
Abstract
Background:
Patients with severe mental disorders (SMD) are at substantially elevated risk for metabolic syndrome (MetS), contributing to excess cardiovascular morbidity and premature mortality. Adverse childhood experiences (ACEs) have been associated with dysregulation of metabolic pathways, yet their contribution to MetS risk in SMD remains poorly understood.
Objective:
This study aimed to investigate the association between ACEs and MetS in outpatients with bipolar disorder (BD) and schizophrenia (SZ) in clinical remission and to identify independent and incremental predictors of MetS using a hierarchical analytical framework.
Methods:
This cross-sectional study included 140 outpatients with SMD (96 with BD and 44 with SZ) in clinical remission, recruited from a university hospital in Eastern Turkey. MetS was defined according to NCEP-ATP III criteria, and ACEs were assessed using the Turkish version of the Adverse Childhood Experiences Scale (ACE-TR). Hierarchical and multivariable logistic regression analyses were performed to examine factors associated with MetS.
Results:
MetS was highly prevalent in this sample (46.4%). ACE-TR total score was independently and consistently associated with MetS across all hierarchical models (odds ratio [OR] range: 1.68–1.77), with each one-unit increase conferring approximately 71% higher odds in the fully adjusted model (OR = 1.71; 95% confidence interval [CI] 1.26–2.32; P = 0.001). The number of hospitalizations was the only other independently associated variable (OR = 1.19; 95% CI 1.02–1.39). Sexual abuse (16.9% vs. 2.7%; P = 0.004), emotional neglect (63.1% vs. 30.7%; P < 0.001), and physical neglect (30.8% vs. 14.7%; P = 0.022) were significantly more prevalent in the MetS group. ACE-TR total score was positively correlated with waist circumference and triglyceride levels.
Conclusion:
The strong and consistent association between ACEs and MetS underscores the importance of trauma-informed care models in psychiatric practice, where metabolic comorbidity remains a leading cause of premature mortality.
Keywords
Introduction
Schizophrenia (SZ) and bipolar disorder (BD) are severe mental disorders (SMD) with a lifetime prevalence of approximately 1%, leading to substantial functional impairment.1,2 Compared with the general population, individuals with severe mental illness have a reduced life expectancy of approximately 12–15 years. Although suicide represents an important cause of premature mortality among individuals with mental disorders, most excess mortality in this population is attributable to cardiometabolic and other physical diseases. 3
Metabolic syndrome (MetS) is a clinical condition characterized by the co-occurrence of hypertension, abdominal obesity, hypertriglyceridemia, low high-density lipoprotein (HDL) levels, and disturbances in glucose metabolism, and it is considered one of the major determinants of cardiovascular mortality in individuals with SMD. 4 MetS is a common cardiometabolic condition affecting approximately 25%–33% of the general population. 5 Available evidence indicates that the prevalence of MetS is two to three times higher in individuals with SMD compared with the general population. In a systematic review by Vancampfort et al. examining 37 studies including approximately 7000 patients with BD, the prevalence of MetS in BD was reported as 37.3%. 6 In a meta-analysis by Mitchell et al. that included 71 publications from diverse samples, the overall prevalence of MetS among patients with SZ was reported as 32.5%. 7 Although the increased prevalence of MetS in individuals with SMD is partly attributable to genetic factors, it is primarily associated with illness duration, advancing age, the metabolic effects of antipsychotic and mood-stabilizing medications, lifestyle limitations, chronic stress processes, and disrupted neurobiological mechanisms.8,9 However, these mechanisms remain insufficient for clinically predicting which patients will develop MetS; therefore, this limitation requires the systematic evaluation of additional determinants.
Adverse Childhood Experiences (ACEs) encompass multiple early-life stressors, including emotional, physical, and sexual abuse, neglect, poverty, and household dysfunction. ACEs are well-established risk factors for psychiatric disorders and are considered high-impact risk indicators for MetS in the general population.10,11 In a large meta-analysis including 190,285 participants from diverse samples, childhood abuse was found to significantly increase the lifetime risk of obesity. 12 Similarly, exposure to multiple types of trauma in patients with SZ and BD has been shown to be associated with increased waist circumference. 13 A comprehensive systematic review examining the association between childhood trauma and obesity in adulthood demonstrated that 81% of the included studies reported a positive relationship between these two variables. 14 In the relationship between ACEs and MetS, multiple pathophysiological processes are thought to play a mediating role, including dysregulation of the stress response within the hypothalamic–pituitary–adrenal (HPA) axis, alterations in cortisol rhythm, autonomic hyperactivity, chronic inflammation, epigenetic modifications, and immunometabolic imbalances, along with behavioral risk patterns such as high-calorie dietary intake, low physical activity, sleep disturbances, and a predisposition to substance use.15–17 Nevertheless, findings regarding the ACE–MetS relationship remain inconsistent due to methodological heterogeneity, small sample sizes, and variability in the measurement of ACEs, and only a limited number of studies have specifically focused on individuals with SMD. Moreover, the majority of existing studies have been conducted in Western societies, and differences in cultural norms, family structures, and modes of trauma expression limit the generalizability of these findings to other sociocultural contexts. To the best of our knowledge, no study to date has systematically examined the association between ACEs and MetS in patients with SZ and BD within a Turkish clinical sample.
The present study aimed to address this gap by examining the ACE–MetS association in a non-Western clinical sample using standard NCEP-ATP III criteria, specifically to determine the prevalence of MetS in patients with SZ and BD, to investigate whether ACE total score is independently associated with MetS and related metabolic indicators, and to examine the distribution of ACE subtypes according to MetS status. A hierarchical logistic regression framework was employed, in which sociodemographic variables were entered first, followed by smoking and chronic disease status, clinical characteristics, and psychotropic medication classes, to evaluate whether the ACE–MetS association persists beyond each successive layer of adjustment. We hypothesized that higher ACEs score burden would be associated with increased odds of MetS independently of known clinical and pharmacological risk factors.
Materials and Methods
This cross-sectional study included adult patients aged 18–65 years who attended the outpatient clinic of İnönü University Turgut Özal Medical Center between July and October 2024. Eligible participants had a DSM-5 diagnosis of BD or SZ, had been followed regularly in the outpatient clinic for at least 6 months, and were in remission at the time of assessment. Patients with any comorbid psychiatric disorder apart from BD or SZ, intellectual disability severe enough to interfere with comprehension of the study questions, or neurological disorders associated with cognitive impairment were excluded.
Ethical approval for the study was obtained from the İnönü University Health Sciences Scientific Research Ethics Committee (Approval No: 2024/6177). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. All participants were informed about the scope and purpose of the study, participation was voluntary, and written and verbal informed consent was obtained from all participants.
MetS was assessed according to the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III, 2001) criteria. 18 Accordingly, a diagnosis of MetS was established when at least three of the following five components were present: waist circumference >102 cm in men and >88 cm in women; triglyceride (TG) levels ≥150 mg/dL or current use of relevant treatment; HDL cholesterol <40 mg/dL in men and <50 mg/dL in women or use of HDL-raising therapy; blood pressure ≥130/85 mmHg or use of antihypertensive medication; fasting plasma glucose (FPG) ≥110 mg/dL or treatment for hyperglycemia. For biochemical parameters, the measurements obtained at the time of the clinical visit were used for evaluation. Abdominal obesity was assessed by waist circumference measurement. Blood pressure measurements were performed at the brachial level using a digital sphygmomanometer after an adequate resting period.
Measures
Sociodemographic and clinical data form
A structured form was prepared by the researchers to systematically assess basic characteristics of the participants, including age, gender, educational level, diagnostic status, illness duration, number of previous psychiatric hospitalizations, type of psychotropic medications used, and presence of comorbid medical conditions.
Adverse Childhood Experiences Scale—Turkish Form
The ACE scale is a 10-item self-report instrument developed within the framework of the CDC–Kaiser Permanente study to assess exposure to abuse, neglect, and household dysfunction before the age of 18 years. 19 The ACE-TR score is calculated by summing the number of items endorsed with a “yes” response across these 10 domains, yielding a total score ranging from 0 to 10, with higher scores indicating a greater number of ACEs. The Turkish adaptation of the scale was validated by Gunduz and Anil. 20
Statistical analyses
All analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation or median (minimum–maximum), and categorical variables as number and percentage. The normality of continuous variables was assessed using the Kolmogorov–Smirnov test, and correlations between ACE-TR total score and clinical and metabolic parameters were examined using Spearman’s correlation analysis.
Hierarchical logistic regression analyses were conducted to examine the stability of the ACE–MetS association across sequential adjustment for sociodemographic, behavioral, clinical, and pharmacological covariates, with independent variables entered in theoretically and clinically informed blocks. The unadjusted association was assessed in Model 1. Model 2 adjusted for sociodemographic variables (age, sex, and education level); Model 3 additionally included smoking status and presence of chronic disease; and Model 4 further incorporated clinical variables (psychiatric diagnosis, age at illness onset, number of hospitalizations, and number of suicide attempts). Models 5 through 8 introduced psychotropic medication variables sequentially: mood stabilizer use (Model 5), typical antipsychotic use (Model 6), atypical antipsychotic use (Model 7), and antidepressant use (Model 8). Model fit was evaluated using the −2 log likelihood, Cox & Snell R2, and Nagelkerke R2 statistics, alongside the Hosmer–Lemeshow goodness-of-fit test, with P > 0.05 indicating acceptable fit. Changes in explanatory power across successive models were interpreted on the basis of reductions in −2 log likelihood and increases in pseudo-R2 values. Results were expressed as regression coefficients (B), odds ratios (ORs), 95% confidence intervals (CIs), and P-values.
To complement the hierarchical approach and identify factors independently associated with MetS, a fully adjusted multivariable logistic regression model was also estimated using the Enter method, in which all independent variables were entered simultaneously. Statistical significance was set at P < 0.05 (two-tailed).
RESULTS
Participant characteristics
The study included 140 participants with a mean age of 42.54 ± 11.39 years. The sample comprised 96 individuals with BD (68.6%) and 44 with SZ (31.4%). Men represented 55.7% of the sample and women 44.3%. Most participants were single (63.6%), unemployed (66.4%), and had grown up in an urban setting (74.3%). Current smoking was reported by 46.4% of participants, while 34.3% had a history of chronic disease. The median ACE-TR total score was 2 (range: 0–6). The sociodemographic characteristics of the patients are summarized in Table 1.
Sociodemographic and Clinical Characteristics of the Study Sample
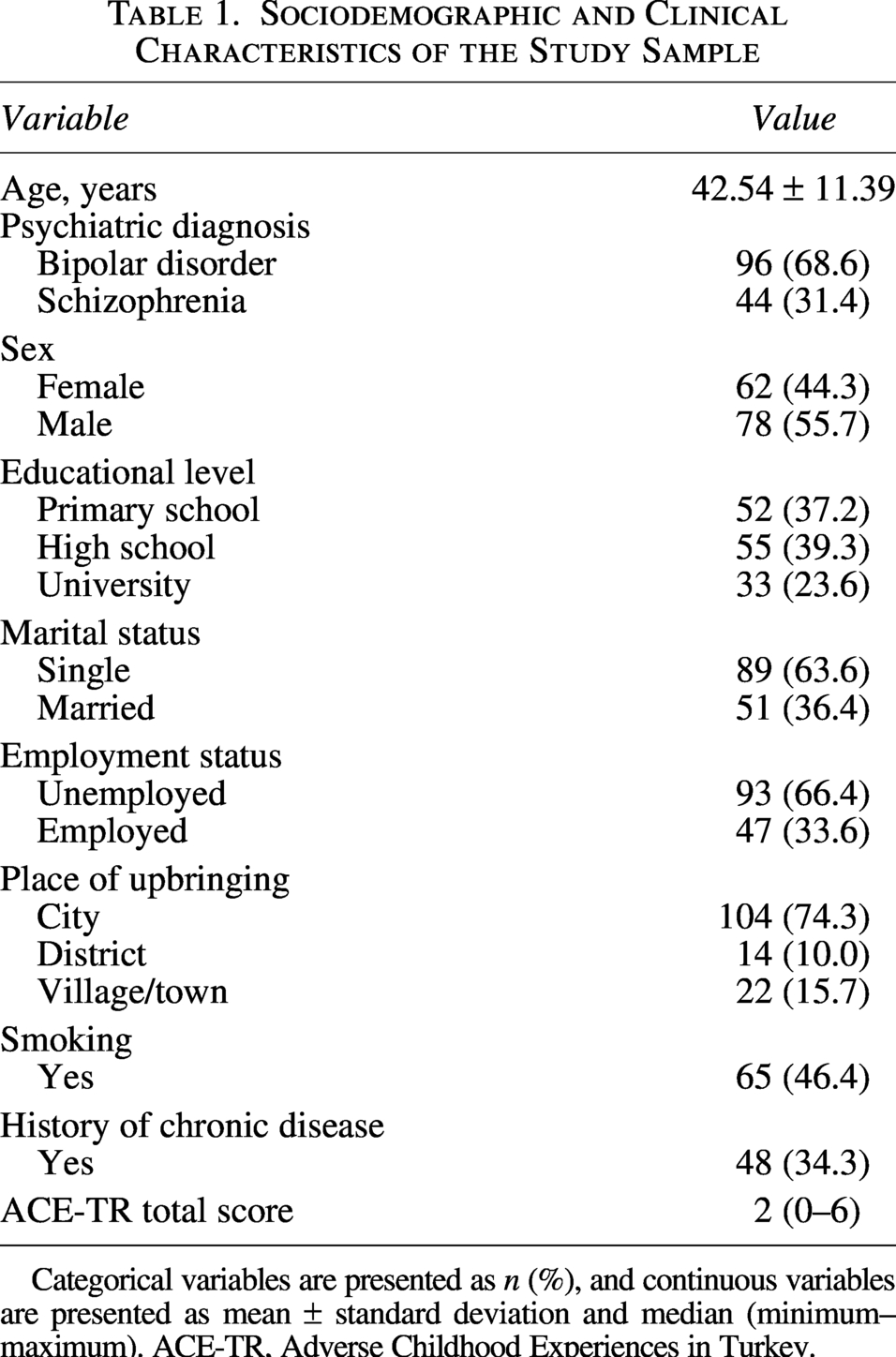
Categorical variables are presented as n (%), and continuous variables are presented as mean ± standard deviation and median (minimum–maximum). ACE-TR, Adverse Childhood Experiences in Turkey.
Clinical and metabolic characteristics of the study sample
Participants had a mean illness duration of 16.25 ± 9.26 years and a median age at illness onset of 23 (range: 12–55) years. The median number of hospitalizations was 2 (range: 0–30), and 26.4% of the sample had a history of suicide attempt. Mood stabilizers and atypical antipsychotics were the most frequently used medications, reported in 67.9% and 80.7% of participants, respectively. The mean waist circumference was 99.63 ± 13.24 cm, and the prevalence of MetS was 46.4%. These findings are summarized in Table 2.
Clinical and Metabolic Characteristics of the Patients
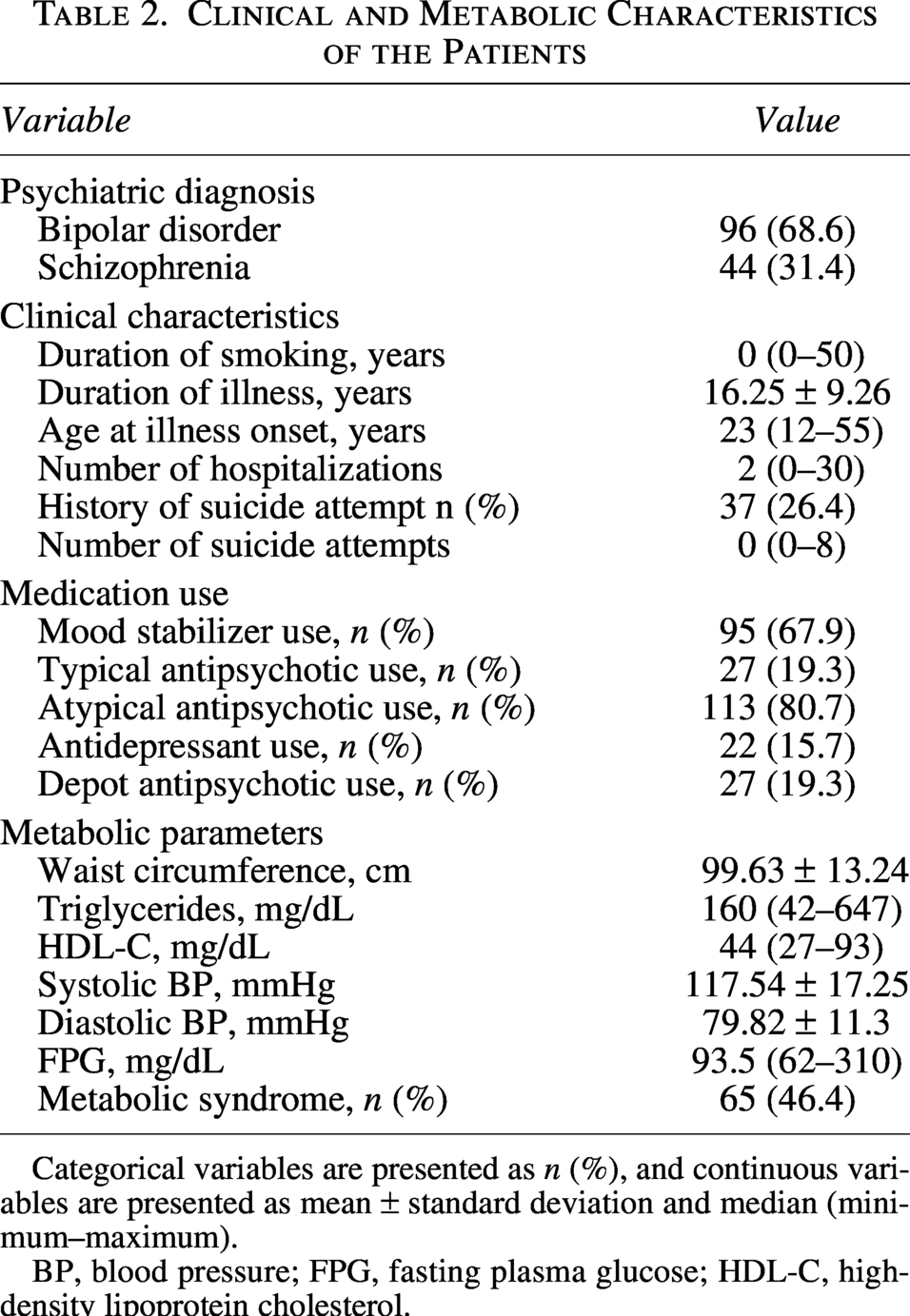
Categorical variables are presented as n (%), and continuous variables are presented as mean ± standard deviation and median (minimum–maximum).
BP, blood pressure; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol.
Correlations between ACE-TR total score and clinical and metabolic variables
Table 3 presents the Spearman correlation coefficients among the study variables. ACE-TR total score was significantly and positively correlated with waist circumference, TG level, number of hospitalizations, smoking amount, and duration of smoking, with the strongest association observed for TGs (r = 0.329, P < 0.001). By contrast, ACE total score was not significantly correlated with HDL-C, blood pressure, FPG, number of suicide attempts, or age at illness onset. These results are summarized in Supplementary Table S1.
Association between ACE-TR Total Score and MetS across Hierarchical Logistic Regression Models
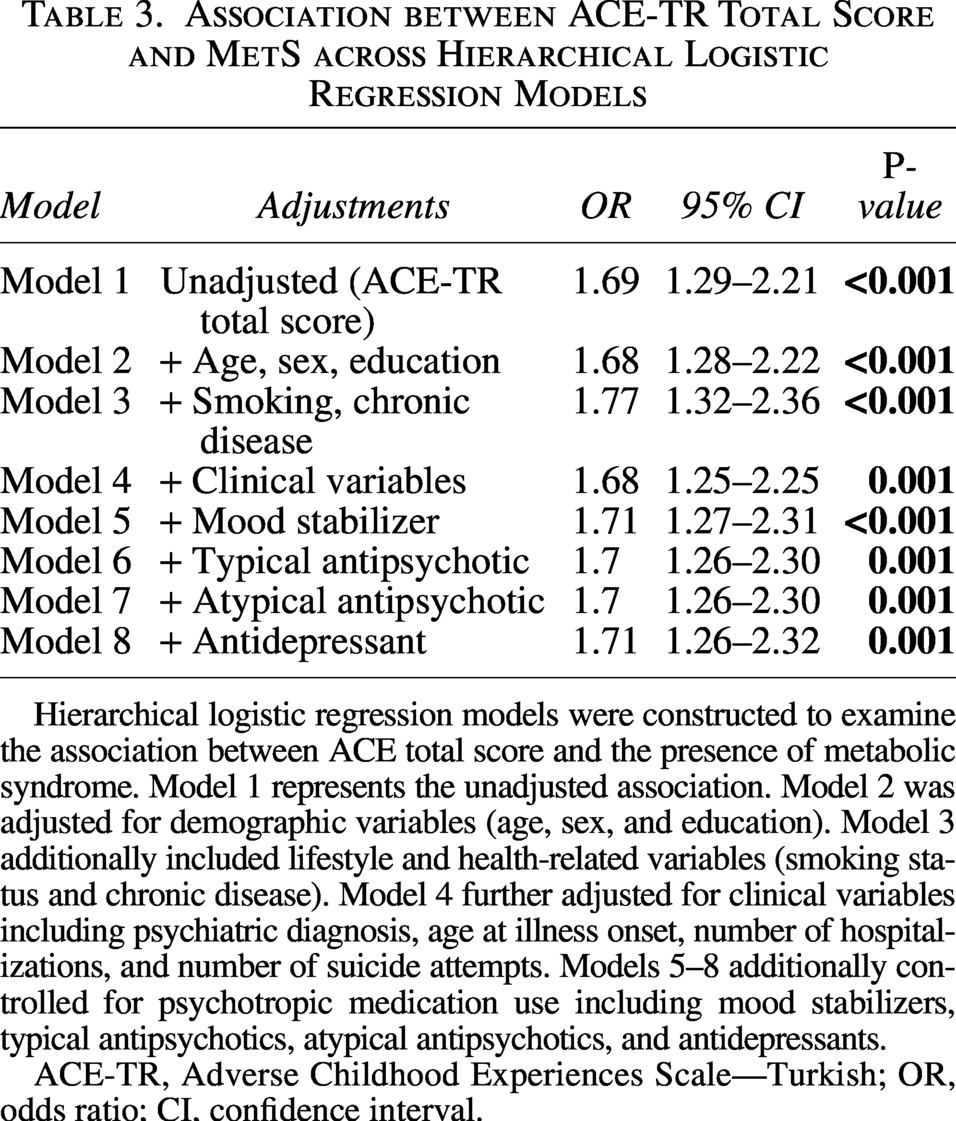
Hierarchical logistic regression models were constructed to examine the association between ACE total score and the presence of metabolic syndrome. Model 1 represents the unadjusted association. Model 2 was adjusted for demographic variables (age, sex, and education). Model 3 additionally included lifestyle and health-related variables (smoking status and chronic disease). Model 4 further adjusted for clinical variables including psychiatric diagnosis, age at illness onset, number of hospitalizations, and number of suicide attempts. Models 5–8 additionally controlled for psychotropic medication use including mood stabilizers, typical antipsychotics, atypical antipsychotics, and antidepressants.
ACE-TR, Adverse Childhood Experiences Scale—Turkish; OR, odds ratio; CI, confidence interval.
ACE and MetS: Hierarchical and multivariable logistic regression analyses
Hierarchical logistic regression analyses were performed to examine the stability of the ACE–MetS association across sequential adjustment for potential confounding variables. As shown in Table 3, higher ACE-TR total score was significantly associated with increased odds of MetS in the unadjusted model (OR = 1.69, 95% CI: 1.29–2.21; P < 0.001). This association remained statistically significant after adjustment for demographic variables including age, sex, and education (Model 2: OR = 1.68, 95% CI: 1.28–2.22, P < 0.001), as well as smoking status and chronic disease (Model 3: OR = 1.77, 95% CI: 1.32–2.36, P < 0.001). Further adjustment for clinical variables including psychiatric diagnosis, age at illness onset, number of hospitalizations, and number of suicide attempts, the association remained robust (Model 4: OR = 1.68, 95% CI: 1.25–2.25, P = 0.001). The association remained significant after additional adjustment for psychotropic medication use, including mood stabilizers, typical antipsychotics, atypical antipsychotics, and antidepressants (Models 5–8). Across all models, ACE-TR total score showed a consistent association with MetS, with odds ratios ranging between 1.68 and 1.77. Full model coefficients and model fit indices are provided in Supplementary Tables S2 and S3.
Table 4 presents the final multivariable logistic regression model including all covariates. In the fully adjusted model, ACE-TR total score was independently associated with MetS (OR = 1.71; 95% CI: 1.26–2.32; P = 0.001), indicating that each one-unit increase in ACE-TR total score was associated with approximately 71% higher odds of MetS. The number of hospitalizations was also significantly associated with MetS (OR = 1.19; 95% CI: 1.02–1.39; P = 0.028). Other variables, including age, sex, education level, smoking status, chronic disease, psychiatric diagnosis, age at illness onset, suicide attempts, and psychotropic medication use, were not significantly associated with MetS in the fully adjusted model (P > 0.05).
Multivariate Logistic Regression Analysis for Factors Associated with MetS
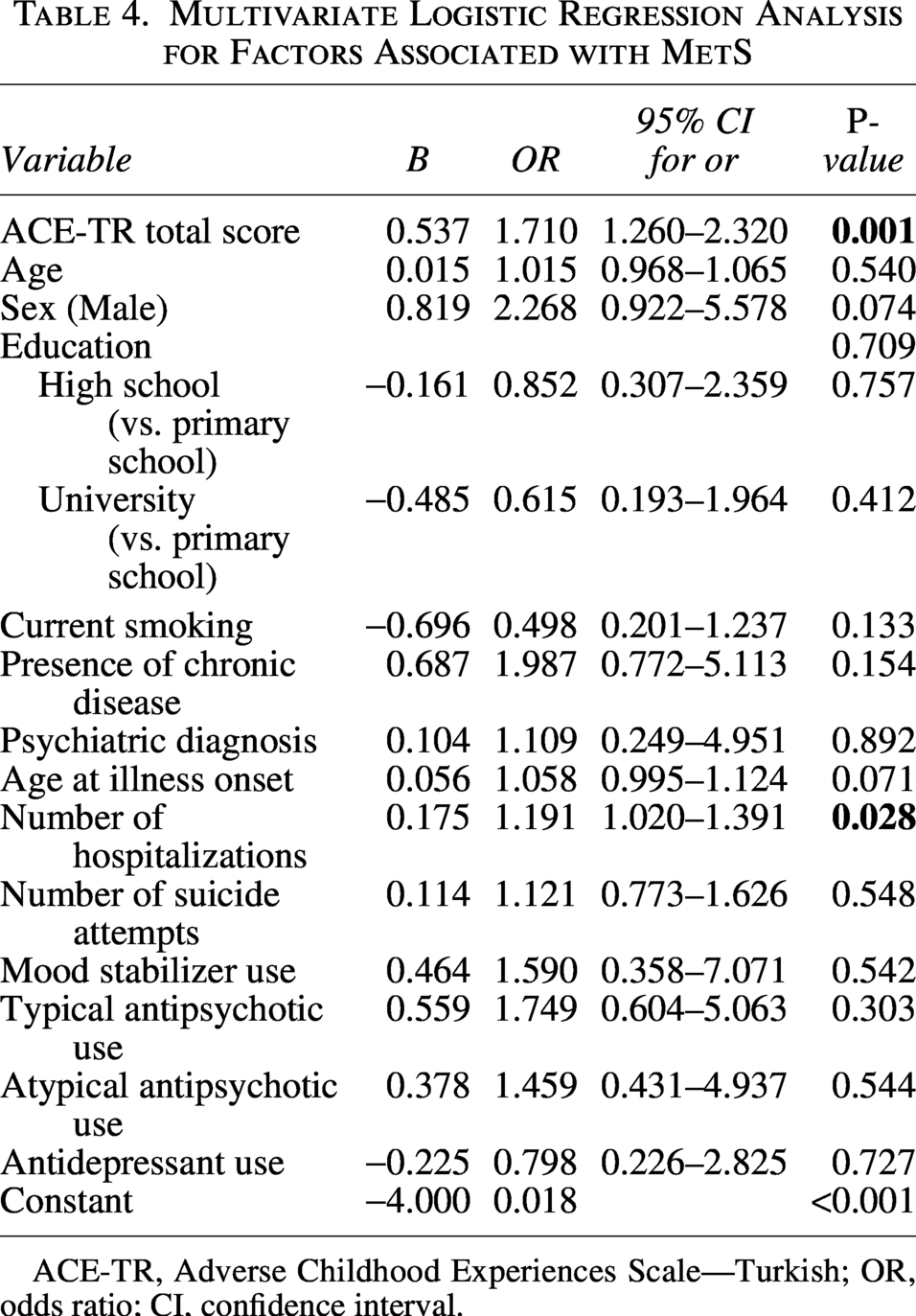
ACE-TR, Adverse Childhood Experiences Scale—Turkish; OR, odds ratio; CI, confidence interval.
Distribution of ACE subtypes according to MetS status
Among the ACE subtypes examined, sexual abuse, emotional neglect, and physical neglect differed significantly between participants with and without MetS. Specifically, sexual abuse was more frequent in the MetS group than in the non-MetS group (16.9% vs. 2.7%, P = 0.004). Similarly, emotional neglect was markedly more common among participants with MetS (63.1% vs. 30.7%, P < 0.001), as was physical neglect (30.8% vs. 14.7%, P = 0.022). In contrast, no statistically significant group differences were observed for emotional abuse, physical abuse, parental separation or divorce, household domestic violence, household substance abuse, household mental illness, or incarceration of a household member (all P > 0.05). The distribution of ACE subtypes according to MetS status is presented in Table 5.
Distribution of ACEs Subtypes according to MetS
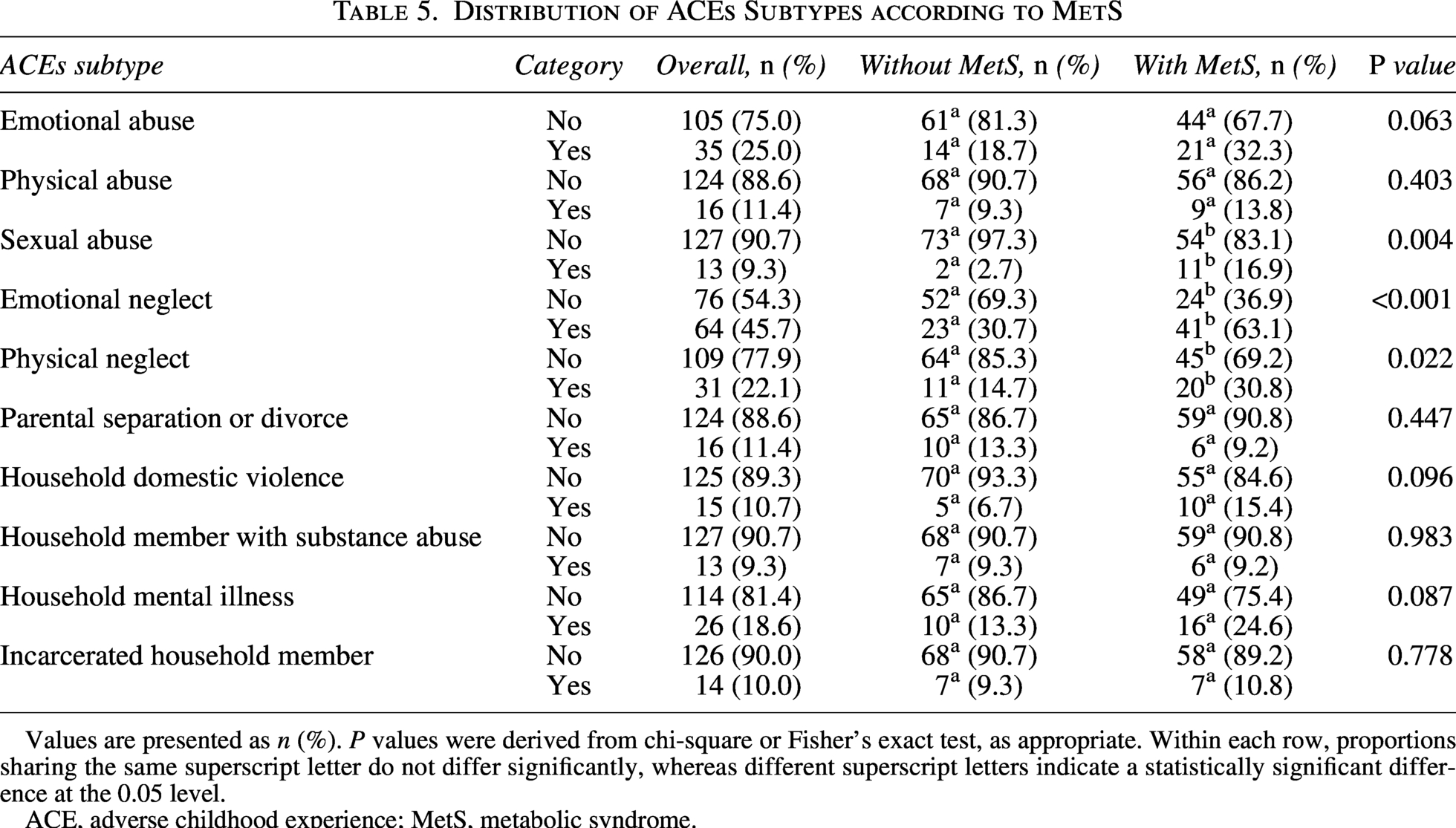
Values are presented as n (%). P values were derived from chi-square or Fisher’s exact test, as appropriate. Within each row, proportions sharing the same superscript letter do not differ significantly, whereas different superscript letters indicate a statistically significant difference at the 0.05 level.
ACE, adverse childhood experience; MetS, metabolic syndrome.
DISCUSSION
The central finding of this study is that advs are independently associated with MetS in patients with SZ and BD, and this association held firm across eight successive models, surviving sequential adjustment for demographic factors, smoking, chronic disease, clinical severity, and every psychotropic medication class examined. For each additional adverse childhood experience reported, the odds of having MetS increased by approximately 71%. This is not a fragile statistical association that fades with adjustment; it appears to reflect a genuine and clinically meaningful relationship between early life adversity and adult cardiometabolic health.
The prevalence of MetS in our sample was 46.4%, consistent with prior meta-analytic estimates for individuals with SMD.6,7 Notably, the association between ACEs and MetS was stronger in our sample (OR = 1.71) than the pooled estimate reported in general population studies (OR = 1.24) 21 . This difference may reflect a synergistic interaction between early life adversity and the biological and psychosocial burden inherent to SMD: the neurobiological dysregulation, cumulative medication exposure, and lifestyle constraints associated with SZ and BD may create a milieu that amplifies the metabolic sequelae of childhood stress.
The pattern of metabolic correlations offers an important nuance. ACE-TR total score was associated with waist circumference and TG levels, but not with HDL-cholesterol, blood pressure, or fasting glucose. This is not a pattern of indiscriminate metabolic disruption; it suggests that childhood adversity preferentially affects abdominal fat distribution and lipid metabolism. Visceral adipose tissue is particularly sensitive to chronic cortisol exposure, and sustained activation of the HPA axis following early life stress may direct fat storage preferentially to the abdomen. TG levels, in turn, are closely linked to cortisol and insulin sensitivity. Blood pressure and glucose are shaped by a broader array of influences aging, genetics, pharmacology that may dilute the detectable signature of early adversity in a cross-sectional study. Longitudinal studies support this interpretation: abdominal changes tend to emerge early and persist, while blood pressure effects accumulate gradually over years, a timing difference that may partly account for the selective pattern observed in our sample. 22
Among the ACE subtypes, sexual abuse, emotional neglect, and physical neglect were significantly more common in patients with MetS. What these three experiences share is not acute severity but chronicity; they tend to unfold gradually, often without being named or witnessed, and their biological effects may accumulate precisely because they go unacknowledged. Sexual abuse in particular carries a heavy burden of stigma and silence in the Turkish cultural context,23,24 while emotional and physical neglect may be frequently normalized within family structures and go unrecognized even by those who experienced them. The subtypes that did not differentiate between groups—emotional and physical abuse, domestic violence, and household dysfunction—may reflect limited statistical power in smaller subcategories, but may also differ in a more fundamental way: their metabolic consequences may operate through indirect pathways, such as depression, anxiety, or substance use rather than through direct stress biology, and since these mediating mechanisms were not assessed, any such effects would not have been captured in our models.23–26
Although prior studies have linked ACEs to earlier illness onset,27–29 increased suicide risk, 26 and tobacco use in SZ and BD,30–32 our findings only partially replicate this pattern. The significant correlations between ACE-TR score and both smoking quantity and duration are consistent with the well-established relationship between childhood adversity and nicotine dependence,30–32 however, the absence of an independent association between smoking status and MetS in the fully adjusted model likely reflects the measurement constraints of a binary coding approach and the limited variance in this variable within our sample. That the ACE–MetS association retained both its significance and effect size after controlling for smoking suggests that the metabolic consequences of early adversity are not simply mediated through behavioral pathways independent biological mechanisms appear to be involved as well. The absence of significant associations with suicide attempt history and age at illness onset may reflect limited variance across both variables and the resulting insufficient statistical power rather than true null effects; these questions warrant examination in larger samples.
In the fully adjusted model, number of hospitalizations emerged as independently associated with MetS, alongside ACE-TR total score. More frequent hospitalizations signal a more severe and unstable illness trajectory, bringing with it accumulated psychosocial stress, disrupted routines, loss of agency, and greater difficulty maintaining the conditions necessary for physical health. That ACEs are themselves a risk factor for psychiatric re-hospitalization raises the possibility that early adversity exerts its metabolic effect not only directly but also indirectly through the worsening of illness course. 33 The correlation between ACE-TR score and hospitalization count in our data supports this interpretation.
Psychotropic medications, psychiatric diagnosis, age, sex, and education level were not independently associated with MetS in the fully adjusted model. This should not be read as evidence that these factors are metabolically irrelevant. Atypical antipsychotics are well-known contributors to weight gain and dyslipidemia, and the fact that 80.7% of our sample used them leaves little variance for the model to detect. The borderline association for female sex (OR = 2.27, P = 0.074) may reflect a real but underpowered signal, and the similar metabolic burden across diagnostic groups likely explains the non-significance of psychiatric diagnosis. What is worth emphasizing is that across all eight hierarchical models, the odds ratio for ACE-TR total score remained stable between 1.68 and 1.71 a consistency that speaks to the robustness of this relationship regardless of what else is held constant.
Finally, the mean ACE-TR score in our sample (1.74 ± 1.44) was relatively low compared with global estimates. 34 This likely reflects the high reporting thresholds in Eastern Türkiye for sensitive experiences such as sexual abuse and household dysfunction, shaped by cultural norms around family privacy and gender roles.23–25 From this perspective, the strong association we detected despite conservative reporting is striking: it suggests that the true exposure burden may be higher than captured and that our effect estimate is, if anything, conservative.
Limitations and strengths
This study has several limitations. The cross-sectional design precludes causal inference; however, since ACEs by definition precede the onset of psychiatric illness and MetS, temporal precedence can reasonably be assumed. The reliance on self-reported data introduces the risk of recall bias. Although several ACE subtypes were associated with MetS, simultaneous exposure to multiple categories was not disentangled; effects attributed to specific subtypes may partly reflect cumulative trauma burden, and individual effect sizes should be interpreted accordingly. The ACE-TR instrument assesses cumulative exposure before age 18 as a single time frame and does not include developmental intervals; consequently, the differential effects of adversity timing on metabolic outcomes could not be examined. Psychotropic medications were coded by broad class rather than by individual agent, which may have limited the detection of agent-specific metabolic effects. Several potentially important variables—including sleep disturbances, alcohol and substance use other than tobacco, family history of metabolic disease, dietary intake, and physical activity—were not assessed. Additionally, biological mediators that may underlie the ACE–MetS association, such as cortisol and inflammatory markers, were not measured. Although restricting inclusion to patients in remission reduces the potential confounding effects of acute psychopathology on metabolic parameters, it may limit the generalizability of findings to patients with more severe or treatment-refractory illness. Finally, given that the experience and disclosure of trauma vary across cultural and socioeconomic contexts, generalization of our findings to other populations warrants caution.
Despite these limitations, the study has several methodological strengths. To the best of our knowledge, this is the first study to systematically examine the ACE–MetS relationship in a non-Western clinical sample of patients with SMD using standard NCEP-ATP III diagnostic criteria. The use of a validated Turkish-language instrument (ACE-TR), objective biochemical and anthropometric measurements, and a hierarchical modeling strategy with sequential adjustment for 16 covariates across eight models strengthen the reliability of the findings. Data from Eastern Türkiye contribute meaningful geographic and cultural diversity to a literature predominantly based on Western cohorts.
Conclusion
In conclusion, this study demonstrates that ACEs are independently associated with MetS in patients with SZ and BDr, an association that persists after comprehensive adjustment for sociodemographic, behavioral, clinical, and pharmacological factors. Sexual abuse, emotional neglect, and physical neglect emerged as the ACE subtypes most closely linked to MetS status. These findings support the integration of trauma history screening into routine cardiometabolic assessment of patients with SMD and highlight the need for targeted preventive strategies in those with high ACE burden. Future research should employ prospective longitudinal designs, incorporate biological mediators, and evaluate whether trauma-informed interventions can improve metabolic outcomes in this population.
Authors’ Contributions
N.C.: Investigation, writing, original draft, writing—review and editing. M.Ç.Ö.: Resources, conceptualization, data collection, and drafting. Ş.İ.N.M.: Resources, editing, and review. Ş.Y.: Analysis and editing. All authors contributed to the writing and approved the final version of the article.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to all patients who voluntarily participated in this study.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.