
Abstract
Purpose:
Cancer-related fatigue (CRF) is the most common symptom of cancer patients. This study aimed to investigate the prevalence of CRF among patients with breast cancer-related lymphedema (BCRL) and to indentify the factors associated with its occurrence.
Methods:
In this cross-sectional study, women with BCRL (N = 260) were recruited from the three general hospitals. Lymphedema status was determined using the Norman telephone questionnaire as the patient-reported occurrence of hand/lower arm/upper arm swelling. CRF status was assessed using the Functional Assessment of Chronic Illness Therapy-Fatigue questionnaire. Multiple binary logistic regression analysis was used to identify factors associated with CRF.
Results:
The median time from BC diagnosis was 29 months (interquartile range, 15.0–62.0 months). The prevalence of CRF among BCRL patients was 88.46%. The median sedentary time was 245 min/day (IQR: 150–330min/day), and 34.23% of the patients did not meet the moderate-intensity physical activity level. Abnormal postoperative wound healing status, radiotherapy, hormonal therapy, lymphedema severity and failure to meet moderate-intensity physical activity level were associated with an increased risk of CRF.
Conclusion:
CRF is highly prevalent among patients with BCRL. Targeted interventions aimed at promoting moderate-intensity physical activity and improving long-term symptom management may help alleviate fatigue.
Introduction
Breast cancer-related lymphedema (BCRL) remains a common complication of breast cancer treatment, affecting at least 20% of survivors within 7 years of follow-up. 1 Characterized by the accumulation of protein-rich fluid in the interstitial tissues and regional swelling, BCRL can result in substantial upper-limb dysfunction, including reduced range of motion, weakness, paresthesia, and impaired quality of life. 2 Regular physical activity is recommended for breast cancer survivors because it can improve physical function, alleviate fatigue, and enhance overall well-being. 3 Nevertheless, cancer-related fatigue remains highly prevalent among cancer survivors and continues to adversely affect daily functioning and quality of life. 4,5 Cancer-related fatigue (CRF) differs from ordinary fatigue in that it resists rest and significantly exacerbates its impact on the quality of life and daily functioning of BCRL patients. 4,6
The underlying causes of CRF are multifaceted, encompassing biological, psychological, and environmental factors. 7 The social ecology theory elucidates the intricate relationship between individual health behaviors and health outcomes, highlighting the influence of individual characteristics, behavioral patterns, disease-related variables, and environmental conditions on CRF. 8,9 Among the disease-related factors, chemotherapy and radiotherapy are associated with a higher prevalence of fatigue compared to surgery, possibly due to cumulative side effects. 5,10 In terms of individual factors, CRF was consistently greater in older individuals 7,11 and obese patients due to a higher number of comorbidities, 11 while psychosocial variables like self-efficacy may mediate the impact of sedentary behavior and CRF. 12 Lower education level patients have previously been associated with higher levels of fatigue, as well as with more health problems and poorer access to health care services in different samples. 12 Previous studies have shown that cancer-related fatigue is associated with impaired work functioning and changes in employment status. Fatigue may reduce an individual's ability to maintain work performance and participate fully in occupational activities, thereby affecting employment outcomes. 13
Despite established evidence supporting physical activity regimens (including low-to-high intensity protocols) for CRF mitigation, 14 –16 critical knowledge gaps persist regarding the relationship between CRF and the tolerable level of physical activity in BCRL patients. 4,17 Current guidelines lack objective metrics for synchronizing fatigue states with physical activity parameters (e.g., intensity, limb volume changes), potentially contributing to suboptimal adherence through misaligned patient self-assessment. 4 Several factors contribute to the misalignment. Firstly, some patients may associate a reduction in fatigue with adverse effects such as exercise-induced edema, 17 potentially leading to premature cessation of physical activity. Secondly, some patients may avoid exercise because they dislike sweating, viewing it as an unpleasant symptom rather than a normal physiological response to physical activity. 18 Moreover, cancer survivors may experience a self-perpetuating cycle in which prolonged sedentary behavior and insufficient physical activity contribute to greater fatigue, while elevated fatigue further limits engagement in regular physical activity, thereby hindering symptom improvement. 19,20
Existing research shows that CRF in BCRL patients is influenced by both individual characteristics and broader social-ecological factors, including lifestyle, social relationships, and health care policies. 21 This study employs multivariable binary logistic regression analysis to systematically examine the contributions of demographic, clinical, and behavioral factors to CRF in patients with BCRL. To enhance clinical applicability, identified factors were further categorized as modifiable or non-modifiable, thereby highlighting actionable intervention targets and informing tailored management strategies for CRF.
Methods
Design and participants
This cross-sectional study recruited patients with BCRL from three general hospitals in Henan, China, between August 2023 and October 2024. Inclusion criteria were: (i) age ≥18 years; (ii) diagnosed with unilateral breast cancer; (iii) completed breast cancer surgery at least 6 months earlier and subsequently developed arm lymphedema; (iv) proficiency in the Chinese language. Exclusion criteria were: (i) previous contralateral or synchronous bilateral breast cancer; (ii) other comorbidities that might also induce edema (e.g., renal disease, congestive heart failure); (iii) a history of major trauma, surgery, or infection in the upper limbs or neck unrelated to breast cancer treatment; and (iv) inability to complete the study questionnaire.
Data collection
Data were collected using a combination of paper-based and web-based surveys, allowing participants to choose their preferred format. The web-based survey adhered to guidelines for improving the quality of web surveys 22 and underwent usability and technical function testing by the authors. Feedback from 15 patients in a pilot study was incorporated into the final version of the survey.
Recruitment advertisements were posted on websites dedicated to breast cancer research by oncology nurses from the participating hospitals. No incentives were offered for participation. Eligible patients were identified and invited to participate during routine follow-up visits. The purpose, procedures, and duration of the study were explained both verbally and in writing, and patients were given the opportunity to ask questions and consider their participation. Informed consent was obtained from all participants prior to data collection, and confidentiality of their data was assured.
Participants were provided with either a paper questionnaire or the URL for the online questionnaire. Contact information for the first author was provided for any questions regarding the survey. For illiterate participants, the first author read the questions aloud and recorded their responses. The completeness of returned questionnaires was checked by the other authors. To minimize duplicate submissions, IP addresses and response records were reviewed. 23
Analyzed variables
Socio-demographic and clinical variables
Sociodemographic variables included age, marital status, occupation, education level, and monthly average household income. Additional general information included Body Mass Index (BMI) and lifestyle factors such as physical activity level. Clinical variables encompassed disease duration, Tumor-Node-Metastasis (TNM) stage, surgery type, and use of chemotherapy, radiotherapy, or hormonal therapy. Postoperative wound healing conditions include normal healing and abnormal healing, with the latter encompassing delayed healing, infection, seroma, etc.
Physical activity-related variables
The International Physical Activity Questionnaire-short form was used to assess physical activity during the previous 7 days. 24 Walking, moderate-intensity activity, vigorous-intensity activity, and total physical activity scores (MET-min/week) were calculated according to the IPAQ scoring protocol by multiplying activity duration, frequency, and corresponding MET values. Participants were subsequently categorized according to whether they met the recommended level of moderate-intensity physical activity. 24
Evaluation of cancer-related fatigue
The Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) scale was used to assess CRF. 25 This scale consists of 13 items rated on a 0-4 scale, with total scores ranging from 0 to 52. Higher scores indicate lighter fatigue levels, and a score of 43 or lower is defined as the cutoff for CRF 26 . The Chinese version of the FACIT-F has demonstrated good internal consistency (Cronbach’s alpha = 0.929) and test-retest reliability (r = 0.965). 27
Evaluation of breast cancer-related lymphedema
Lymphedema was assessed using the Norman telephone questionnaire or self-reported doctor diagnosis. 28 The Norman questionnaire, which has been translated into Chinese and validated, consists of questions about swelling in the affected arm compared to the non-affected arm. 29 Patients were classified as having mild, moderate, or severe lymphedema for total scores of 1-3,4-6,7-9,respectively. Additionally, patients who self-reported a doctor or physical therapist’s diagnosis of BCRL were also considered to have lymphedema. 30
Ethical considerations
This study was approved by the Ethics Committee for Life Sciences of Zhengzhou University(approval number: ZZUIRB2023281).
Statistical analysis
Statistical analyses were conducted using SPSS 26.0 software. Categorical variables were expressed as frequencies and percentages, while continuous variables were presented as mean ± standard deviation or median (interquartile range [IQR]), as appropriate. Chi-square tests were used for univariate analysis. Variables demonstrating p < 0.05 in univariate analyses were entered into a multivariable binary logistic regression model to identify factors associated with CRF among patients with BCRL. Statistical significance was set at p < 0.05.
Results
Participant characteristics and prevalence of CRF
This study initially enrolled 313 BCRL patients, with 53 excluded based on predefined criteria, resulting in 260 valid responses. The participants had a mean age of 59.30 ± 9.02 years, a median disease duration of 29 months (Interquartile Range[IQR]: 15–62 months), and a mean BMI of 22.51 ± 3.32 kg/m2. Physical activity assessment revealed a median sedentary time of 245 min/day (IQR: 150–330 min/day), and 34.23% (n = 89) failing to meet moderate-intensity physical activity recommendations. Lymphedema severity distribution showed 35.38% (n = 92) with mild and 64.62% (n = 168) with moderate-to-severe cases. Notably, 88.46% (n = 230) of participants reported CRF. Detailed sociodemographic and clinical characteristics are presented in Table 1.
Univariate Analysis of the Relationship Between the Socio-Ecological Variables and CRF in BCRL Patient
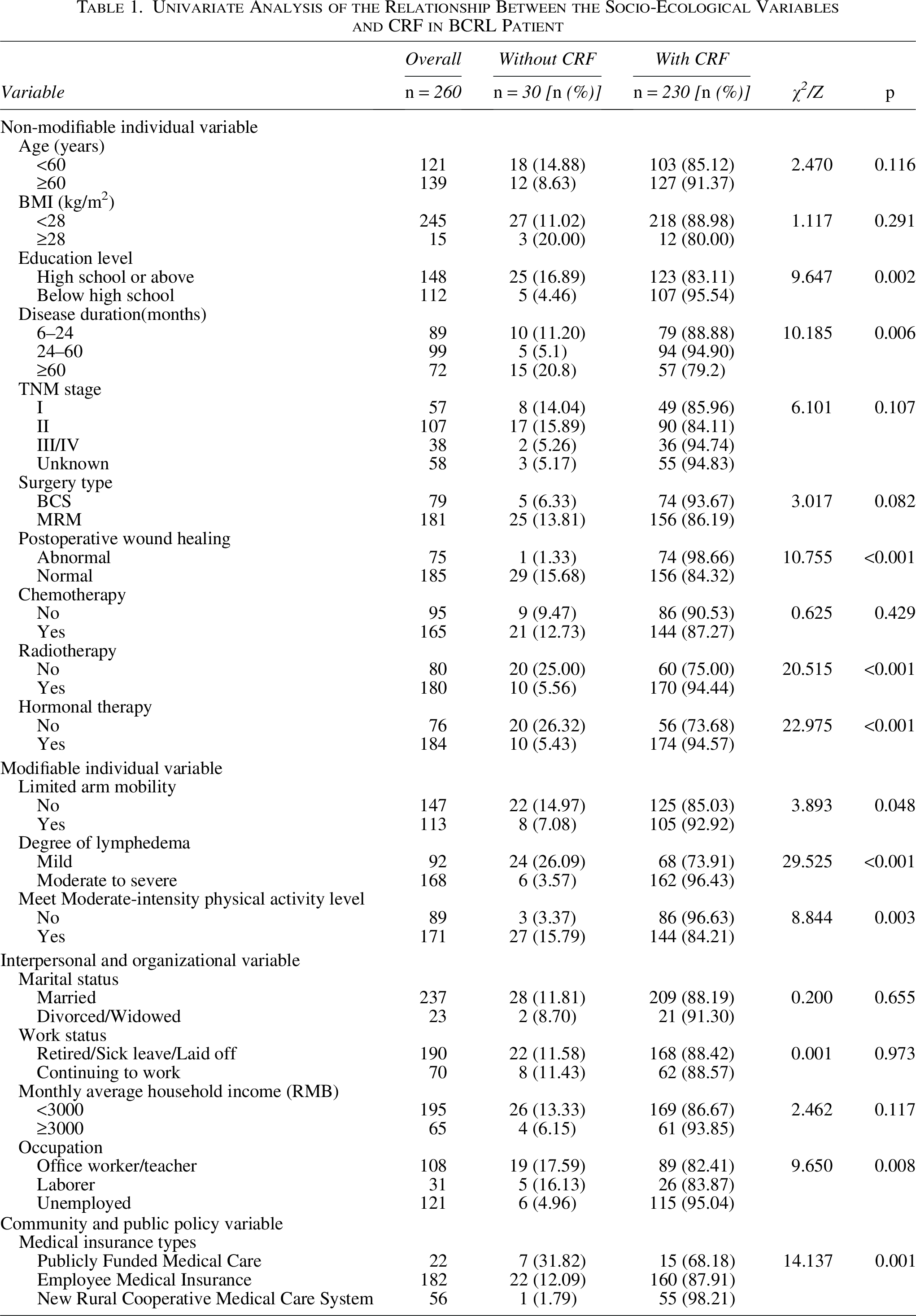
Univariate analysis of factors associated with CRF
Univariate analysis revealed that CRF was significantly more prevalent among BCRL patients who were unemployed, had the new rural cooperative medical system as their medical insurance type, or had education levels below high school. Additionally, CRF was more common in patients with a disease duration of less than 60 months, abnormal postoperative wound healing, prior radiotherapy or hormonal therapy, moderate-to-severe lymphedema, limited arm mobility, failure to meet moderate-intensity physical activity recommendations (Table 1).
Factors associated with CRF in BCRL patients
Multiple binary logistic regression analysis was conducted to indentify factors associated with CRF among patients with BCRL(Table 2). CRF occurrence was entered as the dependent variable.
Binary Logistic Analysis of Influencing Factors of CRF in BCRL Patients
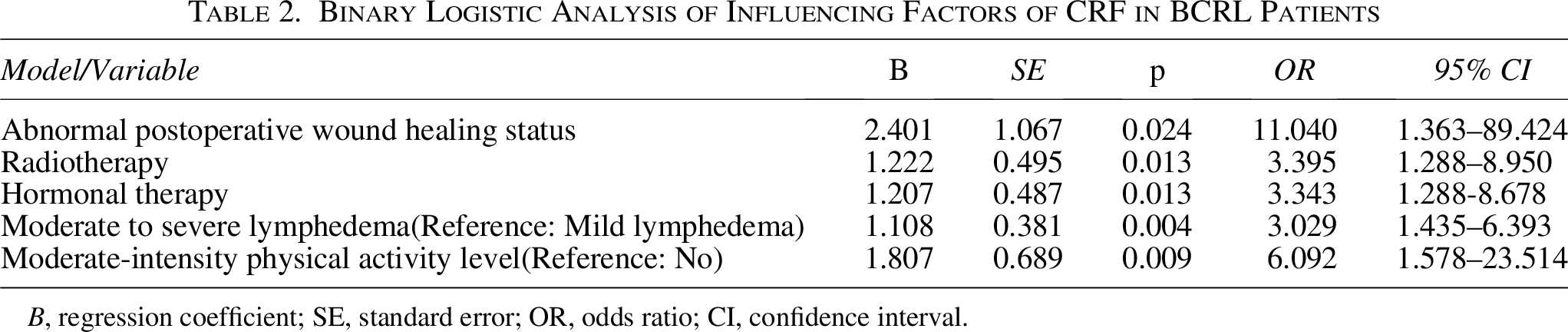
B, regression coefficient; SE, standard error; OR, odds ratio; CI, confidence interval.
The results showed that abnormal postoperative wound healing status (OR = 11.040, 95% CI: 1.363–89.424), radiotherapy (OR = 3.395, 95% CI: 1.288–8.950), hormonal therapy (OR = 3.343, 95% CI: 1.288–8.678), Moderate to severe lymphedema (OR = 3.029, 95% CI:1.435–6.393) and Moderate-intensity physical activity level (OR = 6.092, 95% CI: 1.578–23.514) were indenpendently associated with a high likelihood of CRF (Table 2).
Discussion
This study provides a comprehensive assessment of CRF among patients with BCRL and highlights the complex interplay of clinical, lymphedema-related, and behavioral factors associated with fatigue. 31 Multiple binary logistic regression analysis identified several significant predictors of CRF, including abnormal wound healing status, radiotherapy, and hormonal therapy moderate-to-severe lymphedema severity and insufficient moderate-intensity physical activity. These findings provide valuable insights into the multifactorial nature of CRF in BCRL patients and suggest that comprehensive interventions addressing the modifiable factors may help reduce fatigue burden and improve quality of life in this vulnerable population. 32,33
Prevalence of Cancer-related fatigue in BCRL patients
The observed 88.46% CRF prevalence substantially exceeds rates documented in broader breast cancer survivor cohorts, 34 likely reflecting the additive burden of BCRL and multifaceted interactions between physiological, psychological, and therapeutic factors. Notably, 64.61% of patients exhibited moderate-to-severe lymphedema, a condition frequently causing persistent functional limitations that impede resumption of premorbid activity levels. These restrictions not only impair physical function but may also trigger social disengagement and reduced daily activity, all recognized contributors to CRF pathogenesis. 35 A concerning 65.77% of participants had sustained their condition for over 2 year, with 88.30% of this chronic subgroup reporting CRF. These findings underscore the chronic and enduring nature of fatigue in BCRL survivors and support the importance of integrating fatigue screening and management into long-term survivorship care. 36 Furthermore, patients often lack comprehensive CRF literacy, hindering symptom recognition and appropriate help-seeking. 36 These findings collectively underscore the imperative for targeted educational initiatives to enhance CRF understanding among both clinicians and patients, thereby optimizing therapeutic outcomes and quality of life.
Predictors of Cancer-related fatigue in BCRL patients
Individual-related factors
The binary logistic regression model incorporated both modifiable and non-modifiable individual-level factors, including education level, disease duration, postoperative wound healing status, radiotherapy, hormonal therapy, limited arm mobility,degree of lymphedema and physical activity status. Three clinical factors emerged as significant positive predictors of CRF: abnormal postoperative wound healing status, history of radiotherapy, and hormonal therapy. These findings are consistent with previous studies showing that treatment-related factors contribute substantially to CRF among cancer survivors. 5 Radiotherapy-induced tissue damage promotes pro-inflammatory cytokine release, which amplifies fatigue and other treatment-related symptoms. Similarly, hormonal therapy, including the use of aromatase inhibitors or tamoxifen, can affect the endocrine system, disrupt hormonal homeostasis, potentially inducing fatigue through multiple pathways including vasomotor symptoms, arthralgia, and mood disorders. 7,37
The abnormal postoperative wound healing status was significantly associated with an increased risk of CRF, possibly because complications such as infection or seroma may prolong local inflammatory responses and delay postoperative recovery, thereby increasing fatigue burden. 38 These findings suggest that timely management of wound complications may play an important role in reducing fatigue and promoting functional recovery among patients with BCRL. 6
Physical activity level and lymphedema-related factors.
Among the included variables, lymphedema severity and moderate physical activity were identified as critical determinants of CRF, with psychological distress stemming from physical impairments in BCRL patients potentially amplifying fatigue. 39 Moderate physical activity emerged as a key predictor, as patients attaining this activity level exhibited significantly reduced fatigue compared to inactive counterparts, aligning with prior evidence linking physical inactivity to heightened fatigue. 40 Reduced physical activity may diminish skeletal muscle pump activity, impair lymphatic drainage, and potentially exacerbate lymphedema. 41 Given the close association between symptom burden and fatigue, worsening lymphedema may further contribute to CRF in patients with BCRL. 16 Consequently, a dual intervention strategy emphasizing the promotion of moderate-intensity physical activity is warranted to enhance lymphatic drainage in affected limbs and mitigate CRF symptoms, as supported by existing evidence on the synergistic benefits of these approaches. 18
Socioeconomic-related factors
It is noteworthy that medical insurance type was identified as a potential factor associated with CRF in the univariate analysis. This could be attributed to the fact that low-income individuals or those who are unemployed are more prone to adopting a sedentary lifestyle due to a lack of resources or opportunities for engaging in restorative activities. 42 Furthermore, the type of medical insurance may influence patients’ access to medical resources and their financial burden, thereby affecting health outcomes and symptom management. 43 These findings underscore the importance of considering socioeconomic factors and health care accessibility in CRF management, as both can significantly impact patients’ recovery and their ability to maintain a higher quality of life. Addressing these disparities could lead to more effective interventions and improved outcomes for underserved populations.
Limitations
The limitations of this study are manifested in the following aspects. First, due to the cross-sectional design, causal relationships between variables cannot be established. Second, constrained by the cultural contexts specific to China, the generalizability of findings to diverse recovery stages and patient populations is limited. Third, the exclusion criteria omitting patients with cancer recurrence or severe complications may have skewed the sample toward individuals with better recovery outcomes, potentially compromising the universality of coping flexibility evaluations.
Conclusion
Cancer-related fatigue is highly prevalent among patients with BCRL, with a substantially higher burden than that reported in the broader population of breast cancer survivors. CRF was associated with abnormal postoperative wound healing, radiotherapy, hormonal therapy, moderate-to-severe lymphedema, and insufficient moderate-intensity physical activity. These findings highlight the importance of comprehensive fatigue assessment and targeted management strategies aimed at optimizing treatment-related recovery, promoting appropriate physical activity, and improving long-term survivorship care for patients with BCRL.
Authors’ Contributions
Y.L.: Conceptualization, formal analysis, methodology, validation, resources, writing—original draft, visualization, project administration, and funding acquisition. L.W.: Formal analysis, methodology, validation, software, writing—review and editing, and visualization. X.Z.: Visualization and writing—review and editing. Z.L.: Visualization and writing—review and editing. X.R.: Writing—review and editing. H.S.: Writing—review and editing. W.Z.: Validation, supervision, resources, writing—review and editing, and supervision. F.L.: Methodology, investigation, resources, writing—review and editing, data curation, funding acquisition.
Footnotes
Acknowledgments
The authors express gratitude to all the reviewers for their valuable contributions and support.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Author Disclosure Statement
The authors affirm that no competing financial interests or personal affiliations could be construed as influencing the research presented in this publication.
Funding Information
This work was supported by the Henan Provincial Natural Science Foundation[grant number 252300423873] and the Key Science and Technology Program of Henan Province [grant numbers 242102310236].