
Abstract
Objectives:
To evaluate the efficacy of breast massage (BM) in enhancing breast milk production in postpartum women, as compared to control interventions.
Methods:
A systematic review was conducted using PubMed, Scopus, ScienceDirect, TCI, and ThaiLis. Relevant articles were identified from inception to July 2025. Only randomized controlled trials (RCTs) reporting the effect of BM on breast milk production and breastfeeding discomfort were included. The risk of bias in the included studies was assessed using the Cochrane Collaboration’s tool. Data analysis was performed using RevMan 5.4.1.
Results:
A total of 18 RCTs with 1,099 participants were included. Compared with the control group, BM demonstrated a significantly greater effect on increasing breast milk volume (standardized mean difference = 0.76; 95% CI = 0.47, 1.05; p < 0.00001, I2 = 87%). Additionally, BM significantly reduced scores for breast engorgement, pain, and temperature, while increasing the number of infant urinations compared to the control group. However, the number of infant defecations did not significantly differ. Participants receiving BM also experienced greater resolution of breast engorgement, although there was no significant difference in complete breastfeeding rates. BM was also associated with a significantly lower anxiety level and a significant increase in serum prolactin levels compared to the control group.
Conclusion:
BM appears to be an effective intervention for enhancing breast milk production and decreasing breast engorgement, breast pain, and anxiety levels in postpartum women.
Introduction
Breastfeeding is widely recognized as the best method of infant nutrition, providing numerous health benefits for both the baby and the mother.1,2 For infants, breast milk offers essential nutrients, antibodies, hormones, growth factors, enzymes, and immunoglobulins that support development and protect against infections and chronic diseases.3,4 For mothers, breastfeeding aids in uterine involution, reduces the risk of postpartum hemorrhage, and is associated with a lower incidence of certain cancers, including breast and ovarian cancer.5,6 Recognizing these profound benefits, organizations worldwide, such as the World Health Organization (WHO) and UNICEF, strongly recommend exclusive breastfeeding for the first six months of life, followed by continued breastfeeding with complementary foods until at least two years of age and beyond. 7
Despite the overwhelming evidence supporting breastfeeding, many mothers encounter challenges that can impede successful lactation and lead to premature cessation. Common difficulties reported by postpartum women include insufficient breast milk production, which often results in concerns about infant growth and well-being.8–10
In addition to congenital causes such as insufficient glandular tissue, suboptimal milk production may result from a range of factors, including preterm birth, maternal illness, inappropriate mother–infant separation, relactation following a prolonged interruption, and indirect breastfeeding practices. A typical physical cause is plugged milk ducts, which lead to local milk stasis and painful breasts. 9 Furthermore, painful breast conditions such as breast engorgement and cracked nipples are frequently experienced, causing significant discomfort and distress that often contributes to early breastfeeding discontinuation.11,12 The physical discomfort and the associated emotional burden of these lactation challenges can also heighten maternal anxiety during the delicate postpartum period, impacting maternal well-being and the mother–infant bond. 13
In response to these challenges, various interventions have been explored to support breastfeeding mothers. Among non-pharmacological approaches, breast massage (BM) has emerged as a widely practiced traditional and complementary therapy. Anecdotal evidence and practices in many cultures suggest that BM can facilitate milk flow, reduce discomfort, and promote relaxation. 14 The proposed mechanisms include improved blood circulation, lymphatic drainage, and manual emptying of milk ducts, which may lead to increased milk synthesis and reduced tissue congestion. 15 This action (manual emptying of milk ducts) is hypothesized to reduce feedback inhibition of milk synthesis, thereby directly enhancing breast milk production. Given its noninvasive nature and accessibility, BM holds promise as a supportive measure for postpartum women.
BM has been proposed as a nonpharmacological intervention that may alleviate breast discomfort and address underlying factors contributing to early breastfeeding cessation, particularly by enhancing milk production.10,16–28 While numerous individual studies, including randomized controlled trials (RCTs), have investigated the effects of BM on various lactation outcomes, their findings have been diverse and sometimes conflicting due to variations in methodology, sample size, and the specific BM techniques employed.
Therefore, this systematic review (SR) and meta-analysis (MA) aim to critically appraise and synthesize the current evidence from RCTs to determine the effectiveness of BM in postpartum women on key lactation outcomes, including breast milk production, as well as its impact on secondary outcomes, including serum prolactin levels, resolution of breast engorgement, breast pain intensity, changes in breast temperature, and maternal anxiety. The findings of this review will provide an evidence-based summary for health care professionals, policymakers, and mothers, guiding clinical practice and potentially improving breastfeeding support strategies.
Materials and Methods
Research design
This SR and MA specifically focused on RCTs evaluating the effect of BM on outcomes such as breast milk production, breast engorgement, breast pain, and maternal anxiety in postpartum women. The protocol was registered on PROSPERO (CRD420251088982). The review adhered to the guidelines outlined in the Cochrane Handbook for Systematic Reviews of Interventions, Version 6, 29 and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement. 30
Eligibility criteria
We conducted a SR and MA of RCTs to assess the effect of BM, compared to control interventions (standard medical care, breast care, and active treatment), on breast milk production and secondary outcomes (serum prolactin levels, resolution of breast engorgement, breast pain scores, breast temperature, maternal anxiety, complete breastfeeding, the number of infant urinations and defecations, and adverse events). The search, spanning January 2000 to July 2025, utilized the databases PubMed, Scopus, ScienceDirect, TCI, and ThaiLis, with terms including “breast massage,” “breast milk,” “postpartum women,” and “randomized controlled trial.” Excluded publication types included nonrandomized studies, observational studies, reviews, comments, books, abstracts, case reports, protocols, SRs, and practice guidelines.
Study selection
The data extraction process for this meta-analysis was divided into two principal stages. In the initial stage, two independent researchers (C.C. and W.P.) conducted a preliminary literature screening using the Rayyan software (https://rayyan.qcri.org), 31 based on predefined inclusion criteria and keywords. Only literature unanimously agreed upon by both researchers progressed to the subsequent phase. For studies with discrepancies, a third researcher (S.W.) was involved in discussions to determine final inclusion.
In the second stage, detailed data extraction was performed independently by two researchers (C.C. and W.P.) to ensure the completeness and accuracy of the information. The extracted data were organized using standardized table forms. They included study characteristics (First author’s name, year of publication, study design, and study duration), participant details (sample sizes of intervention and control groups, sex, and age), intervention details (type of intervention, type of control, and selected massage points), and outcome and safety data (outcome measurements and adverse events).
Quality assessment
The methodological qualities of eligible studies were independently assessed by two researchers (C.C. and W.P.). The quality of the RCTs was evaluated using the Jadad et al. 32 This scale has a maximum score of five points and focuses exclusively on three dimensions of internal validity: randomization, blinding, and patient attrition. Studies were classified as low-quality (score of two points or less) or high-quality (score of three or more points).
The risk of bias (ROB) for all included studies was also independently assessed by the same researchers (C.C. and W.P.) using the Cochrane ROB tool for RCTs. This tool incorporates several key domains, including sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other sources of bias.
The overall ROB for each study was classified as low risk (low ROB in all key domains), high risk (high ROB in one or more key domains), or unclear risk (unclear ROB in one or more key domains without high ROB in any domain). 33 Any discrepancies in the assessment were resolved through discussion with a third author (S.W.).
Data synthesis and analysis
The primary outcome of this study was breast milk volume. The secondary outcomes included breast engorgement score, resolution of breast engorgement, breast pain scores, maternal anxiety, serum prolactin levels, complete breastfeeding, breast temperature, and adverse events. The effect sizes of the treatments for improving breast milk volume, breast engorgement score, pain score, serum prolactin levels, anxiety levels, and breast temperature were estimated using standardized mean difference (SMD) with a 95% confidence interval (CI). The resolution of breast engorgement and complete breastfeeding were pooled using relative risk (RR) with a 95% CI. The I2 statistic was used to define statistical heterogeneity among studies, with a significant level set at I2 > 50%. 34 The Der Simonian and Laird’s random-effects model was employed for the analysis of all outcomes. Publication bias was assessed using a funnel plot. Egger’s regression test was used to detect funnel plot asymmetry.35,36 Statistical analysis was performed using RevMan version 5.4.1, and the significance level was set at p < 0.05. A fixed-effects model was used for the sensitivity analysis, which confirmed the robustness of the results.
Results
Study characteristics
The PRISMA flow diagram (Fig. 1) illustrates the steps used to identify and assess the eligibility of studies for inclusion. An initial comprehensive search across multiple databases yielded 1,598 studies. After the screening of titles and abstracts, 60 articles were excluded for the following reasons: five were SRs, one was a SR protocol, 38 were non-RCTs, and 16 were duplicates across databases.
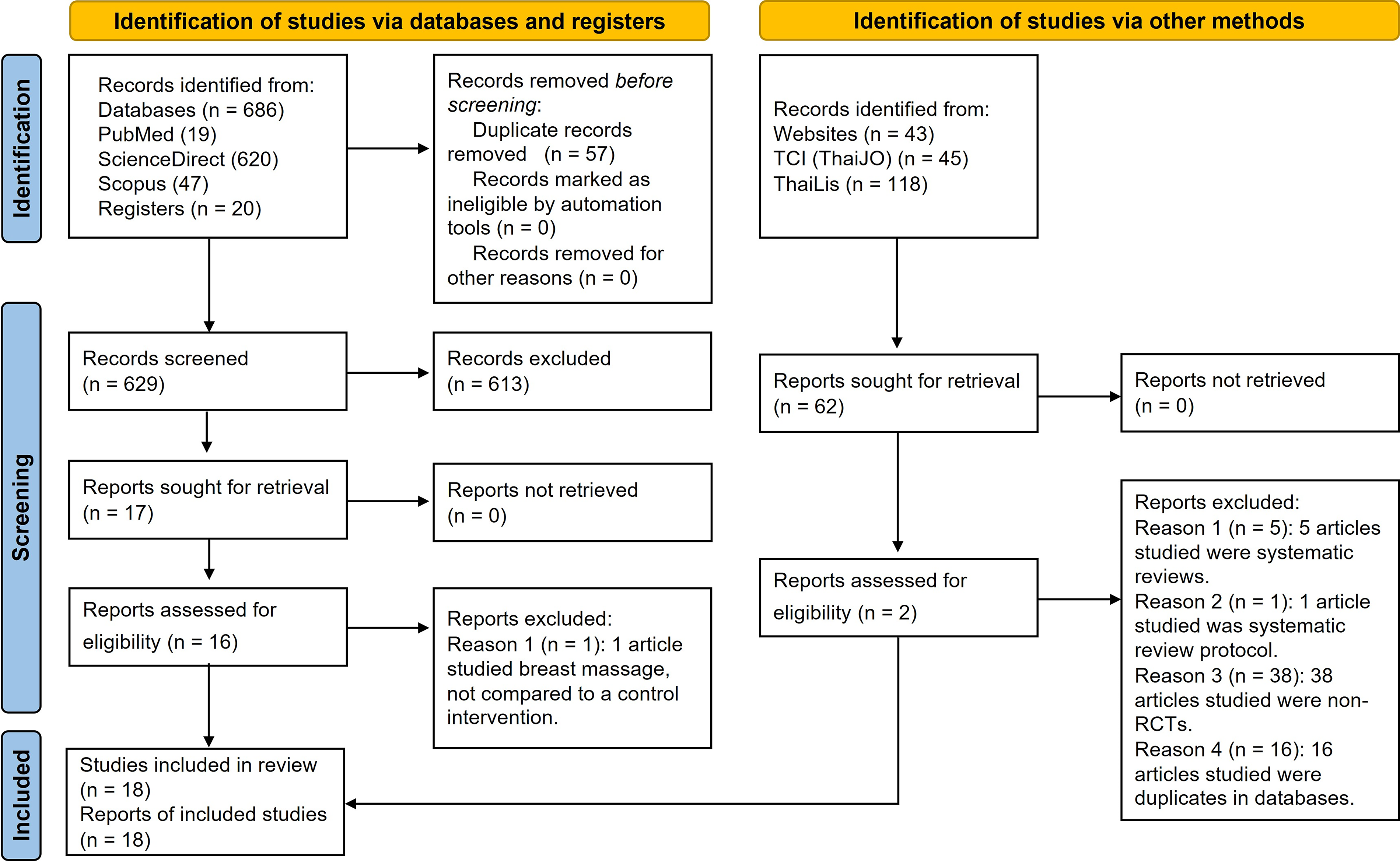
PRISMA 2020 flow diagram for new systematic reviews, which included searches of databases, registers, and other sources.
Subsequently, the identified articles were selected for a full-text review. Two potentially relevant articles were identified via other methods, resulting in a pool of articles for full-text assessment. Only 18 studies were included in the MA, with one article being excluded because it did not compare a control intervention. Therefore, 18 RCTs were eligible for analysis and were included in the SR and MA. The characteristics and details of the included studies are shown in Table 1, and detailed massage techniques are shown in Table 2.
Characteristics of the Included Studies
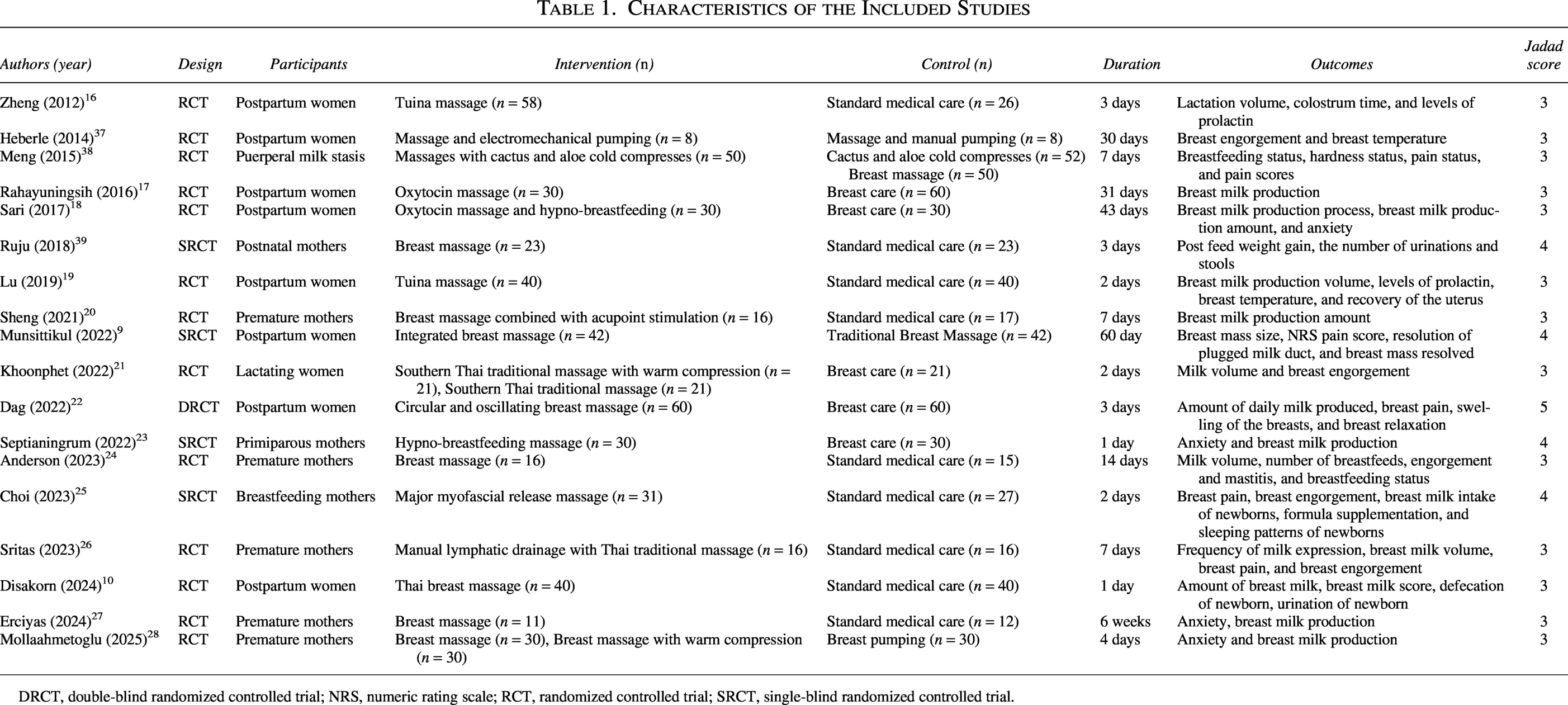
DRCT, double-blind randomized controlled trial; NRS, numeric rating scale; RCT, randomized controlled trial; SRCT, single-blind randomized controlled trial.
Detailed Massage Techniques

A total of 18 studies involving 1,099 participants were eligible for inclusion, covering a diverse range of massage interventions categorized as follows: Tuina massage (2 studies),16,19 Oxytocin massage (2 studies),17,18 general BM (5 studies),9,24,27,28,39 Thai BM (3 studies),10,21,26 and six studies employing combined/other massage techniques, which included massage and electromechanical pumping, 37 massages with cactus and aloe cold compresses, 38 BM combined with acupoint stimulation, 20 circular and oscillating BM, 22 hypno-breastfeeding massage, 23 and major myofascial release massage. 25
Assessment of methodological quality and ROB
The methodological quality assessment revealed that only one trial had a high risk of bias in random sequence generation, allocation concealment, and blinding of participants, personnel, and outcome evaluators. The details of the ROB assessment are shown in Figure 2. Based on the Jadad scale, one study was rated 5/5. Four studies were rated 4/5 because they were single-blind RCTs that did not report on allocation concealment or blinding between groups. The remaining 13 studies were rated 3/5 on the Jadad scale because they were non-blind RCTs (Table 1).
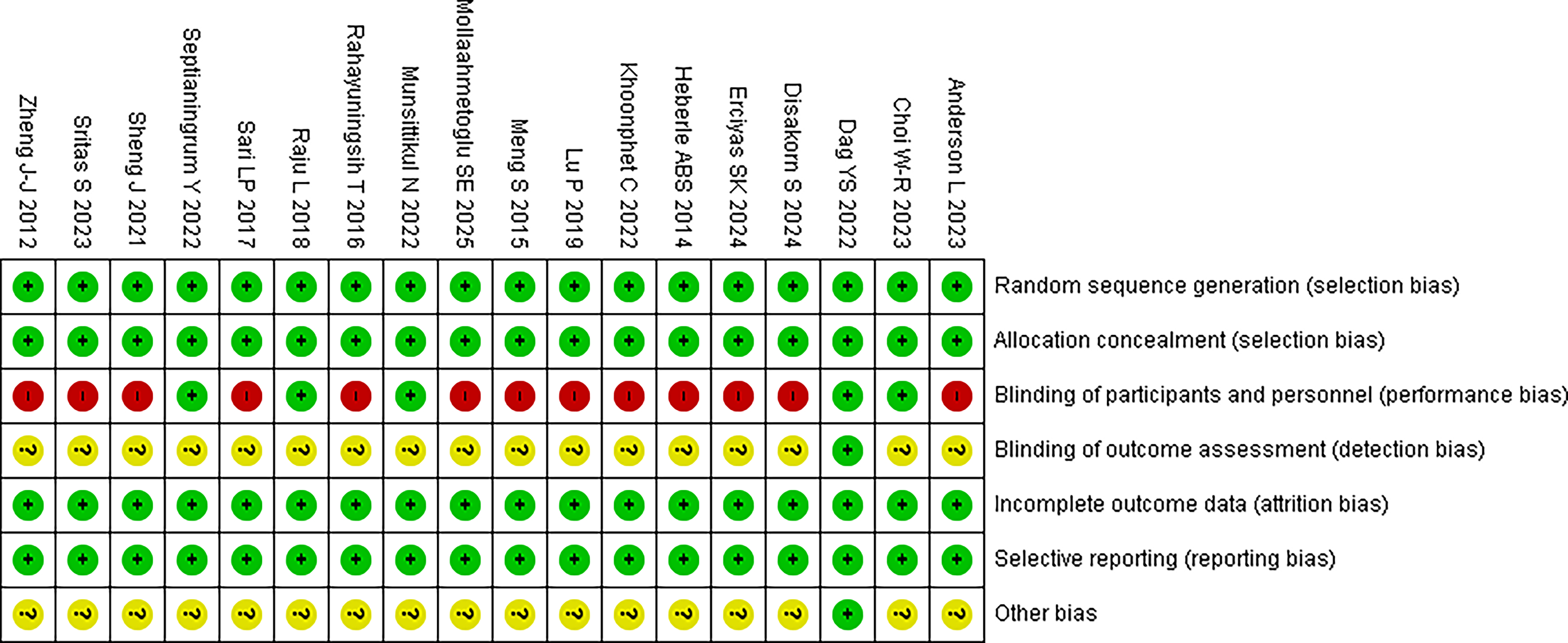
Risk of bias among the 18 included studies. The
Primary outcome
Breast milk volume
The amount of breast milk produced was measured using measuring cups or weighing scales after the massage and compared with the control group. To standardize the volume across studies, measurements reported in grams were converted to milliliters using the accepted density of breast milk (1.03 g/mL).27,40 The overall analysis demonstrated a significant increase in breast milk volume in the BM group when compared with the control group (SMD = 0.76; 95% CI = 0.47, 1.05; p < 0.00001, I2 = 87%). Furthermore, the significant effect was observed across various follow-up time points: Time 1 (SMD = 0.44; 95% CI = 0.00, 0.88; p < 0.00001, I2 = 90%), Time 2 (SMD = 0.83; 95% CI = 0.53, 1.14; p < 0.00001, I2 = 45%), and Time 3 (SMD = 1.38; 95% CI = 0.87, 1.89; p < 0.00001, I2 = 78%) (Fig. 3).
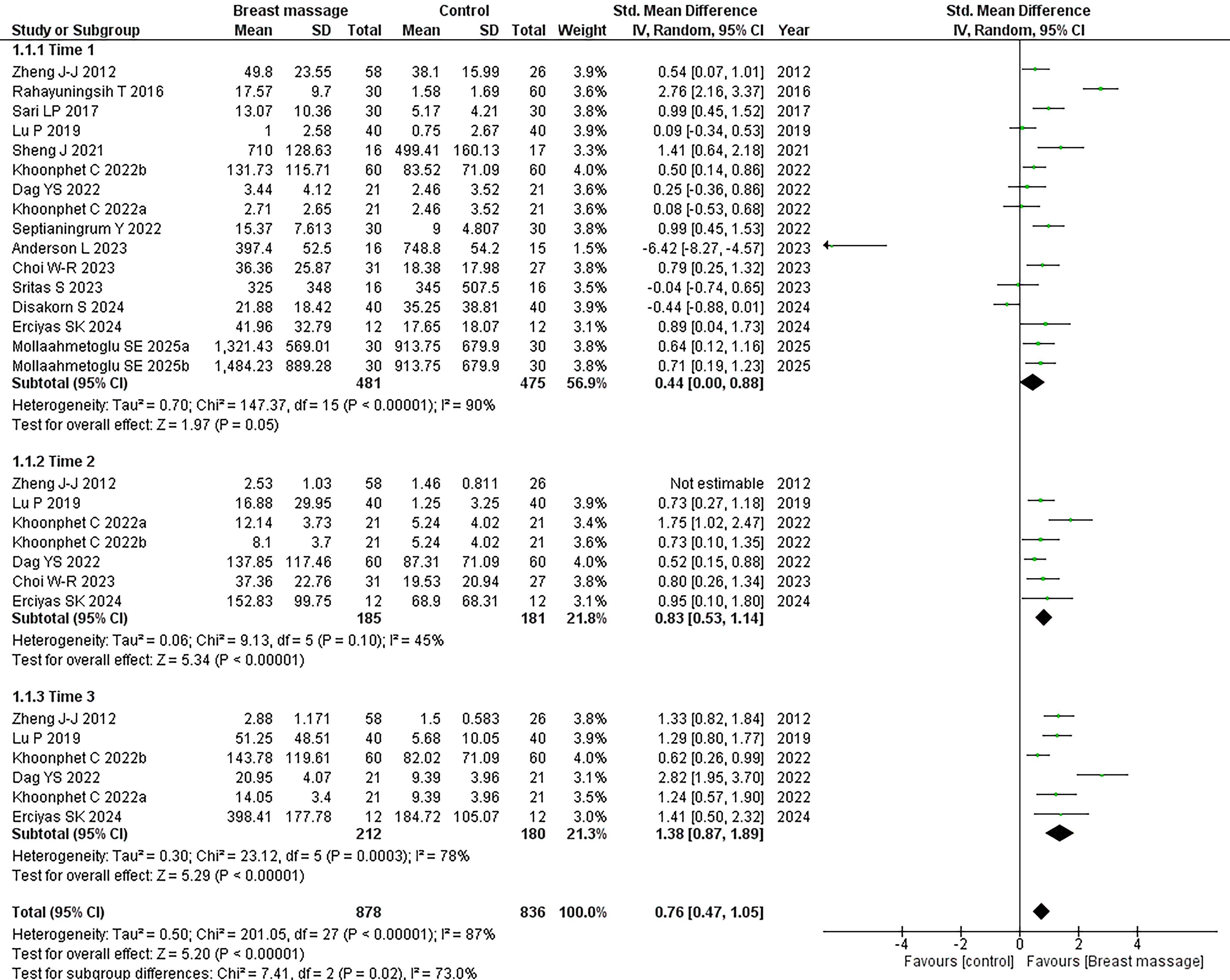
Forest plot for the effect of BM on breast milk volume. Comparison of breast milk volume between the breast massage group and the control group at different follow-up time points (overall assessment, Time 1, Time 2, and Time 3).
Secondary outcome
Breast engorgement score
The six-point engorgement scale was used to assess participants’ breast engorgement (firmness and tenderness). 21 The overall effect, derived from a single study, showed a significant reduction in the engorgement score in the BM group compared with the control group (SMD = −0.75; 95% CI = −1.23, −0.27; p = 0.002, I2 = 70%) (Fig. 4A). Significant reductions were also observed at Time 2 (SMD = −0.88; 95% CI = −1.33, −0.43; p < 0.0001, I2 = 0%) and Time 3 (SMD = −1.28; 95% CI = −2.12, −0.44; p < 0.003, I2 = 67%). However, no significant difference was found at Time 1 (SMD = −0.11; 95% CI = −0.54, 0.32; p = 0.62, I2 = 0%).
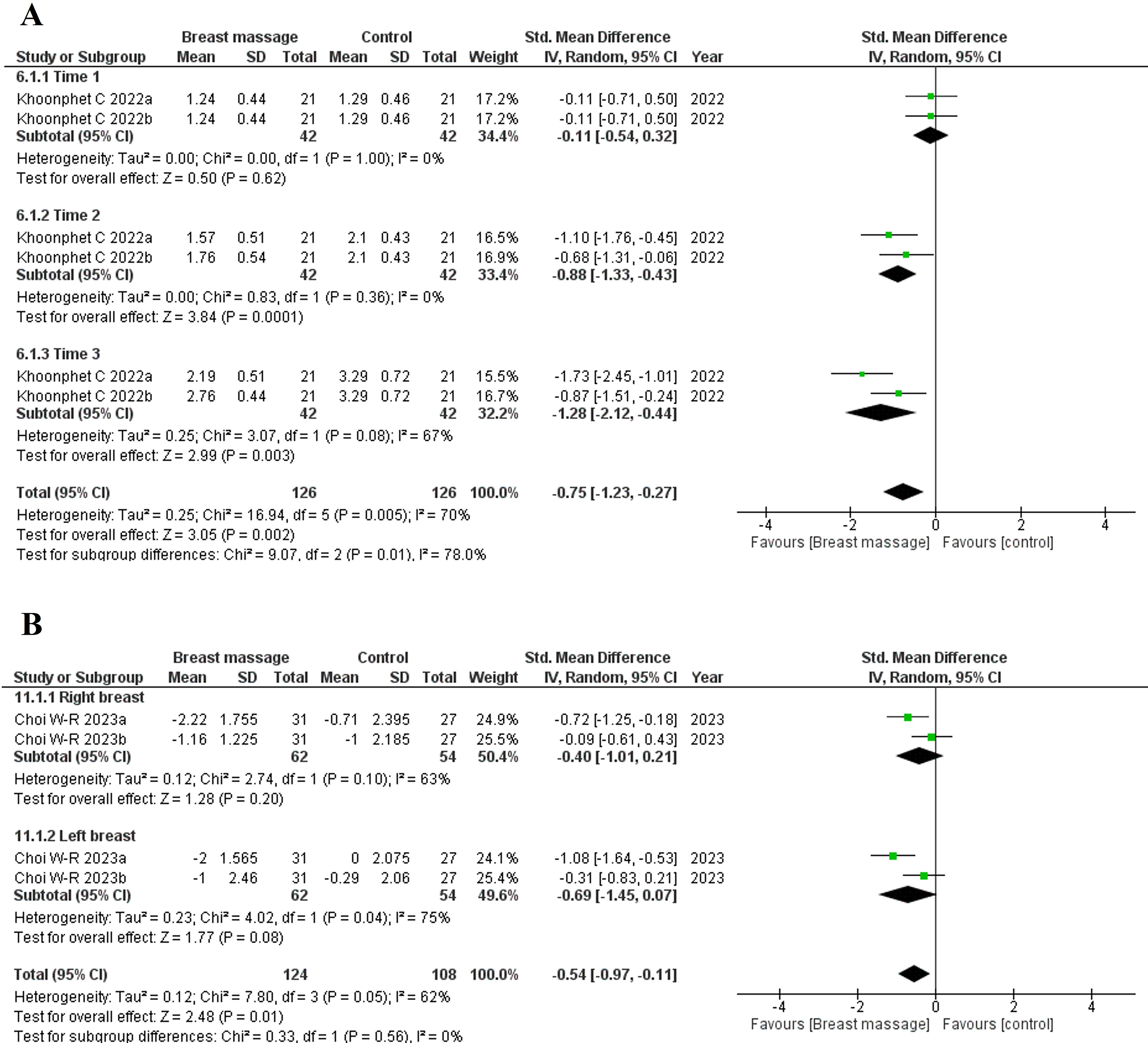
Forest plot for the effect of BM on breast engorgement score compared to control.
Changes in breast engorgement were objectively measured using a rubber hardness tester. 25 The overall effect from a single study showed a significant reduction in the breast engorgement score in the BM group compared to the control group (SMD = −0.54; 95% CI = −0.97, −0.11; p = 0.01, I2 = 62%). However, no significant difference was found when analyzing the right breast (SMD = −0.40; 95% CI = −1.01, 0.21; p = 0.20, I2 = 63%) or the left breast (SMD = −0.69; 95% CI = −1.45, 0.07; p = 0.08, I2 = 75%) separately (Fig. 4B).
Resolution of breast engorgement
The number of participants in the BM group who showed “much better” and “excellent” improvement in breast engorgement was significantly higher than in the control group (RR = 1.53; 95% CI = 1.24, 1.88; p < 0.0001) (Fig. 5A). Importantly, no heterogeneity was observed for this outcome (I2 = 2%, p = 0.36).
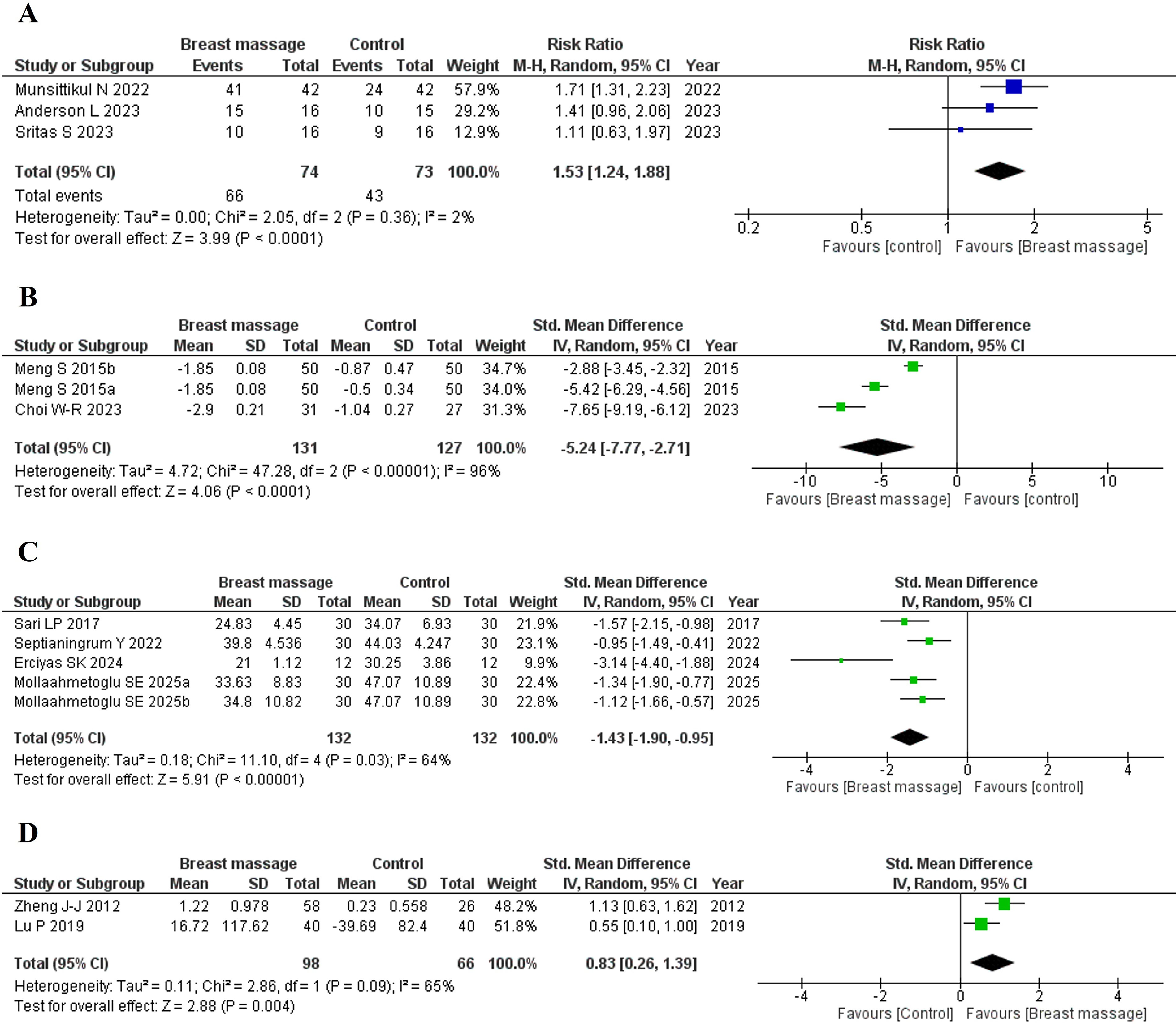
Forest plot for the effect of BM on secondary outcomes compared to control.
Breast pain score
The Visual Analog Scale (VAS) was used to assess changes in the breast pain score. The overall analysis of two studies demonstrated a significant reduction in breast pain in the BM group compared with the control group (SMD = −5.24; 95% CI = −7.77, −2.71; p < 0.0001). However, substantial heterogeneity was observed for this outcome (I2 = 96%, p < 0.00001) (Fig. 5B).
Anxiety levels
The State and Trait Anxiety Inventory (STAI) was used to measure changes in maternal anxiety level. The overall analysis demonstrated a significantly lower anxiety level in the BM group compared with the control group (SMD = −1.43; 95% CI = −1.90, −0.95; p < 0.00001) (Fig. 5C). However, the results showed moderate heterogeneity (I2 = 64%, p = 0.03).
Serum prolactin levels
The overall analysis demonstrated a significantly greater increase in serum prolactin levels in the BM group compared with the control group (SMD = 0.83; 95% CI = 0.26, 2.39; p = 0.004) (Fig. 5D). The results exhibited moderate heterogeneity (I2 = 65%, p = 0.09).
Complete breastfeeding
The number of participants in the BM group did not have a statistically significant effect on this outcome compared with the control group (RR = 1.73; 95% CI = 0.81, 3.67; p = 0.16). Furthermore, substantial heterogeneity was observed for this outcome (I2 = 82%, p = 0.004) (Fig. 6A).
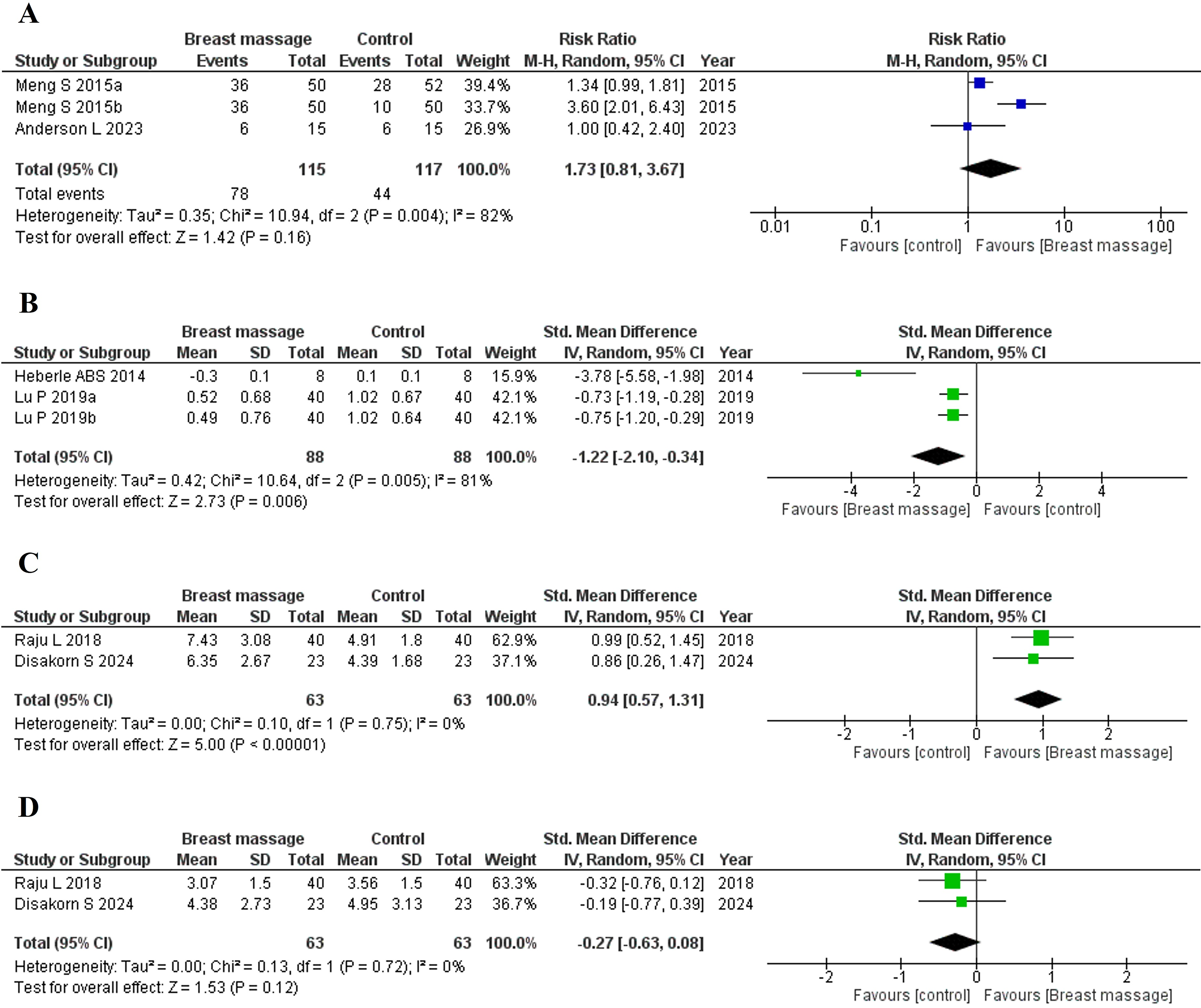
Forest plot for the effect of BM on secondary outcomes compared to control.
Breast temperature
The overall analysis demonstrated a significant decrease in breast temperature (SMD = −1.22; 95% CI = −2.10, −0.34; p = 0.006) in the BM group when compared with the control group. These results, however, showed substantial heterogeneity (I2 = 81%, p = 0.005) (Fig. 6B).
The number of infant urinations and defecations
The overall effect on the number of infant urinations per day showed a significant increase in the BM group when compared with the control group (SMD = 0.94; 95% CI = 0.57, 1.31; p < 0.00001). Importantly, no heterogeneity was observed for this outcome (I2 = 0%, p = 0.75) (Fig. 6C).
Conversely, the overall effect on the number of infant defecations per day showed no statistically significant difference between the BM and control groups (SMD = −0.27; 95% CI = −0.63, 0.08; p = 0.12). This outcome also demonstrated no heterogeneity (I2 = 0%, p = 0.72) (Fig. 6D).
Adverse events
Only one study reported adverse events during therapeutic massage treatment. 26 This study indicated that two participants in the intervention group experienced mild, short-lived side effects, specifically red marks in the massaged area. However, these complaints resolved within 20 minutes and were not accompanied by itching or pain, confirming that the intervention was well tolerated and safe overall.
Sensitivity analysis
The results of the sensitivity analysis are shown in Table 3. In this analysis, the model was adjusted to a fixed-effects model, and the main findings regarding the clinical efficacy of the BM remained unchanged, confirming the robustness of the primary results.
Sensitivity Analysis Outcomes Compared with the Main Analysis
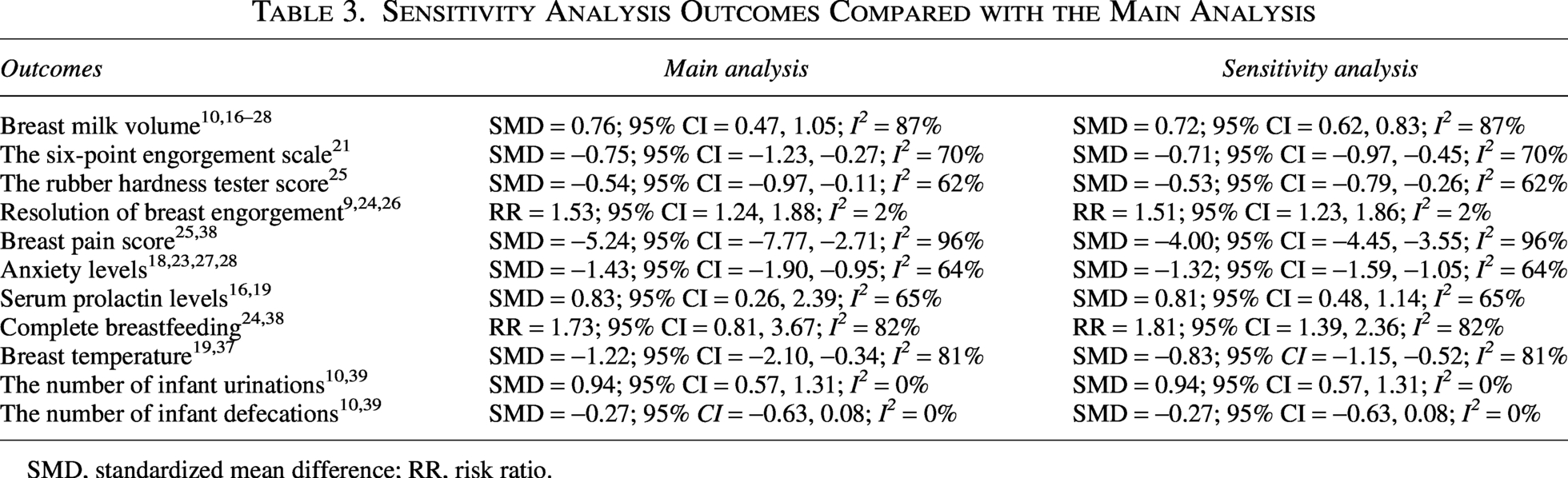
SMD, standardized mean difference; RR, risk ratio.
Publication bias
The publication bias concerning the clinical therapeutic efficacy of BM was analyzed using the data from three studies. The funnel plot appeared nearly symmetrical, indicating no evidence of potential publication bias (Supplementary Figures S1, S2, S3, S4, S5, S6, S7, S8, S9, S10, and S11).
Discussion
The current SR and MA aimed to evaluate the efficacy of BM in enhancing breast milk production. The main findings confirm that therapeutic BM is an effective method to enhance breast milk production (primary outcome). Compared to control interventions, BM also significantly increased serum prolactin levels while simultaneously leading to a reduction in breast engorgement score, breast pain score, maternal anxiety levels, and breast temperature. Furthermore, participants in the BM group demonstrated significantly better and excellent improvement in breast engorgement resolution (secondary outcome), with the important finding of a low incidence of adverse events.
BM has been proposed as a nonpharmacological intervention with evident potential to enhance milk production in both preterm and postpartum mothers.16–28 Additionally, the positive results from two RCTs suggest that BM can increase serum prolactin level, supporting a biological mechanism for enhanced milk production. A low milk production can be caused by problems such as blocked ducts, engorgement, and mastitis, or by factors affecting the mother–infant dyad, including prematurity. 41 A review of the literature found that several BM methods, such as Tuina massage, oxytocin massage, circular and oscillating BM, Thai traditional massage, hypno-breastfeeding massage, and major myofascial release massage, all aim to increase milk production and reduce pain from engorgement.
Our results are consistent with those of other SRs. A review published from 2018 to 2022, 42 which included two RCTs and 11 quasi-experimental studies, found that the most common method for stimulating breast milk flow is massage. These studies utilized diverse techniques and approaches, including traditional Thai massage, oil massage, self-massage of the breast, or BM using various specific movements (e.g., the butterfly wing movement, fingertip rotation, and the diamond sparkling position). However, all reported methods involved massaging the nipples, areola, breasts, and the area under the armpits.
Similarly, a SR published in 2019 43 suggested that Oketani BM, when combined with simultaneous and sequential pumping, may support the breastfeeding process. Another review, 44 which synthesized 5 RCTs and 17 quasi-experimental studies (2013–2020), discussed various massage techniques—such as oxytocin, back, neck, and Oketani massage. However, rather than definitively increasing absolute milk volume, these interventions were primarily associated with improved clinical indicators of milk transfer, such as increased frequency of infant urinations, and enhanced maternal comfort.
BM enhances breast milk production through several proposed mechanisms, including stimulating breast tissue, enriching breast milk with calories, and increasing the overall milk volume. This is achieved by reducing tissue tension and increasing the flexibility of the breast base and pectoralis major muscles,45,46 stimulating the milk flow reflex,47,48 or stretching the breast muscles. 49 It also helps reduce stress, which affects the functioning of the interplay between the hypothalamus, pituitary gland, and adrenal gland. When stress hormones (cortisol) are reduced, hormones related to milk production (prolactin) and secretion work more efficiently. Initially, postpartum mothers often experience fatigue from childbirth, insufficient rest, and anxiety about adjusting to their motherly roles, and this stress and muscle tension can interfere with the initial milk production process, or lactogenesis II. 50
Our positive results from five RCTs suggest that BM can reduce breast engorgement, confirmed by the six-point engorgement scale 21 and the rubber hardness tester. 25 Furthermore, three RCTs measured the resolution of breast engorgement using the number of participants showing improvement. Breast engorgement arises from the increased vascularity and accumulation of milk and secondarily from lymphatic and vascular congestion, 51 leading to signs such as tenderness with painful breasts, interstitial edema, increased breast volume, 52 shiny skin, flattened nipples, with or without accompanying diffuse and reddened areas, 51 and elevation of body temperature, including a febrile state. A reduction in temperature occurs after the breasts are emptied. 37 Since breast pain is a significant factor affecting the duration of breastfeeding, 37 offering a treatment that reduces pain levels immediately may allow mothers to continue breastfeeding.
The positive results from two RCTs included in this review suggest that BM can significantly reduce breast pain. These studies measured pain as an outcome for common breastfeeding problems such as blocked ducts, engorgement, and mastitis, using the validated VAS score. Furthermore, four RCTs indicated that BM can reduce breast temperature.
BM helps alleviate breast engorgement, pain, and elevated temperature by stimulating blood and lymph circulation, allowing the milk ducts to relax and drain milk more effectively. This action helps reduce edema, resulting in a softer areola.22,26,38
Our findings regarding the reduction of breast engorgement and pain are consistent with the available literature. For instance, a previous SR published in 2019, 43 which included three RCTs and three quasi-experimental studies (2001–2015), also supported pain reduction. Since reducing pain for breastfeeding women is an important strategy for increasing breastfeeding rates, in line with the WHO recommendation of exclusive breastfeeding for 6 months, BM holds significant clinical value. Five of the six studies reviewed in the aforementioned SR measured pain using validated tools such as the VAS or Numeric Rating Scale (NRS), although differences in their application were noted across studies.
Postpartum blues frequently occur after childbirth, and the associated maternal stress can inhibit the flow of breast milk production. 53 Anxiety is one of the key symptoms of postpartum blues. Anxiety commonly seen in new mothers includes concerns about infant care, the feeling of not producing sufficient breast milk to satisfy the baby, and distress over a constantly crying baby or one who refuses breastfeeding. Psychological, social, and spiritual stress influences the hypothalamus, which, in turn, affects the pituitary to secrete adrenocorticotropic hormone. This cascade ultimately influences the adrenaline response, resulting in the release of cortisol. 54
Anxiety or stress experienced by postpartum mothers is a significant risk factor influencing the early cessation of breastfeeding. This early stoppage contributes to the high rate of exclusive breast milk failure, particularly in regions like Indonesia. 55 Based on current analysis, suboptimal breastfeeding practice, including nonexclusive breast milk feeding, contributes approximately 11.60% to infant mortality among children under 5 years old. 56
Our positive results from four RCTs suggest that BM can effectively reduce anxiety levels, as measured using the STAI. Massage and relaxation may help balance maternal hormones after childbirth. Oxytocin is produced in the hypothalamus, stored in the posterior pituitary gland, and released following stimulation from both massage and infant suckling. 57 Massage therapy is known to increase positive responses, such as feelings of welfare, enjoyment, and comfort, while decreasing negative emotions, such as anxiety, pain, stress, loneliness, and trauma due to physiological symptoms. 58
Regarding infant outcomes, two RCTs measured the number of infant urinations and defecations per day on Day 3. The number of urinations recorded on the final day was significantly higher in the BM group than in the control group. This finding is consistent with a previous SR that included two quasi-experimental studies. 44 However, the number of defecations recorded on the final day showed no significant difference between the BM and the control groups.
The effectiveness of BM in this meta-analysis should be interpreted alongside the Academy of Breastfeeding Medicine (ABM) Clinical Protocol #36 (2022). 59 The ABM protocol cautions against aggressive massage due to risks of tissue trauma and increased inflammation within the mastitis spectrum. However, a clear distinction exists between the aggressive techniques criticized by the ABM and the gentle manual interventions reviewed in our studies.
The techniques analyzed in this meta-analysis, such as Oketani and lymphatic-based methods, prioritize rhythmic and gentle manipulation. Unlike aggressive pressure that may cause capillary injury, these methods facilitate lymphatic drainage and reduce intramammary pressure. Our findings suggest that therapeutic touch acts by mitigating interstitial edema. This reduction in fluid pressure alleviates ductal compression and improves milk flow, which is a mechanism consistent with the ABM recommendation for gentle edema management.
While the ABM protocol warns against massage as a general term, our data indicate that nonaggressive manual stimulation remains a valuable nonpharmaceutical tool. We propose that clinical practice should distinguish between harmful deep tissue pressure and beneficial edema-reducing touch. When practiced gently, manual breast stimulation safely enhances the neuroendocrine and mechanical aspects of milk production without causing the tissue injury cautioned against in recent protocols.
The results of this study indicate that participants experienced significant improvement through the application of massage techniques (Table 2). This success was achieved by using gentle and consistent pressure, focusing on the reduction of interstitial edema and the stimulation of the neuroendocrine reflex. Crucially, hand expression was not utilized during the study process. This confirms that therapeutic massage using a delicate touch can directly and positively affect milk production and flow. This mechanism helps reduce internal pressure within the mammary ducts and enhances maternal relaxation without causing injury to the breast tissue.
Our findings provide reliable recommendations for BM to stimulate milk production in postpartum women, which may apply to a broader population, including postpartum, preterm, and cesarean-delivered mothers. Despite extensive evidence supporting breastfeeding, many mothers face challenges that can hinder successful breastfeeding and lead to premature discontinuation. A common problem reported by postpartum women is insufficient milk production, which may lead to concerns about the infant’s growth and well-being. Therefore, the strong evidence from this study supports the use of BM as a therapeutic intervention to address this critical challenge.
This review has several limitations. First, the distorting effects of publication bias and location bias in SR and MA are well documented.60,61 While we are confident that our search strategy identified all relevant studies, some uncertainty remains. Another potential source of bias is the preponderance of negative BM trials for lactation cessation being related to the staff’s lack of massage skills and expertise, resulting in the inclusion of only three such negative studies in our review.10,24,26 Our findings may also be affected by significant differences in the characteristics of various BM treatments, including frequency, duration, number of sessions, and massage technique, as our review included several types of BM (e.g., Tuina massage, oxytocin massage, circular and oscillating BM, Thai traditional massage, hypno-breastfeeding massage, and major myofascial release massage). Another point is that only one study reported adverse effects, underscoring the need for further research on the safety profile. Additionally, the variability in the treatment control groups, some of which received active intervention combined with other modalities, further limits the study. Given these limitations, establishing a basic BM standard is crucial for guiding further study, particularly regarding the mechanisms of influence.
Conclusion
BM is an effective intervention that significantly enhances breast milk production in postpartum women. Additionally, BM proves to be an effective intervention for decreasing common discomforts, including breast engorgement, breast pain, and maternal anxiety levels. The intervention may also contribute to improved outcomes, such as a decrease in breast temperature and an increase in the number of infant urinations. However, to fully establish its safety profile across diverse populations and techniques, more studies and reports on the adverse effects of BM in postpartum mothers should be conducted.
Authors’ Contributions
C.C., W.P., R.P., S.W., and N.N. contributed to the conception and design. C.C. and W.P. contributed to data acquisition or analysis and interpretation of data. C.C., W.P., and N.N. were involved in drafting the article. C.C. and W.P. revised the article critically for important intellectual content. All authors have given final approval for the version to be published.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
Did not receive any funding.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.