RQ.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The ethical approval for the study was obtained from the local ethics committee.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by Targeted and Collaborative grants (1801090144, 22010901112) to Firdos Ahmad and Competitive grants (2001090177 and 22010901121) to Rizwan Qaisar from the University of Sharjah.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.