
Abstract
Thalamic neuromodulation for drug-resistant epilepsy has evolved from ablative thalamotomy to network-guided deep-brain stimulation (DBS) and responsive neurostimulation (RNS). Currently, the only Food and Drug Administration-approved DBS target is the anterior thalamic nucleus, which provides substantial and durable seizure reduction, particularly in limbic and temporal epilepsies. There is growing evidence that the centromedian and pulvinar nuclei are implicated in generalized, multifocal, and posterior neocortical epilepsies. Advanced imaging, probabilistic atlases, and connectomics can be used to refine targeting; however, they are limited by patient specificity, acquisition burden, and interatlas variability. Thalamic stereoelectroencephalography may clarify potential neuromodulation target selection by characterizing ictal recruitment, network dynamics, and biomarkers. Although DBS and RNS each have unique benefits, no modality has demonstrated superior. Pediatric data are heterogeneous and scarcer, but seizure reduction and safety profiles are similar to adults. Further studies are needed to optimize neuromodulation target selection and programming paradigms.
Keywords
Introduction
Over the past 8 decades, thalamic neuromodulation has evolved from irreversible lesioning to reversible stimulation techniques. Ablative thalamotomy was used to treat movement and psychiatric disorders in the 1940s to 1950s. 1 In 1947, a human stereotactic frame, developed by Spiegel and Wycis, initiated stereotactic approaches in neurosurgery. 2 Reversible modulation of the thalamus using externalized electrodes was introduced in the 1960s by Carl Wilheim Sem-Jacobsen. 2 More refined deep-brain stimulation (DBS) emerged in 1987, when the first implantable pulse generator was developed by Alim Louis Benabid. 3 An implantable device allowed for continuous, chronic stimulation by a lithium battery, permitting patient mobility and long-term treatment. In the 1970s to 1980s, Velasco et al investigated centromedian nucleus (CMN) stimulation for epilepsy. 4 Twenty-five years later, responsive neurostimulation (RNS) was developed as a closed-loop system.5,6 In 2014, it was approved by the Food and Drug Administration (FDA) as a treatment option for drug-resistant focal epilepsy (DRE) in adults with focal onset seizures. 6 In 2018, following the landmark Stimulation of the Anterior Nucleus of the Thalamus for Epilepsy (SANTE) trial, anterior nucleus of the thalamus (ANT) DBS was FDA-approved. 7 In this review, we explore the current practice and emerging innovations in thalamic neuromodulation for epilepsy, focusing on the latest developments and potential future directions.
Neuromodulation Target Selection
Anterior Nucleus
ANT is the only target currently FDA-approved for DBS in DRE. 7 The SANTE trial was a multicenter, double-blinded, randomized controlled study with 110 adults who had medically refractory focal-onset seizures, including focal to bilateral tonic–clonic seizures. 7 They showed 43% of patients had ≥50% seizure reduction at 1 year, and 68% of patients had ≥50% reduction at 5 years. 7 Subgroup analysis showed better outcomes for patients with temporal lobe epilepsy, followed by those with frontal lobe epilepsy. 7 Sustained seizure reduction and improvement in quality of life were seen over a 5-year follow-up. 7 At 7-year follow-up, median seizure frequency was reduced by 75% from baseline. Ten-year follow-up showed no worsening of adverse effects, suggesting long-term safety. 8 ANT is thought to be a propagation point in focal epileptogenic networks that involve the anterior half of the hippocampus and midline frontal seizures. 9 Direct targeting using FGATIR MRI (fast gray matter acquisition T1 inversion recovery magnetic resonance imaging) sequence is recommended to identify the mammillothalamic tract (MTT), aiming for the anterior half of the ANT with the deepest contact placed at the junction of ANT–MTT. 10 ANT target is highlighted on the FGATIR sequence in Figure 1(a).
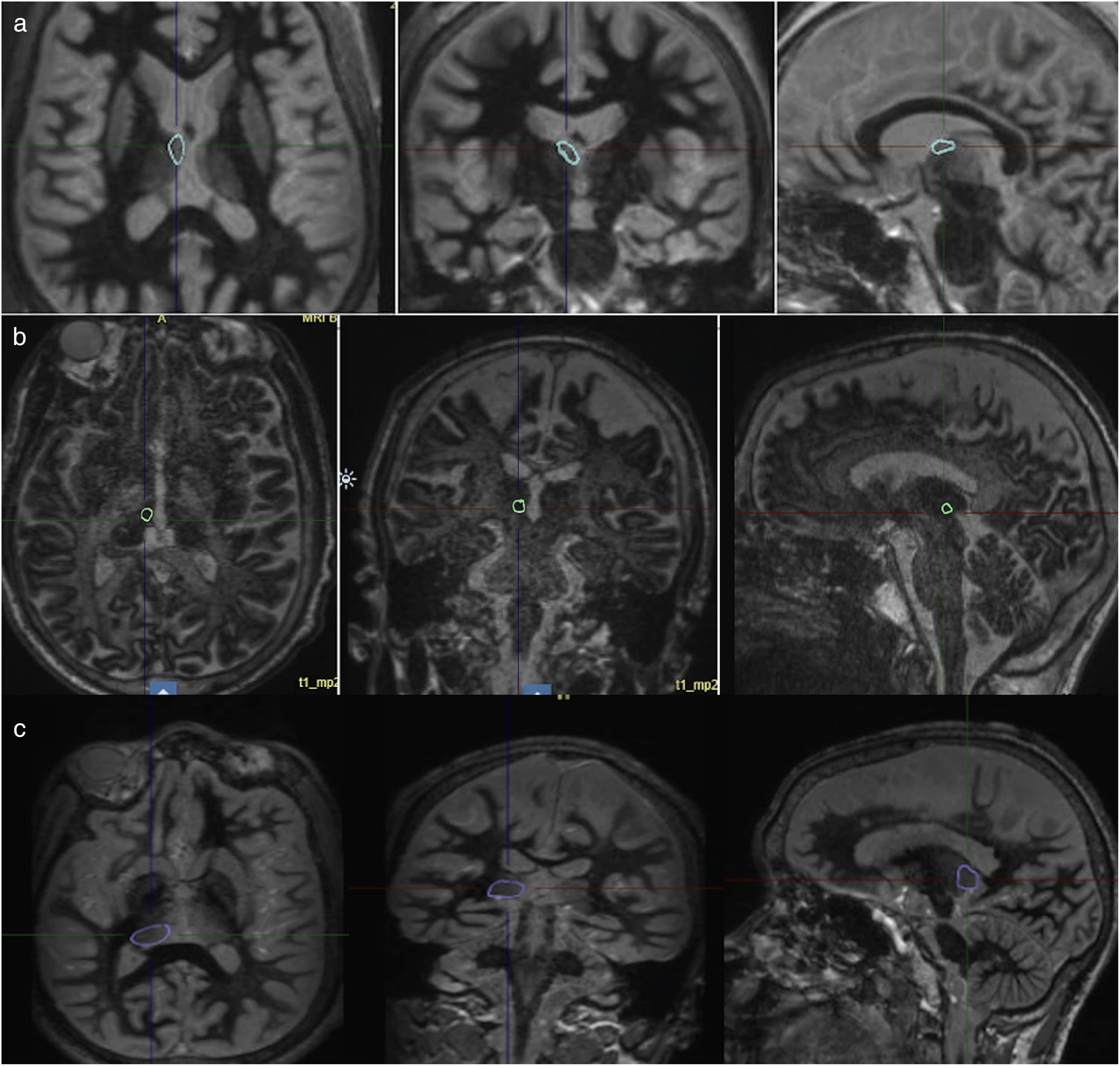
Thalamic targets. (a) FGATIR MRI sequence of the anterior nucleus, right ANT circled . (b) MP2RAGE MRI sequence of the CMN, right CMN circled. (c) FGATIR sequence, right pulvinar circled. FGATIR: fast gray matter acquisition T1 inversion recovery; MRI: magnetic resonance imaging; ANT: anterior nucleus of the thalamus; CMN: centromedian nucleus; MP2RAGE: magnetization prepared to rapid 2 aquisition gradient echo.
Centromedian Nucleus
CMN of the thalamus is a promising target actively being studied. The Estimation of Thalamic Efficiency in Lennox–Gastaut Syndrome trial is a prospective, double-blind, randomized controlled trial which assessed CMN DBS in the Lennox–Gastaut syndrome (LGS). 11 Twenty adults with LGS underwent bilateral CMN DBS. Significant electrographic seizures were observed, but the study was small and underpowered. 11 In a retrospective trial of 5 patients with drug-resistant generalized epilepsy who received CMN DBS, there was a median reduction in seizure frequency by 66%. Volumetric “sweet-spot” was mapped, showing that the best outcomes were associated with stimulating the middle ventral CMN. They conclude that the ideal target in CMN for DBS may be syndrome-specific. 12 The NAUTILUS study is an ongoing, prospective, randomized, single-blinded, sham-controlled, multicenter clinical trial investigating CMN RNS in patients with idiopathic generalized epilepsy. Preliminary results show a satisfactory safety profile and a low rate of adverse events 12 weeks postimplantation. They showed no statistical significance in the time between the first and second generalized tonic–clonic (GTC) seizures when comparing the active with the sham stimulation group. There was clinical and statistical significance in a subgroup of patients who had a lower baseline frequency of GTCs. They show overall a reduced percentage of seizure frequency, improvement with time, and an improvement in seizure-free days over the first year of treatment. 13 CMN is postulated to be a propagation point for generalized and multifocal epilepsy. 9 Direct targeting of the CMN can be achieved using FGATIR, or more clearly on a magnetization prepared to rapid 2 aquisition gradient echo (MP2RAGE) MRI sequence (Figure 1(b)). CMN nucleus is hyperintense to its bordering pulvinar, mediodorsal, and perifascicular nuclei. Advanced imaging is required for better visualization of the CMN due to its indistinct borders.
Pulvinar Nucleus
The pulvinar nucleus has been explored for occipital seizures and as an alternative target for temporal epilepsies. 9 Filipescu et al reported a series of 8 patients with temporal lobe DRE. Ipsilateral pulvinar stimulation showed clinically less severe seizures, but overall seizure duration was unchanged. 14 Burdette et al implanted corticothalamic RNS electrodes in the pulvinar and parietal or occipital cortex in 3 patients. Pulvinar was successfully stimulated when neocortical seizure was detected. 15 Preliminary results from an open-label prospective trial of medial pulvinar DBS for focal DRE show that out of 5 patients, there was a nonsignificant trend to seizure reduction at 6 months that is more evident at 1 year, with a mean reduction of 45%. There was improved seizure severity and an improvement in quality of life. 16 Lateral pulvinar may be implicated in occipital and parietal networks, and medial pulvinar in temporal and orbitofrontal epilepsies. 9 The pulvinar is a large nucleus amenable to direct targeting using MP2RAGE or FGATIR MRI (Figure 1(c)).
Proposed Mechanisms of Network Modulation
Epilepsy is considered a network disorder rather than stemming from a specific epileptogenic focus. Instead of directly removing, ablating, or disconnecting the identified seizure foci from the surrounding healthy network, neuromodulation targets specific propagation points within the epileptogenic network to inhibit the spread of seizure activity, promote plastic changes in thalamocortical networks, and disrupt the epileptogenic network while preserving the healthy brain networks.
Network Jamming
The hypotheses suggested as the mechanism of neuromodulation in seizure propagation include the “jamming theory.” This proposes that high-frequency stimulation causes a functional lesion that blocks the propagation of incoming ictal activity, as well as desynchronizing the brain by disrupting pathological oscillations and coherence. The result of this is neuroplasticity over the long term by changing neurotransmitter release and channel dynamics.15–18
Network Desynchronization
The most accepted mechanism of neuromodulation is desynchronization of the epileptogenic network. The thalamus serves as a propagation point in various epileptic networks. It is an integrative hub from which pathological activity can spread from 1 cortical area to another. Hypersynchronization of brain activity has been observed during seizure activity. 19
In epilepsy with frontal–temporal seizures, the ANT and hippocampus are synchronized. High-frequency stimulation of the ANT causes local field potentials (LFPs) in ANT to desynchronize with LFPs bands in the ipsilateral hippocampus and neocortex. 20 Similarly, in multifocal and generalized-onset epilepsy, bilateral CMN stimulation desynchronizes cortically driven epileptogenic activity from subcortical networks. 21 The neuromodulatory effect of stimulating specific thalamic nuclei is thought to reduce synchronized populations and is the main mechanism for progressive reduction of seizures over time. 22 Stimulation during low-risk seizure states may have a greater impact than desynchronization of an ictal potential by promoting plasticity that reduces abnormal synchronization. 23
Thalamic Imaging
Probabilistic Mapping
Probabilistic atlases are built from high-resolution 7T MRI images combined with histological data to create a precise segmentation map of individual thalamic nuclei. 24 MRI-defined thalamic nuclei are integrated with diffusion-derived fiber tracts to enable the identification of thalamic nuclei. Precise imaging-based localization of thalamic nuclei allows for more informed electrode placement and neuromodulation targeting than just segmentation alone. 9 Limitations of probabilistic mapping include a lack of patient specificity, due to the fact that probabilistic atlases are an average of anatomy from many individuals. Furthermore, segmentation and registration of multimodal imaging data into atlases can introduce targeting error. 25 Lastly, different atlases have variable anatomical definitions, methods of segmentation, and population averages. Target localization may therefore be inconsistent across different atlases. 25
Connectomics
Functional and diffusion MRI are useful to show thalamic involvement in seizure networks by mapping the thalamocortical connections and functional hubs.26,27 Degree centrality (DC) and eigenvector centrality (EC) are metrics used to quantify the importance of specific propagation nodes with the network. 28 A high DC region suggests a region with many direct anatomical or functional connections. EC reflects the quantity and quality of connections and captures the node's influence in the network. High DC and EC in a specific thalamic nucleus, indicating functional hyperconnectivity, suggest that a nucleus is a key epileptogenic propagation point.26,28 In contrast, structural connectomics with diffusion tensor imaging shows disrupted structural integrity in pathological thalamocortical networks. 26
Greater baseline thalamic functional connectivity correlates with better clinical response to neurostimulation and indicates optimal electrode placement. 29 Limitations of high-quality connectomic data include long acquisition and processing times. Advanced computational tools for pre-/postprocessing, noise correction, tractography, and network modeling are resource-intensive, high-cost, and time-intensive, requiring expert knowledge and affecting reproducibility between institutions. 30
Thalamic Stereoelectroencephalography
Thalamic stereoelectroencephalography (SEEG) can be used when the epileptogenic network is hypothesized to propagate through or involve the thalamocortical circuits. 31 Critical information from SEEG, including the epileptogenicity and network dynamics, can guide prognostication, subsequent neuromodulation therapy, and target selection. 32 The main clinical indication for thalamic SEEG is to inform treatment strategies in complex drug-resistant epilepsy cases where cortical localization is inadequate. 33
Target Selection
Seizure semiology and noninvasive evaluation—including video electroencephalogram, MRI, and metabolic studies—are first used to hypothesize the seizure network and propagation pathways. 33 If localization is inconclusive or suggests complex or widespread networks, thalamic involvement can be considered. Based on the anatamo-electroclinical correlations and hypothesis, the thalamic nuclei involved in the seizure propagation can be postulated. 32
ANT is connected with limbic structures and is implicated in temporal lobe epilepsy, as well as seizures originating from the orbitofrontal region. CMN is connected to widespread cortical areas in its use in generalized/multifocal epilepsy, however more specifically, CMN has an association with sensorimotor regions of the precentral gyrus, postcentral gyrus, and supplementary motor areas. The mediodorsal nucleus is connected with the prefrontal cortex. Finally, the pulvinar nucleus is involved in occipital pathways with extension into the parietal and temporal lobes. 32
FGATIR or MP2RAGE MRI should be used to delineate thalamic nuclei. 33 Electrodes can be planned for cortical sampling such that the cortical entry points align with the hypothesized epileptogenic network before reaching the thalamic target. An illustration of SEEG leads (dashed line) in the ANT and CMN is shown in Figure 2(a) and (b), with the sampling of cortex along the trajectory. In addition to an orthogonal approach, an oblique entry from the vertex is possible; however would require additional electrodes.
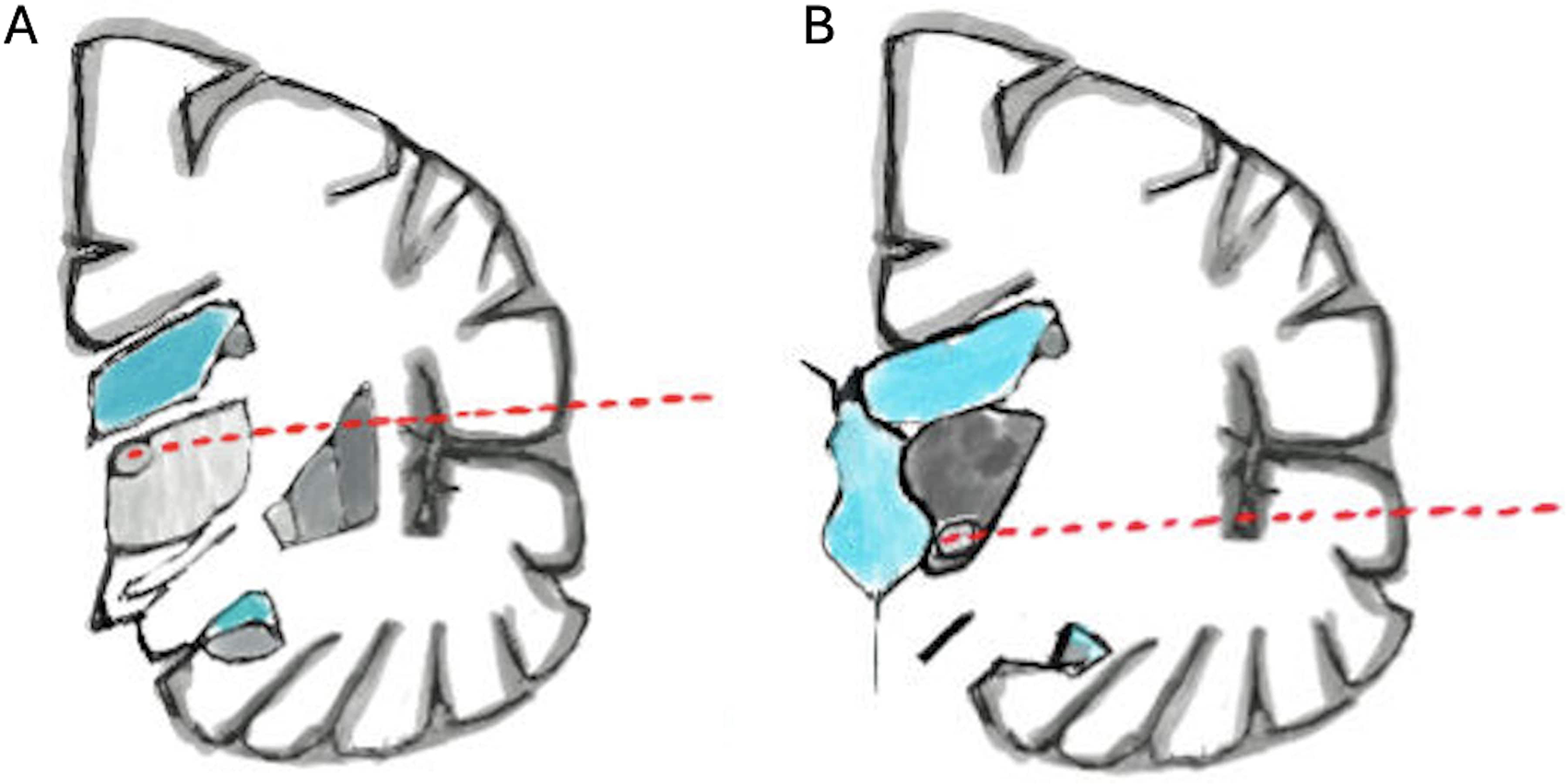
SEEG in thalamic nuclei. We show coronal illustrations of the anterior nucleus and the centromedian nucleus in (a) and (b). Along lateral orthogonal trajectories of the SEEG (red), cortices that are hypothesized as part of the overall epileptogenic network are sampled. In targeting the anterior nucleus (a), the insula and the frontal operculum can be sampled. In targeting the centromedian nucleus (b), the superior temporal gyrus and the temporal operculum can be sampled. In targeting the pulvinar, the posterior superior temporal gyrus, posterior insular gyri, and operculum can be sampled (not shown). SEEG: stereoelectroencephalography.
Neurophysiological Recordings
Thalamic SEEG helps characterize the role and timing of thalamic involvement in seizure generation and propagation, serving both as a bridge between diagnostic mapping and neuromodulation planning and as means to validate hypotheses about regional involvement prior to resection. 33 With the advent of chronic sensing from thalamic leads, the same signals are now interrogated to answer 2 practical questions: where should we stimulate, and where should we record. In this framework, SEEG interpretation emphasizes not only whether a nucleus participates in seizures, 34 but also the reliability, latency, and spectral content of that participation, so that the most informative contacts can later be selected for DBS or RNS. 33
Thalamic contacts typically show low-amplitude activity relative to neocortex, and careful visualization, that is, turning up the gain on the thalamic channels, is required to appreciate their dynamics. Connectivity analyses applied to thalamic SEEG, together with diffusion and functional MRI-based connectomics, further illustrate how each nucleus is embedded in the epileptogenic network and help identify propagation hubs. Ongoing prospective work is standardizing these analytic approaches and their integration into presurgical and neuromodulation planning. During ictal evolution, LFPs reveal trends in patterns across thalamic nuclei. ANT tends to be engaged early in temporal and limbic seizures, with increases in low-frequency power and higher-frequency activity as seizures propagate and secondarily generalize.34,35 The CMN is preferentially recruited in generalized and frontal epilepsies, often with ictal delta activity and spike–wave complexes that mirror its broad cortical projections.36,37 The pulvinar acts as a key relay for parietal, occipital, and lateral temporal networks, as well as those that secondarily generalize. 37 The mediodorsal nucleus participates in cognitive and behavioral seizures through its connections with prefrontal cortex, frequently demonstrating ictal theta and alpha rhythms. 37 Multisite recordings, however, highlight substantial variability in the timing and consistency of thalamic recruitment both between patients and across seizures in the same individual, underscoring the need for individualized targeting strategies.
In practice, these neurophysiological signatures are integrated with anatomy, imaging, and clinical semiology to decide whether a given nucleus should be used primarily as a sensing site, a stimulation target, or both. Nuclei that show consistent, early recruitment with reproducible spectral changes are attractive candidates for closed-loop detection and responsive stimulation, whereas late or inconsistent involvement may favor cortical stimulation with thalamic leads reserved for monitoring network spread. Ongoing prospective thalamic SEEG studies and early thalamic RNS experience will be essential to determine which biomarkers best predict long-term seizure reduction and to refine how thalamic recordings are used to plan and optimize neuromodulation.
Mode of Stimulation
As a cortical synchronizer, the thalamus mediates the propagation of epileptic activity. By desynchronizing pathological rhythms, neuromodulation acts to induce plastic changes in thalamocortical circuits. 36 Given that the brain demonstrates dynamic changes, the constant stimulation through open-loop is questioned and gives way to the possibility of closed-loop stimulation.
Open- Versus Closed-Loop
Open-loop neuromodulation delivers continuous stimulation at fixed parameters set manually by the programmer. The advantages are lower-energy requirements (due to the lack of closed-loop detection algorithms), extensive validation, and it has predictable programming.9,38 The disadvantages are the lack of feedback control, risk of overstimulation or side effects, and the inability to adapt to daily changes or seizures. 39 Closed-loop neuromodulation is on-demand, uses feedback from physiological activity in the form of a biomarker, such as delta–theta rhythms, to adjust stimulation in real time. 39 The stimulation paradigm can be either responsive, as in RNS or vagus nerve stimulator (VNS), or adaptive, as in DBS. Responsive stimulation stimulates when the given biomarker is detected, while adaptive stimulation constantly stimulates, but varies the amplitude based on LFPs. The advantage of these is that therapy can be individualized to reduce side effects, improve efficacy, and permit longer battery life. The disadvantages are the need for advanced signal processing, and risk of artifacts or false detections.38,40,41 It is not yet clearly demonstrated which modality and which paradigm (responsive vs adaptive stimulation) is optimal.
Cortico–Thalamic Stimulation
Cortico–thalamic stimulation targets the reciprocal networks between cortex and thalamus. It modulates the excitatory and inhibitory homeostasis between seizure-generating and relay circuits. Currently, corticothalamic stimulation studies are retrospective, small-cohort investigations showing promising efficacy and safety in DRE. In a retrospective series of 7 patients evaluating open-loop 4-lead thalamocortical stimulation, simultaneous cortical and thalamic leads were implanted. The seizure networks of their cohort were diverse, and the implantation targets varied. They showed median seizure reduction of 93% and no serious complications. 42 Closed-loop corticothalamic systems, such as RNS, can be applied for tailored therapy to neurophysiological dynamics rather than static programming, allowing for optimized seizure control and limiting extraneous stimulation. Since DBS is only in a depth electrode configuration, it is usually not used in this manner.
RNS in ANT and CMN
The FDA approval for RNS indicates its use for adults with 1 or 2 localized epileptogenic zones causing focal-onset seizures. 42 The RNS System Pivotal trial was a randomized, multicenter, double-blinded, sham-controlled study evaluating the efficacy of RNS with stimulation of cortical or near-cortical targets. 6 Thalamic targets were not explored. 6 Various groups have investigated RNS in ANT and CMN by extrapolating indications from open-loop DBS trials—particularly the SANTE trial, which targets the limbic propagation pathways through the ANT in focal epilepsy, and case series on CMN DBS, targeting generalized or multifocal epilepsies. Elder et al published a series of 3 patients with longstanding focal epilepsy with impaired consciousness. RNS leads targeted the ANT and epileptogenic cortex. 43 Two patients had bilateral ANT stimulation, and 1 patient had unilateral stimulation. All patients had a 50% reduction in seizures and no adverse effects at 33-month follow-up. 43 Beaudreault et al published a series with 14 patients implanted with bilateral ANT or CMN, or unilateral ANT or CMN in combination with cortical strip leads. 44 The median follow-up was 3.1 years. They showed 4 of 14 patients had 75% to 99% improvement in seizure frequency, 1 of 14 had 50% to 74% improvement in seizure frequency, and 3 of 14 had 0% to 24% improvement. 45 Burdette et al published a retrospective study of 19 patients with broad onset focal epilepsy implanted with closed-loop RNS that targeted the ANT, CMN, or pulvinar. A total of 79% of patients achieved ≥50% seizure reduction across all the thalamic targets. 45
Pediatric Thalamic Neuromodulation
Pediatric thalamic neuromodulation is a growing area that has shown evidence supporting safety and efficacy in DRE. 45 Pediatric patients with DRE who are not candidates for resection or disconnection, or those with multifocal or generalized epilepsy, may be considered for neuromodulation. 46 In a systematic review of 38 children with generalized drug-resistant epilepsy who received thalamic RNS, 57.9% had >50% seizure reduction. 47 Uchitel et al showed in a series of 8 children implanted with RNS (targets: bilateral hippocampi and temporal lobes), 80% of patients achieved seizure freedom, and 20% had >90% seizure reduction. 48
In the same pediatric series, 9 children were implanted with DBS (targets: ANT, CMN, or Pulvinar). They showed that 71% of patients with DBS had ≥50% reduction in seizures, and all patients had reduced seizure burden at ≥1 year follow-up. 48 A systematic review of 40 children who received DBS (CMN and ANT) for mixed seizure types showed that 85% had reduced seizure frequency, and 12.5% became seizure-free. 47 A meta-analysis including 72 children with DBS showed that 75% of patients had over 50% seizure reduction, with 11.1% achieving seizure freedom. 49 In total, 80% of patients with LGS who were treated with DBS reported favorable outcomes with CMN as the preferred target. 49 In a systematic review of 50 children who received DBS for multifocal and generalized seizures, 76.8% had >50% seizure reduction. 47
The Pediatric Epilepsy Research Consortium and LGS Special Interest group published a review that reports neuromodulation methods (a combination of VNS, DBS, and RNS) in the treatment of LGS have an outcome ranging from 50% to 60% reduction in seizure burden. 50 Overall, the safety and outcome profile in pediatric populations aligns with that of adults. 50 However, the pediatric literature is characterized by smaller sample sizes and heterogeneity in baseline seizure network, stimulation target selection, type of neuromodulation therapy, and follow-up duration. 50
Conclusion
Thalamic neuromodulation is an evolving approach for DRE that leverages neurostimulation of thalamic nuclei to modulate epileptogenic networks. Current methods have transitioned from thalamotomy and open-loop DBS to closed-loop stimulation utilizing network-guided strategies. The ANT, the only FDA-approved DBS target, has shown durable seizure reduction and is effective for limbic and temporal epilepsies. The CMN nucleus of the thalamus is actively being studied for multifocal and generalized epilepsies by responsive targeting of thalamocortical synchronization. Recent network-based approaches, including characterization of thalamocortical pathways, thalamic SEEG, and use of closed-loop systems, allow us to expand management options for patients with poorly localized or multifocal epilepsies. These advances position thalamic neuromodulation as a developing field that integrates anatomical precision, network physiology, and responsive technologies to improve care for patients with refractory epilepsy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics and Patient Consent
Ethics and patient consent were not necessary for this review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.