
Abstract
Mental health problems among youth in the juvenile justice system are of particular concern given their high prevalence rate. The current study applies attribution theory and focal concerns to examine how mental health problems influence the judicial decision to commit youth to confinement. Furthermore, the study examines whether the effect of mental health problems is conditioned by race and ethnicity, hypothesizing that minorities with mental health problems will be treated more severely than Whites with mental health problems. Using administrative court records from Maricopa County, AZ (n = 5,501), findings reveal that mental health problems increased the likelihood of confinement, and this effect was moderated by race. Implications for theory and policy are discussed.
Introduction
The juvenile justice system is often faced with the challenge of responding to youth who suffer from mental health problems. Studies have demonstrated that a large proportion of youth processed through the juvenile justice system suffer from mental health problems (Fazel, Doll, & Langstrom, 2008; Garland et al., 2001; Shufelt & Cocozza, 2006; Teplin, Abram, McClelland, Dulcan, & Mericle, 2002; Teplin et al., 2006; Vincent, Grisso, Terry, & Banks, 2008; Wasserman, McReynolds, Lucas, Fisher, & Santos, 2002). The high rates of mental health disorders among youth in the juvenile justice system, compared to the general public, suggest detention centers and correctional facilities for youth are serving as surrogate mental health hospitals (Cocozza & Skowyra, 2000; also see Wilson, 2013). Furthermore, certain individuals are more likely to have unmet mental health needs and have their needs met through the juvenile justice system, rather than the mental health system (Cohen et al., 1990; Lyons, Baerger, Quigley, Joel, & Griffin, 2001; Rawal, Romansky, Jenuwine, & Lyons, 2004; Rosenblatt, Rosenblatt, & Biggs, 2000; Stoep, Evans, & Taub, 1997; Thomas & Stubbe, 1996).
An extensive amount of research has examined legal and extralegal factors, particularly racial disparities, in decisions to process youth in the juvenile justice system, but little research has explored the role of mental health problems (Cappon & Vander Laenen, 2013; Cauffman et al., 2007; Leiber, Johnson, Fox, & Lacks, 2007). More specifically, research has found minorities are treated more severely in the juvenile justice decision-making process leading to a disproportionate number of minorities in the system (Kempf-Leonard, 2007; Piquero, 2008). Minorities with mental health disorders also tend to have higher rates of unmet needs (Rawal et al., 2004); therefore, it is important to understand how the juvenile justice system responds to these youth.
We rely on juvenile court data from an urban jurisdiction in Arizona to examine the role of mental health problems in the disposition outcome to commit youth to a juvenile correctional facility and the extent to which the effect of mental health problems differs by the race or ethnicity. Attribution theory (Albonetti, 1991) and the focal concerns perspective (Steffensmeier, Ulmer, & Kramer, 1998) provide a framework to assess the relevancy of factors, such as race/ethnicity or mental health, in the processing of offenders and court outcomes. Although the current study does not provide a direct test of these theories, attribution theory and focal concerns provide a framework to understand decision making in the justice system.
The disposition outcome to commit youth to a correctional institution versus community supervision is examined because it has implications for the juvenile justice system’s obligation to provide treatment and the extent to which the juvenile justice system ensures services are completed (Grisso, 2004). Specifically, the juvenile justice system is more responsible for providing treatment services to a youth in correctional confinement and is better able to monitor the progress of the treatment. Finally, youth with mental health disorders who are committed to correctional confinement may be perceived as more dangerous than those who receive community supervision.
Background
Youth and Mental Health Problems
A substantial body of research has assessed the prevalence of mental health disorders among youth in the juvenile justice system, particularly detention. Research has generally found consistent estimates that 65–70% of youth in the juvenile justice system have at least one mental health disorder (Fazel et al., 2008; Garland et al., 2001; Shufelt & Cocozza, 2006; Teplin et al., 2002, 2006; Vincent et al., 2008; Wasserman et al., 2002). This can be compared to a prevalence rate of 20% for the general public of adolescents with mental health problems (Kazdin, 2000). In a more recent review, Shufelt and Cocozza (2006) found that 70.4% of youth in 29 programs met criteria for at least one mental health disorder and 79% of those had two or more diagnoses. In addition, roughly one in five youth in the juvenile justice system suffer from a serious mental health disorder, and the rate of mental health disorders among youth remains about 60% even after conduct disorder is removed of prevalence rates (Cocozza & Skowyra, 2000).
In regard to differences across demographic groups, females in the juvenile justice system tend to have higher rates of mental health disorders (Shufelt & Cocozza, 2006; Teplin et al., 2002; Vincent et al., 2008; Wasserman, McReynolds, Ko, Katz, & Carpenter, 2005), and rates of mental health disorders tend to be higher among White juveniles (Teplin et al., 2002). Few research studies have been designed to compare rates of mental health disorders across racial/ethnic groups in the juvenile justice system, especially across different types of disorders. Teplin, Abram, McClelland, Dulcan, and Mericle (2002) found that Latinos in a single detention center had higher rates of depressive and anxiety disorders than Whites and African Americans. Racial and the ethnic differences in mental health disorders may have implications for assessment of treatment need and disposition outcomes because of lack of knowledge regarding diagnoses and treatment among minority populations.
Other research has found a significant overlap between the mental health system and the juvenile justice system, with involvement in one system increasing the risk for involvement in the other (Evens & Stoep, 1997; Rosenblatt et al., 2000; Stoep et al., 1997; Thomas & Stubbe, 1996; Yeh, McCabe, Hough, Dupuis, & Hazen, 2003). That is, youth in the mental health system are more likely to have arrests and have higher adjudication rates than youth in the general population (Evens & Stoep, 1997; Goodkind, Shook, Kim, Pohlig, & Herring, 2013; Schwalbe, Hatcher, & Maschi, 2009; Stoep et al., 1997). Lyons, Baerger, Quigley, Joel, and Griffin (2001) compared mental health needs across three samples of youth, those on probation (community setting), those confined in a correctional institution, and those referred to residential treatment. These authors found that youth with behavioral problems were more likely to be incarcerated, and youth in the institutional settings had greater mental health needs than youth in the community. Additionally, youth with prior mental health treatment or substance abuse treatment, poor caregiver supervision, a greater need for medical care, and who posed a danger to themselves or others were more likely to be incarcerated (Lyons et al., 2001).
Rosenblatt, Rosenblatt, and Biggs (2000) also found that those in the juvenile justice system tend to suffer from more severe disorders, with higher rates of conduct disorders, greater externalizing problems, and more functional impairment as a result of mental health problems. In general, “it appears the courts consider youth with multiple and complex problems to be poor candidates for community placement, particularly when their caregivers do not seem to accept the gravity of their adolescents’ needs” (Lyons et al., 2001, p. 81). These studies, however, do not take into account the nature of the youth’s delinquent behavior and their prior involvement in the juvenile justice system. It may be that youth in the juvenile justice system have more serious offenses or an extensive record, therefore, it is important to control for these factors.
Campbell and Schmidt (2000) found that the youth’s criminal characteristics had the greatest influence on disposition decisions and that mental health factors had limited influence on court disposition outcomes. More specifically, judges followed clinician’s recommendation for youth’s disposition less than 70% of the time (Campbell & Schmidt, 2000). When controlling for legal factors, however, these authors did find that youth with more serious substance abuse disorders and those from negative family environments were more likely to receive custodial dispositions. Other studies have found that the presence of a mental health disorder or mental health report increased the likelihood of harsher dispositions, such as residential treatment or correctional confinement (Gebo, 2007; Kempf-Leonard & Sontheimner, 1995; Nairhos & Routh, 1992; O’Donnell & Lurigio, 2008; Rodriguez, 2003).
A more recent study by Schwalbe, Hatcher, and Maschi (2009) examined the influence of treatment needs and prior social service use on disposition outcomes, while controlling for other legal and extralegal variables. These authors found that those who had received prior social services were more likely to have more severe dispositions. These authors suggest that judges are less likely to place juveniles who have prior service use in community-based sanctions because they perceive the social services as unsuccessful in preventing delinquency (Schwalbe et al., 2009).
In general, this body of research suggests that youth with certain mental health problems are more likely to end up in the juvenile justice system and they tend to be treated more severely when processed through the system. Often mental health problems in youth go unrecognized and untreated until they come under the attention of the juvenile justice system. Unfortunately, despite high rates of prevalence of mental health problems among youth in the juvenile justice system, there is a small probability of receiving mental health placement (Herz, 2001). Given the small proportion of youth who receive services, understanding the factors that influence disposition outcomes can provide a foundation for future research to expand upon when considering how youth with mental health problems are processed in the juvenile justice system. Mental health problems and need for services are relevant extralegal factors for determining the most appropriate disposition for youth, but the effect of mental health status on decision to commit youth to correctional confinement may not be equal across groups.
Racial and Ethnic Differences
Little research has focused on mental health problems among minority youth in the juvenile justice system, but studies have found demographic differences between youth referred to the mental health system and youth processed through the juvenile justice system (Dalton, Evans, Cruise, Feinstein, & Kendrick, 2009; Herz, 2001; Lopez-Williams, Stoep, Kuro, & Stewart, 2006; Maschi, Hatcher, Schwalbe, & Rosato, 2008; Rogers, Pumariega, Atkins, & Cuffe, 2006; Rogers, Zima, Powell, & Pumariega, 2001). Cohen et al. (1990) found that African Americans with serious emotional disorders were more likely to end up in corrections than in a psychiatric hospital; however, Whites in correctional facilities scored much worse on the Child Behavior Checklist (see Achenbach & Edelbrock, 1983) compared to African Americans. Another study found that Whites, females, and younger youth were more likely to be involved in the mental health system than the criminal justice system (Thomas & Stubbe, 1996), whereas minorities tended to be disproportionately represented in the juvenile justice system compared to the mental health system. In addition, Stoep, Evans, and Taub (1997) found that African Americans had the highest rate of referrals to the criminal justice system regardless of involvement in the mental health system, whereas involvement in the mental health system increased the risk of criminal justice involvement for Whites, Latinos, and Native Americans. Finally, Lyons et al. (2001) also found that African Americans were more likely to be referred to corrections versus residential treatment. These findings would suggest that mental health problems have different effects on which system the youth comes into contact with depending on the race/ethnicity of the individual. Specifically, minorities with mental health problems appear to be adversely affected in regard to being placed in the juvenile justice system compared to Whites with mental health problems.
Race and ethnicity also have been found to influence the degree to which youth’s mental health needs are met with services (Golzari, Hunt, & Anoshiravani, 2006; Rawal et al., 2004; Rogers et al., 2001, 2006). Rawal, Romansky, Jenuwine, and Lyons (2004) assessed differences in mental health service needs and service use across racial/ethnic groups from a random sample of petitioned, adjudicated, and incarcerated juveniles. These authors found African Americans had the greatest need for services and that minorities, in general, had much lower rates of service use. Similar to African Americans, Latinos had little treatment use despite high rates of mental health problems, whereas White youth had much lower rates of mental health needs, but had the highest rate of service use. These findings suggest that minorities with mental health problems do not get diagnosed and receive treatment until they enter the juvenile justice system (Rawal et al., 2004). Differences in service use may be a result of lack of resources and access to services as well as differences in definitions of mental disorders and the appropriate response to such problems (Cauffman & Grisso, 2005). It appears that minorities with mental health problems may be a unique group of youth where needs are only going to be met through juvenile justice system involvement, and judges dispositional decisions may be influenced by factors, particularly unmet need and limited availability of services.
Theoretical Framework
In light of the work on mental health problems among youth and racial/ethnic disparities in the juvenile justice system, attribution theory (Albonetti, 1991; Bridges & Steen, 1998) and the focal concerns perspective (Spohn & Holleran, 2000; Steffensmeier et al., 1998) provide a useful theoretical framework to help understand judicial decision making for youth with mental health problems. These theoretical perspectives were primarily developed to understand racial/ethnic disparities in sentencing outcomes, but can be applied to other extralegal factors such as mental health problems. The primary argument of attribution theory is that individuals consider whether causes of behavior are due to internal/personal factors or external/environmental factors (Albonetti, 1991; Heider, 1958). Based on where the cause of behavior is attributed, the individual’s level of responsibility for the behavior differs. Attributions are used to explain reasons for youth engaging in delinquent behavior and judges use stereotypes associated with groups to assess an individual’s culpability in delinquent behavior (Bortner, 1982; Dannefar & Schutt, 1982; Emerson, 1969; Mears et al., 2014; Rodriguez, 2013). Furthermore, identifying the underlying “cause” of delinquent behavior can help determine the appropriate response to the problem (Rodriguez, Smith, & Zatz, 2009). Individuals where delinquency is attributed to internal causes, such as bad personality traits, are seen as more responsible for their actions justifying harsher treatment (Bridges & Steen, 1998).
Attributions and stereotypes also play an important role in the focal concerns perspective. Due to bounded rationality (see Albonetti, 1987, 1991) and attributions about causes of behavior, courtroom decision makers, particularly judges, use three focal concerns to assist sentencing decisions—blameworthiness, dangerousness of the offender or threat to public safety, and practical constraints (Steffensmeier et al., 1998). Blameworthiness and dangerousness are linked to attribution theory in that the cause of behavior can help determine the level of responsibility of an individual in delinquent behavior and the risk of future offending. Perceptions of blameworthiness and dangerousness often differ depending on stereotypes associated with specific social groups, which can help explain disparities across race, gender, and age (Spohn & Holleran, 2000; Steffensmeier et al., 1998). The last focal concern, practical constraints, also has been influenced by defendant characteristics, such as women and older defendants presenting more practical constraints due to dependent children left behind or health-care costs (Steffensmeier et al., 1998).
In regard to mental health problems, there may be two different causal mechanisms (internal and external attributes) that may increase the likelihood of a youth being committed to juvenile commitment. First of all, research on perceptions of mental illness has found that people attribute the causes of different mental illnesses to different sources, such as stressful life circumstances, chemical imbalance, or to bad character or “the way a person was raised” (Link, Phelan, Bresnahan, Stueve, & Pescosolido, 1999, p. 1330). Although it has not been empirically examined, there is reason to suggest that where people attribute the cause of mental illness and its roles in delinquency may influence how it is responded to by the juvenile justice system.
Similar to statuses like race, age, gender, and unemployment, mental illness carries stereotypes that can influence judges’ focal concerns and their perceptions of blameworthiness, dangerousness, and practical constraints. Historically, persons with mental illness are viewed as “dangerous, dirty, unpredictable, and worthless” (Nunnally, 1961, p. 51). Even with more knowledge today about mental illness, those with mental illnesses are still stigmatized and discriminated against (Corrigan et al., 2003; Crisp, Gelder, Rix, Meltzer, & Rowlands, 2000; Phelan, Link, Stueve, & Pescosolido, 2000; Wahl, 2003). Additionally, behaviors and symptoms of mental illness are often viewed as voluntary and controllable (Weiner, Perry, & Magnusson, 1988), therefore, judges may attribute behavior to the individual, instead of to the mental health disorder, holding them responsible despite their mental health disorder. Pescosolido, Fettes, Martin, Monahan, and McLeod (2007) found that youth with mental health disorders, such as Attention Deficit Hyperactivity Disorder, and those labeled “mentally ill” were perceived as more dangerous and at an increased potential for violence. Respondents also felt that legal means were appropriate to force these youth into treatment (Pescosolido, Fettes, Martin, Monahan, & McLeod, 2007). If a judge associates mental illness with a youth having “bad character” and believes the youth is dangerous and cannot be rehabilitated, then juvenile confinement may be viewed as the most appropriate disposition. Furthermore, these perceptions of mental illness may vary by race and ethnicity. For example, an African American youth with a mental illness may be perceived as more dangerous than a White youth with a mental illness (see Bridges & Steen, 1998).
Delinquent behavior and mental illness attributed to adverse external environments may also be used to justify state intervention. External attributions, such as a disadvantaged neighborhood, may put youth at great risk for reoffending and may also suggest parents’ inability to provide needed levels of supervision (Rodriguez, 2013). As noted by Rodriguez (2013) “negative external attributes may not only be used as a mechanism through which assigned responsibility is reduced, but also as a basis for more severe treatment” (p. 6). In the case of mental health problems, if it is perceived that a youth is not receiving care for mental health problems in the community, especially for those who reach disposition, a judge may decide the youth should be placed in an institution to obtain necessary treatment (see Schawlbe et al., 2009).
African American youth are more likely to live in disadvantaged areas, which some may use as a marker to identify youth who need services and ensure that treatment is provided when a family is unable to meet this need (Bortner, 1982). These youth have higher risk for reoffending because of living in a disadvantaged community and because their unmet mental health needs. In fact, mental health problems and lack of treatment may be one of the mechanisms through which disadvantage affects the disposition outcome found in the study by Rodriguez (2013). In contrast, some may perceive that White families are more capable of providing services because they are viewed as being from more affluent communities where there are more resources for youth with mental health problems. As a result, court officials may recommend the youth remain in the community to receive treatment.
Based on this research, attribution theory and the focal concerns perspective provide the framework to suggest that mental health problems may have an adverse effect on how youth are processed in the juvenile justice system. Similar to some extralegal factors, such as age or school status, mental health problems are considered relevant in disposition outcomes (Fader, Harris, Jones, & Poulin, 2001). Mental health problems have implications for treatment and public safety, but they also allow the opportunity for unwarranted disparities to arise. Not all youth with mental health diagnoses need treatment (Grisso, 2004), but perceptions of mental health problems may influence judge’s disposition decisions regardless of the relevance of mental health and treatment need of the youth. Although mental health problems pose relevant issues for judges to consider, mental illness is also associated with negative stereotypes that lead to discrimination in individual’s lives (Corrigan et al., 2003). These stereotypes may be further influenced by the race or ethnicity of the youth leading to unwarranted disparities. As a result, mental health problems among minorities likely have further implications for how youth are treated in the juvenile justice system. The decision to confine a youth at disposition is the most serious outcome within the juvenile justice system, but it is also the state’s last effort to provide programs and treatment to rehabilitate a youth offender (Rodriguez, 2013).
The Current Study
The current study examined the relationship between mental health problems of youth and being committed to correctional confinement. Additionally, the role of race/ethnicity as a moderating variable on the effect of mental health problems was examined. Based on high rates of mental health problems in the juvenile justice system and the negative stereotypes associated with mental illness in general, we tested two hypotheses:
We hypothesized that youth with mental health problems would be more likely to be committed to correctional confinement versus community supervision, net of legal, and extralegal factors. The effect of mental health problems differed by the race/ethnicity of the youth. In particular, we hypothesized that African Americans and Latinos with mental health problems would receive a more severe disposition than their White counterparts.
The second hypothesis would suggest that mental health problems may be an aggravating factor for minorities, where African Americans and Latinos with mental health problems are viewed as more dangerous or in greater need of services than their White counterparts. In contrast, mental health problems for Whites may be a mitigating factor, where mental health problems are used to explain delinquent behavior and these individuals need treatment rather than punishment. The current study did not test these mechanisms directly, but findings can contribute to understanding juvenile justice decision making at the last stage in the process and the role of mental health problems.
Data and Method
Sample
Data used in the current analysis were drawn from all delinquent referrals made to Maricopa County Juvenile Probation Department, Arizona, between 2009 and 2011, which represented 21,284 referred youth. Only youth who were adjudicated and received a disposition from the juvenile court were included in the main analysis, resulting in a final sample of 5,501 cases for analysis. The Arizona juvenile court records provided information regarding the legal-case characteristics as well as individual demographic characteristics of the youth at each referral. The unit of analysis was the individual, so for individuals with multiple referrals during this time frame, the most recent referral was used. This ensured that information about delinquent referrals between 2009 and 2011 was captured as prior behavior for each youth. These data consisted of multiple files for each stage of the juvenile justice system that were merged to control for background characteristics and prior stages in the juvenile justice system, particularly preadjudication detention.
Table 1 presents the descriptive statistics of the sample of adjudicated youth. The descriptive statistics for the entire sample of referred youth can be found in Appendix A. Consistent with prior research, a majority of the sample was male, and the average age was 16.2 years. In regard to race and ethnicity, roughly 41% of the sample was White, 12.6% of the sample was African American, 42.1% was Latino, and 4.5% was some other racial or ethnic group. Approximately 24% of the sample was not enrolled in school. In regard to the legal variables, 61.8% of the youth had an obstruction of justice offense and 23.1% had a felony offense, 16.7% were detained prior to adjudication, and the mean number of prior referrals was 2.84. Finally, 6.5% of the sample was sentenced to correctional confinement for their disposition and of particular interest to the current study, 38.1% of the sample had a reported mental health problem.
Descriptive Statistics of Variables.
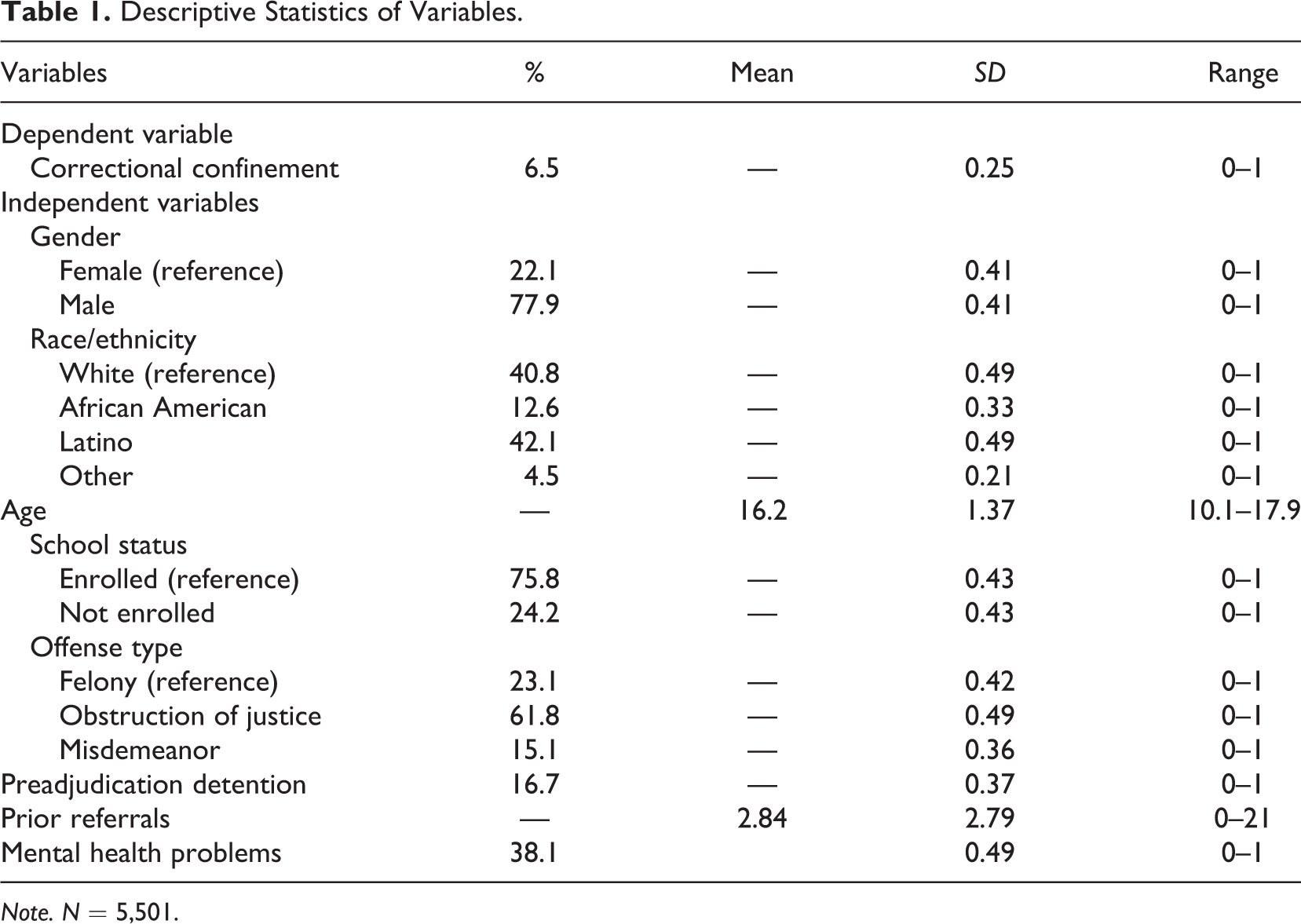
Note. N = 5,501.
Measures and Procedures
In the present study, the dependent variable of interest was juvenile correctional confinement (yes = 1, no = 0). This variable was measured by comparing youth sentenced to the Arizona Department of Juvenile Corrections (ADJC) to youth sentenced to community supervision. Research on disposition outcomes among youth has focused exclusively on out-of-home placement of youth in correctional confinement or leaving them in the community (Jordan, 2012; Rodriguez, 2013; Secret & Johnson, 1997). The operationalization of this variable in the current study is consistent with this body of research. As previously mentioned, descriptive statistics presented in Table 1 indicate that 6.5% of youth at disposition were committed to ADJC. The primary independent variable was mental health problems (yes = 1, no = 0). This variable was measured using a single item from the risk assessment tool administered for all youth upon referral to the juvenile justice system for a delinquent offense in Arizona. The Arizona Risk/Needs Assessment (ARNA) is an empirically validated actuarial risk assessment instrument used to predict risk of future offending and identify risks and needs of juveniles (see Krysik & LeCroy, 2002; Schwalbe, 2009). The ARNA is completed by probation officers following the youth’s initial intake assessment, which involves an interview with the youth and review of records. The item used in the current study asked whether the youth had behavioral problems/mental health issues. With the exception of 2 items on the instrument, a risk factor, including behavioral problems/mental health issues, should only be coded as “present” when there is “a clear statement by the juvenile, family member, or collateral contact supporting the risk factor” (Schwalbe, 2009, p. 208). The probation officer should not code the item as “present” based on their own reason to suspect the presence of the risk factor. Results from the risk assessment are available to judges during the court process and used to inform disposition hearings regarding youth placement and treatment decisions.
The other independent variable that was of particular interest for this study is the race or ethnicity of the youth. Race/ethnicity was measured using dummy variables for African Americans, Latinos, and other races with Whites as the reference category. Additional demographic variables that were controlled for were gender (0 = female, 1 = male) and age at referral, measured as a continuous variable. The school status, whether the youth was enrolled in school during the time of the referral, was also included as a control variable (0 = enrolled, 1 = not enrolled). 1
Prior record and offense severity are typically the strongest predictors of more severe punishments in the criminal justice system and often play an important role in how youth are processed. The type of offense was measured by including dummy variables for misdemeanor offenses and obstruction of justice with felony offenses as the omitted category. Prior record was measured using number of prior referrals. Lastly, preadjudication detention has been found to have an effect on subsequent decisions in the juvenile justice system, especially to sentence a youth to confinement (Jordan, 2012; Leiber, 2013; Leiber & Fox, 2005; Rodriguez, 2010). Therefore, whether the youth was detained in preadjudication detention was also controlled for in the analysis. Before proceeding with the analysis, listwise deletion was used to remove missing data, which did not exceed 10% for any of the measures included in the current study. Additionally, a number of collinearity diagnostics were performed to rule out multicollinearity among the independent variables.
Analytic Strategy
The analysis to test the proposed hypotheses involved two primary steps. First, a series of χ2 tests and independent samples t-tests were conducted to determine whether relationships between the independent variables and the disposition outcome were in the expected direction. The second stage of the analysis involved the use of multivariate regression models to predict the binary outcome—whether a youth is sentenced to juvenile corrections or community supervision. The direct effects of mental health problems and race/ethnicity were examined as well as the interactive effect between the two variables. One-tailed significant tests were used in the analysis given the directional hypotheses that mental health problems and race would increase the likelihood of correctional confinement.
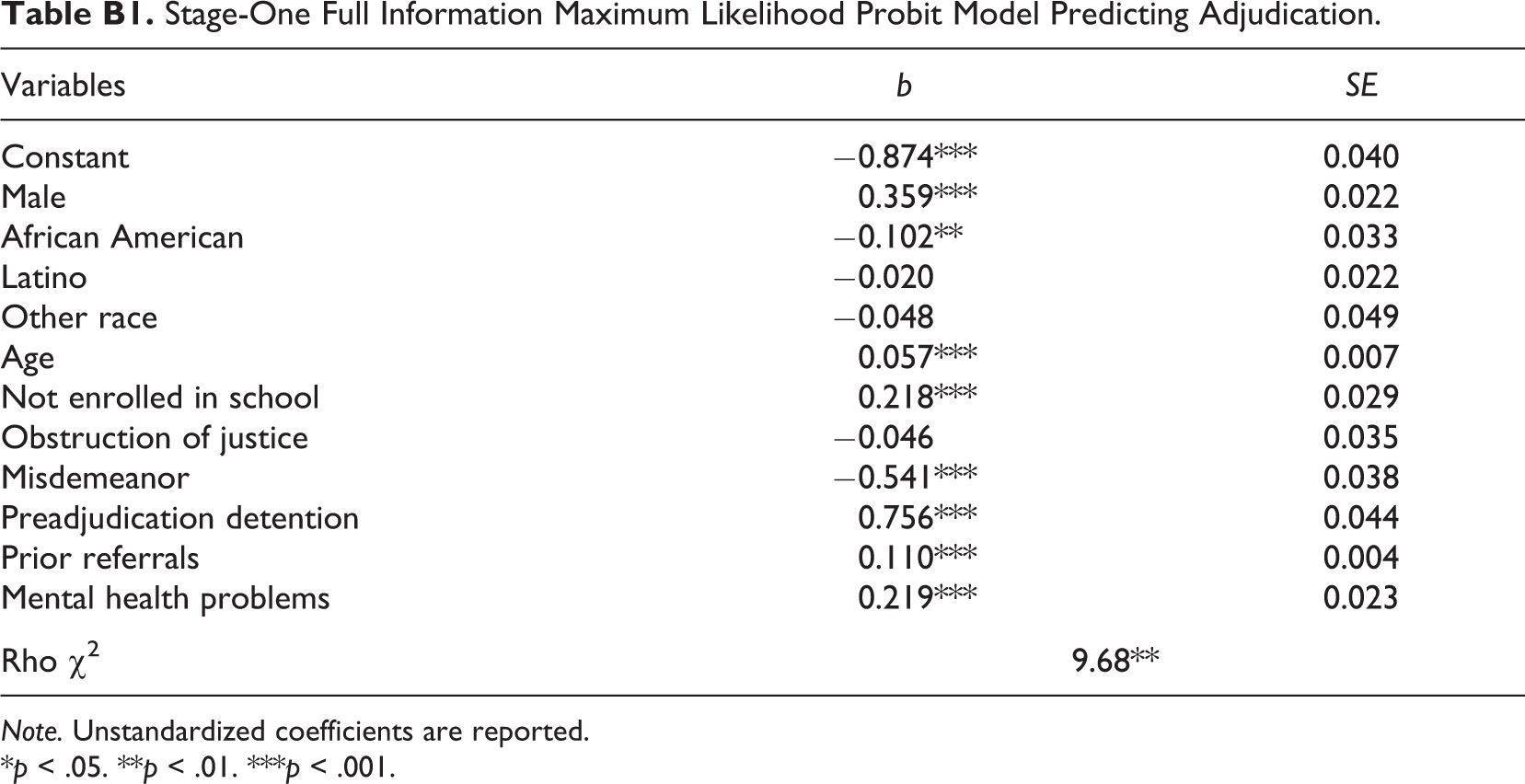
The multivariate analyses predicting correctional confinement are estimated using a two-stage full information maximum likelihood (FIML) model to control for possible selection bias (Berk, 1983). Selection bias is problematic when those selected into the subsample, in this case those who reach disposition, is not random, but influenced by factors also associated with previous stages, such as adjudication or detention. Research on sentencing often suffers from selection bias that has not necessarily been taken into account when looking at decisions further down in the court process (Bushway, Johnson, & Slocum, 2007; Jordan, 2012). FIML models estimate two probit models simultaneously, the first model is for selection, predicting adjudication in the full sample (N = 21,284), and the second model predicts the primary outcome of interest—disposition. In the current analysis, felony offenses was significantly associated with adjudication but not disposition, therefore, it was an appropriate variable to use as an exclusion restriction (see Bushway et al., 2007; Turanovic & Pratt, 2014).
Results
The bivariate descriptive statistics comparing youth sentenced to juvenile corrections versus community supervision are presented in Table 2. The independent and control variables were related to incarceration at the bivariate level in expected direction. The main variable of interest, mental health problems, was greatly represented among the youth sentenced to juvenile corrections. Similar to rates found in previous research on mental health disorders in the juvenile justice system (Shufelt & Cocozza, 2006; Teplin et al., 2002), 73.1% of the youth sentenced to correctional confinement had a reported mental health problem. This compared to only 35.8% of the youth sentenced to community supervision having a reported mental health problem.
Bivariate Descriptive Statistics of Variables.

Note. Continuous measures were examined using a t-test, and categorical variables were examined using a χ2 test.
aBonferroni corrections were calculated to reduce the risk of Type 1 error. The results did not change substantively, with the exception of age which was recoded as a categorical variable and the only significant difference in correctional confinement was between 13 and 14 year olds and 17 year olds.
*p < .05. **p < .01. ***p < .001.
In regard to race and ethnicity, Table 2 demonstrates that African Americans and Latinos had a greater representation among youth sentenced to correctional confinement, 20.2% and 49%, respectively, whereas Whites were more likely to be sentenced to community supervision, 41.8%. Youth who were sentenced to correctional confinement also tended to be male, not enrolled in school, slightly older in age, to have committed an obstruction of justice offense, were detained prior to adjudication and had a greater number of prior referrals. Finally, given our interest on the interaction effect between mental health problems and race/ethnicity, the bivariate relationship between the two variables was calculated and it was found that African Americans had the highest rate of mental health problems at 49.8%, followed by “other race/ethnicity,” White, and Latinos with lowest rate at 33.5% (χ2 = 66.7, p < .001).
Results from the stage-two FIML probit model predicting juvenile confinement are presented in Table 3. The stage-one model predicting adjudication is not discussed, but results can be found in Appendix B. In general, it is apparent that the predictors of adjudication are similar to that of the disposition decision, demonstrating the importance of controlling for the selection bias at the different stages of the juvenile justice system. Furthermore, it is important to note that the rho χ2 for the two-stage FIML was statistically significant (p < .001), which indicated significant selection bias and justified the need for the two-stage FIML (see Appendix B). In Model 1, the direct effects of the independent variables are estimated, followed by Model 2 with the interactions between mental health problems and race/ethnicity included. The odds ratios are presented for significant variables for easier interpretation.
Stage-Two FIML Probit Model Predicting Juvenile Confinement.
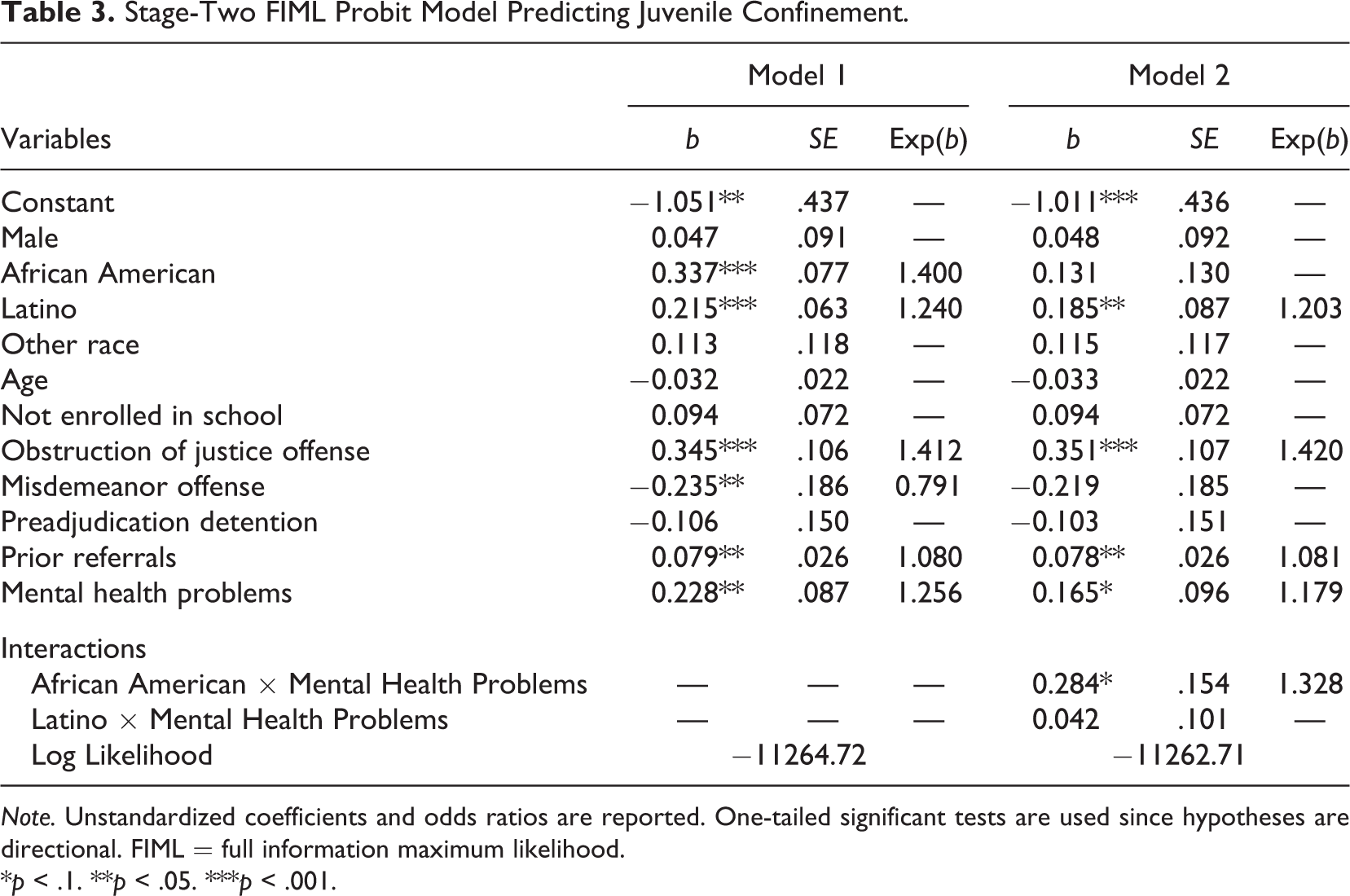
Note. Unstandardized coefficients and odds ratios are reported. One-tailed significant tests are used since hypotheses are directional. FIML = full information maximum likelihood.
*p < .1. **p < .05. ***p < .001.
There were a number of variables that had significant main effects across both models. The effects African American, Latino, felony and misdemeanor offense, prior referrals, and mental health problems were significant in the first model, with similar findings in the second model with the exception of African American. In Model 1, African Americans and Latinos were more likely to be incarcerated, 40% more likely for African Americans and 24% more likely for Latinos. The effect of African Americans was no longer statistically significant in Model 2 when the interaction between African Americans and mental health problems was included in the model. Those who committed misdemeanors were less likely to be incarcerated than those committed felony offenses and those who committed obstruction of justice offenses were more likely to be incarcerated. For each additional prior referral, the likelihood of being confined increased 8%. Finally, the direct effect of mental health problems was significant in both models, increasing the likelihood of incarceration by 25.6% in Model 1 and by 17.2% in Model 2, supporting the first hypothesis. In partial support for the second hypothesis, the interaction between being African American and having mental health problems was statistically significant and positive, but the interaction between Latino and mental health problems failed to reach significance. More specifically, African Americans with mental health problems received harsher sentences compared to Whites with mental health problems (see Table 4).
Race/Ethnicity–Mental Health Status Joint Effects.

Note. All control and county variables are included in the model.
*p < .1. **p < .05. ***p < .001.
To provide an alternative way to interpret the interaction effects, an additional model was estimated with all previous control variables plus dummy variables for each race/ethnicity-mental health status subgroup combinations. Of particular interest is how the influence of mental health problems depends on the race of the youth. Results from these comparisons are presented in Table 4. There are two reference categories presented—White youth with no mental health problems and Whites with mental health problems. It is apparent from these results that African Americans with mental health problems are treated the most severely, with a 72.8% greater likelihood of being incarcerated than Whites with no mental health problems. This was followed by Latinos with mental health problems being 43.3% more likely to be incarcerated, and Latinos with no mental health problems were 18.5% more likely to be incarcerated. The fact that the interaction effect in Model 2 of Table 3 was not significant and the main effect of Latinos was significant suggests that these disparities were largely driven by Latinos not mental health problems. Furthermore, African Americans with mental health problems were 50.8% more likely and Latinos were 25.1% more likely to be incarcerated than Whites with mental health problems. Lastly, mental health problems had no effect for White youth, thus, the more severe treatment of mental health problems only pertained to minorities.
Finally, to further demonstrate the effect of race/ethnicity and mental health problems predicted probabilities were calculated and presented in Figure 1 to provide a visual interpretation of the findings. Reference categories for the control variables were used to form the reference youth with exception that the individual was male, at mean age, and with mean number of prior referrals. As shown in Figure 1, African Americans with mental health problems stood out from all other groups, with a 49% probability of being sentenced to correctional confinement. Latinos with mental health problems were slightly more likely to be confined than Whites with mental health problems, and Whites with no mental health problems were least likely to be sentenced to correctional confinement. Thus, it is clear that the effect of mental health problems influences disposition decisions and differs across racial and ethnic groups.
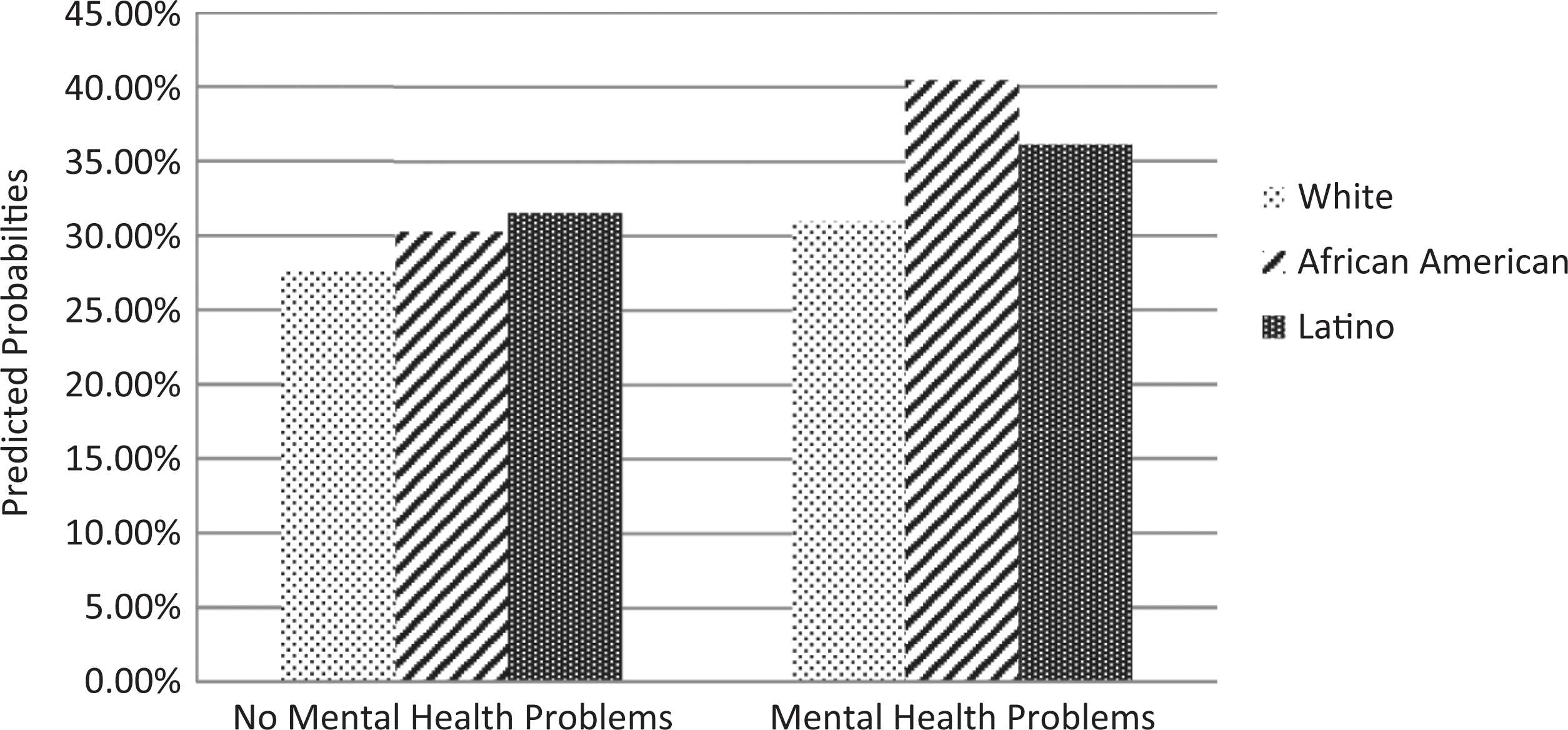
Predicted probabilities for correctional confinement. The reference category is males, age and prior referrals mean-centered, and all other controls set at zero.
Discussion
The purpose of the current study was to examine the role of mental health problems in judges’ decision to sentence youth to correctional confinement using attribution theory and focal concerns as a theoretical framework. Additionally, given the racial/ethnic disparities that exist in the processing of youth, whether the effect of mental health problems was conditioned by race/ethnicity was also examined. More specifically, we tested the hypotheses that (1) youth with mental health problems would be more likely to be committed to correctional confinement and (2) the effect of mental health problems would be exacerbated by race and ethnicity. The high prevalence of mental health problems among youth in the juvenile justice system is well established, but it has not been examined from a sentencing perspective. Supporting the hypotheses, findings revealed that mental health problems and race/ethnicity both increased the likelihood of being sentenced to correctional confinement. More notable is the conditional effect of mental health problems based on race. Specifically, the effect of mental health problems was greater for African American compared to Whites, putting African Americans with mental health problems at a greater disadvantage. The effect of race has been found to have joint effects with other legal and extralegal factors, such as age, gender, and family or community context (DeJong & Jackson, 1998; Guevara, Herz, & Spohn, 2006; Leiber, Brubaker, & Fox, 2009; Leiber & Johnson, 2008; Leiber & Mack, 2003; Rodriguez, 2013), and the current study contributes to this body of literature. The significant effect for African Americans and Latinos is consistent with prior work on racial disparities in the processing of youth in the juvenile justice system (Engen, Steen, & Bridges, 2002; Kempf-Leonard, 2007; Rodriguez, 2010, 2013). Additionally, few studies have exclusively focused on the disposition stage of the juvenile justice process and considered the role of ethnicity is juvenile court outcomes (Rodriguez, 2013). In light of these findings, the theoretical and policy implications of the current research are discussed below.
Research on perceptions of mental illness has revealed the negative stereotypes associated with mental illness, such as dangerousness and unpredictability (Hinshaw, 2005; Link et al., 1999; Martin, Pescosolido, & Tuch, 2000; Pescosolido et al., 2007). These perceptions can be understood from attribution theory and the focal concerns perspective that have been used to explain disposition and sentencing outcomes in the juvenile and criminal system. Similar to other youth characteristics, the mental health status of youth is likely considered by judges and other juvenile justice actors when deciding the best course of action for youth (Campbell & Schmidt, 2000). Consistent with earlier work, the current study found that mental health problems were an aggravating factor, increasing the likelihood of confinement for youth (Campbell & Schmidt, 2000; Cappon & Vander Laenen, 2013). There are two possible theoretical mechanisms that may explain why judges are more likely to incarcerate youth with mental health problems—(1) these youth may pose a danger to others and the community and (2) these youth need services to treat their mental health problems.
More specifically, this research informs attribution theory and focal concerns by addressing an important characteristic that can influence attributions of the cause of delinquent behavior and perceptions of dangerousness. In some cases, it may be that mental health problems are attributed to internal causes and pose a threat to public safety. Judges may not be immune to negative perceptions of mental illness and with limited information on mental health disorders they may rely on characteristics of the individual and the nature of their delinquent behavior to determine the best sentence rather than the role of the mental health problem (Black & Downie, 2010; Campbell & Schmidt, 2000). Specifically, youth offenders with mental health problems may be treated more severely because they are perceived as more dangerous and need to be held responsible for their behavior (i.e., are more blameworthy; Mukolo, Heflinger, & Wallston, 2010; Pescosolido et al., 2007; Wahl, 2003). Judges may place greater weight on legal factors rather than mental health problems and ignore recommendations of clinicians and mental health professionals on the most appropriate placement of youth (Campbell & Schmidt, 2000). In other cases, judges may attribute mental health problems and delinquency to external factors and determine that the youth has limited access to needed mental health services in the community, particularly for minorities, and that rehabilitation may be better achieved for these youth in an institutional environment than in the community (Cauffman et al., 2007).
Attributing behavior to external factors also pertains to the practical constraints focal concern. Assessing and treating mental health problems is a financial burden on the juvenile justice system that must be considered by judges. This includes identifying cost-effective treatments that meet the needs of youth and help reduce recidivism, given limited resources. Judges may assess whether treatment service needs of the youth will best be met in the community or in correctional confinement and whether the youth is capable of obtaining those services through private insurance or other means. Furthermore, these factors may be contingent on the youth’s race and ethnicity as discussed below; therefore, judges may perceive youth with mental health problems as posing more risk to public safety as well as in need of services that may go untreated if not confined.
The moderating effect of race/ethnicity on mental health problems can be explained by attribution theory and focal concerns as well. Consistent with prior work (Bishop, 2005; Engen et al., 2002; Leiber, 2002; Pope & Feyerherm, 1992; Pope, Lovell, & Hsia, 2002), the current study found that both Latinos and African Americans were treated more harshly in general, but African Americans with mental health problems were treated even more harshly than Whites with mental health problems. Latinos were more likely to be committed to juvenile corrections compared to Whites, regardless of mental health problems, whereas African Americans with mental health problems were the most likely to receive the harsher disposition. Based on the theoretical framework and prior research, there are two possible explanations for the more severe treatment of African American youth with mental health problems.
First, stereotypes of African American youth include that they are undisciplined, delinquent, and dangerousness; living in dysfunctional households with single mothers; and prone to drug offenses (Feld, 1999; Leiber, 2003). Bridges and Steen (1998) found that probation officers attributed delinquency among African Americans to bad character and personality traits that are not “amenable to the correctional treatments the courts typically administer” and, therefore, are perceived as more dangerous (Bridge & Steen, 1998, p. 576). Following this line of thought, judges may view mental health problems as part of an African American youth’s personal traits, holding them more accountable for their actions and viewing African Americans with mental health problems as exceptionally dangerous. Whereas, delinquency and criminal behavior of White youth may be viewed as the primary cause, but if treated, the individual would no longer be delinquent. “The difference between perceiving the actions of a youth as criminal (bad) rather than symptomatic of emotional difficulties (mad) may be determined in part by race” (Rawal et al., 2004, p. 251). Campbell and Schmidt (2000) found that judges more closely followed clinicians’ recommendations for dispositions of males compared to female youth and were more likely to place females with mental health problems in custody, possibly due to more dysfunctional family life. Similarly, minorities in the current research may also be experiencing similar biases unrelated to their mental well-being.
Alternatively, minorities with mental health problems may have greater need for services that are not available in the community and can be better supervised in correctional confinement. Based on Rodriguez’s (2013) findings, judges may perceive African Americans to be from disadvantaged neighborhoods and poor family environments, where mental health needs are less likely to be addressed and, therefore, views it as the state’s responsibility to intervene to ensure mental health problems are treated. The low rates of service use among African Americans and Latinos have been attributed to living in poverty (Stoep et al., 1997), and inadequate caregiving has also been found to increase the likelihood of out-of-home placement, such as juvenile corrections (Campbell & Schmidt, 2000; Lyons et al., 2001). Pullman and Heflinger (2009) found that youth in rural environments were less likely to be referred to substance abuse treatment. This was largely explained by the court’s limited contact with service providers and the court’s belief that rural areas have fewer quality service providers. Maricopa County is largely urban and the court has contracts with a number of service providers in the county, but Pullman and Heflinger’s (2009) study speaks to how the court’s perception about quality and accessibility of service providers may influence disposition decisions of youth. Judges may perceive youth in disadvantaged communities as having difficulty accessing treatment due to limited reliable transportation or parental involvement and, therefore, are hesitant about leaving these youth in the community after multiple contacts with the juvenile justice system.
Most juvenile justice research has focused on treatment of African Americans, with less attention to other minorities; however, explanations for the more severe treatment of African Americans with mental health problems likely apply to Latino youth as well. Latinos tend to share similar negative stereotypes as African Americans, such as poor, unintelligent, and prone to violence (Marin, 1984). Additionally, Latino youth are the least likely to have received mental health services (Rawal et al., 2004) and have the lowest rate of health insurance coverage in the United States (Vega & Lopez, 2001). Therefore, attributions associated with African Americans and mental health problems are likely similar for Latinos.
To provide insight on the theoretical mechanisms through which mental health problems affect judicial decision making, future research should examine case files and interview judges in the juvenile justice system. It would be informative to assess judges’ perceptions of mental health problems, its role in delinquent behavior, and the reason for sentencing these youth to correctional confinement. Additionally, it would be beneficial for research to examine how perceptions of mental illness vary based on the race/ethnicity of the individual. Mental health problems are an understudied characteristic in sentencing research but appear to play an important role in outcomes in the juvenile justice system; therefore, future research should attempt to include measures of mental health problems and need for treatment to examine its role in the criminal justice system, among both youth and adult offenders.
Findings from the present study also have important implications for policy. Regardless of the reason for sentencing those with mental health problems to correctional confinement, youth are suffering from mental health problems, and the state is responsible for providing care and treatment to those in its custody. There is growing recognition and concern for youth with mental health problems and their unmet needs (Burns, 1999; Grisso, 2004, 2008; National Research Council, 2013). Although not ideal, the juvenile justice system may be the first time where mental health problems and a need for services are recognized in a youth and the best opportunity to ensure treatment is received. This is particularly important for minority youth who are more likely to have needs go unmet. Minorities experience multiple barriers to service, such as limited access to health care and often express more negative beliefs and stigma associated with seeking out treatment for mental health problems (Connor, Copeland, Koeske, & Reynolds, 2010; Cooper et al., 2003; Gonzalez, Alegria, & Prihoda, 2005). Additionally, definitions, diagnoses, and symptoms of mental health disorders are predominately based on Western cultures and not necessarily sensitive to different cultures (Cauffman & Grisso, 2005). When mental health problems come to the attention of the juvenile justice system, it is beneficial for the youth, the juvenile justice system, and the community to have these needs addressed as to prevent future involvement in the juvenile justice system.
The degree to which mental health problems are identified and treated should be an important goal of the juvenile justice system to prevent future delinquency, but there are many challenges to address. First, there is the risk of too much assessment, such as mental health screening being used to send youth to inpatient care to free up space in detention centers (Grisso, 2004). Second, the juvenile justice system would have the difficult task of determining when they are obligated to provide mental health treatment at various stages of the juvenile justice system, without violating legal rights (Grisso, 2004). Third, for those where treatment is deemed necessary, a mental health treatment plan should be developed and implemented by trained staff, which may involve other agencies (Cocozza & Skowya, 2000). Despite the difficulty of addressing these challenges, the juvenile justice system and community will benefit from devoting resources to better meet the needs of these youth.
Despite these findings, there are limitations for future research to address. First, the primary independent variable of mental health problems was not an ideal measure of mental health disorder. The measure grouped behavioral and mental health problems together and could not be teased apart in the ARNA instrument. Access to psychological evaluations with mental health diagnoses would help researchers and practitioners better understand the role mental health disorders have on court outcomes. Second, the present study was largely exploratory, as the causal mechanisms of attribution theory and focal concerns were not examined to explain the effect of mental health problems on juvenile confinement. As discussed previously, future research should attempt to capture the perceptions of judges working with youth with mental health problems. Finally, data from this study came from one jurisdiction in the United States and only focused on the final stage of the juvenile justice system. The study took place in a single county in the United States, but international research on the role of mental health problems in the juvenile justice system has also started to emerge (Black & Downie, 2010; Campbell & Schmidt, 2000; Merlevede, Vander Laenen, & Cappon, 2014; also see Pleasence, Balmer, & Hagell, 2015). While racial and ethnic composition in other countries differs from the United States limiting the generalizability of the current study, the stigmatization of mental illness in the justice system appears to be prevalent concern in other countries (Black & Downie, 2010). Furthermore, these perceptions may differ across demographic groups, such as the conditioning effect of gender found by Campbell and Schmidt (2000) in Canadian courts. One study in Belgium found that the content of court records differs considerably between youth with and without mental health disorders, demonstrating that even the information judges may be receiving is not standardized across youth, likely influencing justice outcomes (Merlevede et al., 2014). Future research should continue to examine the role of mental health problems in justice systems and how youth of different cultural backgrounds are processed differently in other countries. Additionally, the current study only focused on the final stage of the juvenile court process, but mental health problems are likely to have effects at different stages, such as when youth are assessed for treatment service when placed on diversion or probation. Whether the youth received treatment services and the degree to which those services appeared effective may affect future decisions if the youth returns to the juvenile justice system. Research should continue to understand the role of mental health problems at various decision points in the juvenile justice system, not just independently, but also as a process.
Conclusion
This is one of a few studies that has examined the role of mental health problems and race/ethnicity from a court outcomes and sentencing perspective, providing a starting point for future research to examine how youth and adult offenders with mental health problems are perceived and processed in the court system. Some extralegal factors may lead to unwarranted disparities, but there are also extralegal factors that should be considered because they have important implications for rehabilitation efforts and public safety. Not every youth with mental health problems is dangerous or needs treatment, and access to services is not equal across racial/ethnic groups; therefore, these factors pose unique challenges for the juvenile justice system. Judges must not only consider the safety of the public but also the well-being of youth and the best intervention to ensure that needs are met while also reducing the risk of recidivism.
Footnotes
Appendix A
Descriptive Statistics of Variables for Full Sample of Referred Youth.

| Variables | % | Mean | SD | Range |
|---|---|---|---|---|
| Gender | ||||
| Female (reference) | 35.2 | — | 0.48 | 0–1 |
| Male | 64.8 | — | 0.48 | 0–1 |
| Race/ethnicity | ||||
| White (reference) | 41.5 | — | 0.49 | 0–1 |
| African American | 11.8 | — | 0.32 | 0–1 |
| Latino | 42.2 | — | 0.49 | 0–1 |
| Other | 4.5 | — | 0.21 | 0–1 |
| Age | — | 15.9 | 1.61 | 8.2–18.2 |
| School status | ||||
| Enrolled (reference) | 86.7 | — | 0.34 | 0–1 |
| Not enrolled | 13.3 | — | 0.34 | 0–1 |
| Offense type | ||||
| Felony (reference) | 13.0 | — | 0.34 | 0–1 |
| Obstruction of justice | 59.2 | — | 0.49 | 0–1 |
| Misdemeanor | 27.8 | — | 0.45 | 0–1 |
| Preadjudication detention | 6.7 | — | 0.25 | 0–1 |
| Prior referrals | — | 1.56 | 2.42 | 0–25 |
| Mental health problems | 24.6 | 0.43 | 0–1 | |
Note. N = 21,284.
Appendix B
Stage-One Full Information Maximum Likelihood Probit Model Predicting Adjudication.
| Variables | b | SE |
|---|---|---|
| Constant | −0.874*** | 0.040 |
| Male | 0.359*** | 0.022 |
| African American | −0.102** | 0.033 |
| Latino | −0.020 | 0.022 |
| Other race | −0.048 | 0.049 |
| Age | 0.057*** | 0.007 |
| Not enrolled in school | 0.218*** | 0.029 |
| Obstruction of justice | −0.046 | 0.035 |
| Misdemeanor | −0.541*** | 0.038 |
| Preadjudication detention | 0.756*** | 0.044 |
| Prior referrals | 0.110*** | 0.004 |
| Mental health problems | 0.219*** | 0.023 |
| Rho χ2 | 9.68** | |
Note. Unstandardized coefficients are reported.
*p < .05. **p < .01. ***p < .001.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.