
Abstract
Low empathy has been implicated in antisocial, aggressive, and criminal behavior, especially among adolescents. Less understood is the extent to which empathy is amenable to treatment, and whether an improvement in empathy can mitigate the deleterious effects of known risk factors, such as childhood maltreatment. A sample of 11,000 serious juvenile offenders in long-term residential placement is leveraged to examine whether over cumulative traumatic exposure, measured by the adverse childhood experience (ACE) score, is associated with the initial level of empathy at admission to a residential program, and whether changes in empathy during treatment moderate the impact of ACEs on juvenile recidivism. Results show youth with higher ACE scores have less empathy at admission and both ACEs and empathy predict recidivism. Most importantly, large gains in empathy are able to dampen the effect of ACEs on recidivism.
Introduction
Since the early part of the 20th century, philosophers have linked a concept referred to as empathy to delinquent and criminal activity. What exactly is empathy? For Buber (1923), empathy entails one’s ability to distinguish between the “I-you,” where one is connecting with another person’s thoughts and feelings, and the “I-it,” where one is treating the person as an object. More recently, Cohen and Strayer (1996) define empathy as “the ability to understand and share in another’s emotional state or context” (p. 988). And Joliffe and Farrington (2004) suggest that this definition acknowledges “that empathy is both a cognitive process (i.e., the ability to understand another’s emotional state) and an affective capacity (i.e., the sharing of the emotional state of another)” (p. 442). What these definitions and interpretations all have in common is the notion that in some way, shape, or form, empathy connotes a regard for, or the ability to appreciate, the feelings of others (Miller & Eisenberg, 1988). Not surprisingly, then, low empathy has consistently been linked to antisocial, aggressive, delinquent, and criminal behavior (Joliffe & Farrington, 2004, 2007) while higher empathy serves as a protective factor for such behavior (Broidy et al., 2003).
Although the knowledge base regarding the relationship between empathy and crime is strong, there remain some important gaps in the literature. In particular, while many prison treatment programs have empathy as a part of their intervention strategy—especially within the context of cognitive-behavioral strategies (Mulloy et al., 1999; Ross & Ross, 1995), less research has examined the extent to which empathy is sensitive to treatment intervention among juvenile offenders, and the extent to which empathy may serve as a buffer that limits the effects of other known risk factors on criminal activity, especially those surrounding childhood maltreatment. Accordingly, the current study uses data from a large sample of adjudicated serious juvenile offenders in the state of Florida to examine whether changes in empathy during residential treatment moderates the impact of one very strong risk factor composite, adverse childhood experiences (ACE), on juvenile recidivism. A focus on juvenile offenders is especially important because: (1) prior research has found that empathy is more strongly related to offending among adolescents than adults and (2) juvenile offenders are at a pivotal time period when some of them will continue their criminal activities into adulthood and others will desist (Piquero et al., 2012). The extent to which these juveniles can learn protective factors, such as improving their empathy, is an important policy issue. Before we turn to the results of our analyses, we provide overviews of the literatures that we integrate in the current study, namely: empathy, childhood maltreatment, ACEs, and their inter-relationships to criminal activity.
The Role of Empathy and Delinquency
Defining Empathy
Definitions of the concept of empathy have differed on two main components: the emotional component, where one is able to experience the emotions of another, or the cognitive component, where one is able to understand the emotions of another. More recently, however, researchers who study empathy have started to agree that empathy likely encompasses both emotional and cognitive components (Joliffe & Farrington, 2006).
Empathy and Offending
Within the criminological and psychological research, studies continue to demonstrate strong support for the relationship between empathy and offending, with lower empathy being related to an increased risk of offending. Studies have shown that individuals who had previously demonstrated violent behavior also demonstrated lower empathy, a finding that is true for both males and females (Joliffe & Farrington, 2007). Much of the reasoning behind this connection centers on the notion that those individuals with lower empathy do not feel repressed from engaging in behavior that might be harmful to others since they do not fully understand or appreciate the harm done to that person (Feshbach, 1975; Joliffe & Farrington, 2006; Miller & Eisenberg, 1988). Empathy has been found to be a factor in self-reported offending, violent offending (Joliffe & Farrington, 2007), sexual offending (Barnett & Mann, 2013; Burke, 2001; Mann & Barnett, 2013), and bullying behaviors (Joliffe & Farrington, 2006).
In one prominent study of 720 male and female adolescents (mean age = 14.8) in the United Kingdom, Joliffe and Farrington (2007) compared measures of cognitive and emotional empathy to self-report offending. They found that both males and females who had committed a violent offense had lower empathy than those who had not committed a violent offense, and that high-rate offenders of both sexes had lower empathy than low-rate offenders. Results differed between males and females with respect to overall offending, where males who had committed any offense (not just violent) had lower empathy scores overall; for females, however, those who had committed any nonviolent offense did not differ on their levels of empathy compared to the other females who had not offended. Other research has looked specifically at empathy and sexual offending (Hanson, 2003). Most of the research on this subgroup of offenders suggests that they do not lack empathy in general, but rather mainly for their victims (Fernandez & Marshall, 2003; Marshall et al., 2009).
Empathy Intervention
Given how consistently empathy has been found to be related to antisocial behavior, it is not surprising to find that it is a key component of many treatment and intervention programs, many of which have been applied to sex offenders. Yet, results have been mixed with respect to its effectiveness on samples of sex offenders in particular (Brown et al., 2012; Hanson, 2003; Jackson & Bonacker, 2006; Mann & Barnett, 2013). For example, in an evaluation of an empathy-focused victim impact training (VIT) program, Jackson and Bonacker (2006) found overall support for the program, where VIT participants were less likely to recidivate than those in the control group; however, they found that empathy alone had no significant effect on recidivism. Conversely, in their 10-year longitudinal study of 105 sex offenders in England and Wales, Brown and colleagues (2012) found that victim-specific empathy improved during treatment and was related to overall change, but that a small group of offenders whose victim-empathy scores decreased from pre- to post-treatment had higher rates of recidivism as compared to the rest of the sample.
In samples other than sex offenders, some research has documented a significant relationship between empathy and recidivism. For example, Bock and Hosser (2014) evaluated the role of empathy in predicting recidivism among a sample of 748 male offenders between the ages of 15 and 28. Their longitudinal study found that global empathy scores, especially the subscales of perspective taking and empathic fantasy, contributed to the ability to predict recidivism. Researchers have also included parenting style into the model, examining the role of empathy and parenting on the development of antisocial behavior. Schaffer and colleagues (2009), for example, conducted a self-report survey of 242 undergraduate students that asked questions pertaining to their antisocial behaviors, empathy, and mothers’ and fathers’ parenting styles. They found that parenting style, specifically maternal permissive parenting, contributed to antisocial behavior through its effects on cognitive and emotional empathy development.
Childhood Maltreatment and Juvenile Offending
Early experiences of childhood maltreatment such as abuse and neglect are associated with a number of negative outcomes later in life including: substance use problems (Chatterjee et al., 2018; Dube et al., 2003), poor mental health outcomes (Chapman et al., 2004; Jones et al., 2018; Perez et al., 2016), poor physical health outcomes (Felitti et al., 1998; Thompson et al., 2015), involvement in serious offending and/or violence (Duke et al., 2010; McCord, 1983; Stouthamer-Loeber et al., 2001; Widom, 1989), juvenile offending (Smith & Thornberry, 1995), and an earlier age of onset in offending (Barrett et al., 2014; Dannerbeck & Yan, 2011).
In attempting to shed light on the underlying nature of this relationship, some scholars have proposed the cycle of violence hypothesis, which highlights the negative consequences that early abuse and neglect have for crime and violence over the life course. Indeed, retrospectively, a majority of offenders report some history of victimization when compared to the general population (e.g. Baglivio et al., 2014). In a 20-year longitudinal study involving 908 children in Indianapolis who were abused or neglected before the age of 11, Maxfield and Widom (1996) found that those who were abused or neglected were significantly more likely to have arrests in adolescence and in adulthood as compared to a matched control group. In a follow-up study, Widom and her colleagues (2017) examined variability in criminal careers across the control and abused/neglected groups, as well as gender, and found that childhood maltreatment affects life-long patterns of offending, with the highest rate offenders being male and abused/neglected.
Adverse Childhood Experiences (ACEs)
There are limitations to considering exposure to only one maltreatment event (e.g. abuse) in a given study, particularly in light of research examining poly-victimization, suggesting that early victimization experiences are highly interrelated and have cumulative effects on an individual throughout the life course (e.g., Anda et al., 2010; Dong et al., 2004). In a seminal study, Felitti et al. (1998) sought to examine the relationship between adverse life experiences in childhood and subsequent health outcomes and social functioning in adolescence an adulthood. In doing so, they developed the adverse childhood experiences (ACE) scale, which in its initial iteration referred to an individual’s exposure to seven categories of abuse and household dysfunction: psychological abuse, physical abuse, sexual abuse, household substance use, household mental illness, violence towards mother, and household history of incarceration. The resulting score ranged from 0 to 7, each additional score representing the exposure to another type of childhood adversity. Thus, the aggregate ACE score takes into consideration both the cumulative impact of poly-victimization, as well as the contextual background of the negative family environments in which these abusive experiences take place. Using a sample of 17,421 adults in their initial investigation of ACEs, Felitti et al. (1998) found that a greater number of ACEs reported increased the probability of poor physical health, chronic disease, health risk behaviors (alcohol and drug use, sexual risk behavior), mental illness, and early mortality in adulthood. In successive iterations (see for example Dube et al., 2003), the ACEs scale was expanded to include physical neglect, emotional neglect, and parental separation or divorce, resulting in a composite score ranging from 0 to 10.
Since the original ACE scale was developed, studies have employed more advanced statistical analyses to elucidate the relationships between ACEs and health outcomes. Recently, Jones et al. (2018) used structural equation modeling to examine the pathways from ACEs to mental health impairment in adulthood among a sample of 14,000 adults in Washington State. ACEs had prevailing effects on adult mental health both directly and indirectly through low income in adulthood and adult adversity. Examining heterogeneity of exposure to ACEs over time, Thompson et al. (2015) found that chronic exposure to ACEs in childhood was significantly predictive of self-reported physical health concerns at age 18. A primary conclusion drawn from the initial ACE studies was that there was a graded relationship between the number of ACEs and the risk of poor health outcomes, suggesting that as the number of ACEs an individual experienced increased, so did the risk of these negative outcomes.
Juvenile Offending Outcomes
Since the Felitti et al. (1998) study, ACEs research has advanced beyond the initial focus on physical and mental health outcomes. Recent studies support the existence of a similar dose-effect response of ACEs on offending behavior, i.e. a greater accumulation of ACEs is associated with a more serious pattern of offending. For example, ACEs have also been associated with both self-directed and interpersonal violence perpetration among a sample of high school students, with each additional type of ACE resulting in an increase in the risk of violence perpetration from 35% to 144% (Duke et al., 2010).
In particular, a number of studies have examined the relationship between ACEs and juvenile offending using data collected from the Florida Department of Juvenile Justice (e.g., Baglivio, Jackowski, et al., 2014; Baglivio et al., 2015; Fox et al., 2015; Wolff et al., 2017). In one study, Baglivio, Epps, et al. (2014) highlighted the pervasiveness of child maltreatment within at-risk youths’ lives, finding that 96% of youth in their sample of juvenile offenders had experienced at least one ACE in their lifetime, and 40% had experienced four or more.
With respect to serious offending, Fox and colleagues (2015) found that each additional ACE resulted in an increased likelihood of being a serious, violent, and chronic offender (as defined in the study as a juvenile offender with three or more felony referrals, wherein at least one of these was for a violent offense) by 35 times, as compared to the non-violent “one-and-done” comparison group. Similarly, Baglivio et al. (2015) found that having more ACEs was also associated with an earlier onset of offending and a chronic level of offending. Youth with more ACEs were also found to be more likely to reoffend (Wolff & Baglivio, 2017) and to reoffend sooner (Wolff et al., 2017) following completion of a community-based program. Furthermore, ACEs assessed at age 12 were significantly predictive of residential placement by age 18 for Black and Hispanic males, as well as for Black females (Zettler et al., 2018).
In addition to the assessment of direct effects of ACE exposure on delinquent activity, researchers have begun to explore other factors that may enhance our understanding of the relationship between ACEs and offending. For example, studies have examined the relationship between ACEs, substance use, and juvenile offending among a statewide sample of youth in the state of Florida. Craig et al. (2019) found that the relationship between ACEs and recidivism is particularly pronounced among youth who engaged in moderate-to-high substance use. A second explanatory mechanism linking substance use and offending is through gang involvement. Using a sample of over 100, 000 juvenile offenders, Wolff et al. (2020) found a relationship between ACE scores and both self-report and official measures of gang involvement by age 18. Furthermore, this relationship was mediated by the effect of ACEs on substance use and a difficult temperament. Thus, substance use may be one way in which ACEs exacerbate the risk of juvenile offending. Lastly, another construct worth considering is the role of self-control, particularly given the relationship between low self-control and delinquency (Pratt & Cullen, 2000). On this score, Meldrum et al. (2020) found an inverse relationship between ACEs and self-control in both a community sample and within a correctional sample of adolescents, with ACEs accounting for 7% of the variation in self-control for both groups. Although a growing number of empirical studies have started to pay closer attention to the mechanisms underlying the ACEs-offending relationship, the role of potential protective factors remains relatively underexplored. In other words, the types of factors that may inhibit the potentially adverse effect of ACEs from influencing antisocial behavior has been ill-studied.
On the Relationship Between ACEs and Empathy
Much like self-control, the development of empathy has been linked to positive parental attachment and socialization (Knafo & Plomin, 2006). Conversely, lack of empathy has been linked to childhood neglect, abuse, victimization, and deprivation (Simons et al., 2002). Given the negative consequences of each of these instances of maltreatment independently, an individual who has experienced not just one of these instances but rather a constellation of them may be less likely to develop empathic traits. ACEs, therefore, might serve as a barrier to empathy development. To date, little research has looked at the relationship between ACEs and empathy. Instead, researchers have focused on the effects of specific types or victimization or poly-victimization on empathy. For example, Simons and colleagues (2002) evaluated the effects of childhood victimization on later sexual offending, and examined empathy as a mediator in this relationship. They found that individuals who reported childhood abuse or victimization displayed less empathy in a number of different situations. Other work has looked at the effects of bullying and victimization during childhood on cognitive empathy development. In their sample of youth, Williford and colleagues (2016) found that cognitive empathy decreased over time as a result of bullying victimization. Despite the evidence that a number of different negative experiences or instances of maltreatment might have an effect on empathy, little research has looked directly at the relationship between ACEs and empathy. We add to research in this area by assessing the relationship between ACEs and youths’ levels of empathy at the time of admission to a juvenile justice residential facility.
Impact of ACEs on Recidivism Moderated by Changes in Empathy
As reviewed above, low empathy and ACEs are each independently related to antisocial behavior. Yet, little research has been conducted on changes in empathy during treatment, specifically residential treatment, and whether gains in empathy are not only protective against offending but also potentially help to buffer other known risk factors such as ACEs. Research has shown that empathy is not a fixed trait, but instead one that may change over time in response to different life experiences. For instance, empathy can decrease in individuals who have been victims of bullying behaviors (Williford et al., 2016) or increase in individuals who undergo specific empathy-focused therapy or programming (Marshall et al., 1996). 1
Given the research highlighted above, we propose that changes in empathy during residential treatment may moderate the impact of ACEs on recidivism upon release. That is, improvements to empathy might serve as a protective factor against ACEs, and in turn decrease the risk of recidivism. Conversely, if individuals demonstrate decreases in empathy – or do not gain in empathy during treatment, they might be at an increased risk of recidivism and may not be able to ward off the deleterious consequences of childhood maltreatment.
Current Study
The current study aims to add to this body of literature by examining if 1) ACEs are associated with the initial level of empathy at time of admission to a residential program and 2) whether changes in empathy during residential treatment moderate the impact of ACEs on juvenile recidivism as measured by both rearrest and readjudication. We examine this issue with a unique multiyear statewide sample of 11,053 juvenile offenders returning to the community following residential placement.
Sample
The current study employs a sample of youth who completed a juvenile justice long-term residential program in Florida during the three fiscal years of July 1, 2009 through June 30, 2012. The sample was limited to using only the first residential placement for each adolescent during the study period (ensuring each youth was included only one time in the data). Additionally, only youth who were assessed at a minimum of two times during placement were included. The risk/needs assessment used by the Florida Department of Juvenile Justice (FDJJ), the Residential Positive Achievement Change Tool (R-PACT) was implemented in 2009, with only new admissions being required to be assessed. As such, some earlier admissions in 2009 were excluded. The policy surrounding the importance of initial assessment and reassessment of risk and protective factors includes R-PACT administration at admission, every 90 days thereafter, and prior to release. As the current study focuses on ACEs, empathy, and changes in empathy over time, the initial assessment (admission R-PACT) is used for ACEs, Time 1 empathy, and all covariates, while the exit assessment (R-PACT at release) is leveraged for computing a change in empathy (discussed below). As such, data for each youth includes two R-PACT assessments. This results in a final sample of 11,053 unique youth who completed a FDJJ residential program between 2009 and 2012.
Uniquely, FDJJ juvenile justice residential facilities are 100% privatized and located throughout Florida. In Florida, only a judge can place a juvenile in a residential facility, and only a judge can release that juvenile. Additionally, each residential program is “specialized” meaning all youth placed in a given program have similar overarching treatment needs (e.g., substance abuse treatment, comprehensive mental health needs, prior sexual offending behavior), with services individually tailored within the specialized program. The length of stay for each youth is based on completion of an individualized performance and treatment plan, which are based on the R-PACT assessed risk/needs as well as the youth’s clinical diagnoses. Length of stay is not determinate, with the exception of maximum risk facilities which garner an 18-month minimum stay. All youth without a high school diploma or equivalent are required to attend school year-round and all youth are assigned a case manager and therapist. FDJJ Administrative Code requires any youth with a mental health or substance abuse condition to receive treatment for that issue.
Measures
To briefly elaborate on the R-PACT assessment, the tool measures static and dynamic risk and protective factors across the following domains: criminal history, education/vocation, use of free time, employment, relationships/peer associations, family, substance use, mental health, attitudes, aggression, and social skills. The assessment is administered as a semi-structured interview protocol by bachelor-level case management staff who have completed a three-day R-PACT software and case planning training (inclusive of interrater reliability exercises) and a standardized two-day Motivational Interviewing training. Selection of forced-choice responses to each item produces software-scored dynamic and static risk and protective scores for each domain (with the exception of criminal history which produces only static risk). The validity of the R-PACT has been demonstrated, as higher domain risk scores at release increase the odds of subsequent recidivism (Hay et al., 2018). Additionally, the ability of dynamic changes in R-PACT domain risk scores to predict recidivism post-release has multi-sample support from several studies (c.f. Baglivio et al., 2017; Baglivio et al., 2018; Wolff et al., 2017).
Dependent Variables—Recidivism
Two dependent measures were used to capture official recidivism: rearrest and readjudication. Rearrest was measured as a subsequent referral or adult arrest for a new-law offense committed within 365 days of the release date for a given participant. Readjudication uses the official definition of the FDJJ of a subsequent adjudication, adjudication withheld, or adult conviction for a new-law offense that occurred within 365 days of a given participant’s release date. The offense must have occurred within 365 days, but the tracking period is months longer to allow for court processing time. Both measures of recidivism included juvenile and adult official records as some participants were (or turned) 18 years of age (the age of majority in Florida) during the tracking period. As shown in Table 1 58.2 of the sample was rearrested within one year of release, and 40.1% was readjudicated (or had adjudication withheld) or reconvicted (in the adult system) for an offense committed within one year.
Descriptive Statistics (n = 11, 043).

Key Independent Variables
Empathy
Empathy was the first key independent measure critical to the current study and is measured as a standardized index of four R-PACT items, as assessed at admission (Time 1 empathy). A direct R-PACT item assessing the extent to which the youth has empathy, remorse, sympathy, or feelings for the victim(s) includes the following response options: does not have empathy for victims, has some empathy for victims, or has empathy for victims (coded 1–3, with higher values indicating a greater extent of empathy). Second, respect for the property of others classifies youth as having no respect for the property of others, conditional respect for personal property of others, respects others personal property but not public property, and respecting the property of others (coded 1–4, with higher values indicative of greater empathy). Third, respect for authority figures classifies youth as defies or hostile toward most authority, resents most authority, does not respect authority figures and may resent some, and respects most authority figures (coded 1–4, with higher values indicating more empathy). 2 Finally, whether the youth accepts responsibility for his/her antisocial behavior is measured as proud of antisocial behavior, accepts antisocial behavior as okay, minimizes or justifies antisocial behavior, or the youth accepts responsibility for antisocial behavior (coded 1–4 with higher values indicative of greater empathy). The four items were standardized and combined into an empathy index (α = .716).
Change in Empathy
A measure of the extent of change in empathy from admission to release was created using the Time 1 empathy measure (described above), and an identical measure of Time 2 empathy created from the exit R-PACT (at release; α = .746). A change in empathy score was created by subtracting Time 1 empathy from Time 2 empathy (the absolute change in empathy from Time 1 to Time 2).
Adverse Childhood Experiences (ACE) Score
The ACE score measures the youth’s extent of cumulative exposure to the 10 ACE indicators. In keeping with the prior ACE-specific work discussed above, we include binary (yes/no) indications for the ten indicators, then summing exposures for 0 (no exposures) to 10 (exposure to each of the ten indicators) ACE score. A brief description of each ACE and responses indicating affirmative exposure are as follows: (1) Emotional abuse: Parents/caretakers were hostile, berating, and/or belittling to youth; (2) Physical abuse: The youth reported being victimized or physically abused by a family member; (3) Sexual abuse: The youth reported being the victim of sexual abuse/rape; (4) Emotional neglect: Family has little or no willingness to support youth and/or youth does not feel close to any family member; (5) Physical neglect: The youth has a history of being the victim of neglect (includes a negligent or dangerous act or omission that constitutes a clear and present danger to the child’s health, welfare, or safety, such as failure to provide food, shelter, clothing, nurturing, or health care); (6) Family violence: Domestic violence or sexual abuse in the home (not against the youth him/herself), or if the youth has witnessed violence in either their home, or in a foster/group home; (7) Household substance abuse: Problem history of parents and/or siblings in the household includes alcohol or drug problems; (8) Household mental illness: Problem history of parents and/or siblings in the household includes mental health problems; (9) Parental separation/divorce: Youth does not live with both mother and father; and (10) Incarceration of household member: There is a jail/prison history of family members. The ten exposures were summed, resulting in an average ACE score for the sample of 3.35 (SD = 1.86). 3
Control Variables
Demographics
Demographic measures included age at admission (measured continuously, mean = 16.5, sd = 1.31), male (85.6%), and race/ethnicity measured as a series of dichotomous items for Black (52.6%) and Hispanic (11.5%). Of note, according to FDJJ protocol, ethnicity supersedes race such that Black youth were all non-Hispanic and Hispanic youth may be either Black or White.
Criminal History
Measures of the youth’s prior offending included age at first arrest, prior felony arrests, prior against-person felony offending, and prior residential placement. Importantly, all criminal history indicators are automated from the FDJJ information system and therefore do not depend on recall of the youth or ability of the R-PACT assessor to understand and aggregate prior charges. Age at first arrest was captured according to the R-PACT protocol of under 12, 13–14, 15, 16, or over 16 years old at first arrest (coded 1–5, with higher values indicative of being older when first arrested. Felony offending classified youth as having no, one, two, or three or more prior felony arrests at admission (coded 1–4, with higher values indicating a greater number of felony arrests). Against-person (violent) felony offending assessed whether the youth had no, 1–2, or 3 or more against-person felony arrests (coded 1–3 with higher values indicating more violent offending). Finally, whether the current residential placement was the youth’s first such residential placement or if the youth had one or more prior residential placements was included (a dichotomous indicator; 10% had a prior residential placement).
Self-Reported Gang-Involvement
A measure of self-reported gang involvement was drawn from the initial R-PACT. An item assessing self-reported gang-involvement along with delinquent peer associations includes a response option of “been a gang member/associate.” This option was used to determine youth who reported being gang-involved (13%, sd = .336). While there is some disagreement in the literature regarding such measures, we note here that several studies have used a single self-report item for gang association (e.g., Melde & Esbensen, 2011) and have indicated the validity of self-reported gang-involvement items (e.g., Krohn et al., 2011).
Self-Control
The adolescent’s self-control was drawn from four R-PACT items. The youth’s ability to exhibit self-control was captured using a categorical measure including lacks techniques to use self-control, rarely uses such techniques, sometimes uses techniques, and often uses techniques for exhibiting self-control (coded 1–4, with higher values indicative of more self-control). The second item assessed whether the youth believed he or she can avoid/stop antisocial behavior, somewhat believes antisocial behavior is controllable or believes his or her antisocial behavior is out of his or her control (then recoded 1–3, such that higher values indicate greater self-control). Third, the youth’s level of impulsivity was assessed as using self-control/usually thinking before acting, sometimes thinking before acting, impulsive, or highly impulsive/usually acts before thinking (then recoded 1–4, with higher values indicative of less impulsivity). Lastly, the youth’s ability to control impulsive behavior was assessed as lacks techniques to control impulsive behavior, rarely uses techniques to control impulsive behavior, sometimes uses such techniques, or no problems with impulsivity/often uses techniques to control impulsive behavior (coded 0–3, with higher values indicating less impulsivity). Each of these items was first standardized, and an index of self-control was created by summing the standardized scores (α = .787). 4
Mental Health Problems
A dichotomous indicator for youth no history of mental health problems (=0) and those with mental health problems (=1) was included. Mental health problems included schizophrenia, bipolar, mood, thought, personality, and adjustment disorders. Conduct disorder, oppositional defiant, ADD/ADHD, and substance abuse disorders were excluded. All mental health problems must have been confirmed by a professional qualified to do so (e.g., psychologist, licensed mental health counselor).
Past Drug Use
Whether the youth had a history of drug and/or alcohol use was captured by an R-PACT item distinguishing youth without a history of drug and/or alcohol use from those with prior use and those whose substance use has caused problems across life domains such as school, family, health, peer associations, or criminal behavior (coded 0–2, respectively).
Length of Stay (LOS)
The length of time the youth was placed in the residential program was included (measured in days, mean = 244). LOS allows for statistical control of the length of time each youth received treatment in the facility to allow for a change in empathy to occur (positive or negative). Descriptive statistics for all variables included in the current analysis are shown in Table 1.
Analysis Plan
The relationship between ACEs, empathy, and juvenile recidivism was explored using a number of traditional bivariate and multivariate methods including rank-order correlations, ordinary least squares regression (OLS), and logistic regression. First, we examined the bivariate correlations among all variables included in the analysis to ensure that collinearity was not an issue as well as assess the relationships present among the measures included in the current study. Subsequently, OLS regression was used in order to evaluate the potential for ACEs to impact levels of empathy at the time of admission to residential placement. 5 Following this, logistic regression was used to evaluate the impact of ACEs and empathy on two measures of juvenile recidivism (rearrest and readjudication). Finally, the effect of ACEs on reoffending was estimated across three subsamples of youth, who varied in terms of changes in empathy during residential placement (small, moderate, and large). This “pick-a-point” method has been used in past research to probe the interaction between two variables within the context of logistic regression (Hayes & Matthes, 2009). This method involves selecting representative values on the moderator variable (changes in empathy during residential placement) and then estimating the effect of ACEs at those specified values (see, e.g. Cohen et al., 2003). The results presented here are based on samples among the top 25%, middle 50%, and bottom 25% of the changes in empathy measure. 6
Results
Table 2 presents the bivariate correlations for all key variables included in the current analysis. Results of this preliminary analysis indicate that collinearity is not an issue as the majority of the correlations are well below r = .5. Further, the bivariate relationship between the independent variables and both measures of juvenile recidivism were consistent with theory and past research. ACEs were positively and significantly associated with both rearrest and readjudication, although this association can be considered small in terms of magnitude. Empathy at time of admission was also significantly related to both measures of recidivism post-release, with higher levels of empathy being associated with lower rates of recidivism. Among the control variables, sex (male), race (Black), and age at first offense were also positively and significantly related to both measures of recidivism as was history of residential placement, history of gang involvement, and self-control (negatively correlated).
Spearman Rank-order Correlations between Measures in the Analysis of Adverse Childhood Experiences, Empathy, and Juvenile Recidivism.
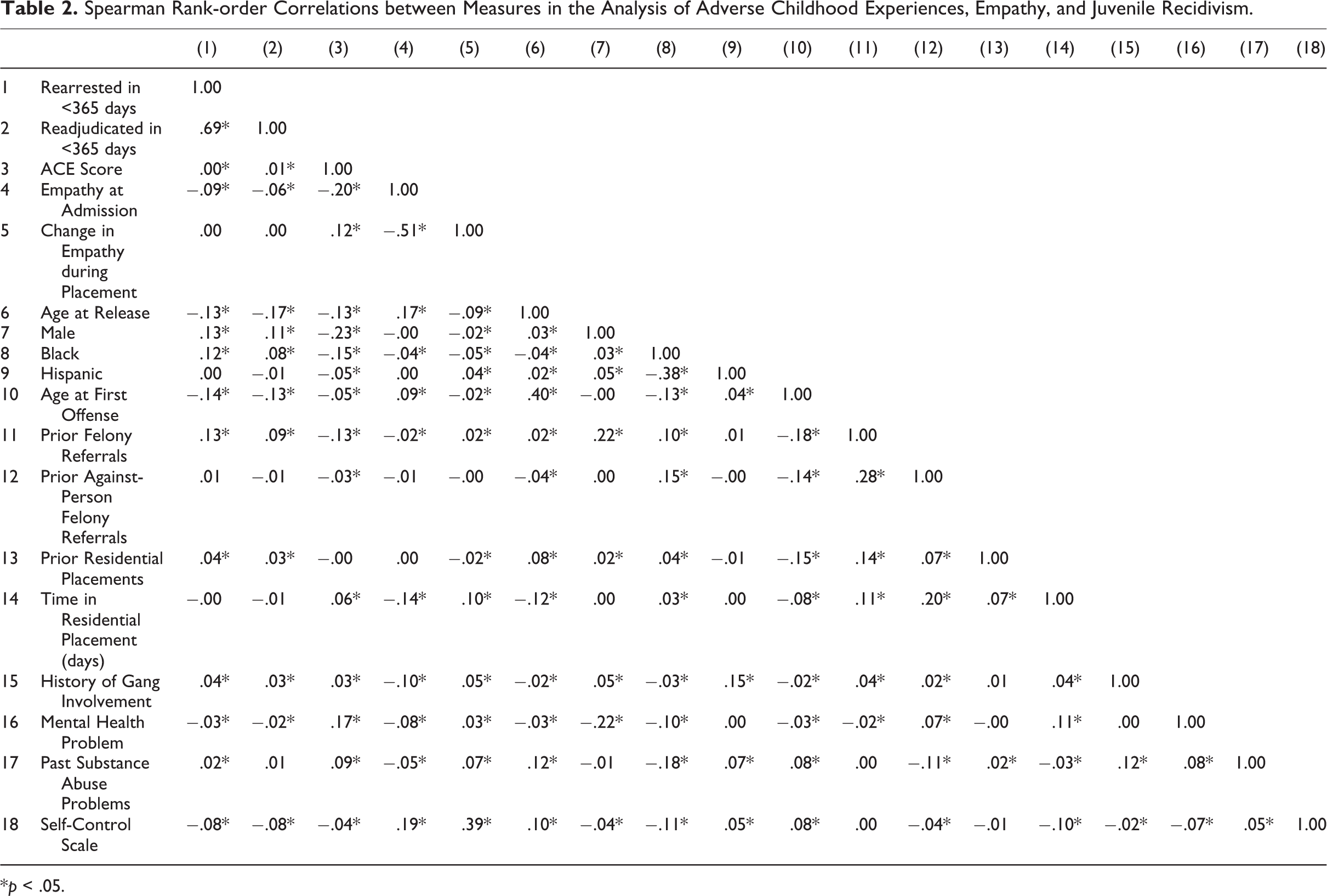
*p < .05.
Relationship Between ACEs and Empathy
Results presented in Table 3 evaluate the relationship between the ACE score and empathy at the time of admission to residential placement. In each of the models shown, higher ACE scores were associated with lower empathy at time of admission. Results highlight the relationship between ACEs and levels of empathy among this sample of high-risk juveniles involved in the criminal justice system.
Effect of ACEs on Empathy at Admission to Residential Placement.

n = 11, 043. *p < .05, **p < .01, ***p < .001.
Relationship Between ACEs, Empathy, and Recidivism
The analyses presented in Table 4 assess the main effects of ACEs, empathy at admission to residential placement, and changes of empathy on our two measures of juvenile recidivism using logistic regression. The first two models indicate that higher ACE scores were related to an increased likelihood of rearrest, net of all control variables included. Specifically, with each additional ACE reported, the likelihood of recidivism increased by 4.4% to 4.7%. Empathy at admission was also significantly related to rearrest post-release from residential placement, with higher empathy being associated with a lower chance of recidivism. Further, the results in model one suggest that increases in empathy, achieved during time in residential treatment, were associated with lower recidivism likelihoods. However, this effect became non-significant (p > .05) following the inclusion of the full list of control variables. Consistent with past research on juvenile recidivism in the state of Florida, age at first offense, prior felony referrals, a history of residential placement, past substance abuse problems, and levels of self-control were related to rearrest among this sample of youth. Finally, as shown in models 3 and 4, the vast majority of these significant associations held when looking at the second measure of juvenile recidivism (readjudication). The one notable exception to this was that the main effect of empathy at admission on readjudication was not significant in the model that included the full list of control variables. 7 Overall, the results highlight the role of both ACEs and empathy in youth reoffending. We further probe the relationship among these variables using a series of models designed to assess the role of changes in empathy in the ACE-recidivism relationship.
Effect of ACEs and Empathy on Juvenile Recidivism (n = 11, 043).
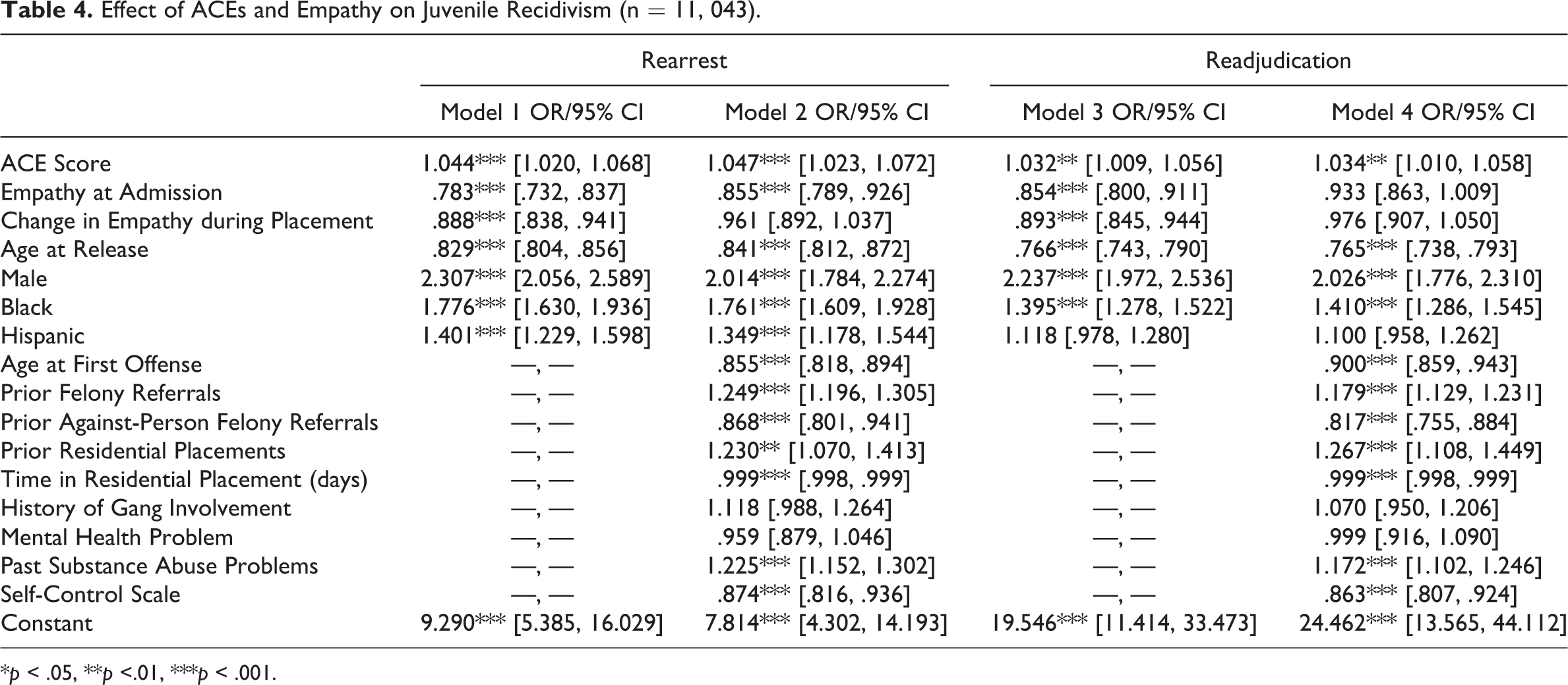
*p < .05, **p <.01, ***p < .001.
Moderating Effect of Changes in Empathy on the ACE-Recidivism Relationship
Turning to the results most central to the current research, Table 5 presents the estimates from six logistic regression models. Here, the effect of the focal variable, ACEs, on both measures of recidivism was estimated for a total of three groups (youth with small, moderate, and large changes in empathy during their time in residential placement). Importantly, although not displayed in tabular form, each of the models shown in Table 5 include the full range of control variables presented in earlier models. The results shown in Table 5 indicate that ACEs exerted a significant positive effect on both rearrest and readjudication among youth who fell within the bottom 25% of the change in empathy measure (i.e., had a decrease or the smallest increases in empathy). Specifically, for each additional ACE a youth had experienced, it was estimated that they had a 7.1% greater chance of being rearrested (Model 1) and a 5.5% greater chance of being readjudicated (Model 4). Among those with moderate changes in empathy during residential treatment, the effect of ACEs on both measures of recidivism was still significant, although this effect was reduced slightly (4.6% greater chance of being rearrested (Model 3) and a 3.8% greater chance of being redjudicated (Model 5)). However, for youth with the largest increases in empathy (top 25%), ACEs were no longer significantly related to rearrest or readjudication. This last finding is critically important as it shows gains in empathy during placement are able to dampen the negative effects of ACEs on subsequent recidivism.
Effect of ACEs at Different Changes in Empathy During Residential Placement.
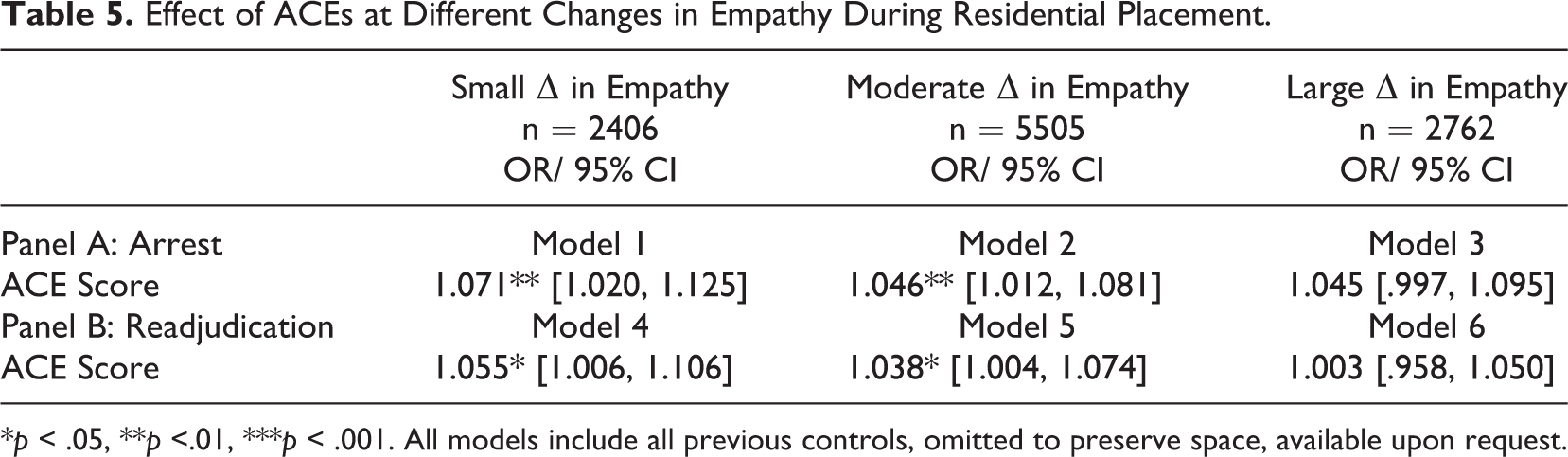
*p < .05, **p <.01, ***p < .001. All models include all previous controls, omitted to preserve space, available upon request.
The results shown in Table 5 are presented graphically in Figure 1. It is observed that the predicted probability of rearrest or readjudication following release increases as ACEs increase among all groups (based on changes in empathy) of youth assessed. However, the magnitude of the effect (positive slope) is smaller (flatter) among youth who saw greater gains in empathy during their time in residential placement, highlighting the potential role of empathy in moderating the effect of ACEs on juvenile recidivism.
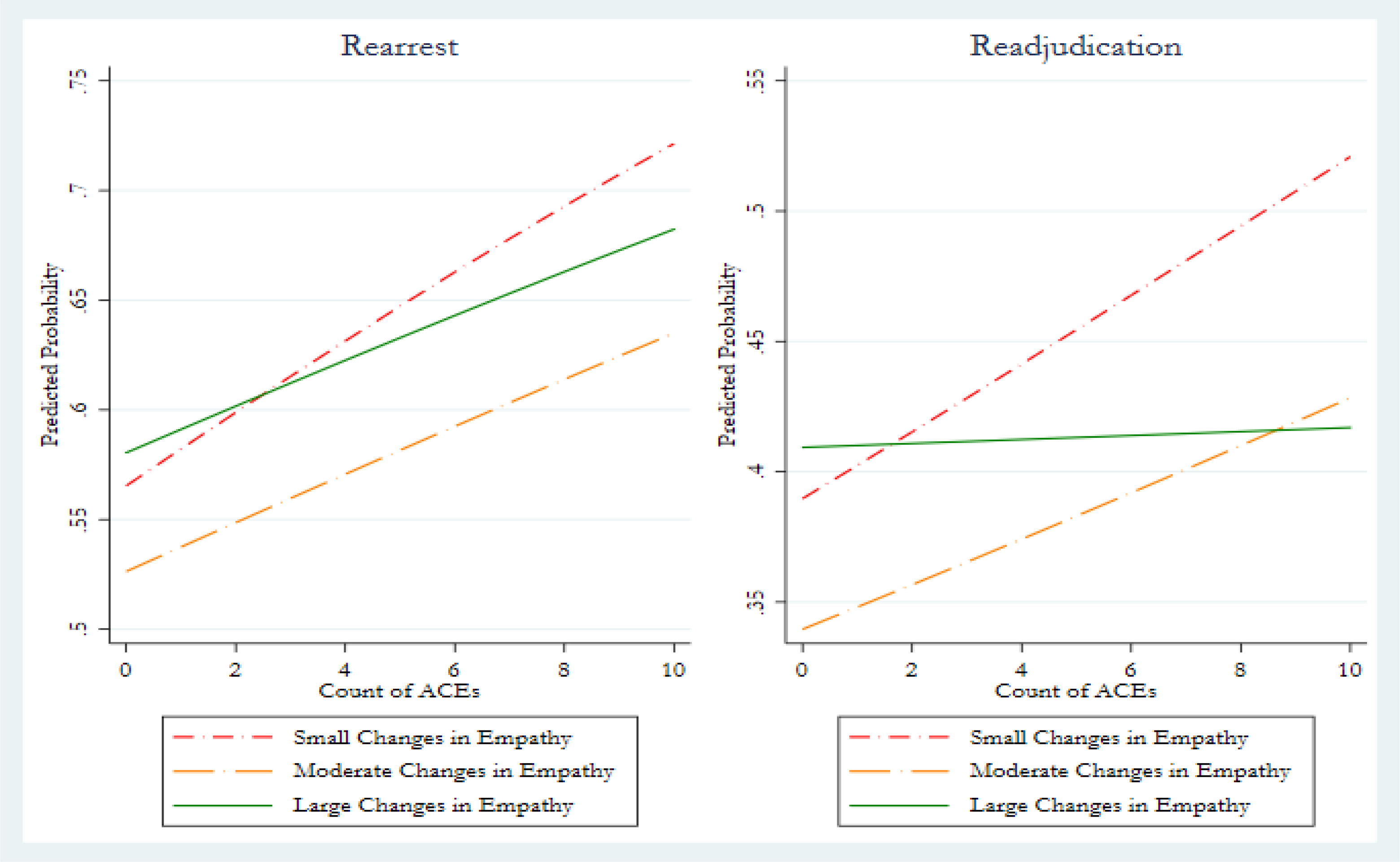
The Effect of adverse childhood experiences on juvenile recidivism given varying degrees of change in empathy.
Discussion
In this paper, we joined two strands of literature that focus on two key risk/protective factors of crime: empathy which protects against offending, and ACEs which increase the likelihood of crime. In doing so, we move beyond the prior research that has examined how these two concepts relate to offending by: (1) considering the extent to which ACEs are detrimental for empathy (2) and most importantly by examining the extent to which empathy, or more specifically, changes in empathy achieved during residential placement, are able to protect against the negative effects of ACEs. Using a large, statewide sample of serious adjudicated offenders in residential placement programs, our results generated three primary conclusions.
First, we found that a higher number of ACEs was related to less empathy, a finding that held after controlling for a number of variables that have been found to be related to empathy. Second, with respect to the predictors of recidivism (both rearrest and readjudication), we found that ACEs were significantly and positively related to both measures, adding to the dramatically growing body of work finding similar effects. Regarding empathy, our results showed that empathy at admission was related to both rearrest and readjudication in three of the four models examined (the exception was for readjudication in the fully specified model) while changes in empathy during placement was related to rearrest and readjudication in a baseline model. Lastly, and most importantly, our analysis showed that both small and moderate changes in empathy during residential treatment were unable to suppress the negative effect of ACEs on increasing the risk of recidivism. Most notably, we saw that when youth experienced large improvements in empathy during treatment, the effect of ACEs on both rearrest and readjudication was no longer significant. In short, these results show that (1) empathy is modifiable during residential treatment and (2) empathy can serve as a protective factor buffering the risk of ACEs on recidivism.
The results presented herein have important ramifications for juvenile justice policy. The negative repercussions of childhood maltreatment and cumulative traumatic exposure transcend domains of physical health (Felitti et al., 1998), neurological development (Anda Butchart et al., 2010), mental health (Perez et al., 2016), substance abuse (Dube et al., 2003), and offending during adolescence (Wolff et al., 2017) through middle adulthood (Craig et al., 2017). Finding that enhancing empathy can buffer the effects of ACEs on subsequent recidivism among serious offenders may be instrumental in increasing the efficacy of juvenile justice system rehabilitative efforts.
Interestingly, one of the primary intervention services provided across Florida juvenile justice residential programs is a victim impact curriculum, which includes chapters such as victim impact and restorative justice, introduction to harm, and the “ripple effect” of crime examining perceptions of levels of victimization that occur throughout different crime types in efforts to build empathy. 8 This intervention, Impact of Crime: Addressing the Harm to Victims and the Community, has demonstrated efficacy in decreasing risk factors in a randomized control trial study, including skills related to understanding the feelings of others (Baglivio & Jackowski, 2015). Importantly, youth who received at least 20 of the curriculum’s 24 objectives evidenced even greater risk reductions, meaning there most likely are dosage requirements to maximize efficacy (see also Baglivio, Wolff, Howell, et al., 2018), as well as potential fidelity and treatment quality components in intervention delivery (e.g., Baglivio, Wolff, Jackowski, et al., 2018). Residential service providers, and the juvenile justice systems that monitor service provision, would be wise to ensure interventions are being provided at sufficient dosages, and with fidelity to ensure all youth are benefitting from treatment. What is lacking is any examination of that curriculum, or any other victim impact curriculum, across levels of ACE exposure. That remains an important project to be undertaken.
Additionally, prior work has indicated that childhood maltreatment, especially within one’s household and at the hands of trusted family members, may lead to long-term emotional numbing (e.g., Kerig et al., 2012), which diminishes the capacity of the victimized individual to engage in perspective taking (arguably reducing empathy). If so, it is reasonable to suggest juvenile justice facilities that espouse a more correctional culture and milieu and/or have more extensive use of physical intervention from staff as a response to misbehavior may exacerbate lower levels of empathy, while more trauma-informed facilities, promoting the reduction of seclusion and restraint may foster empathy enhancement. Future work should examine these hypothesized potential facility-level characteristics that may be involved in the ACE-empathy-recidivism relationship. Lastly, future work might want to explore the variability that has been shown with respect to the strength of the effect of ACEs on crime. For example, while recent work has found that ACEs are a significant correlate of criminal behavior, the current findings demonstrated small effect sizes for ACEs on both empathy and recidivism, especially when compared to several of the control variables such as race/ethnicity and self-control. While the findings were nonetheless significant, as in line with prior research, it would be worthwhile to further explore the substantive nature of these effects. Recent research has found a nonsignificant effect of ACE on recidivism among a cohort of serious state incarcerated juvenile offenders (Craig et al., 2020; see also Baglivio, Wolff, Piquero, et al., 2015), suggesting the effects of ACEs on recidivism may not always be as strong among more serious juvenile offenders released from residential placements as has been found for community-based juvenile justice placements (e.g., Wolff et al., 2017). It may also be the case that ACEs are much more important for the onset of criminal behavior when compared to its persistence, a point made in the more general risk factor literature within the criminal career context (see Piquero et al., 2003). In short, while the current study examined recidivism among serious offenders, future work should explore whether levels of empathy moderates the relationship between ACE exposure and initial offending, thus warranting potential prevention efforts. If replication studies provide such confirmation, efforts can be made to include empathy enhancement strategies in education or after school settings to reduce the adolescents entering the juvenile justice system.
To be sure, while our work and the findings uncovered here are novel, some limitations about our research offer opportunities for future consideration. First, we had a one-year recidivism follow-up. The extent to which our empathy effects hold over longer periods of time awaits additional years of data collection. Second, given that there is some indication in the literature regarding potential gender differences in empathy (and how it relates to offending; Broidy et al., 2003), examination of the issues assessed herein across sex would be of interest. Third, space did not permit a detailed investigation of the extent to which the recidivism risk would vary by crime type. Given that empathy appears more strongly linked to violence (Jolliffe & Farrington, 2004) this awaits additional exploration. A fourth limitation concerns the ACE score. The ACE score’s binary measurement neglects the frequency, duration, or severity of each exposure, which have been found relevant in prior work (e.g., Smith & Thornberry, 1995). Furthermore, several critiques of the 10-item score have been levied, arguing for additional exposure types to be considered, such as witnessing violence in the community or systemic racism (Finkelhor et al., 2015). While many additional exposures are traumatic, the simplicity of the ACE score in only considering abuse, neglect, and household dysfunctions within the youth’s immediate family and home, make for more targeted policy implications and prevention/intervention initiatives than inclusion of community and societal exposures as well. Finally, some research has pointed to a slightly different pattern of relationships regarding ACEs. Greenberg et al. (2018), for example, report that traumatic experiences before late adolescence may be related to more empathy in adulthood (Greenberg et al., 2018). It may be that as youth age and continue to develop both emotionally and cognitively (Monahan et al., 2015), it is possible that they are better able to manage the stress of the past and learn better ways to cope, including by developing increases in empathy. This seems like an important topic of future research.
Conclusion
The results of our study call for optimism. Even among the most serious of juvenile offenders, those deemed by the juvenile courts as too dangerous to remain in the community, these youth can change, they can learn empathy, and this process can occur from juvenile justice system services. We are encouraged that empathy inhibits offending, and it helps to moderate traumatic early life experiences. Fortunately, the public shares our optimism and believes that it is never too late to help juvenile offenders turn away from a life of crime (Piquero et al., 2010) and that public is willing to support rehabilitation efforts over further incarceration for juvenile offenders (Nagin et al., 2006). Our charge as researchers and practitioners, therefore, is to strive for a more complete understanding of the methods and resources needed to intervene among offenders who were themselves first victimized and give them the tools and the chance to actualize their full potential.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.