
Abstract
Introduction:
Hand expression (HE) of breast milk enables milk collection at any stage of lactation. Its use is widely recommended for breastfeeding mothers. However, evidence surrounding utilization, outcomes, and experiences using HE is limited.
Objective:
This scoping review aims to broadly examine the literature describing patient and health care provider experiences, utilization, and clinical outcomes of HE of breast milk.
Methods:
We conducted systematic searches in MEDLINE, Embase, Web of Science, Scielo, and DialNet. We included both primary research and quality improvement reports. Four reviewers screened all papers for eligibility, read the full text of included studies, and extracted data.
Results:
Of the 620 reports identified, 118 studies from 30 countries met eligibility criteria. Studies found high rates of familiarity with HE but variable rates of use. Most women expressed favorable views and experiences with HE. Multiple successful methods of teaching HE to lactating women and health care professionals were described. Many studies report teaching HE within wider interventions, such as antenatal milk expression programs and initiatives to increase breastfeeding among preterm infants. Most reports of breastfeeding outcomes, breast milk volume, and constituents gave mixed results, although HE in the first days postpartum was often associated with improved outcomes. No studies were found testing the use of HE for particular breast conditions such as mastitis or hyperlactation.
Conclusions:
While HE is generally favorably experienced by women and health care providers and may improve breastfeeding outcomes, further research is needed on HE as a primary exposure to better apply it in clinical lactation management.
Introduction
Hand expression (HE) is a technique that enables pregnant and lactating individuals to remove breast milk at any stage of lactation, and in particular in the first days postpartum. Records dating back to the year 100 CE (common era) show that it was used to relieve pressure and increase breast milk production, and it has been discussed in medical literature since the 1940s. 1 In recent years, there has been an upsurge in the practice of prenatal colostrum expression, most often performed with HE. At the same time, the growth of pump accessibility in many countries shifted research, clinical, and patient interests toward electric pumping.
HE is recommended widely. The World Health Organization emphasizes that HE requires no costly equipment and thus can be done in low-income countries and in settings such as emergencies and natural disasters.2–5 Baby-Friendly USA recommends that HE be taught to all mothers at Baby-Friendly Hospitals in the United States. 6 HE is often used in the immediate postpartum period to establish milk production and can be used at any time during lactation.7,8 The Academy of Breastfeeding Medicine (ABM) recommends HE in 17 of their 34 published protocols as an intervention or skill in clinical scenarios, including such issues as management of lactation after late preterm delivery, mastitis management, and hyperlactation.9–25 However, most of these cite only a few published papers on HE,26–28 suggesting that the evidence base may be limited for specific clinical scenarios addressed in each protocol, such as mastitis.
While HE is widely recommended, clinical guidelines and study protocols utilizing it rarely reference evidence regarding mothers’ experiences or rates of utilization of HE, best practices for teaching HE, or the utility of HE in particular clinical scenarios. Given this gap between clinical recommendations and evidence, the objective of this scoping review is to broadly examine the literature describing patient and health care provider experiences, utilization, and clinical outcomes of HE of breast milk and to identify gaps in knowledge for further research needs.
Methods
Study design
We conducted a systematic search using a scoping review methodology to review the published literature regarding HE of human milk (HM). The authors chose to conduct a scoping review because there are no published reviews for HE outcomes, other than volume and composition. 29 Scoping reviews differ from other systematic reviews in their breadth and are often used as a precursor to meta-analyses. Scoping reviews can include multiple study designs, outcomes, and interventions in order to compile a comprehensive understanding of the topic and state of research on it. They typically do not assess the quality of included articles. The authors chose a scoping review to characterize the existing literature regarding patient and health care provider experiences, utilization, and clinical outcomes of HE in order to identify gaps in knowledge, trends in use, and outcomes with HE, and areas requiring further research. We utilized the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISAM) Extension for Scoping Reviews (PRISMA-ScR) checklist alongside the JBI Manual for Evidence Synthesis to guide protocol development.30,31 There is no published protocol.
Search strategy
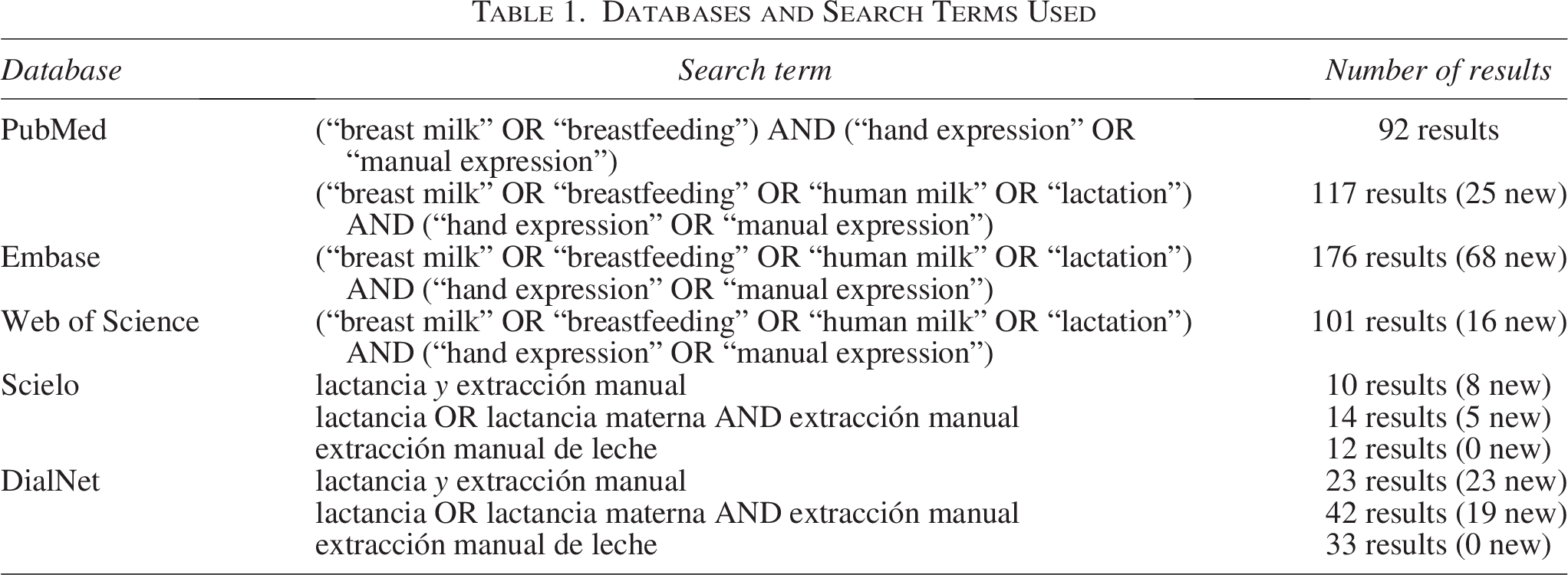
We conducted an initial search of MEDLINE (PubMed) to identify articles related to the topic. The text of titles, abstracts, and index terms of all articles was analyzed to develop a full search strategy. We then conducted a second search using the additional keywords (Table 1) across MEDLINE, Embase, Web of Science, Scielo, and DialNet: (“breast milk” OR “breastfeeding” OR “human milk” OR “lactation”) AND (“hand expression” OR “manual expression”), in English; (“lactancia” OR “lactancia materna”) AND (“extracción manual” OR “extracción manual de leche”) in Spanish.
Databases and Search Terms Used
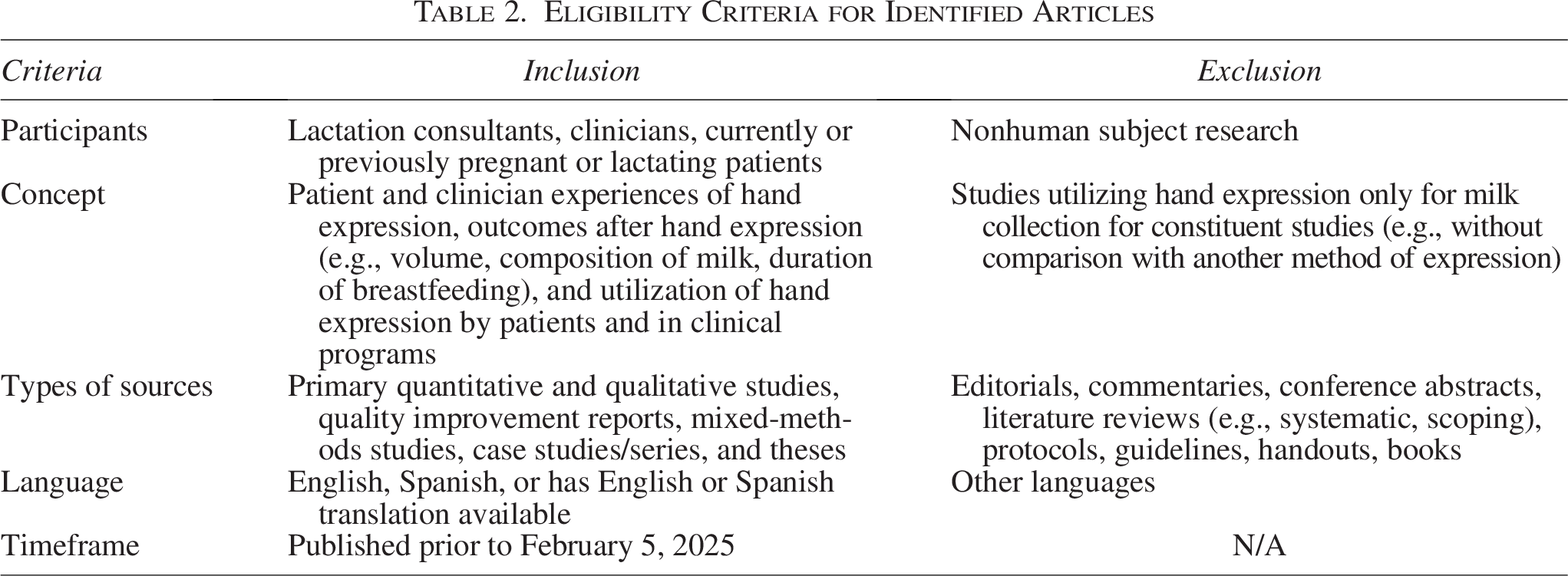
Included studies (Table 2) were those that had an outcome related to patient or health care worker experience of HE or in which HE was the outcome, intervention, or part of a larger intervention. 29 We included primary qualitative, quantitative, and mixed-methods studies, quality improvement (QI) reports, case studies/series, and theses reporting primary research. We excluded editorials, commentaries, conference abstracts, literature reviews, clinical guidelines, and handouts or other nonempirical, nonprimary sources. For feasibility purposes, we included articles in English or Spanish (reviewers K.R.S. and M.J.P. are fluent in Spanish) and those that had an English translation readily available. Sources were all published prior to February 5, 2025, with no beginning date, as no prior scoping review had been published on this topic. Articles were not limited by contexts such as location or population.
Eligibility Criteria for Identified Articles
Evidence selection
The authors reviewed all sources identified from the searches and removed duplicates. Prior to source selection, a pilot test was conducted to ensure the eligibility criteria were clear and well defined. Two reviewers independently reviewed 25 randomly selected sources and determined whether they met eligibility criteria. The reviewers agreed on eligibility in 100% of cases, above the recommended threshold of 75% interreviewer agreement. 30
The authors then independently screened titles and abstracts to determine eligibility and then moved on to full-text review, at which time eligibility was confirmed. The reference lists of selected sources, as well as relevant ineligible sources (e.g., ABM protocols, commentaries, systematic reviews), were screened for additional sources.
Data extraction and analysis
The four reviewers independently extracted data from each source into a shared spreadsheet. Extracted data included year of publication, country of origin, aims, sample size, participant characteristics, methodology, intervention(s), outcome(s), and key findings related to the scoping review objective (HE). The authors met to reach consensus regarding extracted data and key findings. The studies were then further evaluated for common themes to help guide the presentation of the results. Throughout the text, we refer to research participants’ genders as they are reported in each study. In line with the ABM’s position, we acknowledge the diverse gender identities of individuals with the capacity for lactation. While we recognize the limitations of solely using female-specific terminology in capturing this inclusivity, we adopt these terms for clarity and consistency, particularly reflecting the populations included in cited studies. 32
Results
Studies identified
Of the 620 identified articles, after removing duplicates and adding articles identified from reference lists, 118 articles were found to be eligible (Fig. 1). Articles were excluded for no mention of HE, no differentiation between methods of milk expression, not meeting inclusion criteria, no full text available, and/or not available in English or Spanish.

Search results and process of inclusion of studies.
The final set of 118 papers included randomized controlled studies, cross-sectional survey studies, pre–post intervention studies, qualitative and mixed-methods studies, observational retrospective and prospective cohort studies, QI reports, Delphi technique, and case reports/series. Studies were from 30 different countries (Fig. 2), with the most from the United States (30.5%), Australia (11.0%), and India (10.2%); overall 34.7% were from low- or middle-income countries (Table 3). Studies were conducted in various periods and settings: prenatal (antenatal milk expression), the birth hospitalization, and other preterm or term hospitalizations, and in community settings. Below, we briefly summarize studies in antenatal, neonatal intensive care unit (NICU), and community settings and then give overall findings for patient and health care worker experiences and clinical outcomes (Table 4).
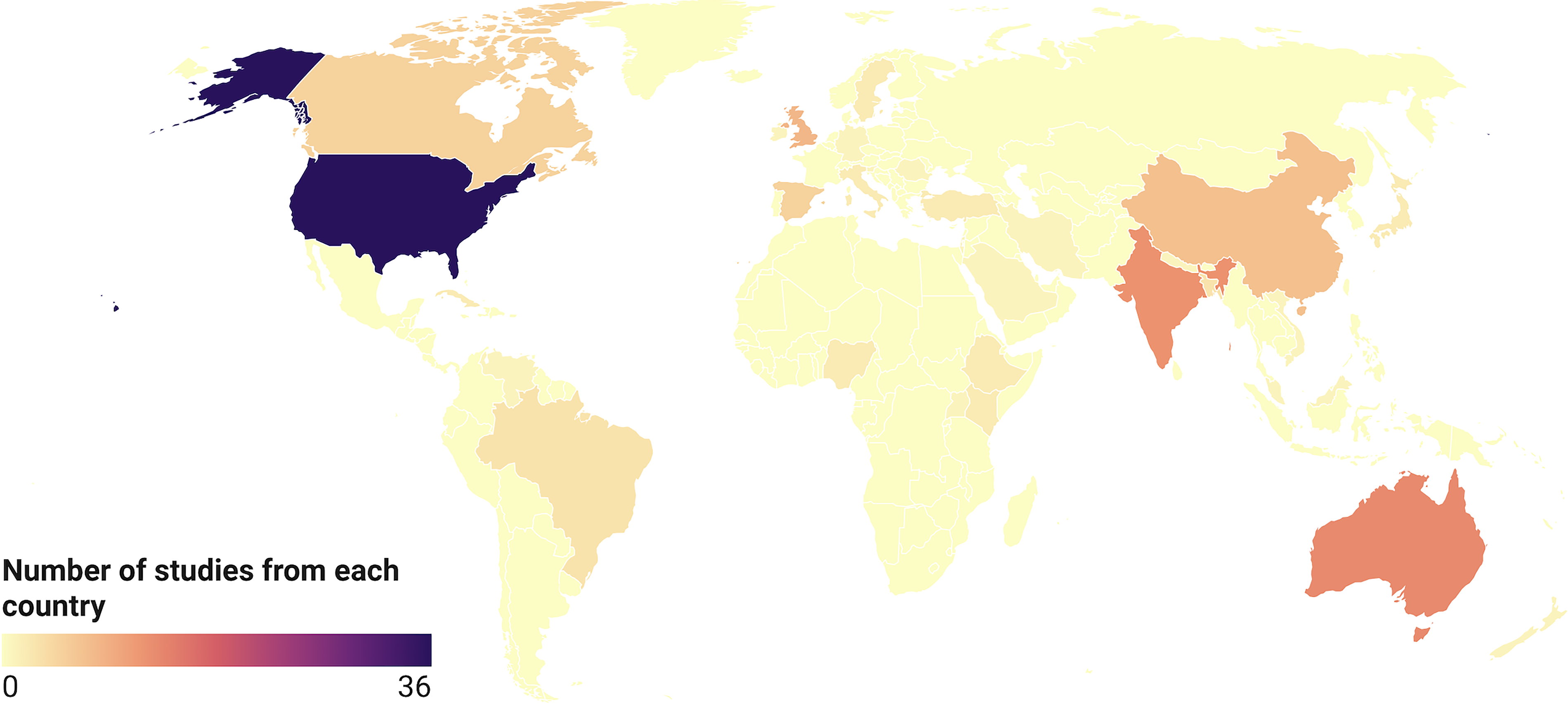
Countries in which included articles (n = 118) were conducted, with the number of included articles from each country represented by a gradient of green (white = 0 articles, darkest green = 36 studies).
Countries in Which the Included Studies (n = 118) Were Conducted

One study each: Germany, Iran, Israel, Malaysia, Nepal, New Zealand, Romania, Saudi Arabia, Slovenia, Uganda, Venezuela, and Vietnam.
Two studies each: Cuba, Ethiopia, Italy, Japan, Kenya, Nigeria, Sweden, and Turkey.
Themes Regarding Hand Expression Extracted from the Included Studies (n = 118)
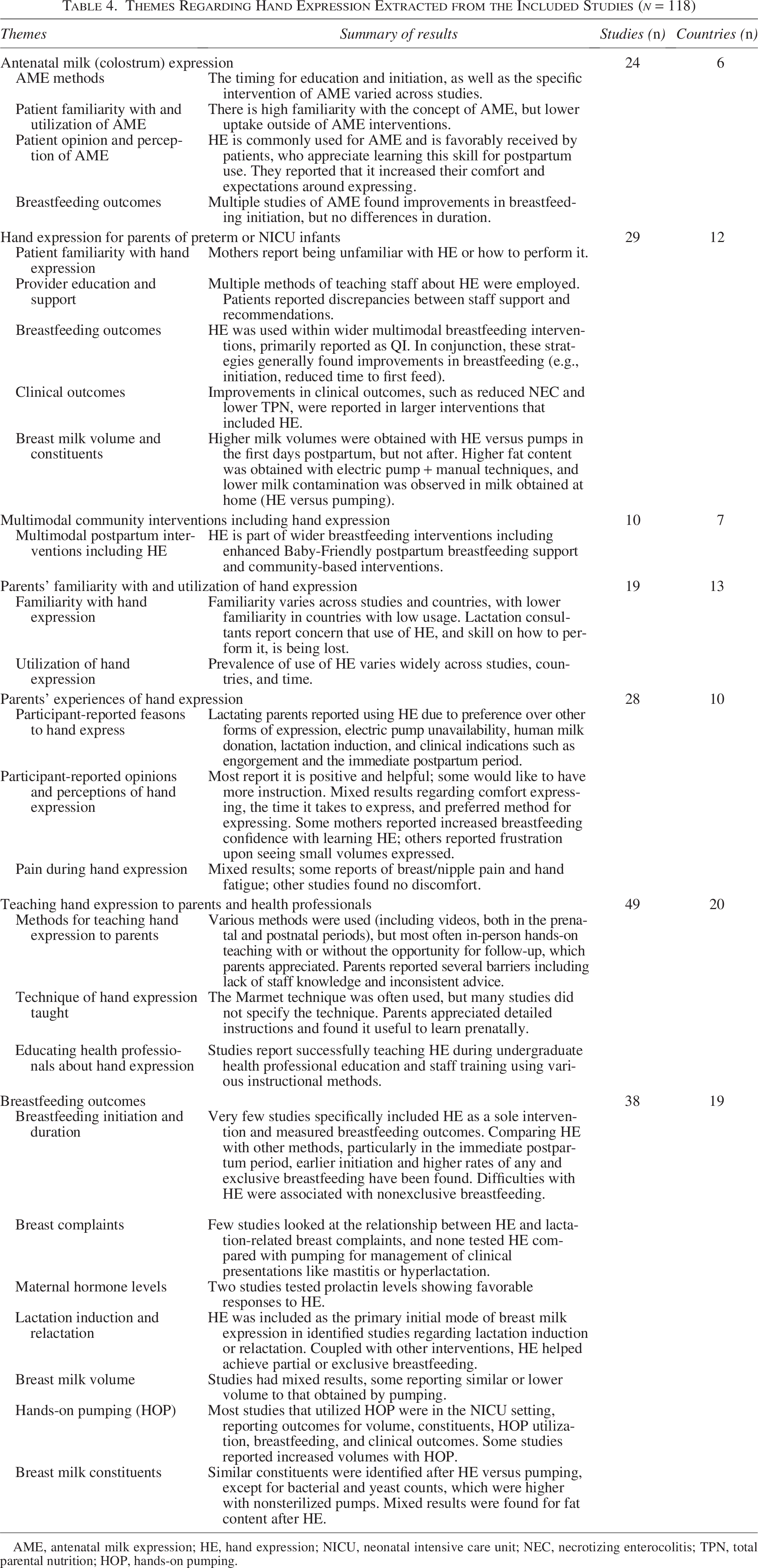
AME, antenatal milk expression; HE, hand expression; NICU, neonatal intensive care unit; NEC, necrotizing enterocolitis; TPN, total parental nutrition; HOP, hands-on pumping.
Antenatal milk (colostrum) expression
HE was the method taught to pregnant women in 24 reports of antenatal milk (colostrum) expression (AME), 21 of which were conducted in high-income countries and the remaining 3 in India. Eight were limited to patients with diabetes (gestational or pregestational).33–39 The specific intervention of AME varied across studies. In some studies, it was started as early as 20 weeks’ gestation or early third trimester,40–42 but in most recent studies, it was recommended at 36–37 weeks’ gestation, reflecting the safety at this gestational time demonstrated in the only large randomized controlled trial of AME, the Diabetes and Antenatal Milk Expressing (DAME) trial.39,43–45 Studies of AME included multiple components, including the prenatal timing of expression and other breastfeeding counseling and services, which limit the applicability of AME study outcomes to HE generally, that is, when performed postpartum. However, these studies provide information on methods of teaching HE, patient acceptability and perceptions, and utility of HE after delivery, as well as some insights into early postpartum use of HE, as reported in each section below.
HE for parents of preterm or NICU infants
Twenty-nine of the identified studies had been carried out in the NICU setting with mothers of preterm or very-low-birth-weight infants. Sixteen of these were QI initiatives that included HE in the larger intervention but did not specifically test or measure HE. Both QI and research sources reporting on breastfeeding outcomes, breast milk volume, and constituents are outlined in the respective sections.
Multimodal community interventions including hand expression
HE was included in larger breastfeeding support interventions without being the primary intervention or outcomes of study. In Bangladesh, peer counselors taught HE to factory workers to enable them to express and store breast milk at work, resulting in higher rates of exclusive breastfeeding at 6 months than among the control group.46–48 In Ethiopia, compared with a control group, those who were taught HE by peer counselors were more likely to express breast milk, to have a longer duration of lactational amenorrhea, and to have higher rates of both breastfeeding initiation and exclusivity. 49 Another peer counseling intervention targeting malnourished infants admitted to a pediatric ward in Kenya facilitated maternal gains in HE skills. 50 A smartphone-based intervention including HE teaching identified significant increases in breastfeeding self-efficacy and knowledge. 51 Implementing team-based breastfeeding visits including HE instruction in a socioeconomically and racially diverse population resulted in higher breastfeeding rates at 2 weeks and 4 months. 52
“Parents' familiarity with and utilization of hand expression”
The number of parents in these reports who have heard of (though not necessarily practiced) HE varied from 24% to 95.1%.33,50,53–55 Internationally, rates of utilization of HE vary widely, from <10% to 80.5%,33,54,56–66 depending on country, lactational stage, and study year. A survey of pre- and postpartum women in Canada in 2020–2021 found that 95.1% of participants had heard of HE and 80.5% had practiced it. 54 However, in other settings and populations, it was less prevalent. One study of adolescent mothers found no HE use. 67 A study in a general postpartum population found low (15%) use at 1.5 months postpartum that further decreased by 6 months. 56 A study in the United States found 62% of mothers learned HE in the hospital, but only 14% of those experiencing engorgement utilized it to relieve symptoms. 60 An Ethiopian study in the NICU setting found that HE was the most used method of expression, whereas hands-on pumping was the least used method. 62 HE use may be changing over time; one study of public hospital patients in Australia noted a decrease in HE utilization from 30% in 1992–1993 to approximately 10% in 2002–2003. 59 Despite this, in two Australian studies, HE was the preferred mode of milk expression for 8–15% of mothers.57,68 In terms of antenatal use of HE, recent surveys of pregnant and postpartum women demonstrate high familiarity with the concept of AME (65–70%) but lower uptake outside of AME interventions (14.2% in one large internet-based survey, n = 688).33,36 In many NICU settings, mothers report being unfamiliar with HE or how to perform it.63,69 Notably, one study in China found that mothers who had mastered the technique of HE also had higher scores on the Latch, Audible swallowing, Type of nipple, Comfort, Hold (LATCH) questionnaire for assessing breastfeeding techniques. 66
Parents' experiences of hand expression
Participant-reported reasons to hand express
Women found the use of HE helpful in a variety of situations, including managing engorgement; obtaining breast milk for supplementation; increasing milk production when there was no access to electric pumps, particularly in low-income settings; as a way of expressing breast milk when away from home; for antenatal expression; and to induce lactation.33,47,50,60,70–73
Participant-reported opinions and perceptions of hand expression
Women’s opinions of HE were generally positive. In multiple studies of prenatal and postpartum HE, patients reported that it was helpful to learn how to hand express.33,34,45,52,54,60,69,70,74 A quote from a British mother who learned AME illustrates the point: “I would have found it helpful…to have already got used to hand expressing as this was something I needed to do a lot once baby was born.” 33 One mother in a qualitative study noted that she did not consider HE to be “expression of milk,” viewing that term as reserved for pump use. 75
Antenatally, patients found HE to be beneficial in preparing to breastfeed, with many qualitative study participants specifically reporting they used it in the immediate postpartum period, though no studies reported rates for postpartum HE use among those who learned the skill for AME.36,38,70,72,76 Patients in AME studies reported it increased their comfort and expectations around expressing.39,45,77 One participant emphasized the importance of learning HE prenatally for postpartum use: “I think you guys should teach every single woman how to hand‐express. I think it’s a key skill, and they don’t teach you that in the hospital.” 70
Some mothers expressed feelings of unease or reservations about HE, particularly when performed prenatally, including concern about whether HE was depriving their infant of nutrients. 35 Studies from multiple countries reported that collecting small volumes of breast milk when expressing was perceived as a failure, both antenatally and postnatally,35,43,78,79 but having reassurance that any colostrum collected was beneficial helped mitigate these concerns. 38 Findings were mixed for overall comfort with HE in the presence of others or related to environmental factors, such as being in a NICU setting.34,62,70,76,80 However, mothers randomized to perform HE during the birth hospitalization reported feeling more comfortable expressing breast milk in front of others compared with mothers randomized to pumping. 26
Regarding time spent on HE, results were again mixed, with some mothers finding it more time-consuming than pumping and other mothers finding it a quick way to collect milk.38,71,78 Some studies reported patient challenges, such as difficulty seeing the cup for collecting milk or struggling to capture all of the colostrum expressed. 81
Pain during HE
Feelings of physical discomfort or pain have also been reported in both AME and postpartum HE, but the findings are mixed, ranging from no discomfort with HE to reports of hand fatigue and breast and nipple soreness, generally in a minority of participants and/or of mild intensity.34–36,45,70,71,82,83 Among a group of women randomized to HE or pumping in the immediate postpartum period, there were few reports of significant pain with either form of expression. 26 In a small observational study (n = 20) comparing experiences of NICU mothers who used HE versus electric pump, there were more reports of breast pain with HE; however, this was noted by the authors to be due to improper technique or to engorgement. 78 In a randomized crossover study of alternating HE and pumping by the same participant, report of pain was greater with pumping than HE. 84 This study provides possible explanations for these differences in reported pain, as the researchers also observed significantly greater nipple diameter and length changes with pumping than with HE, as well as the presence of erythema and swelling after approximately half of the pumping sessions and an absence of erythema and swelling with HE.
Teaching hand expression to parents
A variety of educational strategies for teaching HE to patients across prenatal, postpartum, and NICU settings were described. Videos and in-person instruction including hands-on teaching by a knowledgeable health care worker were most common.27,34,43,70,79,85,86 SMS messages, links to websites, and printed materials were also utilized widely.27,34,43,54,55,60,70,76,87–92 One study utilized telehealth services to teach mothers. 45 Some AME and preterm programs provided HE toolkits with syringes and feeding instruments (cups, spoons).36,38,93,94 In NICU settings, most of these were QI interventions providing educational materials on HE alongside several other unit improvements. Some of these included NICU parent-oriented messages that included the importance of early HE, the benefits of colostrum, and the importance of colostrum as the first feed, hands-on pumping, and expressing milk at home for use in the NICU.63,95,96 Instructions on HE to parents also included hand hygiene and other methods of decreasing contamination. One study that assessed bacterial growth in HM mentions instructing HM donors on breast hygiene and on how to manually express into sterile containers. This study proposed using a “stripping” method (i.e., discarding the initial milk portion) and found this technique resulted in decreased bacterial count in donated milk. 97
Women indicated that while nurses and lactation consultants were their primary sources of information, they also received information from the internet, friends and family, and other mothers.36,62,65,98 Educational interventions were effective in increasing confidence (using the Breastfeeding Self-Efficacy Scale) 51 and knowledge of HE, 87 as well as increasing the uptake of the practice across setting types.50,60,63,88 In one study, utilization of HE was associated with improved LATCH score. 66
Women generally responded well to all HE educational strategies.50,54,55,69,76 When asked explicitly about the quality of the education, women tended to rate the interventions highly.38,99 Across multiple studies that solicited patient feedback, mothers often reported appreciating—or in its absence, desiring—more help, such as through a follow-up visit to check technique. 35 One qualitative study noted that mothers received inconsistent advice on HE and felt that providers did not address all of their learning needs. 98 Suggestions for improvements from participants included showing realistic volumes of antenatal colostrum, specifics about the recommended frequency and timing of HE, storage guidelines, the influence of HE on milk production, and general encouragement and support.54,98 A UK study found that mothers found it helpful to be shown and told how to express, with some needing assistance with the syringes used to collect milk. 69 In two studies with preterm populations, discrepancies between staff support and recommendations in the postpartum and NICU settings were reported, indicating how education can fall through the cracks.63,69
Only seven studies indicated the precise HE technique taught (i.e., hand and finger placement, compressions). All seven reported teaching the three-step “Marmet” method in antenatal, postpartum, and NICU settings.38,43,70,83,85,100,101 A Delphi study of HE teaching with lactation professionals from multiple countries found agreement that finger placement was very important, but that finding the right position behind the nipple where milk expression is most effective is one of the most challenging aspects of learning. 71 Echoing this, a participant in a longitudinal qualitative study regarding milk expression reflected, “it’s probably different for every woman. And you just have to fiddle around a bit.” 79
Educating health professionals about hand expression
Health care worker educational activities took multiple approaches including simulated models, observed training, video, and in-person trainings. 102 Video trainings of HE technique for a variety of perinatal providers in the UK and China found increases in knowledge and confidence.103,104 A 40-hour training among Cuban nursing assistant students reported large increases in confidence teaching HE (10% pretraining to 94% post-training). 105 In a training for more experienced providers (nurse-midwives), no improvement in knowledge of HE was identified. 106 Simulation models for learning HE have been largely well-received and increased confidence in teaching HE to patients.107–109 A short HE training utilizing a mannequin as part of observed structured clinical training for nursing students resulted in a high average score for demonstrating the skill. 109 A survey of health care practitioners felt competent in teaching HE to patients but also noted they thought it was important to regularly update their skills in teaching HE. 110 In a qualitative study among lactation consultants, some expressed concern that the use of HE was being lost as the use of electric pumps increased. 111 However, it is still reported to be widely taught: a survey of US hospitals participating in the Better Outcomes through Research for Newborns network reported that 97% of the well-newborn nursery respondents taught HE in their facility (3% were unsure). 112 There were fewer reports with trainees, and baseline knowledge of HE was reported in only one study.
In NICU settings, multiple methods of teaching staff about HE were employed. These included in-service and online trainings for nursing and lactation staff, and sometimes for midwives and physicians, and hands-on and simulation-based training on HE.95,96,110,113–115 One comprehensive multiphase QI intervention included monthly meetings, initial training of nursing and lactation staff, creation of a lactation care map, online training for physicians, inclusion of lactation in daily notes/rounds, and development of educational materials for parents. 96 Many other sources described similar interdisciplinary and multiphase breastfeeding support interventions that included HE.86,94,114,116
Breastfeeding initiation and duration
We identified very few studies that specifically studied HE as a sole intervention and measured breastfeeding outcomes. These few, along with reports that included HE within larger multimodal breastfeeding interventions, are discussed below.
In terms of breastfeeding initiation, multiple studies of AME found improvements among those who performed AME, but no differences in longer-term duration.45,117,118 Three studies in India all found that HE decreased the need for top-off (supplemental) feeds and provided earlier establishment of full lactation in the immediate postpartum period among mothers assigned to practice AME and, in one of these, improved infant weight gain.119–121 In the DAME trial, compared with controls, participants assigned to AME had greater exclusive breastfeeding in the first 24 hours after birth, but no differences were found at discharge or 3 months postpartum. In the same study, among infants with hypoglycemia, more of those whose mothers were in the AME group received breast milk for hypoglycemia management and fewer received formula, though statistical testing was not reported. 39
Included studies that reported improvement in breastfeeding duration were those that included HE in the immediate postpartum period, rather than those limited to the prenatal period (AME). A randomized controlled trial of HE versus electric pump use during the birth hospitalization of newborns (12–36 hours old) with poor latch found that at 2 months postpartum those assigned to HE were more likely to be breastfeeding than those assigned to electric pumping (97% versus 73%). 26 In that study, participants were only required to express once and were then advised that continuing the method was optional. Other studies in which HE was included in multimodal breastfeeding support programs also found improvements in breastfeeding outcomes.41,42,122 Among these, an Italian hospital applied a high standard to breastfeeding support (complying with the Baby-Friendly Ten Steps) and used HE widely, and found much lower infant weight loss than typical. The mean weight loss was 5.95%, with the mean time to nadir 43 hours, occurring within the hospital stay, and no infant losing more than 10% of birth weight. 123
Two older studies from England after World War II provide important insights into how targeted HE in the first postpartum days may promote improved breastfeeding outcomes. Both tested the “Woolwich” method of AME and other prenatal breastfeeding preparation including carefully applied HE in the first 7 days postpartum (during which patients were in the hospital for “lying-in”). HE was used specifically to prevent or address engorgement and ensure adequate volume intake by infants at the breast, supported by nurses and midwives. In the original report of the method, carried out in Woolwich, England, Waller et al. report decreased rates of engorgement and increased exclusive breastfeeding at discharge, 3 months, and 6 months compared with control mothers. 41 In a subsequent study, Blaikley et al. present results among mothers who delivered at home (AME versus control) and another group that delivered in the hospital (AME + postpartum HE versus controls). 42 In the home-delivery group, no differences in breastfeeding outcomes were seen. In the in-hospital group, among which the Woolwich HE support was applied to the intervention group, double the rate of exclusive breastfeeding at 6 months (51%) was observed in intervention mothers compared with both in-hospital controls (26%) and home-birth mothers (22% in the AME group and 31% in controls). In-hospital intervention mothers also had lower rates of engorgement and cracked nipples. A final study of the Woolwich method in-hospital from this era did not repeat these findings and, in fact, reported higher rate of mastitis among those who received the intervention and no differences in breastfeeding duration. However, strict feeding schedules of 4–5 hours (common at the time) and less management of engorgement with HE were described by the authors, differing from the earlier studies. 40
NICU-based sources often included an emphasis on HE within wider multimodal breastfeeding interventions, primarily reported as QI. However, the precise techniques, recommendations, and intensity of HE support are rarely described, nor is maternal uptake of HE. Despite these limitations, such reports generally found improvements in breastfeeding outcomes. Many report improvement in breastfeeding initiation, breast milk as first feed, and reduced time to first breast milk feeding.92,93,102,113 Many sources report increases at later time points, primarily at discharge.86,89,90,95,96,102,113,116,124 Other noted improvements included decreased use of formula 125 or donor milk, 96 decreased necrotizing enterocolitis,89,95,126 and lower numbers of infants receiving total parenteral nutrition. 113
Breast complaints
We identified a few studies that looked at the relationship between HE and lactation-related breast complaints, and none that tested HE compared with pumping for clinical presentations like mastitis or hyperlactation. In one of the “Woolwich” studies in which HE was carefully used before or after nursing in the first week in the intervention group, lower rates of mastitis and engorgement were seen than in the control group, 42 and less engorgement was also seen with HE in a more recent study. 116 In a large prospective study (n = 946), HE was not associated with the incidence of mastitis. 127 While two studies identified higher rates of breast complaints (e.g., nipple lesions, mastitis) among those who were taught or reported using HE, these studies had methodological limitations. These included additional interventions concurrent with HE that may have caused adverse outcomes (e.g., scheduled feeds), 40 and a retrospective cross-sectional design that could not account for temporality as HE may have been used because they were experiencing pain or engorgement. 53
Maternal hormone levels
Two studies tested prolactin levels, showing favorable responses to HE. A study among exclusively breastfeeding mothers of term, healthy infants 1 month postpartum had each participant use five different milk expression methods over consecutive days, with blood collection every 10–15 minutes throughout the expression session. HE and manual pumping showed similar prolactin area under the curve, but both were lower than both breastfeeding and electric pumping. Oxytocin results were not significantly different by method. 100 In a relactation study of mothers of preterm and very low birth weight infants who had stopped breastfeeding within 2 weeks due to low milk production and were recommended to either hand express or use a manual pump, on the day that milk flow began again, the prolactin level was not significantly different from exclusively breastfeeding controls. 128
Lactation induction and relactation
HE was included as the primary initial mode of breast milk expression in six studies of inducing lactation or relactation. Three of these were case reports of postpartum relactation or treatment of profound hypogalactia, which included HE along with direct breastfeeding, use of supplemental nursing systems, electric and manual pumping, and galactagogues; all three cases achieved exclusive breastfeeding.73,129,130 In another relactation study of mothers of preterm and very low birth weight infants who had stopped breastfeeding within 2 weeks due to low milk production and who were instructed to hand express or use a manual pump 12 times daily, all achieved relactation in a mean of 6 days, although exclusivity was not described. 128 In a case report of nonpuerperal lactation induction, a transgender woman on hormonal augmentation produced 3–5 oz daily with HE alone after experiencing irritation with an electric pump. 131 Finally, another lactation induction study of nonpuerperal, nonbiological mothers found that exclusive and partial breastfeeding was possible through the use of HE, nipple stroking, infant suckling, and metoclopramide. 132
Breast milk volume
Studies examining milk volume obtained via HE versus mechanical or manual pumping show mixed results across various settings and patient populations. Studies conducted with healthy mothers of term babies have found that HE produced either similar 133 or lower volumes100,134 compared with pumping.
The majority of studies on this topic focus on mothers of infants in the NICU due to prematurity or very low birth weight. Few studies assigned participants to use only HE or pumps. A small US-based study found lower volume of milk output with HE starting on the first day postpartum; however, patients in the HE group expressed fewer times daily (mean = 5) compared with the electric pump group (mean = 6). 135 An observational study in which all parents used electric pumps reported higher volumes than among the HE group in Lussier et al.; however, this comparison is limited by the low volumes and lower frequency of expression. 136 A larger study instructed mothers to express every 2 hours, documenting higher volumes for the electric pump group than the HE group. 137 One study found higher milk volumes during HE sessions than electric pump sessions in the first days postpartum; however, the crossover nature of the study (each mother alternated between HE and electric pump every 3 hours) leaves the possibility that electric pumping may have contributed to overall volumes. 83 Another crossover study showed no differences in volumes between manual pumps and HE. 80 Two studies that assigned groups to use only HE or only a manual pump in the first week postpartum reported similar, although slightly higher volumes with the manual pump groups, and notably, both emphasized frequent expression.85,137
Hands-on Pumping
Multiple included sources report on combining HE with other expression techniques. A study comparing once-daily hands-on pumping versus once-daily hands-on power pumping while maintaining a practice of HE every 3 hours found higher volume in the power pumping group, though similar rates of exclusive breastfeeding at discharge. 138 Two studies report high and sustained volumes with the combination of HE and electric pumping in the first days, followed by hands-on pumping, and an emphasis on frequent expression. Morton (2009) recommended electric pumping 8 times daily, along with as-frequent-as-possible HE until lactogenesis II, followed by frequent hands-on pumping. 27 Those who hand expressed more often during the first 3 days, defined as at least 6 times/day, achieved over 700 mL/day at week 2 and sustained statistically greater daily volumes at weeks 2 and 4 and, though not significant, maintained higher production at week 8 (955 mL/day) compared with those who hand expressed <2/day in the first 3 days (658 mL/day). A study using a similar protocol of frequent (8–9 times daily) HE plus electric pumping in the first 3 days, then continued frequent hands-on pumping, also found participants achieved >700 mL/day by 2 weeks. 139
Breast milk constituents
Studies indicate that the method of milk expression can influence both HM composition and bacterial contamination. Different bacterial species have been identified based on the expression method used. 140 Specifically, several studies associated milk obtained via HE with less bacterial contamination compared with milk obtained via pumps.141–144 However, when cultures were done on milk obtained via HE and via washed, sterilized pumps, or when expression was performed in the hospital environment, the contamination rates were similar.141,144–146
There are mixed findings regarding the association between lipid content in HM and the method of expression. Two studies found higher fat and energy concentrations in colostrum 147 as well as in later stages, 101 while others found no statistically significant difference.133,134,148 In the NICU setting, expressed milk achieved a high fat content (>60 g/L) with the combination of an electric pump and manual techniques. 28
Lastly, the method of expression was also analyzed for other constituents. For example, a study from Slovenia found a similar lactoferrin composition in breast milk obtained with human expression and by pumping. 149 Another study also found no difference in nitrogen composition according to the method of expression. 148 When analyzing total breast milk nitrous oxide (NO) concentrations during the first 5 days postpartum, researchers found that concentrations were highest in breast milk from women who were exclusively breastfeeding (though the authors did not specify the criteria used for this classification). The next highest concentrations were found in breast milk from women who used a combination of HE and formula feeding. The lowest concentrations were found in women who were exclusively formula feeding and had not experienced suckling at the breast. 150
Discussion
This scoping review identified 118 articles looking at HE of breast milk, including utilization and outcomes as well as patient and health care provider experiences. These studies show that HE is generally well accepted among lactating patients, in both the prenatal and postpartum periods, yet use remains low in many settings where it is not emphasized. Interventions to teach HE are well received by parents, particularly in NICU settings. We found very few studies that directly test HE as a solitary intervention. The clinical utilization and study of HE are, rather, more often incorporated into wider multimodal breastfeeding interventions or studied along with other expression methods. Despite this limitation, the bulk of the literature reviewed suggests improved breastfeeding outcomes in settings where HE is taught or used.
The timing of HE use, as well as how it is applied along with other interventions, may be key aspects affecting its use and impact. We identified multiple studies that used HE in the first few days postpartum in cases of difficult latch, engorgement, and slow onset of lactogenesis II with good results. During the same time period, its use—with or without electric pumps—may be most helpful for improving breast milk access for preterm infants. HE is already widely recommended in clinical guidance and appears to be regularly taught by postpartum staff, 112 yet patient utilization of the practice is low, and parents report getting mixed messages around when to use it. We found that use was variable, without any clear patterns by country income level (there were both high and low rates in low-income and high-income countries), suggesting a need for education broadly. As electric pumps become more widely available and used globally, HE needs to be taught and continue to be emphasized as an important technique. Clinical interventions can apply HE more rigorously and ensure parents have adequate education and follow-up about HE as part of infant feeding plans and breastfeeding management. Research is urgently needed that more carefully examines the impact of HE as a primary intervention, particularly in the immediate postpartum period, as a form of prevention of the common breastfeeding problems (pain, low milk production) that lead to unplanned early cessation of breastfeeding. This should include studies that investigate the timing of HE, the clinical scenarios in which it is applied, and the techniques for teaching and implementing it (e.g., frequency, duration).
HE may have particular benefits to preterm infants. Its inclusion in interventions that have successfully increased breast milk utilization in NICUs should be of particular interest to health care administrators, as reductions in human donor milk usage, total parenteral nutrition, and rates of NEC may all reduce health care costs, as well as save lives. However, high-quality randomized studies that investigate the timing of HE and how it may be combined with other interventions such as pumping are needed in order to identify best practices for increasing breastfeeding in NICUs.
While prenatal HE to collect colostrum (AME) is increasingly utilized and studied, it appears that careful application of HE in the first few days postpartum may have the most impact, with some studies finding reduced engorgement, improved LATCH scores, and reduced need for early supplementation. However, familiarity, use, and positive experiences with AME suggest that the prenatal period is a ripe time to teach HE. Patients in AME interventions report on its usefulness postpartum. Recommendations to continue practicing HE postnatally should be a key educational component of AME programs. Research on AME that measures postpartum use of HE will provide a greater understanding of the impact of HE prenatally versus postnatally.
One group of investigators reported evidence that utilization of HE may have decreased over the past two decades. 59 The marketing of pumps could undermine the use and transfer of knowledge of how and when to use HE. 151 Lack of knowledge and use of HE could lead to worsening breastfeeding outcomes. Health care staff and breastfeeding support programs should emphasize to parents the importance of learning both HE and pump use and counsel patients on when different methods may be most useful. Among the included studies in this review, five disclosed funding from pump and formula companies.44,133,134,139,146 Unbiased research on HE and pumps is needed. Furthermore, research on HE—like much breastfeeding research—may have fewer funding sources and thus should be prioritized by governmental and other funders without conflicts of interest.
Critically, in situations of human and armed conflicts, economic depression, and natural disasters, parent and health care worker familiarity with HE are required, as electric pumps may not be available. Even when readily available, they may be rendered useless due to the lack of a reliable electric source to connect them and the scarcity of clean water for proper sanitation.4,5,152 Of the studies in this review, 34% originated in low- and middle-income (LMIC) countries, reflective of the public health interest in both HE and breastfeeding in those settings. Overall, research from LMICs is underrepresented given the proportion of the world’s population represented,153,154 but the relatively greater representation in the results of our search suggests growth in research and publication from LMICs. Scoping reviews, which allow for a wider range of study designs, can be a means of sharing global research more widely.
The results show that in-person counseling with a provider is often desirable for patients learning HE, as is exposure to the technique prenatally. Although there are different methods to express milk by hand, the exact technique that is best for teaching (e.g., hand positioning) has not been studied, and most included sources did not describe how it was taught. Some mothers report pain or discomfort, and this should be considered when teaching and counseling. Educating women prenatally will ensure they will be more likely to hand express properly postpartum. Providing support after an educational intervention is also important to ensure patients are expressing properly. Because some participants perceived their inability to collect large volumes of colostrum with HE as a personal failure, providing appropriate counseling could have positive effects both on self-efficacy and mental health. Staff should receive regular education that includes HE in order to maintain skills and ensure consistent messaging and recommendations. Studies on techniques for teaching mothers HE (e.g., C-shape fingers) are needed in order to determine and share best practices. AME studies should test different strategies and schedules of AME, and how this impacts the volume of colostrum and prevalence of any colostrum expression. Learning and practicing HE can take many forms, and much learning may need to be done by women on their own.
Strengths and limitations
Our study had wide inclusion criteria that did not limit studies to those looking only at HE as an intervention or outcome, as is often the case in review studies. This allowed for the inclusion of a wide variety and large number of studies that incorporated HE in multiple ways. However, for this reason, the conclusions that can be drawn are limited, and in many studies and QI reports, HE was but just one of many breastfeeding support practices applied, and thus the specific impact of HE was not demonstrated. Many studies were observational and retrospective and could not accurately test temporality or causality, and they may be subject to recall bias by participants. Following the scoping review design, a review for study quality was not performed. Scoping reviews are intended to include a variety of study designs and qualities in order to identify nascent areas of investigation and future research needs. Additionally, there are likely many additional reports that incorporated HE as part of larger interventions that did not come up in our search, as HE may not be included in keywords, abstracts, or titles when it is not the primary focus of the study. However, given the breadth of studies included, we believe the sources likely reflect the body of literature on HE. Relevant studies may have been missed inadvertently during selection or because they were in languages other than English or Spanish; however, overall, our included sources represented a wide diversity of countries, in part due to the inclusion of Spanish texts.
Future research
In addition to those recommendations above, much additional research is needed. First, researchers must document HE precisely. Research on HE is limited by poor reporting and definitions. Studies of breast milk expression need to clearly differentiate between forms of expression including HE, manual pumps, and types of electric pumps (e.g., wearable) as different outcomes and complications may be associated with each. Studies of breast milk expression should also document the timing of HE (i.e., in the first days postpartum or later). There were limited reports of negative outcomes of HE (time spent, discomfort), which may be reflective of bias in research or a gap for future exploration. The existing literature could be systematically reviewed, with meta-analyses, for example, of rates of utilization of HE or patient satisfaction.
Clinical trials of HE compared with other forms of expression for particular clinical scenarios are needed, such as mastitis and hyperlactation, in order to identify evidence-based clinical management strategies. HE is widely recommended as part of the management and prevention of these conditions, yet we found no studies testing this. Overall, the large number of QI and observational studies and the few randomized controlled trials is a reflection of the poor state of research on clinical breastfeeding issues, particularly those that are most common such as low milk production and nipple pain.
We found very few studies that incorporated patient perspectives or codesign of research with affected communities. Future studies of HE should take a patient-centered approach in determining relevant interventions and outcomes that support patient definitions of breastfeeding success. 155
Conclusions
This review, which had wide inclusion criteria regarding study design and inclusion of HE and thus included a wide variety of reports, found broad application of HE and numerous instances of improved breastfeeding outcomes related to its use. While HE is currently recommended in clinical guidelines and is generally favorably experienced by mothers and health care providers, its use is variable, and more research is needed on its use in particular clinical scenarios. If HE indeed has benefits that electric pumps do not, then efforts should be made to ensure that both mothers and health care providers are taught and exposed to both methods of milk expression. The influence of the pump industry on research that involves pumps needs to be counterbalanced by continued research on the original method of breast milk expression that human mothers have used for millennia: HE.
Ethical Committee
This is nonhuman subject research and thus did not require ethical committee approval.
Authors’ Contributions
The authors confirm contribution to the paper as follows: S.E.A. performed conceptualization, methodology, investigation, writing (original draft and review and editing), visualization, supervision, and project administration. K.R.S. performed conceptualization, methodology, investigation, writing (original draft and review and editing), visualization, and supervision. M.J.P. performed investigation, writing (original draft and review and editing), and visualization. S.T.G. performed investigation and writing (review and editing).
Footnotes
Disclosure Statement
The authors declare that they have no relevant or material financial interests that relate to the research described in this article.
Funding Information
The authors confirm no receipt of financial support for the research, authorship, and/or publication of this article.