
Abstract
Background:
Breast pumps can support breastfeeding continuation in the United States, where federal law permits only 12 weeks of unpaid maternity leave. Despite widespread use, research on individuals’ experiences with breast pumps is limited.
Methods:
An interdisciplinary research team developed a cross-sectional Qualtrics survey to explore the perspectives of breast pump users in the United States. Participants were recruited online over a 30-day period in 2021. Descriptive statistics summarized breast pump attributes valued by users, while open-ended responses were analyzed using content analysis.
Results:
A total of 641 participants completed 906 pump evaluations. Respondents were located across the United States, with the majority from the Midwest (42%) and South (29%). Most participants were non-Hispanic White (85%) and highly educated (60% held a master’s or doctoral degree). Eight thematic categories with positive, negative, and neutral/mixed experiences emerged: flange fit (user cited need for better sizing guidance and access to multiple sizes), mobility (wearable pumps improved flexibility; electric pumps required accessories for hands-free use), cost and insurance (coverage often excluded replacement parts or alternate flanges), efficacy (some pumps emptied breasts efficiently, others lacked adjustable suction or cycle), longevity (durability was valued for frequent use), manufacturer support (experiences from helpful to inadequate information available to maximize pump efficacy and fit), noise (quiet pumps were preferred), and discomfort (proper fit reduced pain, though soreness and nipple trauma were reported).
Conclusions:
Centering users’ experiences can inform improvements in pump design, insurance coverage, and professional support to reduce barriers to breast milk expression and promote breastfeeding success.
Introduction
Experts recommend exclusive breastfeeding for 6 months. 1 However, in the United States, exclusive breastfeeding directly from the breast is uncommon. Nearly 98% of mothers intend to use a breast pump, and 69% plan to begin pumping before their infant turns 6 weeks old.2,3 Limited paid maternity leave in the United States 4 contributes to early pump use to sustain breastfeeding among mothers returning to work. 3 Pumping may also be medically necessary for mothers of preterm or hospitalized infants. 5 Additionally, breast pumps can relieve engorgement, help manage milk supply, support milk expression for later feeding, or allow others to feed the baby. 2
Breast pumps may extend breastfeeding duration.6,7 A cross-sectional analysis of data from the Centers for Disease Control and Prevention’s Pregnancy Risk Assessment Monitoring System from four U.S. states (2016–2021) found that mothers who used a breast pump had a 37% lower likelihood of breastfeeding cessation and breastfed for an average of 21 weeks longer than those who did not. 6 This benefit was greatest among mothers who were non-Hispanic Black, 6 suggesting pump access may reduce disparities in breastfeeding duration.
As breast pump technology, policy, and social norms evolve, exploring perspectives of pump users is important. Bartels et al. (2020) identified portability, ease of use, low weight, fast milk extraction, comfort, quietness, and discretion as important features. 8 Becker (2021) emphasized the need to examine pumping experiences in the context of varying user needs, shaped by factors such as pumping frequency and necessity. 9
Qualitative studies have highlighted challenges with pumping, including inconsistent professional guidance, confusion about effective pumping techniques, and heightened maternal concerns about the adequacy of milk supply.10,11 Some mothers also describe pumping as time consuming and disruptive to infant bonding. 11 These findings illustrate the complex experiences surrounding pumping.
Federal policies have aimed to reduce barriers to milk expression. The Patient Protection and Affordable Care Act (ACA) and the Providing Urgent Maternal Protections for Nursing Mothers (PUMP) Act were signed into law in 2010 and 2022, respectively.12,13 These policies mandated insurance coverage of breast pumps and lactation counseling, and required employers to make accommodations for milk expression.12,13 Although these policies are associated with improved breastfeeding outcomes, 14 implementation varies. 15
Neither the ACA nor the PUMP Act specifies standards for the type, quality, or functionality of breast pumps to be covered. Therefore, insurance coverage varies substantially from private insurance covering broad categories of pumps, for example, a manual or standard electric pump (a nonhospital grade) 16 to more specific state-level guidance, such as New York’s minimum specifications for Medicaid pump reimbursement. 17 Despite these efforts, access to efficient, well fitting, portable, and durable pumps often hinges on insurance coverage and personal financial resources.
Breastfeeding and human milk researchers have identified the need to prioritize alternative modes of human milk expression. 18 This study aimed to explore individuals’ experiences with breastmilk expression using a breast pump, focusing on factors influencing access, satisfaction, and continued use.
Methods
We conducted a cross-sectional online survey of individuals in the United States who had used a breast pump within the past 2 years. The survey assessed perspectives on pump efficiency (i.e., timeliness and completeness of milk extraction), portability, fit, manufacturer support, product longevity, and factors influencing access and affordability. Participants identified their most valued pump attributes. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist for cross-sectional studies guided our study design and reporting. 19
Survey participant recruitment and consent
Participants were recruited via online platforms, including Dr. Milk Facebook group, the Institute for the Advancement of Breastfeeding and Lactation Education (IABLE) listserv, and Facebook groups serving underrepresented populations. In addition, printed flyers were distributed in lactation medicine clinics. Digital and printed flyers included a QR code or URL linking to the Qualtrics survey. Email invitations also contained study details and a link to the survey.
Before beginning the survey, participants reviewed an informed consent statement and indicated agreement by clicking “Next.” No signatures or personally identifying information were collected to ensure anonymity. At the end of the survey, participants were offered a separate link to enter a gift card drawing for one of eight $25 gift cards.
This study was deemed Exemption 2 by the Institutional Review Board at Northern Illinois University.
Inclusion criteria
Inclusion criteria included: having an infant and experience using a breast pump within the past 2 years; being 18 years of age or over; and being fluent in English.
Survey instrument
An expert committee convened by IABLE and Northern Illinois University designed the survey. The team included two breastfeeding medicine physicians who were International Board-Certified Lactation Consultants (IBCLCs) and certified by the North American Board of Breastfeeding and Lactation Medicine (NABBLM-Cs), an advanced practice nurse who was also an IBCLC, two researchers, and two engineers. An initial version of the survey was pilot tested (n = 221), and both qualitative and quantitative feedback informed revision to improve content and face validity.
Open-ended questions were added to explore pain, flange size fit, insurance challenges, and pump-related expenses. The revised instrument also allowed participants to evaluate a second pump, if applicable. The final survey included 36 closed-ended questions (Likert-scale, binary, categorical, sliding scale) and 14 open-ended questions, including 10 optional free-text comment boxes and 4 unrestricted paragraph fields (see Supplementary Data).
Surveys were self-administered online in English. Participants began by rating pump attribute importance (e.g., quietness, cost, portability) using a 0–100 sliding scale, where 100 represented the most important quality. Next, they selected from a list of 37 pumps (with images). An “other” option allowed for manual pump entry. Quantitative responses included a mix of 5-point Likert scales (Strongly Agree to Strongly Disagree) and binary response options (e.g., Yes, No), with many having optional free-text comment boxes. Demographic and contextual data included race/ethnicity, education, zip code, insurance coverage, pumping expenses, need to pump while at work, and work environment characteristics. Pump use was assessed with the item, “Did you pump exclusively or for a period of time?” with response options including: “exclusively pumped (no breastfeeding),” “pumped several times a day,” “pumped several times a week,” “pumped sporadically, and other (free text).”
Data extraction
Data were collected via Qualtrics over a 30-day period (September to October 2021). Incomplete surveys were excluded from analysis.
Pump classification
All pumps listed and manually entered pumps were reviewed and categorized by an IBCLC as follows: Hospital Grade Electric, Electric (“standard,” nonhospital grade, singer-user breast pump requiring a battery or electrical outlet), Wearable Electric (single user battery-operated breast pump designed to fit inside a bra for hands-free use), and Hand Pump (manually operated breast pump that uses hand compression to create suction without batteries or electricity). Codes were used to blind pump brand names.
Statistical analysis
Quantitative data were analyzed in R version 4.2.3. 20 Descriptive statistics summarized sociodemographic characteristics and attribute ratings. Other quantitative data were analyzed and used for contextual information, but are not included in this article.
Qualitative data analysis
Fourteen open-ended questions were analyzed using content analysis 21 in NVivo 15.1.0 (QSR International Pty Ltd., Burlington, MA). An initial deductive codebook was based on survey constructs (e.g., flange fit, manufacturer support). Inductive codes were added for emergent concepts. Descriptions were developed for each code, and multiple codes were applied to some excerpts. The research team met regularly throughout the coding process to refine the codebook, resolve discrepancies, and build consensus on emerging themes. Reflexivity was supported through ongoing team discussions, allowing us to consider how our diverse clinical, research, and professional backgrounds could influence data interpretation. Consensus was achieved for all coded data.
Results
Data from 641 participants were analyzed. Geographic distribution included 42% from the Midwest, 29% from the South, 15% from the West, and 10% from the Northeast, with 4% of respondents not reporting their location. All states were represented in the sample, except Idaho, Montana, North Dakota, and Delaware. Of the participants, 376 evaluated one pump, while 265 participants evaluated two pumps, resulting in 906 pump evaluations. Figure 1 shows the participant flow and pump evaluations.
Selection criteria applied to determine the population in the analysis.
Sociodemographic characteristics of survey participants
Table 1 presents the study population’s demographic characteristics. The majority of participants were non-Hispanic (92.4%) and Caucasian/White (85%), followed by East Asian (2.7%) and African American/Black (2.5%). Most participants held a master’s or doctoral degree (60%). Table 2 presents participants’ experience with breast pumps, costs, and work environment. The majority pumped while at work (82%), with nearly half (49%) working in health care. Frequent pump use was common, with 18% exclusively pumping and 51% pumping several times per day. While 69% received a pump through insurance, 30% reported spending over $200 USD on pump supplies.
Demographic Characteristics of Study Participants (N = 641)
Participant Experience with Breast Pumps: Frequency, Work Environment, Insurance Coverage, and Related Costs (n = 641)
N/A, not available.
Participant-Reported Breast Pump Experiences: Ranked Categories, Descriptions, and Illustrative Quotes (n = Number Coded Responses, % of Total Coded Responses)
Note that some excerpts were assigned multiple codes. Categories reflect themes identified from a total of 3,022 coded responses across 906 pump evaluations submitted by 641 participants. Counts represent the number and percentage of coded responses per category. Sentiment classifications (positive, negative, neutral) are presented as proportions of the total responses for each respective category. Pumps were classified into four types: Hospital Grade Electric, Electric (“standard,” nonhospital grade, single-user breast pump and requiring a battery or electrical outlet), Wearable Electric (single user battery-operated breast pump designed to fit inside a bra for hands-free use), and Hand Pump (manually operated breast pump that uses hand compression to create suction without the use of batteries or electricity). FSA, flexible spending account; n, number of coded responses; %, percentage of all coded responses; WIC, Women, Infants, and Children.
Quantitative findings on pump attributes rated most valuable/important to participants
Pump efficiency received the highest average score (89), followed by portability (82), ease of use (81), easy to clean (77), and whether the pump was covered by insurance (71). Attributes rated lower included mobility (ability to move while pumping) (64), noise level (60), and cost of the pump (57).
Characteristics of electric breast pumps
Figure 2 displays the number of evaluations completed across 31 distinct pump brands, organized by pump classification. The majority of evaluations were for electric pumps (69%), followed by wearable pumps (23%), Hospital-grade (5%), and hand pumps (3%), were evaluated less frequently.
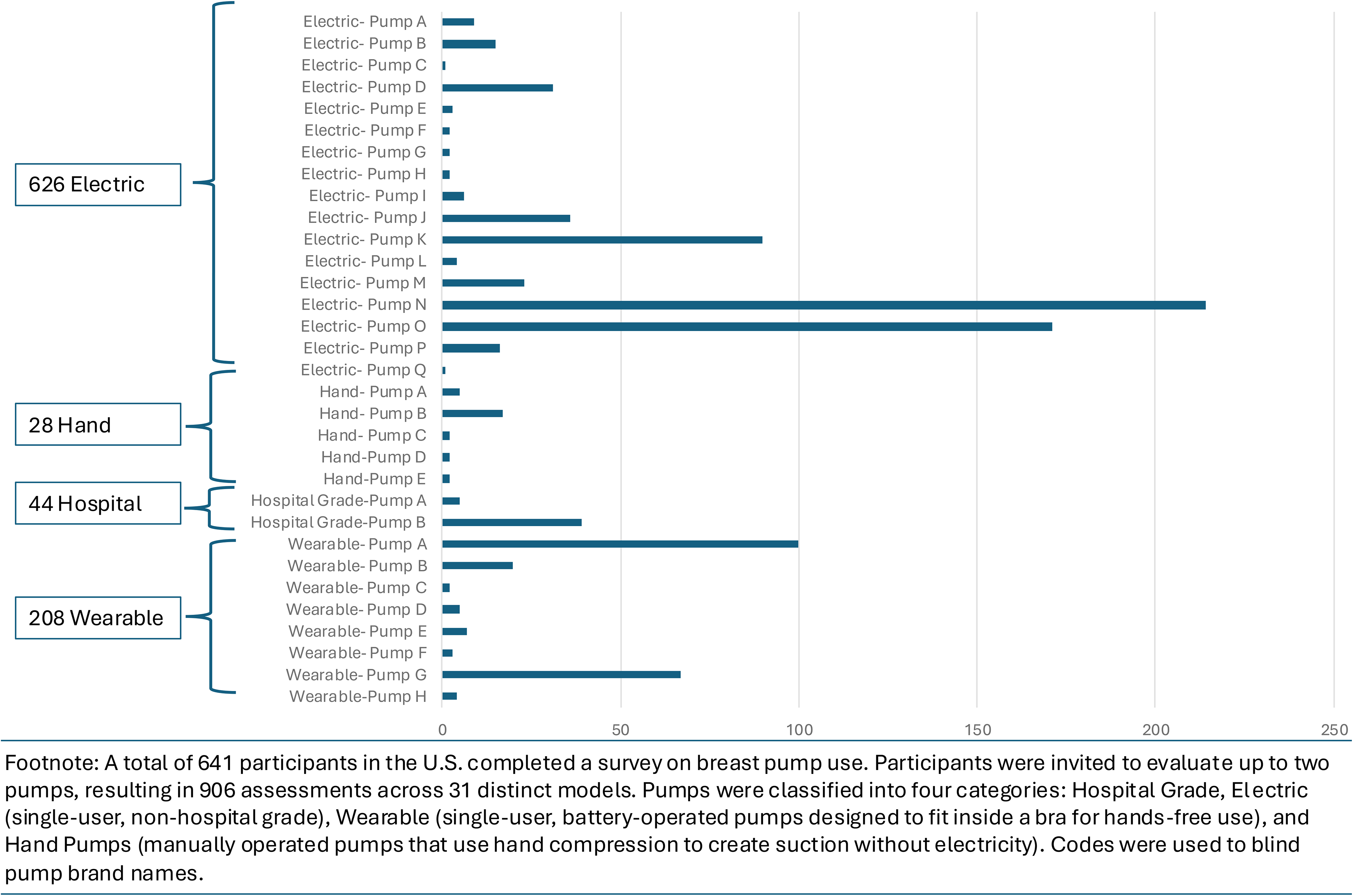
Number of breast pump evaluations organized by classification (Electric, Hand, Hospital Grade, and Wearable).
Qualitative experiences
In a content analysis, nine main categories were identified, including: (1) breast pump flanges; (2a) mobility with electric pumps; (2b) mobility with wearable pumps; (3) cost and health insurance coverage; (4) efficacy at “emptying” the breasts; (5) longevity of the pump over time; (6) manufacturer support; (7) noise; and (8) discomfort and pain related to the pumping. These categories are presented in order of frequency of responses and summarized in Table 3.
Category 1: Breast pump flanges
Flange fit was a common issue, with many reporting that insurance rarely covers multiple flange sizes. Many questioned the rationale for “standard” flange sizes included with pumps. Participants reported paying out of pocket for alternative sizes to improve comfort or milk output. As one electric pump user explained, “For this pump, I used what it came with and didn’t think I needed to change it (aka trusting the manufacturer). This led to inefficiency and harm.” A recurring statement was using “trial and error” to determine an appropriate fit, with many seeking advice from online communities or social media. Of the comments related to flange fit and sizing, about 26% of respondents reported receiving professional fitting assistance from a lactation consultant or health professional. Among those receiving professional help, over 90% were positive. One individual noted, “It would be INCREDIBLY helpful to have someone you can consult with to find a proper fitting pump so you know what style/brand/flange sizes work best for you and you can have a plan in place.”
Category 2: Mobility with electric and wearable pumps
Qualitative data were collected from participants who had experience using both traditional breast pumps that require an outlet and wearable breast pumps that operate using a battery. Participants using electric pumps expressed frustration with being “stuck” when using pumps that require connection to a wall outlet. Wearable pumps were viewed positively for mobility, but concerns were raised about leaking or milk spillage when not properly fitted.
Category 3: Cost and health insurance coverage
While many received a pump through insurance, others reported lack of coverage for replacement parts, or alternative flanges or the need to purchase a second pump. Approximately 30% of participants reported spending more than $200 USD on pump-related accessories and supplies.
Category 4: Efficacy at “emptying” breasts
Participants valued pumps that emptied breasts efficiently. Approximately 13% of overall responses were associated with efficiency, of which 75% were overall positive, while the remaining 18% described frustrations with suction strength and incomplete emptying. Many participants reported that their pumps emptied “well,” “quickly,” or “better than others,” especially when suction felt “natural” or mimicked infant feeding. Concerns were raised about wearable pumps, with some reporting that mobile collection cups reduced suction compared to standard flanges, resulting in incomplete emptying.
Category 5: Longevity
Most participants reported a positive experience with longevity, with one electric pump user stating, “It’s excellent. I’m an exclusive pumper and I used it for a bit over a year. Was pumping 8 times a day in the [beginning].” Conversely, about 88% participants reported issues like pump or battery failure or broken parts. One wearable pump user shared, “Very finicky. Multiple problems with broken parts that were expensive to replace.”
Category 6: Manufacturer support
Participants described relying on manufacturer support to navigate flange sizing and device function. One electric pump user shared, “I used the manual or resources online to determine fit and tried a few flanges to see what worked best. I needed a different size early and late in my year of pumping.” A total of 65 respondents reported that their pump broke. Most described the manufacturer as responsive, with replacements covered under warranty and shipped promptly. An electric pump user shared, “They replaced it, but I was lucky since [I] had a backup [while] waiting on it to ship.”
Category 7: Noise
Pump noise was important, particularly for those needing to pump discreetly at work or while their infant was sleeping. Quite pumps were preferred, while noisy ones caused dissatisfaction.
Category 8: Discomfort and pain
Pain was often reported during initial use, when suction settings were too high, or flange fit was incorrect. Respondents emphasized a learning curve to improve comfort. However, others experienced persistent discomfort, particularly with strong suction or if preexisting nipple damage was present.
Discussion
This study explored breast pump users’ experiences, revealing eight key themes: flange fit, mobility, cost and health insurance coverage, efficacy at emptying breasts, longevity, manufacturer support, noise, pain, and discomfort.
Participants frequently expressed frustration with flange fit. Standard flanges (21, 24, and 28 mm) do not accommodate for large anatomical variation between individuals. 22 Participants described receiving conflicting information from commercial sources and valued professional support for flange fit. Anders et al. (2024) demonstrated greater comfort and milk output when users were fitted with smaller flanges. 22
Consistent with our findings, mobility is highly valued by pump users. 8 Wearable pumps were favored for mobility, especially among working parents. Among 542 physicians, wearable pumps supported shorter lactation breaks (p < 0.00001) and increased the likelihood of meeting lactation goals (p = 0.005). 23
Costs and insurance coverage emerged as an important factor. Despite ACA mandates requiring coverage for pumps, 14 insurance often excludes additional flanges or supplies. It is unclear whether the out-of-pocket expenses from our sample population reflect financial necessity or the ability and willingness to pay for higher quality pumps and related supplies. Kapinos et al. (2018) reported that reductions in insurer pump reimbursement rates may have led to the availability of lower cost, lower quality options. 24 Beyond the costs of pumps and supplies, time spent pumping has also been cited as a barrier, 25 potentially compounding financial and logistical challenges for families with limited resources. To address these challenges, the U.S. Breastfeeding Committee has issued guidance for health insurance payers that includes providing families with two breast pump kits per birth event and appropriate supplies. 26 Adopting such policies could ease the financial burden and improve equitable access.
Individuals conveyed diverse experiences on pump efficiency. A systematic review found that maternal perceptions of the efficiency/effectiveness of breast emptying were mentioned in only 3 out of 15 trials. 9 In contrast, our findings suggest that pump efficiency was a frequently reported concern. More clinical studies exploring user perspectives on pump “efficiency” seem warranted. Such research could advance more equitable lactation outcomes, particularly for families with fewer resources or less access to high-quality pumps.
Participants noted longevity as an important attribute, especially for frequent or exclusive breast pump users. A durable and consistently functioning pump supports continued milk expression, which is essential for meeting expert recommendations for exclusive breastfeeding.1,27 Pump longevity also aligns with the national public health goals, including the Healthy People 2030 breastfeeding objectives, which emphasize improvements in both breastfeeding duration and exclusivity. 28
Experiences with manufacturer support varied. About half of the participants reported contacting manufacturers for replacement parts or malfunctioning pumps. A review of breast pumps cleared by the U.S. Food and Drug Administration (FDA) between 1976 and 2018 identified 135 devices, including both manual and electric pumps. 29 During this time, 4,656 adverse event reports were submitted to the FDA related to these devices, ranging from product failures and quality problems to serious safety concerns. 29 Although this number does not reflect the overall incidence of such problems among all pump users, it highlights the potential for issues that can interfere with milk expression. Leiter et al. emphasized potential underreporting of pump issues, 29 leaving families to troubleshoot technical issues independently. These challenges underscore the need for accessible, responsive manufacturer support and the need for more than one pump to ensure uninterrupted milk expression.
Although pump noise was mentioned less frequently, it may still contribute to overall satisfaction with a pump. Research on lactating mothers in the United States found that preferences for “low-noise” breast pumps varied. 8 Breast pump noise was relatively important in one subgroup of mothers, while it was irrelevant for others. 8
Several participants reported experiencing pain related to poor flange sizing or underlying nipple pain. Improper flange fit may lead to pain and nipple trauma, 30 which is concerning given the perception of pain is a leading cause of breastfeeding cessation.31,32 Studies have shown that tools like the Flange FITS™ Guide can significantly improve both comfort and milk output. 22 A systematic review of breast pump interventions found that “comfort” or “pain” was mentioned in 13 out of 15 maternal viewpoint trials. 9 In a U.S. survey (n = 264), about half of respondents reported nipple pain and general discomfort with pump use. 8 A randomized control trial by Francis and Dickton 33 comparing breastfeeding, hand expression, and pumping found significantly higher pain scores and localized inflammation with pumping. 33 These findings highlight the need for improved pump design, better flange fitting resources or professional support for fit, and research focused on improving comfort with pumping.
Limitations
This study has several limitations. First, the sample was predominantly non-Hispanic White, highly educated individuals living in the United States, which limit the generalizability of findings to more diverse populations. Prior research has shown that individuals who are younger, with lower income or educational attainment, are unmarried, enrolled on Medicaid, or who identify with racial and/or ethnic populations other than non-Hispanic White are less likely to use breast pumps (p < 0.001). 6 Additionally, exclusive pump users are more likely to have public insurance or be uninsured, have lower educational attainment, deliver via cesarean section, report low income, and participate in the Special Supplemental Nutrition Program for Women, Infants, and Children. 5
Recruitment through platforms such as Dr. Milk and the IABLE listserv likely contributed to the overrepresentation of health care professionals and individuals with advanced degrees, introducing selection bias. Nonetheless, 18% of study participants reported pumping exclusively, and 51% reported pumping frequently, providing meaningful perspectives on pump use.
Additional limitations include the absence of infant health characteristics (e.g., gestational age, prematurity), which may influence pumping behaviors. We were also unable to examine changes in pumping practices over time, for example, we are unsure if those who reported “exclusive pumping” or “pumping several times per day” were practicing exclusive direct breastfeeding prior to returning to work. Insurance type was not stratified by public and private insurance sources, limiting our ability to draw conclusions about how insurance impacts pump access. Finally, the cross-sectional design may introduce recall bias, as participants were asked to reflect on past experiences.
Future directions
Future research should prioritize recruiting more diverse populations to capture a broader spectrum of experiences. Although we examined insurance coverage generally, future studies should differentiate between public and private insurance to better understand how coverage type affects access to pumps and related out-of-pocket expenses. Comparative studies are warranted to evaluate milk transfer efficiency and comfort across various modalities with an added focus on the gestational age and characteristics.
Notably, the National Academies of Sciences, Engineering, and Medicine (2025) recently called for the development and testing of Consumer Assessment of Healthcare Providers and Systems measures to quantify the accessibility, timeliness, and patient centeredness of lactation and breastfeeding care and coverage for support and supplies. 34 Such metrics could help identify gaps and improve the delivery of lactation services and insurance benefits.
Conclusion
Centering users’ perspectives is essential for improving pump design, professional support, and insurance coverage needed to express breastmilk. Pump efficiency, portability, and ease of use were the most valued pump attributes by respondents. Qualitative analysis identified eight categories shaping users’ experiences including: flange fit, mobility, cost and insurance coverage, efficiency, longevity, manufacturer support, noise, and discomfort or pain. Many participants described insurance-related barriers, including limited coverage for replacement parts and alternative flange sizes. Having access to professional support for fit improved experience with comfort and efficiency. These insights can inform education for lactating individuals and health professions, guide pump design, and support health care policy efforts to reduce barriers to expressing breastmilk.
Authors’ Contributions
A.E., J.A.P., M.D., L.M., A.M., and J.D.R. contributed to the instrument and study design. A.E. and L.M. supported participant recruitment. All authors supported data analysis and synthesis of findings. M.A.T. and J.A.P. led the initial draft of article, and all authors critically appraised and revised the content. All authors approved the final submitted version and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgments
The authors would like to thank Rachel Gordon, PhD, and Madeleine Sigman-Grant, PhD, for their thoughtful review of the article.
Funding Information
This study was supported by funding from Northern Illinois University, College of Health and Human Sciences. Additional funding for M.A.T. was provided by the Scholarship for Bavarian Gender Equality Fund (Bayerische Gleichstellungs Förderung) for postdoctoral researchers as well as by LMUexcellent, funded by the German Federal Ministry of Education and Research and the Free State of Bavaria under the Excellence Strategy of the German Federal Government and the Länder.
Disclosure Statement
J.A.P. serves as an instructional consultant for the IABLE and is a member of the Board of Editors for the Journal of Nutrition Education and Behavior. A.E. is the President and CEO of the nonprofit organization IABLE. L.M. serves on the Executive Board of the North American Board of Breastfeeding and Lactation Medicine. L.S. is an instructional consultant and board member for IABLE. The remaining authors report no conflicts of interest.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.