
Abstract
Liu, Zhen, Chao Nie, Lijia Yuan, Hui Jiang, Chuanchuan Liu, Yi Zhang, and Minghua Liu. Impact of acute high-altitude exposure on the timing of tranexamic acid administration in rabbits with traumatic hemorrhagic shock. High Alt Med Biol. 27:79–86, 2026.
Background:
Acute exposure to high altitude (≤3 days)-induced physiological changes may shorten the therapeutic time window for tranexamic acid (TXA) administration after traumatic hemorrhagic shock (THS). This study aims to compare the differences in the TXA therapeutic time window between THS patients with acute high-altitude exposure and those in low-altitude regions.
Methods:
Forty-two anesthetized rabbits were divided into three groups: low-altitude THS (l-THS), high-altitude sham, and high-altitude THS. All h-THS groups were housed for 3 days in 10% oxygen chambers (simulating 5,000 m altitude) before experimentation. THS models were established by reducing mean arterial pressure from 105 to 55 mmHg through blood loss combined with left tibiofibular fracture. Animals received single-dose TXA (90 mg/kg) with the following subgroups: l-THS-2h and l-THS-3h (TXA administered 2 hours/3 hours post-THS), h-THS-1h, h-THS-2h, h-THS-3h and h-THS-4h (TXA administered 1 hours/2 hours/3 hours/4 hours post-THS). Comparative analyses included hemodynamic parameters, complete blood counts, coagulation-fibrinolysis function, endothelial injury markers, inflammatory cytokines, and pulmonary histopathological changes.
Results:
High-altitude exposure required less blood loss to achieve THS compared with low-altitude conditions (51.00 ± 2.45 ml vs. 59.60 ± 3.65 ml, p < 0.05). At 6 hours post-THS, compared to the l-THS-2h group [TIC risk (INR:1.34 ± 0.09), anaerobic oxidation levels, inflammatory response levels, and lung injury score (1.8 (1.0, 2.0))], the l-THS-3h group [INR:1.51 ± 0.08; 2.6 (2.0, 3.0)], h-THS-2h group [1.45 ± 0.06; 2.8 (2.0, 3.5)], h-THS-3h group [INR:1.75 ± 0.11; 5.6 (4.5, 6.5)], and h-THS-4h group [INR:1.99 ± 0.06; 6.2 (6.0, 6.5)] all showed significantly higher values. For the same observational indicators, compared with the l-THS-3h group, the h-THS-1h group had lower values, while the h-THS-3h and h-THS-4h groups showed higher values. No statistically significant differences were observed between the l-THS-2h and h-THS-1h groups, or between the l-THS-3h and h-THS-2h groups for all parameters.
Conclusion:
The optimal time window for TXA administration in traumatic hemorrhagic shock may be shorter at high altitude compared with low-altitude area. These findings could influence therapeutic guidelines for TXA administration at high altitudes in humans.
Introduction
According to statistics, one-third of patients with traumatic hemorrhagic shock (THS) succumb to mortality, and trauma-induced coagulopathy (TIC), characterized by coagulofibrinolytic disorders, elevated blood lactate (Lac) levels, hypothermia, and subsequent progression to disseminated intravascular coagulation (Lindsay et al., 2024; Zanza et al., 2023), is a critical factor contributing to increased mortality. The Tibet region of China, with an average altitude of 4,000 m, hosted over 55 million domestic and international tourists in 2023, marking an 83.7% increase compared with the previous year (China SBoTARotPsRo, 2024). This surge in visitors may elevate the incidence of THS. Rapid exposure of lowland residents to high-altitude environments (>3,500 m) induces acute mountain sickness, including headaches, nausea, dizziness, and fatigue, alongside a hypercoagulable state and suppressed secondary fibrinolysis (Gatterer et al., 2024; Lijuan et al., 2007). Furthermore, traumatic hemorrhage at high altitude exacerbates coagulofibrinolytic imbalances more rapidly and severely than in lowland settings (Zhong et al., 2023).
Tranexamic acid (TXA), a competitive inhibitor of fibrin degradation, stabilizes existing clots (Grassin-Delyle et al., 2018). Clinical guidelines recommend intravenous administration of 1 g (15 mg/kg) TXA within 3 hours post-trauma to reduce bleeding, transfusion requirements, and early mortality (Gruen et al., 2023; Shakur et al., 2010). TXA also mitigates post-THS inflammation, preserves endothelial barrier integrity, and inhibits apoptosis (Grassin-Delyle et al., 2018). However, its efficacy is time-dependent: immediate administration improves survival by over 70%, with a 10% decline in survival benefit for every 15-minute delay, rendering it ineffective beyond 3 hours (Gayet-Ageron et al., 2018). Notably, the U.S. military’s Tactical Combat Casualty Care (TCCC) guidelines revised TXA administration to a 1-minute intravenous bolus of 2 g based on battlefield feedback (Drew et al., 2020). Currently, no studies have explored the therapeutic window of TXA for THS under acute high-altitude exposure. This study investigates the efficacy of prehospital TXA administration at different time points in rabbits with THS following acute high altitude exposure, providing theoretical insights for clinical management.
Materials and Methods
Reagents
TXA injection was purchased from Baiyunshan Pharmaceutical Co., Ltd. (Guangzhou, China, Lot: H20056986).Thromboelastography reagents were obtained from Dingrun Co., Ltd. (Chongqing, China, Lot: 20162400053). Blood gas analysis cartridges were sourced from Abbott Point of Care Inc. (USA, Lot: 03P85-25). Prothrombin time (PT), activated partial thromboplastin time (APTT), D-dimer, and plasma fibrinogen (FIB) assay kits were acquired from Rayto Life and Analytical Sciences Co., Ltd. (Shenzhen, China, Lot: A0423, A0425, A0422, and A0446, respectively). Syndecan-1, interleukin (IL)-6, tumor necrosis factor-α (TNF-α), and plasminogen activator inhibitor-1 (PAI-1) enzyme-linked immunosorbent assay (ELISA) kits were procured from commercial suppliers in the United States (Lots: EK20126, EK20517, EK6264, and EK8673, respectively).
Animal grouping, model establishment and sample collection
All animal procedures were approved by the Ethics Committee of the First Affiliated Hospital of Army Medical University and conducted in compliance with institutional guidelines (Ethics Approval Number: AMUWEC20232980).
Forty-two male New Zealand rabbits (weight 2.52 ± 0.09 kg; 8-month-old) were randomly allocated into three groups: low-altitude THS (l-THS, n = 12), acute high-altitude sham (h-sham, n = 6), and acute high-altitude THS (h-THS, n = 24). All experimental groups received a single 90 mg/kg TXA dose, with subgroup divisions based on intervention timing: l-THS group was subdivided into l-THS-2h and l-THS-3h subgroups (TXA was administered 2 hours/3 hours post-THS), while h-THS group comprised four subgroups (h-THS-1h, h-THS-2h, h-THS-3h, and h-THS-4h) that received TXA at 1 hour/2 hours/3 hours/4 hours post-THS, respectively. The l-THS group experiments were conducted at the Animal Laboratory of First Affiliated Hospital, Army Medical University (260 m elevation, 21% oxygen). The h-sham and h-THS groups underwent 3-day acclimatization in hypobaric chambers simulating 5,000 m altitude (10% oxygen concentration) prior to experimentation. All animals were housed under controlled temperature conditions (18–20°C) with ad libitum access to food and water.
Rabbits were anesthetized with 3% sodium pentobarbital (1 ml/kg). Catheters were inserted into the right carotid artery and femoral vein for blood sampling and hemorrhage induction, respectively. A 12-Fr Foley catheter was placed in the bladder for urine collection. After stabilization for 15 minutes, the left tibiofibular midshaft was fractured, and blood was withdrawn at 3 ml/kg·min until mean arterial pressure (MAP) reached 55 ± 5 mmHg (Moochhala et al., 2009; van Zyl et al., 2015). TXA (90 mg/kg) was administered via a 1-minute femoral vein bolus, adjusted for interspecies dosing (Rabbit:Human = 3:1), and aligned with TCCC protocols (Drew et al., 2020).
Vital signs were recorded, and 6 ml of blood was collected at baseline (T0) and 6 hours post-THS (T1). Euthanasia was performed via potassium chloride overdose at T1, followed by lung tissue extraction for histological analysis (fixed in 4% paraformaldehyde).
Blood sample analyses
Red blood cell (RBC) and platelet (PLT) counts were analyzed using a BC-5180 CRP hematology analyzer (Mindray, Shenzhen, China). pH and Lac levels were measured using a handheld i-STAT 300-G analyzer (Abbott Laboratories, USA). FIB, D-dimer, APTT, and PT were determined via an automated coagulometer (rac-030, Rayto Life Science, Shenzhen, China).
Enzyme-linked immunosorbent assay
Plasma levels of IL-6, TNF-α, syndecan-1, and PAI-1 were quantified using commercial kits (Signalway Antibody, USA). Briefly, took the IL-6, TNF-a, syndecan-1 and PAI-1 kits and prepared for backup. Set up the standard and sample wells, added 50 µl of different concentrations of standards into each standard well; subsequently, added 10 µl of the sample for analysis, followed by 40 µl of sample diluent to the sample wells. Then, dispensed 100 µl of the enzyme reagent into each well, ensured that the sample wells are pre-warmed and thoroughly rinsed. Each well was supplemented with 50 µl of chromogen A and chromogen B, mixed delicately, and the absorbance optical density (OD) value was quantified at 450 nm using an enzyme marker. Standard linear regression curves were plotted, and concentration values were calculated for each sample.
Measurement of lung water
The lungs were dissected free from the heart and great vessels, the trachea was separated at the carina, external liquid was removed by blotting, and the lungs were placed on a preweighed pan to obtain the wet weight. The lungs were then incubated in a dry atmosphere at 80°C for 72 hours and reweighed to obtain the dry lung weight. Total lung water (TLW) and wet/dry (W/D) ratios were calculated as: [TLW =
Hematoxylin and eosin stain
The lung tissue was extracted and placed in a 4% paraformaldehyde solution. Lung tissue sections were dehydrated using anhydrous ethanol and rendered transparent with xylene, immersed in hematoxylin solution for 15 minutes, rinsed in running water, stained in eosin solution for 5 minutes, rinsed again in running water, further dehydrated and made transparent, and finally sealed with neutral gum. The morphological alterations in the lung tissue of rabbits from each group were observed using a light microscope, and images were captured and blindly scored by two pathologists for alveolar capillary congestion, hemorrhage, inflammatory infiltration, and alveolar wall thickness.
Statistical analysis
Data were analyzed using SPSS 26.0 and GraphPad Prism 9.0. Normally distributed data are expressed as mean ± standard deviation and compared via ANOVA with LSD-t post hoc tests. Non-normal data are presented as M (Q1, Q3) and analyzed using Kruskal–Wallis with Dunn’s test. Two-tailed (p < 0.05) was considered statistically significant.
Results
Effects of TXA administration timing on hemodynamics, blood cell counts, and blood gas analysis in rabbits after acute exposure to high-altitude THS
Following traumatic hemorrhage, rabbits exhibited decreased MAP, heart rate (HR), and rapid reduction of RBC (Table 1). The h-THS group demonstrated significantly lower blood loss than the l-THS group when achieving the target MAP of 55 ± 5 mmHg (51.50 ± 2.27 ml vs. 59.20 ± 3.01 ml, p < 0.05; data not shown), confirmed successful model establishment.
Values of Hemodynamic and Physiological Parameters in Rabbits of Each Group
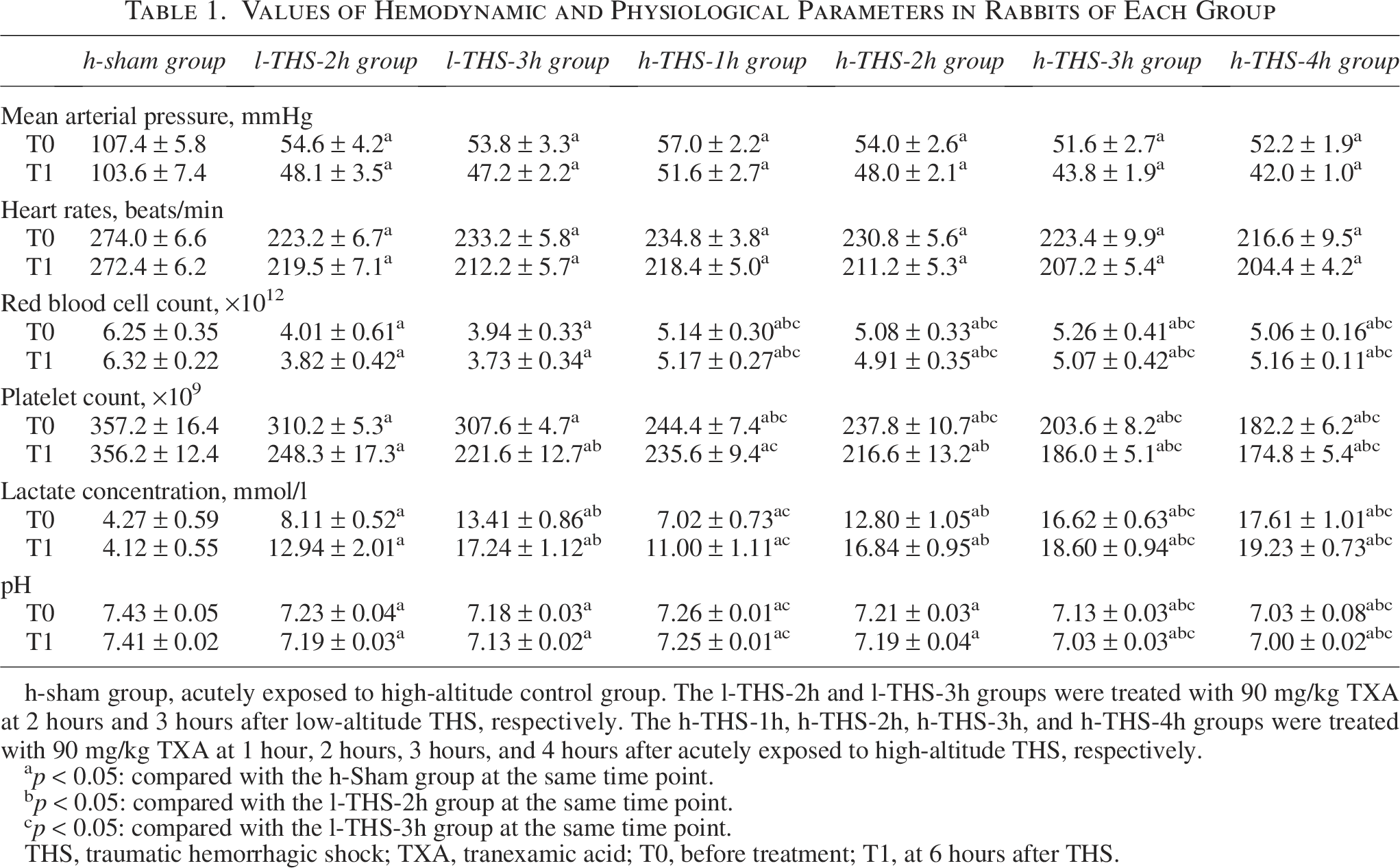
h-sham group, acutely exposed to high-altitude control group. The l-THS-2h and l-THS-3h groups were treated with 90 mg/kg TXA at 2 hours and 3 hours after low-altitude THS, respectively. The h-THS-1h, h-THS-2h, h-THS-3h, and h-THS-4h groups were treated with 90 mg/kg TXA at 1 hour, 2 hours, 3 hours, and 4 hours after acutely exposed to high-altitude THS, respectively.
p < 0.05: compared with the h-Sham group at the same time point.
p < 0.05: compared with the l-THS-2h group at the same time point.
p < 0.05: compared with the l-THS-3h group at the same time point.
THS, traumatic hemorrhagic shock; TXA, tranexamic acid; T0, before treatment; T1, at 6 hours after THS.
Post-THS blood loss induced significant PLT reductions across all experimental groups compared with the h-sham group (p < 0.05). At T0, the l-THS-3h, h-THS-1h, h-THS-2h, h-THS-3h, and h-THS-4h groups demonstrated significantly lower PLT counts than the l-THS-2h group (p < 0.05). Furthermore, the h-THS-2h, h-THS-3h, and h-THS-4h groups exhibited reduced PLT values compared with the l-THS-3h group (p < 0.05). By T1, the l-THS-3h, h-THS-2h, h-THS-3h, and h-THS-4h groups maintained lower PLT counts relative to the l-THS-2h group (p < 0.05), while no significant difference was observed versus the h-THS-1h group (p > 0.05). Compared with the l-THS-3h group, the h-THS-1h group showed elevated PLT counts (p < 0.05), whereas the h-THS-3h and h-THS-4h groups displayed further reductions (p < 0.05). No inter-group differences were detected between the l-THS-3h and h-THS-2h groups at T1 (p > 0.05) (Table 1).
Hypoxia progression post-THS elevated Lac levels in all groups compared with the h-sham group (p < 0.05). At both T0 and T1, the l-THS-3h, h-THS-2h, h-THS-3h, and h-THS-4h groups demonstrated significantly higher Lac levels than the l-THS-2h group (p < 0.05), while no differences were observed versus the h-THS-1h group (p > 0.05). Compared with the l-THS-3h group, the h-THS-1h group exhibited lower Lac levels (p < 0.05), whereas the h-THS-3h and h-THS-4h groups showed increased values (p < 0.05). No significant differences were detected between the l-THS-3h and h-THS-2h groups (p > 0.05).At both timepoints, the h-THS-3h and h-THS-4h groups displayed significantly lower pH values compared with the l-THS-2h group (p < 0.05), while no differences were observed versus the l-THS-3h, h-THS-1h, or h-THS-2h groups (p > 0.05). The h-THS-1h group exhibited higher pH values than the l-THS-3h group (p < 0.05), whereas the h-THS-4h group demonstrated reduced values (p < 0.05). No significant differences in pH were detected between the l-THS-3h group and either the h-THS-2h or h-THS-3h groups (p > 0.05) (Table 1).
Effects of TXA administration timing on coagulation parameters in rabbits after acute exposure to high-altitude THS
Post-THS, all THS groups exhibited significantly increased PT, APTT, and D-dimer levels (p < 0.05) alongside reduced FIB concentrations (p < 0.05) compared with the h-sham group. At both T0 and T1, the h-THS-2h, h-THS-3h, and h-THS-4h groups demonstrated elevated PT, APTT, and D-dimer levels (p < 0.05) but lower FIB values (p < 0.05) relative to the l-THS-2h group, whereas no significant differences were observed compared with the h-THS-1h group (p > 0.05) (Table 2). When compared with the l-THS-3h group, the l-THS-2h and h-THS-1h groups showed decreased PT, APTT, and D-dimer levels (p < 0.05) with higher FIB concentrations (p < 0.05), while the h-THS-3h and h-THS-4h groups displayed opposite trends (p < 0.05). No inter-group differences were detected between the l-THS-3h and h-THS-2h groups (p > 0.05) (Table 1).
Values of Traditional Coagulation Test in Rabbits of Each Group
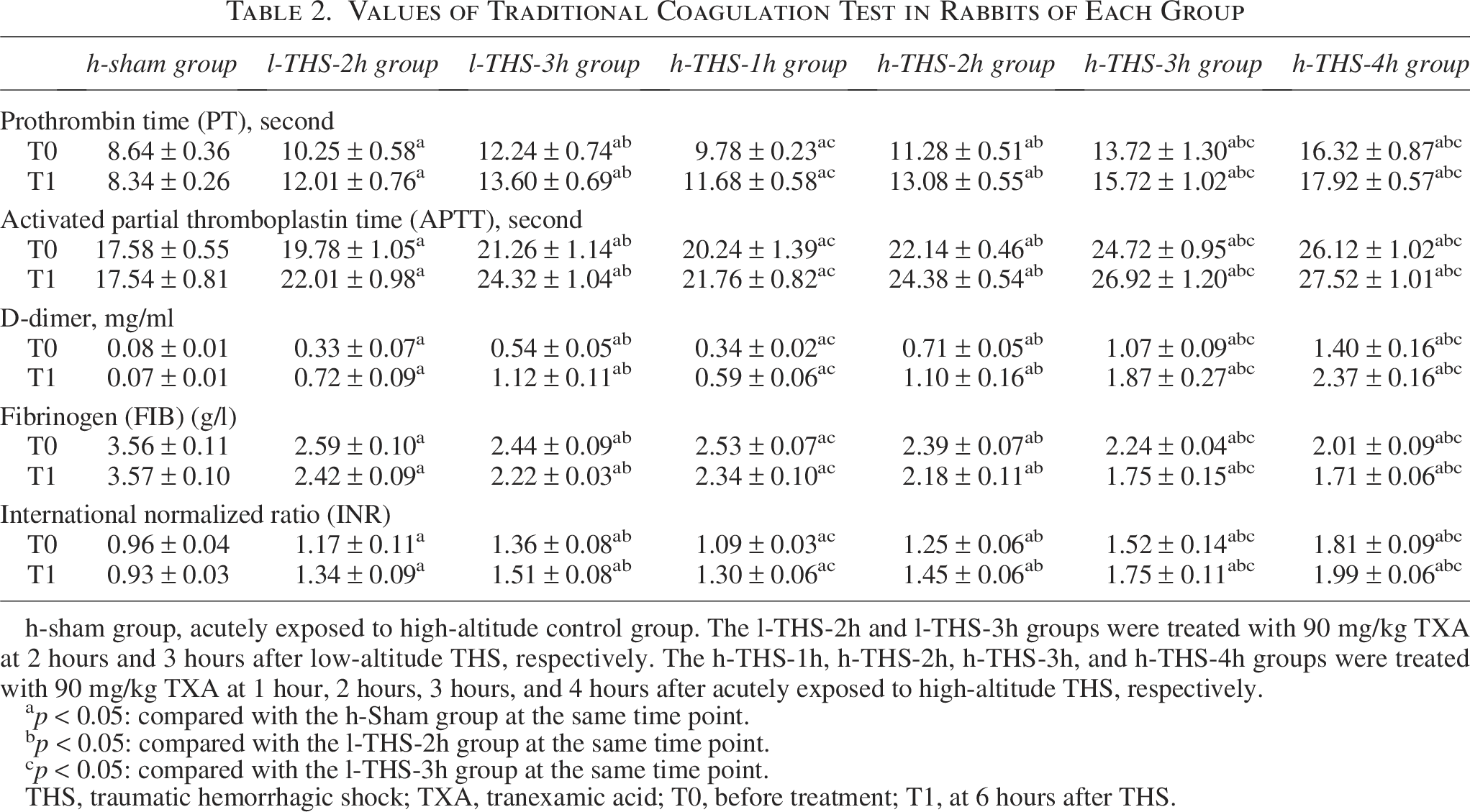
h-sham group, acutely exposed to high-altitude control group. The l-THS-2h and l-THS-3h groups were treated with 90 mg/kg TXA at 2 hours and 3 hours after low-altitude THS, respectively. The h-THS-1h, h-THS-2h, h-THS-3h, and h-THS-4h groups were treated with 90 mg/kg TXA at 1 hour, 2 hours, 3 hours, and 4 hours after acutely exposed to high-altitude THS, respectively.
p < 0.05: compared with the h-Sham group at the same time point.
p < 0.05: compared with the l-THS-2h group at the same time point.
p < 0.05: compared with the l-THS-3h group at the same time point.
THS, traumatic hemorrhagic shock; TXA, tranexamic acid; T0, before treatment; T1, at 6 hours after THS.
INR conversion revealed higher TIC susceptibility in the h-THS-2h, h-THS-3h, and h-THS-4h groups compared with the l-THS-2h group at both timepoints (Leeper et al., 2016; Peltan et al., 2015), with no significant difference observed versus the h-THS-1h group (p > 0.05). Relative to the l-THS-3h group, the l-THS-2h and h-THS-1h groups demonstrated lower INR values, whereas the h-THS-3h and h-THS-4h groups exhibited increased TIC predisposition (p < 0.05). No statistical differences were found between the l-THS-3h and h-THS-2h groups (p > 0.05) (Table 2).
Effects of TXA administration timing on inflammatory response, syndecan-1, and PAI-1 in rabbits after acute exposure to high-altitude THS
Progression of THS induced significant increases in IL-6, TNF-α, syndecan-1, and PAI-1 across all THS groups compared with the h-sham group (p < 0.05). At both T0 and T1, the l-THS-3h, h-THS-2h, h-THS-3h, and h-THS-4h groups demonstrated elevated IL-6, TNF-α, syndecan-1, and PAI-1 levels relative to the l-THS-2h group (p < 0.05), whereas no significant differences were observed compared with the h-THS-2h group (p > 0.05) (Table 3). When compared with the l-THS-3h group, the h-THS-1h group exhibited reduced IL-6, TNF-α, syndecan-1, and PAI-1 concentrations (p < 0.05), while the h-THS-3h and h-THS-4h groups showed further increases (p < 0.05). No inter-group differences were detected between the h-THS-2h and l-THS-3h groups for any parameters (p > 0.05) (Table 3).
Plasma Concentrations of Biomarkers in Rabbits of Each Group Determined by Enzyme-Linked Immunosorbent Assay

h-sham group, acutely exposed to high-altitude control group. The l-THS-2h and l-THS-3h groups were treated with 90 mg/kg TXA at 2 hours and 3 hours after low-altitude THS, respectively. The h-THS-1h, h-THS-2h, h-THS-3h, and h-THS-4h groups were treated with 90 mg/kg TXA at 1 hour, 2 hours, 3 hours, and 4 hours after acutely exposed to high-altitude THS, respectively.
p < 0.05: compared with the h-Sham group at the same time point.
p < 0.05: compared with the l-THS-2h group at the same time point.
p < 0.05: compared with the l-THS-3h group at the same time point.
THS, traumatic hemorrhagic shock; TXA, tranexamic acid; T0, before treatment; T1, at 6 hours after THS.
Effects of TXA administration timing on lung tissue injury and water content in rabbits after acute exposure to high-altitude THS
Histopathological examination under 10 × 40 light microscopy revealed marked thickening of the pulmonary interstitium, cytoplasmic leakage, and extensive infiltration of erythrocytes and inflammatory cells in the h-THS-3h and h-THS-4h groups, accompanied by significantly elevated lung water content compared with other groups (Fig. 1). Relative to the l-THS-2h group [lung injury score: 1.8 (1.0, 2.0); W/D: 6.27 ± 0.13; TLW: 83.36 ± 0.99], the l-THS-3h [2.6 (2.0, 3.0); 6.66 ± 0.23; 84.96 ± 0.51], h-THS-2h [2.8 (2.0, 3.5); 6.61 ± 0.07; 84.88 ± 0.15], h-THS-3h [5.6 (4.5, 6.5); 6.99 ± 0.23; 86.48 ± 1.37], and h-THS-4h [6.2 (6.0, 6.5); 7.20 ± 0.09; 86.71 ± 0.75] groups exhibited significantly higher lung injury scores, W/D ratios, and TLW values (p < 0.05). Furthermore, the h-THS-1h group demonstrated lower lung injury scores, W/D, and TLW compared with the l-THS-3h group, whereas the h-THS-3h and h-THS-4h groups showed further increases (p < 0.05). No statistically significant differences were observed between the l-THS-2h and h-THS-1h groups or between the l-THS-3h and h-THS-2h groups (p > 0.05) (Fig. 1).
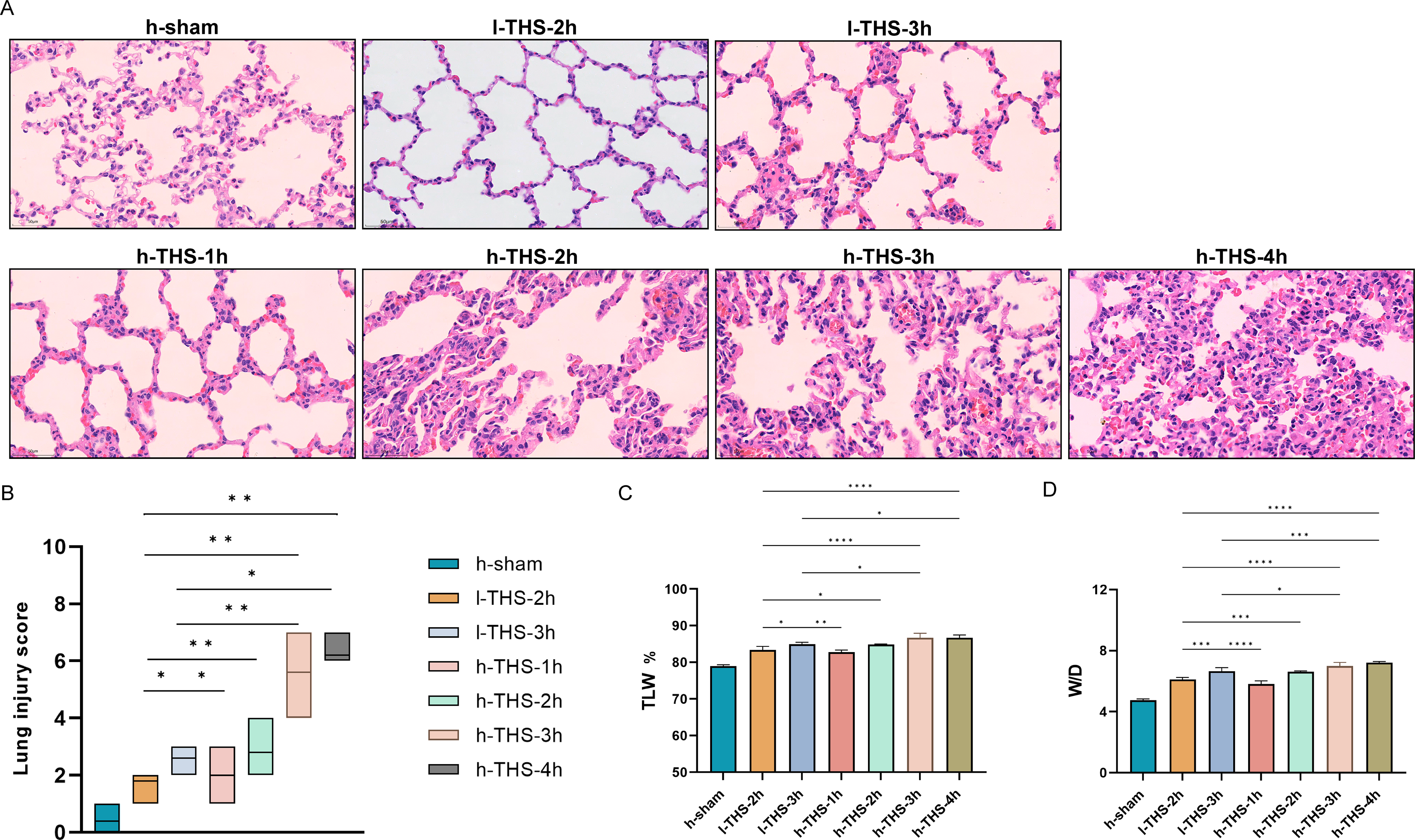
HE staining of lung tissue (×400) and moisture content of lung tissue. Note: *p < 0.05, **p < 0.01, ***p < 0.001, and ****p < 0.0001: compared with the l-THS-3h group.
Discussion
Over 25% of trauma patients develop TIC in the prehospital phase, which elevates their 24-hour mortality risk by 8-fold compared with non-TIC patients (Buzzard and Schreiber, 2024; Jachetti et al., 2019). Timely administration of TXA within 3 hours post-THS significantly reduces transfusion requirements and mortality (Rossaint et al., 2023). However, delayed TXA use (>3 hours) may exacerbate secondary hemorrhage and disseminated intravascular coagulation risks (Gayet-Ageron et al., 2018). Current TXA guidelines are predominantly based on physiological responses in low-altitude populations (Gruen et al., 2023; Rossaint et al., 2023); there have been no studies on the use of TXA after a special physiological response caused by acutely exposed to high-altitude environments. In this animal model, a single 90 mg/kg dose of TXA, administered within 2 hours following THS under acute high-altitude conditions, achieves therapeutic effects comparable with those observed with administration within 3 hours in low-altitude settings. However, the efficacy of TXA diminished significantly when administered beyond this 2-hour frame. These findings may provide valuable reference for optimizing emergency care protocols targeting traumatic hemorrhage populations following rapid ascent to high-altitude regions.
First, field evidence from mass casualty incidents (e.g., 2017 United Kingdom and 2024 Russia incidents) highlights limitations of the traditional 10-minute 1 g TXA infusion in real-world scenarios (Omori and Roberts, 2023). Alternative routes, such as intramuscular or intravenous bolus, may better suit austere environments, with comparable pharmacokinetics across intraosseous, IM, and IV delivery (Goodwin et al., 2022; Haberkorn et al., 2024). Furthermore, a 2 g TXA bolus reduces transfusion needs and mortality without increasing thromboembolic or seizure risks (Drew et al., 2020). Aligning with the updated TCCC guidelines, this study adopted a 1-minute IV bolus of 90 mg/kg TXA (equivalent to 2 g in humans based on a 3:1 interspecies conversion ratio).
Notably, high-altitude THS required 51.00 ± 2.45 ml of blood loss to achieve target MAP (55 ± 5 mmHg), significantly lower than the 59.60 ± 3.65 ml in low-altitude THS group (p < 0.05). By simulating an altitude of 5000 m (10% oxygen concentration), hypoxia-induced compensatory increases in RBC were observed. However, despite higher RBC counts in the high-altitude THS group compared with the low-altitude group, oxygen delivery remained insufficient, leading to a substantial accumulation of Lac from anaerobic metabolism (Zhong et al., 2022). Lac levels were positively correlated with THS severity and served as an effective prognostic predictor (Raux et al., 2017; Zhang et al., 2024; Zheng et al., 2024). In this study, we found that Lac levels increased progressively with prolonged THS duration. Notably, TXA administration at 1 and 2 hours post-THS in the high-altitude group achieved Lac reduction effects equivalent to those observed at 2 and 3 hours in the low-altitude group, respectively. However, delayed TXA administration (>3 hours post-THS) in the high-altitude group resulted in significantly higher Lac levels compared with the low-altitude group at 3 hours, likely due to exacerbated anaerobic metabolism under prolonged hypoxia. This phenomenon may be associated with exacerbated anaerobic metabolic activity in tissues induced by prolonged severe hypoxia.
Importantly, THS induced progressive prolongation of PT and APTT, alongside elevated D-dimer levels and reduced FIB. In the high-altitude THS group, persistent hypocoagulability at 3 hours post-THS exacerbated the consumption of coagulation factors, rendering TXA less effective in restoring fibrinolytic balance compared with the low-altitude group at 3 hours (Zhong et al., 2022, 2023). This accelerated coagulopathy increased the risk of TIC (INR > 1.5) (Leeper et al., 2016; Peltan et al., 2015). Further analysis revealed that TXA administered within 1–2 hours post-THS in the high-altitude group effectively suppressed hyperfibrinolysis, achieving coagulation improvements comparable to delayed treatment (2–3 hours) in the low-altitude group. In contrast, TXA delayed to 3 hours post-THS showed markedly reduced efficacy. This phenomenon may be linked to hypoxia-driven acceleration of PAI-1 responses (Morrow and Mutch, 2023). Specifically, PAI-1 levels in the high-altitude group at 1 hour post-THS reached levels equivalent to those at 2 hours in the low-altitude group, suggesting that rapid “fibrinolytic shutdown” promotes microthrombosis (Prudovsky et al., 2022; Rossaint et al., 2023), a pathological process that early TXA intervention could mitigate.
After the onset of THS, in response to shock-induced stimulation, inflammatory factors IL-6 and TNF-α are massively released, and the integrity of the endothelial glycocalyx is compromised. Syndecan-1, serving as one of the markers for endothelial cell damage, starts to detach 15 minutes post-THS. It has a close relationship with IL-6 and TNF-α. A high level of syndecan-1 can indicate a poor prognosis (Johansson et al., 2011). Our results demonstrated that IL-6, TNF-α, and syndecan-1 levels increased progressively with THS duration. In the high-altitude group, these markers at 1 and 2 hours post-THS matched those at 2 and 3 hours in the low-altitude group, respectively. Delayed TXA administration (3 hours) in the high-altitude group further exacerbated inflammation and endothelial injury. Early TXA intervention (1–2 hours) likely inhibited plasminogen activation, indirectly suppressing plasmin-mediated complement activation and inflammatory cytokine release (Barrett et al., 2019). This mechanism reduced thrombin generation and mitigated direct inflammatory damage to endothelial cells, thereby preserving glycocalyx stability post-THS.
Finally, the ischemia and hypoxia caused by insufficient effective circulating blood volume after THS can lead to irreversible damage to tissue cells. Through histological observation, we found that using TXA 3 hours after acute high altitude exposure and THS can cause significant damage to the morphological structure of lung tissue. The interstitium thickens and is filled with a large number of RBCs and inflammatory cells. Using TXA 3 hours after acute high altitude exposure and THS results in higher lung W/D and TLW compared with using it 3 hours after THS in a low-altitude environment. This may be related to the fact that high-altitude hypoxia exacerbates pulmonary hypertension and the pulmonary inflammatory response, which can activate the plasmin-bradykinin axis and increase vascular permeability (Gatterer et al., 2024), early use of TXA may be related to alleviating the abnormal pathophysiological process caused by the rapid increase of PAI-1 (Gibson et al., 2021). Using TXA 2 hours after acute high altitude exposure and THS has the same effect on alleviating lung tissue damage and reducing lung water content as using it 3 hours after THS in a low-altitude environment.
Our findings suggest that a single 90 mg/kg dose of TXA administered within 2 hours post-THS in rabbits exposed to 5000 m for 3 days provides therapeutic efficacy comparable with administration at 3 hours post-THS in low-altitude environments. TXA effectively mitigated coagulofibrinolytic disorders, stabilized cellular metabolism, suppressed inflammation, reduced tissue injury, and lowered pulmonary edema risk. These results indicate that the optimal TXA administration window for traumatic hemorrhagic shock may be shorter at high altitudes than at sea level. While these findings could influence high-altitude TXA treatment guidelines, further studies are needed to confirm this hypothesis in humans.
This study has several limitations. First, while we selected low-altitude groups at 2- and 3-hour post-THS to validate the 3-hour therapeutic window of TXA and compare it with high-altitude THS, interspecies differences between rabbits and humans may affect translational relevance, necessitating further research. Second, the simulated altitude was fixed at 5,000 m; variations in physiological responses (e.g., coagulation-fibrinolytic dynamics and inflammatory reactions) at different altitudes may influence TXA efficacy, which requires systematic investigation in future studies. Finally, despite statistically significant results, the relatively small animal sample size may introduce instability, and larger cohorts will be included to enhance robustness in subsequent work.
Authors’ Contributions
Z.L. designed and performed the experiments. C.N., L.Y., H.J., C.L, and Y.Z. conducted the experiments and data analysis. M.L. contributed to review and editing, conceptualization, and supervision. All authors have reviewed, edited, and consented to the final version of the article.
Footnotes
Acknowledgments
The authors declare that they have not used AI-generated work in this article.
Author Disclosure Statement
None of the authors have any conflict of interest, financial or otherwise, to disclose. All authors have approved the contents of this article.
Funding Information
No funding was received for this article.
Data Availability
The data that support the findings of this study are available on request from the corresponding author.