
Abstract
Objective:
To describe treatment patterns for perimenopause and menopause symptoms, including hormone therapy (HT), nonhormonal medications, and supplements and to examine peer, social, and structural correlates of HT use in a nationally representative sample of U.S. women.
Methods:
In February 2025, a cross-sectional online survey was conducted through YouGov (n = 1,500 women). Eligible participants were women who reported being told by a healthcare professional (HCP) they were in perimenopause or menopause, or who were within the midlife age range associated with these stages (45–54 years). Participants reported symptom burden, treatment use, peer influences, and perceived barriers to care. Multivariable logistic regression was used to identify demographic and sociocultural predictors of HT use.
Results:
Approximately half of the respondents reported vasomotor symptoms, yet only 7.2% reported current HT use. Marked disparities by education and income were observed: women with a 4-year college degree or higher had more than twofold higher odds of HT use, and those with household incomes >$100,000 had twice the odds compared with those earning <$20,000 (p < 0.001). Peer influence was independently associated with treatment choice: women whose peers used HT had 3.4-fold higher odds of HT use, whereas peer use of mind–body approaches was associated with 63% lower likelihood of HT use.
Conclusions:
In a nationally representative sample of U.S. women with substantial symptom burden, reported HT use was low. Treatment decisions were strongly shaped by sociodemographic disparities and peer influence, suggesting opportunities for targeted risk communication and equitable access to evidence-based menopause care.
Keywords
Introduction
Menopause is a prolonged life stage that can affect health and quality of life. In the United States, women spend up to 40% of their lifespan postmenopausal, and more than 63 million women are aged 50 years or older, reflecting the large population affected.1,2 The menopause transition begins with menstrual cycle variability and continues until the final menstrual period, often spanning several years. Perimenopause encompasses the late menopausal transition and the first year following menopause. Vasomotor symptoms (VMS) are often most severe during perimenopause but may persist for many years.3,4
Hormone therapy (HT) remains the most effective treatment for VMS such as hot flashes and night sweats, as demonstrated by randomized controlled trials and endorsed by major guidelines, including The Menopause Society. 5 However, communication around HT has been shaped by the interpretation of the Women’s Health Initiative (WHI) results, which led to widespread concern and a sustained decline in use due to risks being presented without age stratification. 6 The lack of individualized risk communication influenced both public perception and prescribing practices. 7
No other therapy in recent decades has experienced such a rapid, widely publicized, and enduring decline in use, followed by continued underutilization despite subsequent guideline support for selected patients. Between 1999 and 2020, HT use in the United States declined from 26.9% to 4.7%. 8 Although declines were observed across all groups, they were most pronounced among non-Hispanic Black women. Socioeconomic factors including income, insurance, and education continue to predict use, revealing disparities in access and care. At the same time, Black and Hispanic women consistently report greater symptom burden, suggesting inequities in access, communication, cultural context, and trust in medical guidance.9,10
For context, most other therapies that saw similarly abrupt declines, such as high-dose estrogen for prostate cancer, 11 were either permanently abandoned following evidence of harm or later reestablished for selected indications as data clarified their safety. HT’s trajectory is unique because robust evidence and current guidelines support HT as first-line therapy for bothersome VMS in appropriately selected women younger than 60 years or within 10 years of menopause onset, 5 yet utilization remains low.
These national patterns reflect not only changes in clinical evidence and guideline interpretation but also the influence of peers, family, and healthcare professionals (HCPs) on women’s decision-making and the cultural environment in which information is being shared. Understanding how these social and structural factors interact is essential to narrowing persistent gaps in HT utilization and promoting equitable, evidence-based care.
Few studies have examined how women integrate medical advice with personal, economic, and social factors when deciding about menopause treatment. This study addresses that gap by describing patterns of treatment use for perimenopause and menopause symptoms, including HT, nonhormonal medications, and supplements, by evaluating peer, social, and structural correlates of HT use. By situating HT decision-making within both structural and sociocultural contexts, this work aims to identify opportunities to strengthen health communication and advance equity in menopause care.
Methods
Data collection
Data were collected through a YouGov survey administered between February 22 and 28, 2025, with a total of 1,500 women. Participants were drawn from the U.S. YouGov survey panel, which encompasses approximately 1 million U.S. residents who had agreed to participate in surveys and were provided incentives in the form of YouGov points redeemable for gift cards and other rewards. Eligible participants met one of the following criteria: (1) currently in perimenopause, the menopause transition or postmenopause based on healthcare professional (HCP) communication or (2) aged 45–54 years, regardless of diagnosis. To achieve the final analytic sample of 1,500 women, YouGov screened 3,592 women aged 35 and older across 4 target subgroups and matched respondents down to the final weighted sample.
Participants completed a questionnaire assessing menopause-related symptoms, treatment use, and access to care. Standard YouGov quality control procedures were used to exclude incomplete or low-quality responses. The study was reviewed and deemed exempt by the University of Southern California Institutional Review Board on February 20, 2025 (UP-25-00109). Informed consent was obtained from all participants prior to survey completion.
Survey measures
Survey items were designed by the authors to examine treatment use, barriers to care, and social and structural influences on menopause management. The instrument included five domains: (1) medication, HT, and supplement use and discontinuation; (2) peer and social influences on treatment decisions; (3) health care access, satisfaction, and HCP engagement; (4) affordability and insurance coverage; and (5) symptom impact and support-seeking behaviors.
Most questions used multiple-choice response formats or 4-point Likert scales, with skip logic applied to tailor follow-up items. Open-ended questions allowed participants to elaborate on experiences and perceived challenges. A copy of the full survey instrument, including question wording and recruitment details, is provided in the Supplementary Data.
Study population and menopausal status assessment
Menopausal status was assessed via self-report of HCP communication using the following item: “Have you been told by a doctor or other healthcare professional that you are in menopause or the menopause transition (sometimes referred to as ‘perimenopause’)?” Response options included “Yes, perimenopause,” “Yes, menopause,” or “No.” Women answering “No” remained eligible if aged 45–54 years. Participants were also instructed that if they had not been told by an HCP that they were in perimenopause or menopause, they should answer subsequent questions based on their experience with the transition to menopause and symptoms they believed were related to perimenopause or menopause. Accordingly, menopausal stage in this study reflects participant self-report (based on clinician communication and/or symptom attribution) rather than standardized biological staging (e.g., STRAW+ 10), menstrual history (e.g., 12 months of amenorrhea), or hormonal confirmation. The mean age of the full sample was 54.2 years (standard deviation 9.3).
Demographic and health characteristics were provided by YouGov and summarized using univariate descriptive statistics. Variables included age, race and ethnicity, geographic region, education, income, insurance type, and self-rated health.
Data analysis
Survey data were collected, stored, and managed by YouGov, a global public opinion and data company with a proprietary survey panel of millions of U.S. residents. 12 The sample was weighted by age, race/ethnicity, political affiliation, educational attainment, and region to align with U.S. population benchmarks. De-identified, weighted data were then provided to investigators for analysis. All analyses were performed in R Version 4.4.1.
Descriptive statistics were used to summarize participant characteristics. Bivariate analysis compared participants who reported using HT with those who did not, using two-sided p-values for group comparisons. Multivariable logistic regression models were used to identify predictors of HT use and predictors of peer HT use, with results reported as odds ratios and 95% confidence intervals.
Results
Participant characteristics
Participant characteristics are shown in Table 1. Among 1,500 participants, 53% reported receiving a menopause diagnosis and 47% had not yet received a menopause diagnosis. Menopausal status reflected self-report of HCP communication (i.e., whether an HCP had told the respondent she was in menopause or the menopause transition/perimenopause), and respondents aged 45–54 could be included regardless of reported menopausal status. Respondents who had not been told they were in perimenopause/menopause were instructed to answer subsequent questions based on symptoms they attributed to the menopause transition. The sample was 63.7% non-Hispanic White, with 15.1% identifying as Hispanic. Nearly one-third were covered by Medicaid or Indian Health Service (IHS), and approximately one-third by employer-sponsored insurance. One in six participants reported annual household income ≥$100,000, whereas 22% reported <$20,000. Overall, self-rated health was good to excellent in 75% of respondents.
Sample Characteristics of Survey Respondents
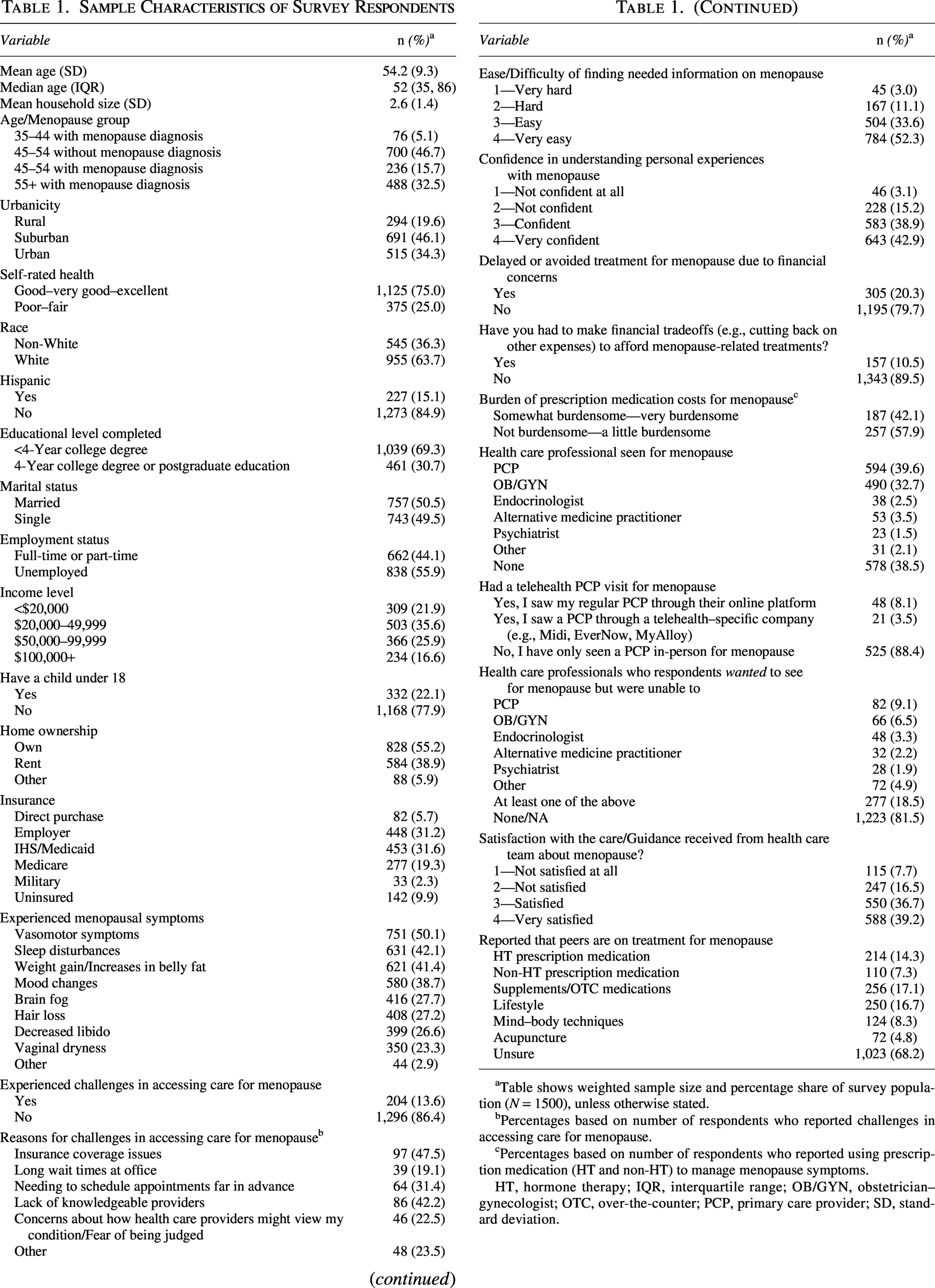
Table shows weighted sample size and percentage share of survey population (N = 1500), unless otherwise stated.
Percentages based on number of respondents who reported challenges in accessing care for menopause.
Percentages based on number of respondents who reported using prescription medication (HT and non-HT) to manage menopause symptoms.
HT, hormone therapy; IQR, interquartile range; OB/GYN, obstetrician–gynecologist; OTC, over-the-counter; PCP, primary care provider; SD, standard deviation.
Symptom burden
Menopausal symptoms were widespread across the cohort (Table 1). VMS were reported by 50% (n = 751), sleep disturbance by 42% (n = 631), weight gain by 41% (n = 621), and mood changes by 39% (n = 580). “Brain fog” was reported by 28% (n = 416), decreased libido and hair loss by 27% each, and vaginal dryness by 23%. Among the respondents who reported VMS, only 78 were current HT users, representing ∼10% of those with the primary indication for therapy. Notably, symptom burden remained high even among respondents who did not report being told they were in menopause or the menopausal transition, consistent with the inclusion of respondents reporting symptoms attributed to the menopause transition. Despite the high prevalence of symptoms, use of HT remained low, supporting further analysis of treatment patterns and correlates.
HT use and correlates
Overall, 7.2% of respondents reported current HT use to manage menopausal or perimenopausal symptoms (Table 2). Among users, oral estrogen, topical estrogen (i.e., transdermal formulations such as patches and creams), and progesterone were the most reported formulations (approximately 31% each), followed by vaginal estrogen and combination therapy, with lower use of testosterone and other formulations (Table 2). The similar rates of estrogen and progesterone use may reflect standard clinical practice, whereby women with an intact uterus who are prescribed estrogen are also prescribed progesterone for endometrial protection. Because respondents could select all applicable formulations, categories are not mutually exclusive, and percentages do not sum to 100%. In this survey, “combination therapy” referred to a single combined estrogen–progesterone product, as distinct from estrogen and progesterone selected as separate formulations. HT users (n = 108) were predominantly White (76%) and had significantly higher self-rated health, educational attainment, income, and home ownership and were more likely to be married compared with nonusers (Table 3).
Hormone Therapy and Non-HT/Supplement Use
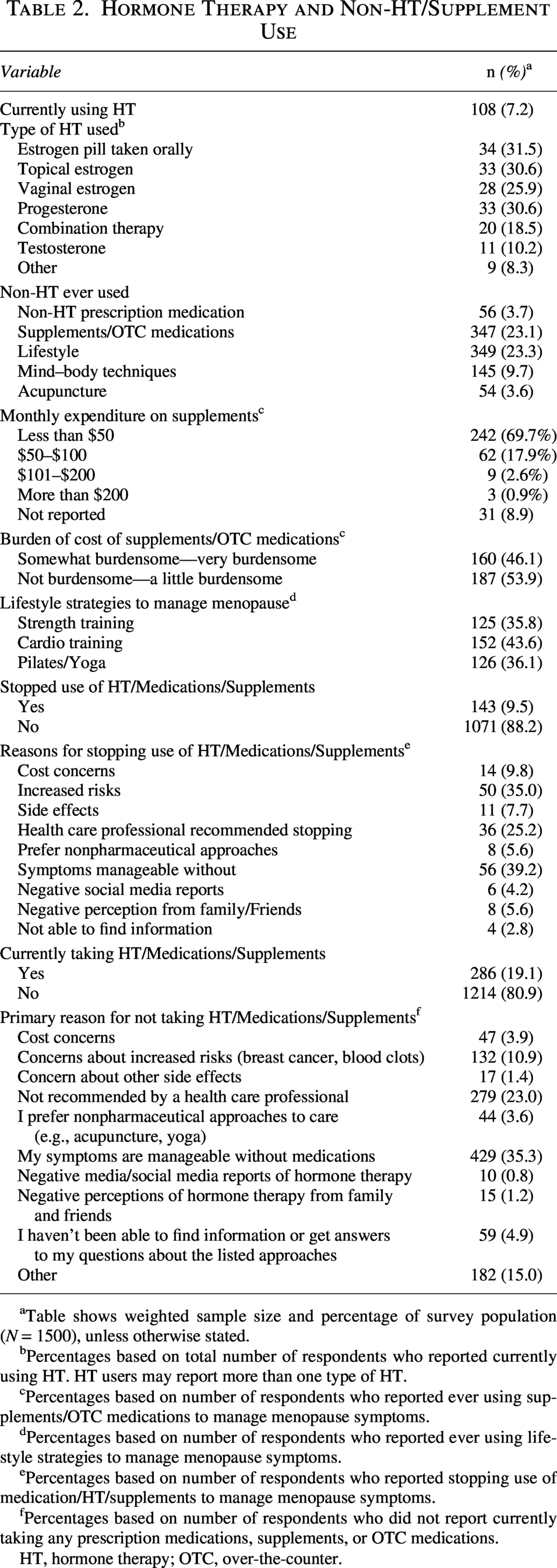
Table shows weighted sample size and percentage of survey population (N = 1500), unless otherwise stated.
Percentages based on total number of respondents who reported currently using HT. HT users may report more than one type of HT.
Percentages based on number of respondents who reported ever using supplements/OTC medications to manage menopause symptoms.
Percentages based on number of respondents who reported ever using lifestyle strategies to manage menopause symptoms.
Percentages based on number of respondents who reported stopping use of medication/HT/supplements to manage menopause symptoms.
Percentages based on number of respondents who did not report currently taking any prescription medications, supplements, or OTC medications.
HT, hormone therapy; OTC, over-the-counter.
Hormone Therapy Use and Correlates Among Perimenopausal and Menopausal Women
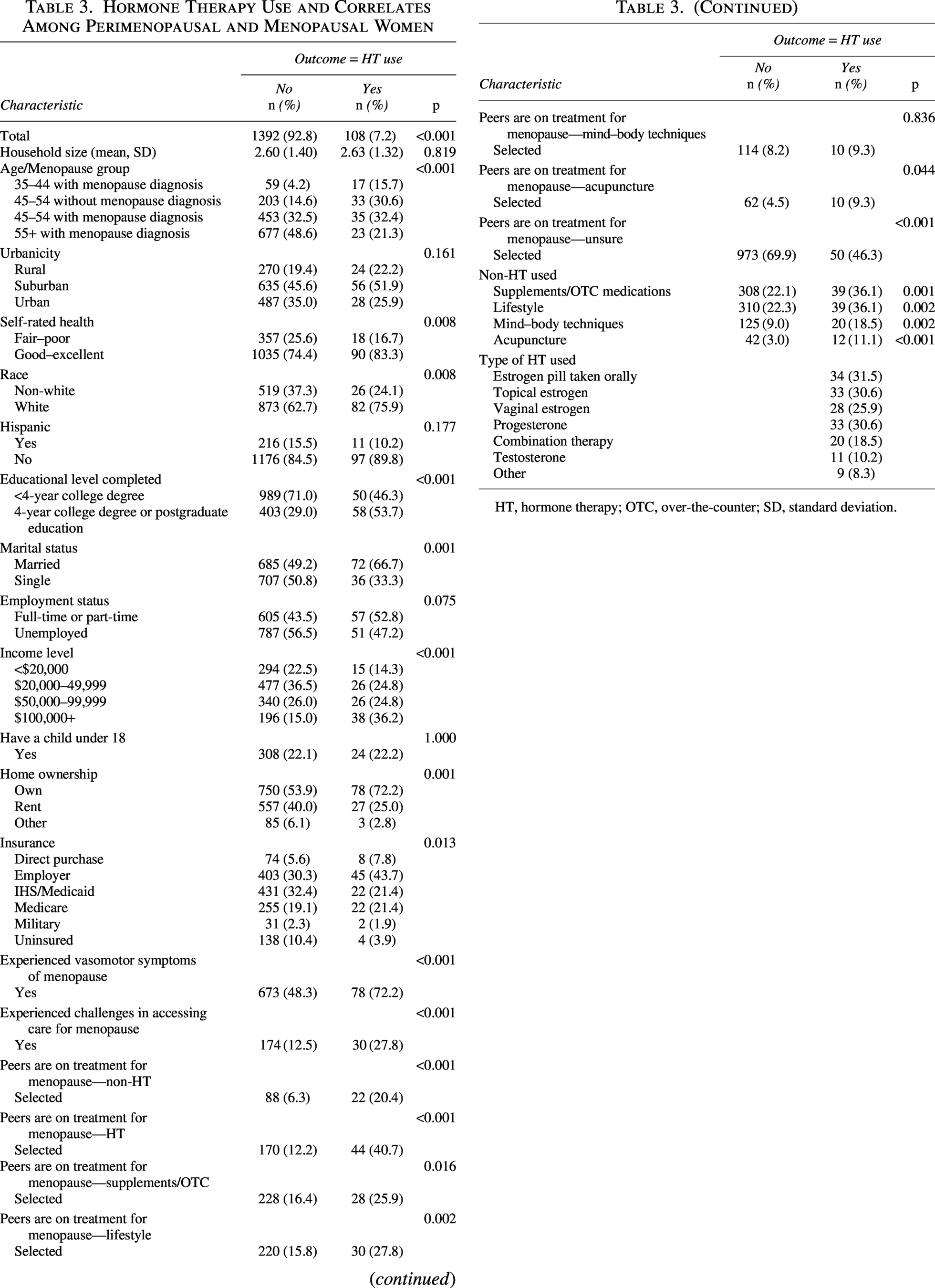
HT, hormone therapy; OTC, over-the-counter; SD, standard deviation.
Nonhormone and supplement use
Nonprescription remedies were more common than prescription therapies (Table 2). Overall, 23.1% of respondents reported using over-the-counter supplements for menopause symptoms, whereas 3.7% used nonhormone prescription medications such as selective serotonin reuptake inhibitors (SSRIs) or gabapentin.
Among supplement users, 18% reported spending $50–$100 monthly and 4% spent more than $100, with 46% reporting supplements as at least somewhat difficult to afford. Concurrent use was common, with 36% of HT users also reporting supplement use (Table 3).
Lifestyle strategies
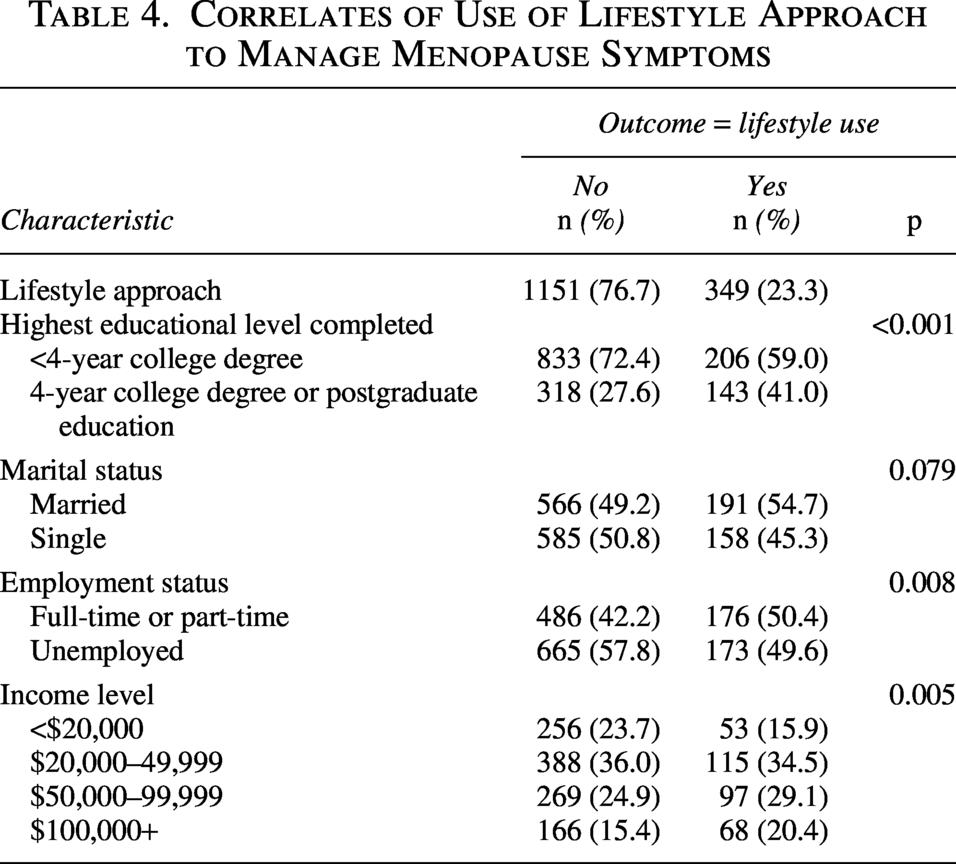
Lifestyle strategies were frequently used for menopause symptom management (Table 2). Overall, 23% of respondents (n = 349) reported using at least one lifestyle-based approach. The most reported activities were cardiovascular exercise (44%), strength training (36%), and yoga and/or Pilates (36%).
Use of lifestyle strategies was associated with higher education, employment, and higher income (Table 4).
Correlates of Use of Lifestyle Approach to Manage Menopause Symptoms
Structural and financial barriers to care
Most participants (86%, n = 1,296) reported no difficulty accessing menopause-related care; however, 20% delayed or avoided care because of financial concerns and 10.5% reported cutting back on essential expenses to afford treatment (Table 1). Prescription costs were described as burdensome for 42% of respondents who reported taking prescription medication (HT or non-HT) to treat menopause.
Access to information was generally high: 1,288 participants found menopause-related information easy or very easy to locate, and 1,266 felt confident in understanding their symptoms (Table 1). However, 204 participants reported difficulty obtaining menopause-specific care, most commonly due to insurance limitations, appointment availability, or lack of knowledgeable HCPs. Overall, 1,138 respondents were satisfied or very satisfied with the care received.
HT users were more likely than nonusers to report barriers to accessing treatment (p < 0.001) despite being more likely to have employer-based insurance rather than Medicaid or IHS coverage (Table 3). Primary care providers (40%) and obstetrician–gynecologists (OB/GYNs; 33%) were the most consulted HCPs for menopause-related concerns, whereas the use of virtual primary care was less common (12%) (Table 1).
Reasons for nonuse and discontinuation
Participants reported reasons for nonuse or discontinuation of menopause therapies (Table 2). Among respondents not using any therapy, the most common reasons for nonuse were that symptoms were manageable without medication (n = 429) and that treatment was not recommended by a HCP (n = 279). Other reasons included concerns about health risks such as breast cancer or blood clots (n = 132), difficulty obtaining information or answers (n = 59), and cost (n = 47). Fewer participants cited a preference for nonpharmacologic approaches (n = 44) or concerns about other side effects (n = 17). Social or media influence was infrequently reported. Cost was cited less frequently than lack of an HCP recommendation as a reason for nonuse.
One hundred forty-three respondents reported previously using any menopause therapy (Table 2). The most common reasons for discontinuation were symptoms being manageable without medication (39%) and perceived health risks (35%). In open-text responses, concern about cancer risk was cited most frequently.
Peer and social influences
Peer and social context strongly influence treatment behavior (Table 3). Women using HT were significantly more likely to report peer use of HT (p < 0.001), non-HT medications (p < 0.001), and lifestyle strategies such as exercise or yoga (p = 0.002). Peer use of supplements (p = 0.016) and acupuncture (p = 0.044) was also associated with HT use.
Peer use variables reflect participant report of whether peers used these therapies, rather than peer-reported behaviors.
Predictors of HT use
In multivariable logistic regression models, higher income, higher education, VMS, and peer influence emerged as predictors of HT use (Table 5). We sequentially specified logistic regression models to examine the independent effects of income, education, and peer medication use (Models 1–3), then assessed their joint associations (Model 4), and finally added VMS as a clinically relevant covariate to obtain the fully adjusted model (Model 5).
Multivariable Logistic Regression Model for Predictors of Hormone Therapy Use
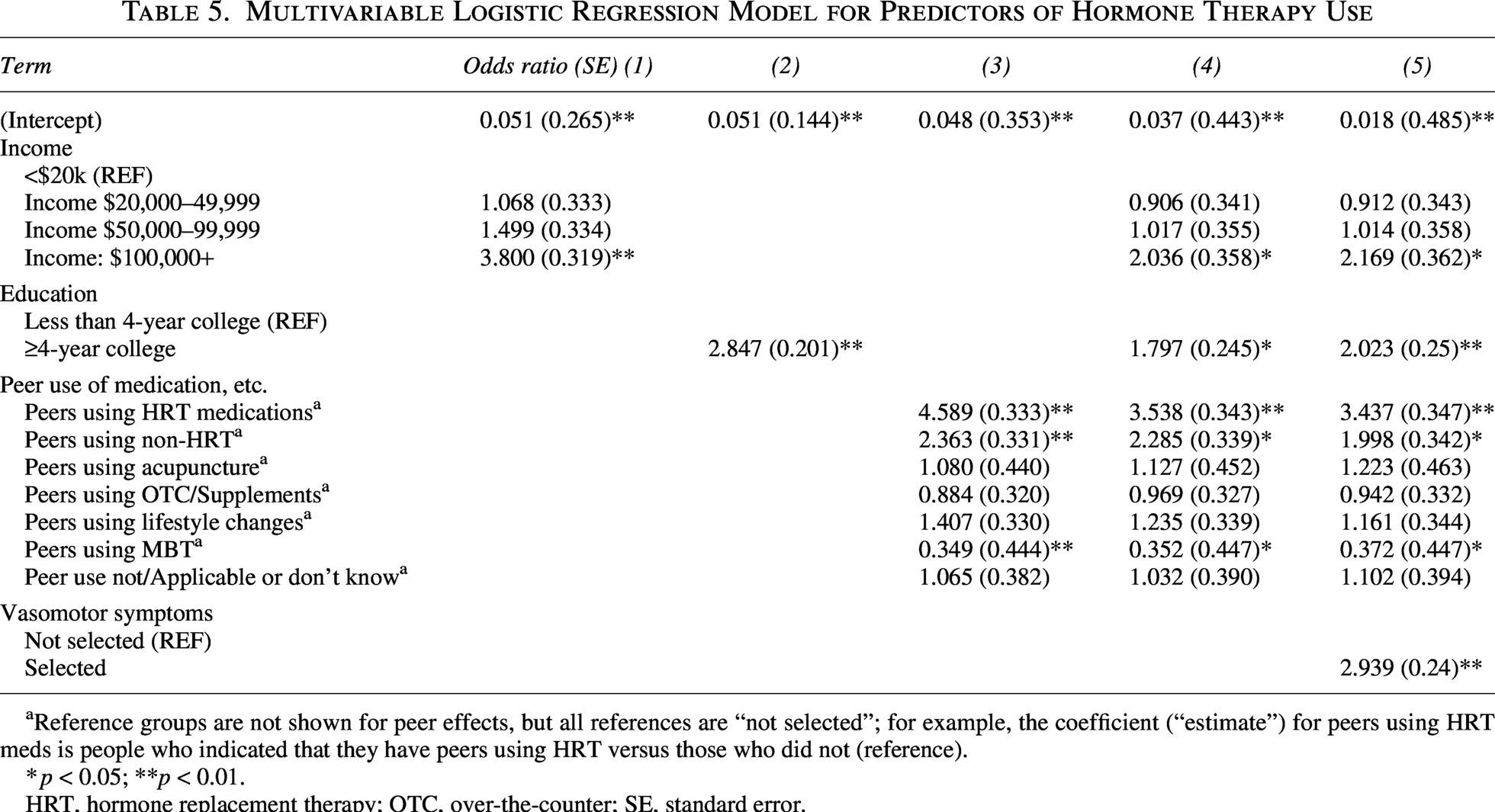
Reference groups are not shown for peer effects, but all references are “not selected”; for example, the coefficient (“estimate”) for peers using HRT meds is people who indicated that they have peers using HRT versus those who did not (reference).
*p < 0.05; **p < 0.01.
HRT, hormone replacement therapy; OTC, over-the-counter; SE, standard error.
Compared with respondents earning <$20,000 annually, those with incomes above $100,000 had 2.2-fold higher odds of HT use, all else equal. Similarly, women with at least a 4-year college degree had approximately twice the odds of HT use, and women reporting VMS had 2.9-fold higher odds, all else equal.
Peer influence was particularly strong: regardless of income, education, or presence of VMS, women whose peers used HT were 3.4 times more likely to use HT themselves, whereas peer use of non-HT medications was associated with a twofold increase in HT use. In contrast, peer use of mind–body approaches (e.g., cognitive behavioral therapy, mindfulness, and hypnosis) was associated with a 63% lower likelihood of HT use (Table 5).
Discussion
Major findings
This national survey highlights the persistent gap between symptom burden and treatment uptake for menopause-related symptoms. Despite half of respondents reporting VMS, only a small minority used HT, mirroring national estimates. 8 Education, income, and peer influence independently predicted use, underscoring that treatment decisions are shaped not only by symptoms but also by broader social and economic contexts. 13 Because the survey included respondents across the menopause transition spectrum, including women without HCP-labeled perimenopause or menopause who responded based on symptoms they attributed to the transition, these findings reflect real-world treatment patterns among midlife women experiencing menopause-related symptoms. Overall, these findings reveal a complex interplay between access, belief, and community influence in determining whether women pursue evidence-based therapy.
Socioeconomic and structural barriers to HT access
Socioeconomic status was a major determinant of HT use. Women with higher education and income levels were substantially more likely to use therapy, consistent with longstanding disparities in access to preventive and reproductive health care. 14 Multiple studies show that higher educational attainment and income are consistently associated with greater use of preventive and reproductive health services among women. 15 Although most respondents reported little difficulty obtaining treatment, a notable minority delayed or avoided care due to cost. Many described prescription expenses as burdensome, and some reported cutting back on essentials to afford treatment. Women with employer-based insurance were more likely to use HT than those relying on Medicaid or his coverage, suggesting that access remains tied to employment and insurance design. These findings align with national evidence that financial strain, limited insurance coverage, and system-level fragmentation continue to constrain equitable access to menopause care.16,17 However, not all structural barriers to HT access were equally prominent in this population. Although income and insurance type independently predicted HT use, cost was among the least frequently cited reasons for nonuse, whereas lack of an HCP recommendation was reported far more commonly, suggesting that many women may have adequate financial access to HT but are never offered it in the clinical encounter. For many symptomatic women, the primary barrier appears to be a failure of clinical identification and counseling rather than affordability alone, pointing to HCP education and counseling as critical targets for closing this gap.
Sociocultural and peer influences
Peer networks played a strong and independent role in treatment decisions. Women whose friends used HT were several times more likely to do so themselves, whereas those whose peers practiced mind–body approaches were far less likely to initiate therapy. Peer use of nonhormonal prescription medication was also associated with HT uptake. These findings underscore that menopause care is not only clinical but also cultural, shaped by informal communication, social norms, and perceptions of what constitutes safe, effective, or acceptable care. Although direct research on peer influence in menopause is limited, broader literature shows that social context, including the attitudes of family and friends, strongly shapes decisions about medical treatment. 13 A systematic review including 21 studies (n = 40,226) identified negative perceptions of HT within social circles as one of the most frequent barriers to acceptance. 18
The interplay between social and cultural capital provides a useful framework for interpreting these findings.19–21 Social networks can both amplify and deter evidence-based behaviors, reflecting shared norms tied to socioeconomic position and cultural values. Comparable contagion effects are well documented in lifestyle behaviors such as exercise, breastfeeding, and diet,22–24 suggesting that similar mechanisms may operate in menopause.
Despite prior research showing that negative peer perceptions can deter treatment, few nonusers in our study mentioned negative perceptions of HT from family or friends as a reason for nonuse. Sociological research on behavior adoption suggests that individuals internalize influence within their social “habitus”25,26 without necessarily recognizing its role in shaping behavior. Peers strongly shape behaviors that are visible, reinforced, and shared, rather than deterring from the multitude of unexpressed alternatives. A parallel example is vaccine hesitancy, which is often amplified through online platforms rather than in-person peer groups. 27 Our survey likely captures peer influences that operate implicitly; respondents’ perceptions that peers benefit from HT or hearing about their experiences may increase perceived acceptability even when respondents do not consciously attribute their choices to peer influence. Open-ended responses, by contrast, reflect reasons participants can explicitly articulate. In this context, positive peer examples may implicitly encourage HT uptake, whereas negative or cautious attitudes may exert a quieter influence on perceptions and readiness to initiate treatment.28–30
Socioeconomic position and associated cultural capital further shape these dynamics, 31 as shared resources, social norms, and access to information within more affluent and educated networks may facilitate both treatment uptake and participation in wellness practices, as seen in studies of breastfeeding and other health behaviors.32,33 These same attributes may also enable access to wellness practices that remain financially out of reach for many women. 34
From an implementation standpoint, these insights highlight opportunities to design peer-based and community-level interventions that normalize help-seeking and promote evidence-based HT use. Group education programs can enhance knowledge, symptom management, and confidence among midlife women, 35 whereas emerging evidence suggests that digital communities can shape attitudes and adherence in both positive and negative ways. 36 Integrating peer-informed communication strategies within clinical and public health frameworks may strengthen patient engagement and extend the reach of clinician-delivered menopause interventions. 37
Perceived risk and persistent hesitancy toward HT
In this national survey, concern about breast cancer was among the more frequently cited reasons for avoiding or discontinuing HT. More than one-third of former users stopped treatment due to perceived cancer risk, and similar fears discouraged initiation among many others. These patterns illustrate the enduring influence of the early WHI findings, which, despite later reanalysis and updated guidance, continue to shape perceptions among both patients and clinicians.38,39 While risk varies by formulation, route, and duration, the nuance of this evidence often fails to reach patients in accessible language.40,41 Persistent anxiety about harm reflects a broader communication gap rather than scientific uncertainty, emphasizing the need for risk framing that is contextual, personalized, and culturally sensitive.
Nonhormone and self-directed therapies
Despite broad access to conventional care, over-the-counter supplements were the most used therapies in the sample, exceeding the use of prescription medications. International surveys similarly show that nearly half of midlife women use complementary or alternative medicine for menopause-related symptoms, 42 most often guided by perceptions of safety or naturalness rather than evidence. 43
Supplement use also carried financial implications. Many women reported difficulty affording these products, and a substantial minority spent significant monthly amounts despite limited or absent evidence of efficacy. 44 No dietary supplements are currently recommended by The Menopause Society for symptom relief. 45 Nonhormonal prescription medications such as SSRIs, SNRIs, gabapentin, and fezolinetant were used infrequently, consistent with prior reports of limited awareness and counseling. 46
Lifestyle modification was also common, with many women citing exercise, yoga, or other wellness strategies for symptom management. Although physical activity is strongly recommended for cardiometabolic health, evidence from randomized controlled trials shows limited benefit for VMS compared with estrogen therapy. 47 These preferences likely reflect broader cultural trends favoring behavioral and holistic approaches over pharmacologic ones. 48 Collectively, these findings suggest that preference and perception, not access alone, shape treatment choices.
Information, counseling, and future directions in menopause care
In our study, primary care physicians were the most frequently relied upon HCPs for menopause-related concerns, followed by OB/GYNs, whereas virtual care remained uncommon. Despite high symptom burden, most participants reported satisfaction with the information they received and confidence in understanding their experiences. However, access alone does not fully explain the low uptake of HT, as only 7.2% reported current HT use.
The pattern of broad access to and reliance on primary care, combined with low HT uptake, points to persistent gaps in clinician training and counseling. Although major guidelines endorse HT as a safe and effective option for many symptomatic women in the menopause transition and early menopause (e.g., <60 years or within 10 years of menopause onset), fewer than 5% of U.S. women currently use it. 49 Surveys of family medicine, internal medicine, and gynecology HCPs consistently report limited formal education in menopause management and uncertainty around prescribing. 50 International studies similarly describe brief or incomplete counseling and limited awareness of available therapies in primary care encounters. 51
Addressing these gaps requires stronger emphasis on evidence-based decision support within primary care, incorporating structured menopause counseling into midlife visits, using shared decision-making frameworks, and consulting current guidance from The Menopause Society, The Endocrine Society, and other professional bodies.2,5,7 Directly addressing risk perceptions may help counter misinformation and improve informed use of HT among eligible women.52,53
Limitations
This study has several limitations. Menopausal status was assessed through self-report, including whether respondents recalled being told by an HCP that they were in the menopause transition, perimenopause, or menopause, without medical record verification, standardized staging criteria (e.g., STRAW+ 10), menstrual history (e.g., 12 months amenorrhea), or hormonal confirmation. However, prior evidence supports the clinical validity of self-assessment and symptom-based classification for identifying the menopause transition when considered alongside age and VMS. 3 Respondents who had not been told they were in perimenopause or menopause were instructed to answer subsequent questions based on symptoms they believed were related to the transition to menopause; therefore, the cohort includes women across the menopause transition spectrum, particularly within the 45–54 age group. The sample was predominantly White and drawn largely from urban and suburban populations, limiting generalizability to more diverse or rural groups. Approximately 10% of respondents were uninsured, underrepresenting women with the greatest structural barriers to care.
When participants were asked about reasons for treatment nonuse or discontinuation, the question referred broadly to any menopause-related therapy. As a result, we were unable to distinguish between HT, nonhormonal prescription treatments, and supplements. However, because many open-ended responses cited concerns about breast cancer or clotting risk, some respondents may have interpreted this question as referring specifically to HT; importantly, HT may also be initiated during the menopausal transition for symptom management and is not limited to postmenopausal women.
As with all self-reported survey data, responses may be subject to recall or reporting bias; nonetheless, the national scope and detailed inclusion of structural and sociocultural factors provide valuable insight into the influences shaping menopause treatment decisions in the United States.
Conclusion
This national survey found that women with higher income and education were significantly more likely to use HT, and that peer influence was among the strongest independent predictors of uptake. These findings highlight the intertwined roles of social position, cultural context, and interpersonal influence in shaping decisions about menopause treatment. By identifying modifiable determinants of help-seeking, communication, and access, this study points to specific targets for intervention: strengthening HCP education, integrating peer-informed communication models, and addressing financial barriers, informational gaps, and the counseling deficits that prevent many symptomatic women from ever being offered evidence-based therapy. As one of the first U.S. studies to quantify peer effects on HT use, this work emphasizes the need for public health and clinical strategies that leverage social networks, including social media platforms capable of reaching diverse socioeconomic and demographic groups, to promote equitable, evidence-based menopause care.
Authors’ Contributions
All authors contributed to conceptualization, formal analysis, and writing—review and editing and approved the final article.
Supplemental Material
sj-docx-1-jwh-10.1177_15409996261465480 — Supplemental material for Peer, Social, and Structural Influences on Hormone Therapy Use in Menopause: A U.S. Population Survey
Supplemental material, sj-docx-1-jwh-10.1177_15409996261465480 for Peer, Social, and Structural Influences on Hormone Therapy Use in Menopause: A U.S. Population Survey by Sharon Orrange, Alexandra Guttentag, Amanda Nguyen, and Elizabeth Currid-Halkett
Footnotes
Acknowledgments
The authors gratefully acknowledge the contributions of Maeve Humphrey and Tess Humphrey, who provided substantial support through their review and synthesis of the medical literature that informed this work.
Author Disclosure Statement
A.G. and A.N. are employees of GoodRx. The authors declare no conflicts of interest.
Funding Information
No financial support was required for this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.