
Abstract
Introduction:
Given the functional, emotional, and symbolic challenges imposed by cleft lip and/or palate (CL/P) on exclusive breastfeeding (EBF), mothers often experience early breastfeeding cessation with impacts on maternal identity and the mother–infant bond. This study aimed to explore the meanings, feelings, and experiences of mothers of children with CL/P regarding breastfeeding in the face of these adversities.
Methods:
This qualitative study applied the Clinical-Qualitative Method as proposed by Turato. Six in-depth semistructured interviews were conducted with biological mothers of children with CL/P, recruited from a specialized craniofacial reference center in Brazil. Data were analyzed using a qualitative content analysis approach, grounded in psychodynamic concepts from the Medical Psychology theoretical framework.
Results:
Based on the analysis of the collected material, three analytical categories were identified and constructed: (1) “Existential conflict regarding the inability to fulfill the ideal maternal role”; (2) “Duality between the need and the fear of caregiving”; and (3) “The anguish experienced between tangible and intangible support during breastfeeding.”
Conclusions:
Although the inability to EBF in children with CL/P generates emotional distress, motherhood is reimagined through adaptive forms of care and bonding, highlighting gaps in institutional support and the need for more humanized, emotionally sensitive health practices.
Introduction
Cleft lip and/or palate (CL/P) are congenital orofacial malformations resulting from disruptions in embryonic facial developmental processes, leading to discontinuities in the lip region, termed cleft lip (CL), or in the palatal region, termed cleft palate (CP), when there is communication between the oral and nasal cavities. These conditions may occur independently or in association with one another.1,2
CL/P are the most common malformations affecting the head and neck region, with a prevalence in Brazil of approximately 1 in 2,700 individuals 3 ; These conditions are multifactorial in nature and, therefore, do not have a single defined cause. Globally, this lack of fusion of facial processes affects between 1 in 500 and 2,500 live births. 2 As deformities that involve the mouth and the midface, children with CL/P may experience a wide range of adversities related to speech, including communication, hearing, learning, psychosocial development, and feeding. 4
Can directly interfere with the establishment and maintenance of exclusive breastfeeding (EBF), particularly due to structural alterations that impair effective suction and oral seal. These difficulties emerge early in the postpartum period, often before therapeutic interventions are initiated, and may lead to early interruption of breastfeeding. Although surgical repair, such as cheiloplasty and palatoplasty, is an essential component of treatment and occurs within the first months of life, feeding challenges are present from birth and can significantly affect both infant nutrition and maternal experience.
Infants with CL/P are often unable to maintain adequate suction and oral seal at the breast, which complicates or prevents EBF. According to the World Health Organization (WHO) and the American Academy of Pediatrics, ideally, children should be EBF until 6 months of age, given the associated benefits. 5 Beyond its biological function, breastfeeding also encompasses emotional and symbolic dimensions, being closely linked to the mother–infant relationship and maternal identity. 6 The scientific literature also highlights the relevance of EBF, with improved cognitive development and socioaffective outcomes in children, as well as reduced anxiety and stress in mothers.5,7
However, difficulties experienced by mothers contribute to the early cessation of EBF, 8 resulting in breastfeeding rates below international recommendations. In the context of CL/P, these challenges may be intensified due to feeding impairments such as oropharyngeal dysphagia and the inability to achieve an effective latch, which can compromise nutritional intake and hinder adequate weight gain required for surgical interventions.4,9,10
In this context, the benefits of a multidisciplinary approach to the management of these patients and their families are emphasized in a comprehensive, collaborative, and patient-centered manner in order to address complex medical and surgical needs of individuals with CL/P. 4 Beyond clinical management, mothers face multifaceted challenges that may compromise the initiation and maintenance of EBF. These include biological hurdles, such as managing the anatomobiological feeding difficulties inherent to the infant’s condition; 8 social pressures, involving the stigma of giving birth to a child perceived as imperfect; and psychological demands arising from fantasies associated with fears of handling, injuring, or even drowning the infant. Furthermore, these mothers often navigate the grief stemming from the disidealization of motherhood stereotypes, particularly regarding the perceived failure to fulfill the cultural ideal of EBF.
Such intra- and interpersonal conflicts significantly influence maternal confidence, expectations, and decision-making, often contributing to the early cessation of EBF. 11 These experiences extend beyond technical or biological hurdles, involving complex meanings tied to maternal identity, caregiving, and the mother–infant bond. Despite the profound relevance of these dimensions, qualitative studies exploring mothers’ perceptions of breastfeeding within the context of CL/P remain limited, highlighting a critical need for further investigation.
Accordingly, this study is guided by the assumption that EBF in the context of CL/P constitutes a complex and multidimensional experience, shaped by emotional, symbolic, and social factors, which may influence maternal identity, the mother–infant bond, and the meanings attributed to care.
In light of this, the present study aimed to explore the meanings and experiences of biological mothers of children with CL/P regarding breastfeeding in the face of the challenges imposed by the condition. Particular attention was given to how these women construct breastfeeding experiences and navigate emotional, relational, and contextual dimensions, including the role of family and institutional support. This study addresses a gap in the scientific literature, as qualitative investigations focusing on the subjective and emotional dimensions of breastfeeding in this context remain limited. By advancing understanding of these experiences, the findings may contribute to the development of more humanized, comprehensive, and emotionally responsive health care practices.
Method
Overview
The methodology of this study was designed based on phenomenology, understood as an approach that seeks to explore and interpret individuals’ lived experiences and the meanings they attribute to a given phenomenon, advocated by E. Husserl, and detailed through the Clinical-Qualitative Method (CQM), 12 enabling the exploration of mothers’ meanings regarding breastfeeding in children with CL and/or CP. In-depth interviews were conducted using open-ended questions, aiming to address the topic flexibly and to obtain information, perceptions, and experiences from the interviewees within their work environments. 13
The CQM allows for the identification and interpretation of emotional meanings present in participants’ speech and in what is left unsaid by valuing the narratives of those who bear the natural suffering of human anguish and by considering the presence of nonconscious emotional elements during interviews and in the interpretation of statements. The preparation and reporting of this article followed the guidelines of the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist, ensuring methodological rigor and transparency in the conduct of the qualitative research.
The present project was submitted to the Research Ethics Committee (REC) of the Piracicaba School of Dentistry, University of Campinas (FOP/Unicamp), Brazil, and was approved under CAAE No. 87152725.2.3001.5441, opinion number 7493457: Piracicaba, Campinas-SP, Brazil, April 8, 2025.
Research setting
The Hospital de Reabilitação de Anomalias Craniofaciais (USP, Brazil) (Hospital for Rehabilitation of Craniofacial Anomalies) is a national and international referral center for the comprehensive care of individuals with CL and/or CP and other craniofacial anomalies. Originally founded in 1967 as an interdepartmental center for university studies, it was officially designated as a hospital in 1976. It provides specialized and continuous care through a multiprofessional approach, involving fields such as dentistry, medicine, speech-language pathology, nursing, psychology, social work, and nutrition, accompanying patients from birth through adulthood.
In addition to its clinical activities, the hospital stands out for its scientific production, training of health care professionals, and development of research focused on functional, aesthetic, and psychosocial rehabilitation, constituting a privileged setting for investigations that seek to understand the clinical, social, and subjective dimensions related to CL/P and the caregiving experiences of patients and their families.
Sampling and recruitment
The study population comprised six biological mothers aged between 20 and 42 years. The eligibility criterion was being a user with a child with CL and/or CP. The participants included both first-time and multiparous mothers, with varying levels of prior breastfeeding experience. Most reported limited access to structured breastfeeding counseling specific to CL/P, particularly during the prenatal and immediate postnatal periods. Participant characteristics are described in Table 1.
Sociodemographic Characterization of the Interviewees, Bauru SP, Brazil, 2025
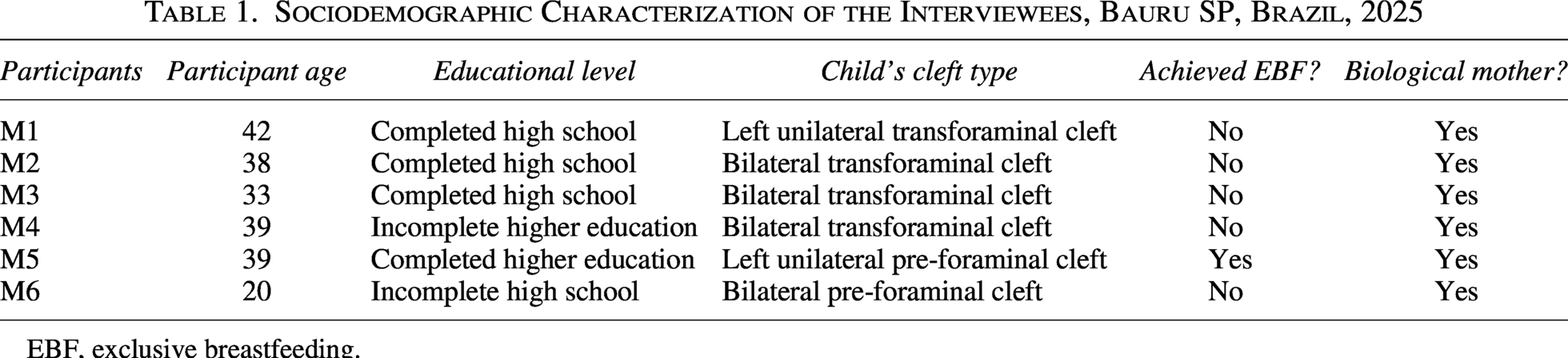
EBF, exclusive breastfeeding.
Data collection was guided by the principle of theoretical saturation, understood as the point at which no new relevant themes or meanings emerged from the data.11–13 Saturation was assessed concurrently with data collection and analysis through iterative examination of interview transcripts and the development of analytical categories. After the sixth interview, no substantially new elements were identified, and the categories were considered sufficiently dense and consistent, supporting the decision to conclude recruitment.
Recruitment presented practical challenges due to the specific inclusion criteria. Although initial acceptance was common, some participants did not respond to follow-up contact or declined participation.
To ensure methodological rigor, two preliminary acculturation interviews were held with eligible participants to refine the interviewer’s technique and mitigate bias. Given the lead author’s clinical history as a long-term patient with CL/P at the facility, a deliberate defamiliarization strategy was employed to safeguard an objective research perspective. Following these steps, the lead author—a female dental undergraduate and research scholar—conducted all formal interviews under the supervision of senior researchers experienced in the CQM. The purpose of these acculturation and defamiliarization strategies is to gain a profound understanding of participants’ perspectives, values, norms, and behaviors by directly observing and engaging with their cultural practices. 12
The researcher established initial contact with the users within the hospital environment. After an explanation of the interview and acceptance of the invitation to participate, the Informed Consent Form (ICF) was provided, discussed, and signed.
Qualitative data collection
Interviews were initiated only after obtaining participants’ signatures on the ICF. Regarding the data collection method, a semidirected in-depth open-ended interview guide was employed, characterized by the inclusion of core questions grounded in theories and hypotheses related to the research topic. This format allows for the emergence of new theories and questions arising from participants’ responses. In addition, it is distinguished by the active and conscious presence of the researcher throughout the information-gathering process.
The interview guide was developed with the following triggering question: “How do you feel about breastfeeding your child?”. As accessory questions used to deepen the participants’ narratives, we included the following: “How is breastfeeding for you? Or not breastfeeding?”; “How has this process been for you?”; “How do you feel/felt about being a mother who does not breastfeed? Or who breastfeeds?”; “How has not being able to breastfeed affected you?”; “Tell me more about how you felt about this”; “‘[adjective used by the mother]’—how so?”; “What makes this ‘[adjective used by the mother]’ for you?”; “Does this not cause anything in you?”.
At the end of each interview, participants were asked about their emotional state and whether they wished to share any additional information. All details of the interview moment, such as the tone of voice, posture, and description of the environment, were carefully recorded in a field notebook.
The data were subjected to processing and validation through peer discussions with researchers from the Qualitative Study and Research Group (Gepeq) of Faculdade de Odontologia de Piracicaba—Universidade Estadual de Campinas (FOP/Unicamp), Brazil. This group, composed of a multidisciplinary team with training in various health fields (medicine, psychology, and dentistry, among others) and experience in conducting interviews, analyzed the performance, and provided suggestions regarding the content of the interview guide and the interviewer’s posture.
The responsible researcher conducted the interviews online via Google Meet, without the presence of observers. The interviews were audio-recorded and subsequently transcribed verbatim by the interviewer, preserving the fidelity of the statements for subsequent categorization and systematization. To ensure participants’ anonymity in the transcripts, their names were replaced with fictitious names.
Data analysis
Interview analysis was conducted using Clinical-Qualitative Content Analysis, following the Seven-Step technique proposed by Faria-Schützer et al. 14 As the interviews were completed, the principal author performed full transcriptions of participants’ statements on the same day, with the aim of examining the data in their entirety and promoting an articulated process of analytical immersion. This strategy sought to foster a deeper understanding of the internal logic and meanings present in the narratives.
The structuring of analytical categories, developed through interpretation of the narratives, was grounded in the theoretical-methodological propositions of dialectical hermeneutics, understood as an approach that integrates interpretation of meanings (hermeneutics) with critical analysis of contradictions and social contexts (dialectics), particularly in its data operationalization stages, which allow the researcher to situate themselves within the participants’ context as social actors.
Although dialectical hermeneutics encompasses three levels of interpretation, this study opted to use the second level, which is based on the observation of facts emerging during the investigation, as well as on individual narratives, subjective aspects, behaviors, customs, practices, and the meanings or significances attributed to the object of study. These elements were essential for the construction of the analytical categories.
Methodological rigor and trustworthiness were established through several strategies. First, the lead researcher underwent extensive theoretical training and participated in role-playing sessions with expert peers to refine interview techniques. Data collection and analysis were conducted under continuous supervision by the senior investigator, with periodic research group meetings to ensure the peer debriefing and plausibility of the findings. The study also adhered to the COREQ guidelines.
The trustworthiness of the method is grounded in the validity of the clinical-qualitative approach—a well-established framework in the human sciences for nearly three decades. By employing specialized listening and the free association of ideas, the researcher captured deep psychological meanings from the participants’ narratives. Furthermore, the credibility of the findings was bolstered by their presentation at scientific conferences and the receipt of an honorable mention from the examining board at the University of Campinas (Unicamp) School of Dentistry.
Results
The interviews had an average duration of 40 minutes. Participants presented diverse maternal experiences, including both first-time and experienced mothers, with varying degrees of prior breastfeeding exposure and access to professional guidance. Based on the analysis of the collected material, three analytical categories were identified and constructed:
“Existential conflict regarding the inability to fulfill the ideal maternal role.” “Duality between the need and the fear of caregiving.” “The anguish experienced between tangible and intangible support during breastfeeding.”
Category 1: Existential conflict regarding the inability to fulfill the ideal maternal role
The participants’ statements revealed the emotional impact of the inability to EBF, experienced as a rupture with the idealization of motherhood. Mothers reported frustration, sadness, and a sense of helplessness, expressing how the act of breastfeeding is imbued with symbolic meanings and understood as an essential gesture of love, bonding, and personal fulfillment. The absence of this experience was perceived as a failure in their maternal role, as illustrated by the excerpts below.
“I felt bad at the time, you know… because we have this whole dream, this hope of holding your little baby… being able to breastfeed…” (M1)
“I felt like an incomplete mother, for not being able to feed my daughter with what I had, you know?” (M4)
“There are people who don’t do it because they don’t want to, and I didn’t because I couldn’t. It wasn’t because I didn’t want to. That’s what hurts. It’s the minimum we can do for our child, right? And I couldn’t do it.” (M2)
In the narratives, breastfeeding emerges as a milestone of idealized motherhood, associated with love and maternal competence. The difficulty in directly providing breast milk to the child triggered feelings of guilt, incapacity, and inferiority, in addition to generating comparisons with other women who were able to breastfeed.
“Why do others manage and I don’t? […] I started to feel frustrated. I just cried.” (M4)
“I had prepared myself for breastfeeding with breast milk. I thought I would breastfeed him. I never imagined I would have to give him a bottle before six months.” (M6)
Participants also expressed attempts to reframe this experience, recognizing their efforts to offer what they could within their possibilities. Even when they were unable to breastfeed, they sought to maintain contact with the baby and provide their milk in other ways, attempting to preserve the bond.
“I expressed my milk… as much as I could… I gave it to him… but it wasn’t the same feeling as having him at my breast.” (M3)
Overall, this category highlights the confrontation between the “ideal mother,” nurturing, complete, and capable, and the “real mother,” who faces physical and emotional limitations imposed by the child’s condition. This conflict manifests in the constant attempt to reconcile maternal love with the pain of not meeting socially constructed expectations regarding the role of motherhood.
Category 2: Duality between the need and the fear of caregiving
The narratives reveal a constant fear of causing pain or exacerbating the infant’s suffering, especially during feeding or when handling the child. Care, which should represent closeness and affection, was initially experienced with tension, insecurity, and anxiety.
“When it was time to feed him, I would do it terrified, tense, afraid of him choking or something happening.” (M2)
“I felt really bad, I started crying, I panicked, because every time I tried to give him the bottle, he would spit it out.” (M6)
“Sometimes I look at him… and I get scared… because I see that it bothers him… and that hurts me, you know? Because I feel like he’s suffering.” (M1)
The fear of hurting the baby and of being unable to ensure their safety intertwines with the need to care for and feed the child. This ambiguity seems to generate a constant tension in which care and fear overlap. Mothers described that, over time, they gradually gained confidence in caregiving as they received guidance or noticed improvements in the child’s condition; however, the beginning of the process was permeated by guilt, crying, and despair.
“You’re terrified, right? My God, what if I hit it and the tube comes out! But I think the one who’s more afraid is us, because the baby doesn’t really suffer, right?” (M4)
Observing the baby’s weight gain and development brought relief and hope, allowing mothers to begin to perceive caregiving as something possible and rewarding.
“Now he’s gained weight… I can see that he’s healthy… the doctor said he’s doing well, that he’s strong… and if it continues like this, he’ll already be able to have the surgery.” (M1)
This category highlights how maternal caregiving is permeated by contradictory feelings, the desire to protect and the fear of failing, demonstrating that motherhood is experienced in a constant conflict between love and anguish, shaped by idealizations associated with being a mother.
Category 3: The anguish experienced between tangible and intangible support during breastfeeding
The lack of professional welcoming and the absence of guidance were mentioned by several participants, who reported indifference and insensitive comments from some health professionals. As previously described in the literature, 15 tangible support refers to concrete and measurable elements that structure care, expressing its objective and operational dimension. Intangible support, in turn, encompasses the subjective and immaterial aspects that sustain caregiving relationships, translating values, affections, and modes of interaction that, although not quantifiable, are essential to the experience of being cared for and of caring.
In the absence of institutional support, mothers sought support in affective and spiritual networks, which emerged as sources of emotional sustenance and hope. Faith and religiosity were identified as central elements for coping with suffering, functioning as a refuge and a source of strength to continue the caregiving process.
“Faith… God was my support there… all the time…” (M3)
“It can also be something spiritual, from other lives, that she needed to go through this, for those who believe, right?” (M4)
The search for spiritual meanings for what occurred reflects an attempt at symbolic reconstruction of the experience, transforming pain into learning and reaffirming hope in the child’s recovery. This intangible dimension of support, represented by faith, beliefs, and affective bonds, emerged as essential for coping with suffering, especially in the face of precarious technical and informational support. The narratives reveal a feeling of helplessness resulting from the lack of information and guidance during the prenatal and postnatal periods. Participants reported that they often did not receive adequate explanations about the cleft condition or about how to manage the necessary care, which generated confusion, fear, and loneliness.
“You feel alone, helpless, because no one says, look, this is going to happen, this and this, you’re going to have to do it like this, like this, like this.” (M4)
“I was lost… because then he was born, they put him close to me, took him away, and I didn’t know anything. It’s a very bad feeling.” (M2)
Discussion
The categories that emerged in this study reveal the symbolic and emotional complexity of the maternal experience in the face of CL/P, exposing tensions between the biological body, the social role of motherhood, and the available institutional support. Motherhood, historically constructed as an ideal of completeness and self-sacrifice, appears here permeated by pain, guilt, and the need for redefining, reaffirming that maternal care is also a field of dispute between the natural and the social, the possible and the expected. The first category, “Existential conflict regarding the inability to fulfill the ideal maternal role,” demonstrates how the imagining of motherhood remains strongly linked to the idea of perfection and fullness, with breastfeeding as one of its main symbols. Altamiro Camacho 16 points out that the discourse of “maternal instinct” was historically shaped by an ideology that naturalizes love and places almost exclusive responsibility for the care and nourishment of children on women. In the context of this study, the inability to EBF caused a rupture between the social ideal and the lived experience, generating feelings of frustration, helplessness, and guilt.
These emotions, often internalized as personal failures, reflect a process of gendered attribution of guilt that persists within biomedical and social discourses on motherhood. Official discourse, in most cases, does not treat women as subjects, but rather as instruments necessary for providing breast milk, the best food, to the child. These are prescriptive and imperative discourses of the WHO, grounded in a historical struggle against infant mortality, whose expressions, such as “breastfeed exclusively until 6 months” and “give your child what is best,” end up producing women who feel guilty or ashamed for not wanting to or not being able to breastfeed. 17 The participants’ statements suggest that the “failure” to breastfeed goes beyond the biological dimension, reaching the realm of identity and self-esteem, corroborating the findings of other authors 18 regarding the social value of breastfeeding as a “measure of the mother.” Nevertheless, a movement of redefining is observed: By seeking other ways to feed and welcome their children, mothers begin to construct new meanings for care, demonstrating adaptation and relational learning. This process, often painful, illustrates a form of “re-existence” that enables the creation of meaning in contexts marked by loss and limitation, thereby bringing into discussion their roles within the family and society.
In the second category, “Duality between the need and the fear of caring,” the act of caring emerges permeated by contradictory feelings, in which love and fear intertwine within the same movement. The fear of hurting the baby, of failing in feeding, or of causing pain reveals that care is not only limited to an affectionate action but also constitutes an experience of vulnerability, in which the maternal body confronts its own boundaries and uncertainties. Zani and Jarussi 19 corroborate these findings, noting that mothers of premature newborns also experience this duality in care. This tension arises from the perception of the child’s fragility and from awareness of their own limitations in the face of caregiving demands. Insecurity also reflects the absence of continuous technical and emotional support from health services. Authors 20 indicate that the first contact with the baby may be marked by fear and rejection and that the presence of welcoming professionals is decisive for the construction of the maternal bond.
Thus, the gradual overcoming of fear and the strengthening of the bond observed in the narratives of the participants in this study are also articulated with the notion of autonomy built through affection, including that arising from relationships between health professionals and patients. Even so, as mothers come to understand the specificities of their children and experience small victories, such as weight gain or success in safe feeding, they begin to conceptualize care as an expression of love rather than merely an obligation, reaffirming their competence and their role.
Finally, the third category, entitled “The anguish experienced between tangible and intangible support during breastfeeding,” broadens the analysis to the social and institutional field, where the absence of clear information, poor communication with health professionals, and the symbolic neglect reported by mothers highlight structural failures in the care network, especially at the interface between birth and multiprofessional follow-up. The feeling of abandonment points to a rupture of the pact of trust between patients and health services, in which care should be comprehensive, humanized, and shared, which may directly influence breastfeeding, according to the findings of Trettene et al. 21
Statements that mention “bad luck” or “misfortune” attributed by professionals reinforce the persistence of stigmatizing attitudes that disregard the subjective dimensions of the maternal experience, echoing “dehumanized care,” marked by fragmented attention and a lack of bonding between professional and patient.
Faced with this institutional “void,” participants turned to alternative sources of support, spirituality, faith, and affective networks, as forms of coping and reconstruction of suffering. Religiosity, in its various expressions, emerges as an instrument of emotional resilience and existential meaning, offering comfort in the face of uncertainty. This phenomenon is particularly evident among mothers who experience the loss of a child or deal with severe health problems, where faith serves as a symbolic technology of care, providing comfort and meaning amid suffering, as demonstrated by the study of Freitas et al. 22
This immaterial dimension of care is articulated with the concept of expanded care, as discussed by Castro, 23 in which comprehensiveness is not restricted to the sum of technical practices but involves recognizing the other in their biological, social, and spiritual totality. By reinterpreting their pain through faith, mothers demonstrate that spirituality, far from being an escape, can be a powerful way to reorganize lived experience and strengthen the bond with the child.
Thus, the three categories reveal that the maternal experience regarding the feeding of children with CL/P is marked by a process of mourning and reconstruction: Mourning for the socially constructed ideal of motherhood that is lost, mourning for the body that fails, but also reconstruction through the creation of new meanings and forms of care. This journey requires a subjective and social repositioning on the part of women, which is only possible when there are spaces for listening and welcoming. In this way, this study reaffirms the need for practices that value the subjective dimension of care through concrete interventions such as active listening, patient-centered communication, psychological counseling, culturally sensitive health education, and the inclusion of family members in the care process. Strengthening multiprofessional teams and fostering humanized dialogue between professionals and users can contribute to reducing guilt, strengthening bonds, and promoting a possible motherhood, not idealized, but lived in a dignified and comprehensive manner.
This study presents limitations inherent to the qualitative approach and the adopted design. The characterization of participants primarily considered age and educational aspects, which did not allow for a more comprehensive analysis of how broader sociodemographic dimensions, such as race, social class, economic vulnerability, and territorial context, may shape the experiences and meanings attributed to breastfeeding. A detailed characterization could contribute to a deeper understanding of how structural inequalities intersect with and reconfigure maternal lived experiences in this context, offering important directions for future investigations.
Conclusions
The maternal experience of feeding children with CL/P shows that, although EBF has historically been associated with the ideal of care and maternal competence, its impossibility, while emotionally impacting mothers, does not prevent the attribution of meaning to being a mother. In contrast, it reveals the capacity to reconstruct the bond through new forms of affection and care within a continuous process of adaptation and resignification. The lack of institutional support and adequate guidance exposes weaknesses in health care delivery, making humanized practices that embrace the emotional and social dimensions of motherhood essential.
Authors’ Contributions
A.L.A.F. contributed to conceptualization, investigation, data curation, formal analysis, and writing—original draft. C.V.B.A. contributed to conceptualization, methodology, formal analysis, supervision, and writing—review and editing. V.R.G. contributed to investigation, data curation, and writing—original draft. G.S.D. contributed to methodology, resources, and writing—review and editing. L.S.V. contributed to formal analysis, visualization, and writing—review and editing. R.A.B. contributed to methodology, validation, and writing—review and editing. N.S.G.R. contributed to project administration, supervision, and writing—review and editing. L.M.G contributed to conceptualization, supervision, funding acquisition, and writing—review and editing.
Data Availability
After publication, the data are available from the authors upon reasonable request, as justified in the article.
Ethical Approval
This project was approved by the REC of the Faculdade de Odontologia de Piracicaba, Universidade Estadual de Campinas (FOP/Unicamp), opinion number 7493457: Piracicaba, Campinas-SP, Brazil, April 8, 2025.
Footnotes
Acknowledgments
The authors are grateful to the Diretoria Executiva de Apoio e Permanência Estudantil da Universidade Estadual de Campinas.
Disclosure Statement
No competing financial interests exist.
Funding Information
Diretoria Executiva de Apoio e Permanência Estudantil da Universidade Estadual de Campinas—Grant No. 01-P-194/2023 and 01-P-161/2024.