
Abstract
Wakeham, Denis J, Andrew R Tomlinson, Giorgio Manferdelli, Matthew M Howrey, Anna K Geib, Murugappan Ramanathan, Marcus Payne, Renie Guilliod, James Berry, Tony G Babb, Peter Hackett, Benjamin D Levine, and Christopher M Hearon. The Physiological and Altitude Lowering Effects of Different Supplemental Oxygen Flow Rates at Extreme Simulated Altitude: A Pilot Study. High Alt Med Biol. 00:00–00, 2025.
Background:
Approximately 80% of high-altitude climbers use supplemental oxygen >8,000 meters, yet optimal dosing strategies have not been established.
Methodology:
Therefore, in six unacclimatized individuals (34 ± 8 years; 2 F/4 M), we quantified the effects of supplemental oxygen flow rates (6, 4, 2, 1 and 0 L/min) using the SUMMIT Oxygen mask at 282 mmHg (rest and cycle ergometry: 60 and 120 Watts) and 253 mmHg (rest only) barometric pressure in a hypobaric chamber. We measured oxygen saturation (SpO2) and gas fractions in the mask during 4-minute exposures to each flow rate.
Results:
Resting at 282 mmHg, SpO2 (6 L/min: 99% ± 0%; 0 L/min: 70% ± 8%, p < 0.001) and mean inspired oxygen fraction decreased (6 L/min: 65.87% ± 14.11%; 0 L/min: 21.50% ± 0.44%, p < 0.001) with lowering of supplemental oxygen. Exercise further decreased SpO2 and oxygen fractions across all flow rates at 282 mmHg. At 253 mmHg, SpO2 followed a similar trend to data collected at 282 mmHg (6 L/min: 96% ± 2%; 4 L/min: 93% ± 3%; 2 L/min: 87% ± 3%; 1 L/min: 71% ± 0%; 0 L/min: 66% ± 9%). Furthermore, at rest at 253 mmHg, 2 L/min of supplemental oxygen lowered the equivalent altitude to 4,489 meters.
Conclusion:
All unacclimatized participants were able to tolerate 253 mmHg at rest on as little as 2 L/min of supplemental oxygen.
Introduction
Exposure to extreme altitude presents a severe physiological challenge, but logistical difficulties have limited the number of comprehensive physiological studies conducted in such conditions, whether simulated in a hypobaric chamber or in the field. The most detailed assessments of human physiology at extreme altitude were part of the Operation Everest II studies (Houston et al., 1987; Wagner, 2010). These investigations helped define the adaptive capacity of humans to extreme altitude and, along with the American Medical Research Expedition to Everest, demonstrated the exceptional physiological ability required to summit Everest without supplemental oxygen (West, 1983; West, 2010). Since then, the number of tourists and summit attempts on Mt. Everest has increased significantly, with over 800 total summits in 2024 alone. This rise in successful attempts is largely due to the widespread use of commercially available supplemental oxygen systems, rather than an increase in highly skilled mountaineers. Despite decades of research and field use of supplemental oxygen (McMorrow et al., 2012; Windsor et al., 2007), the physiological differences between exposure to extreme altitude with and without it have not been thoroughly tested beyond studies providing 100% oxygen, such as in Operation Everest II (Wagner et al., 1987). However, 100% supplemental oxygen does not reflect the effects of modern altitude masks that supply a mixture of 100% oxygen and ambient air.
Approximately 80% of high-altitude climbers use supplemental oxygen above 8000 m, with 98% of climbers using supplemental oxygen to summit Mt. Everest (Himalayan Database, 2025). The use of supplemental oxygen is associated with higher success and survival rates as well as less altitude illness, high-altitude debilitation, frostbite, and hypothermia (Huey and Eguskitza, 2000). Partly because of the higher success rates, there has been about a fourfold increase in the number of first-time climbers to the summit of Mt. Everest over the past two decades (Huey et al., 2020). The physiological implications of such overcrowding are starting to be realized. Increased crowding, coupled with potential unfavorable weather conditions, leaves climbers spending increasing time at extreme altitude. These factors markedly impact the requirement for supplemental oxygen, thereby increasing logistical challenges and reducing the likelihood of summit success. Furthermore, with commercially guided and/or inexperienced climbers spending less time acclimatizing and relying more on supplemental oxygen, it is essential to understand the minimal required “dose” of supplemental oxygen at rest and during exercise at extreme altitude.
Mask altitude, or the fraction of inspired oxygen (FiO2) within the mask and its associated equivalent altitude lowering effect, was first estimated by the pioneering work of Thomas Hornbein, M.D. (Rodway and Schoene, 2025), in 1963 by simulating changes in inspired oxygen volume and ventilation (Hornbein, 1962). However, no study has directly assessed mask altitude by quantifying the oxygen concentration within the mask based on the mixing of 100% oxygen and ambient air. Additionally, no studies have investigated the minimum dose of oxygen required to offset the physiological effects of (severe) hypoxemia at extreme altitude. Therefore, this information remains a critical knowledge gap for guiding supplemental oxygen use on the mountain. Our pilot study aimed to quantify the effect of supplemental oxygen flow rates on oxygen saturation and mask altitude at rest and during exercise at extreme simulated altitudes of 282 mmHg barometric pressure (Pb; 8,100 meters; Annapurna summit) and 253 mmHg Pb (8,848 meters; Mt. Everest summit) in a hypobaric chamber.
Methodology
Six individuals were recruited for this study (four males, two females; age: 34 ± 8 years; body mass: 76 ± 10 kg; BMI: 24.2 ± 2.1 kg/m2), of whom three (two males, one female) spent ∼48 hours above 10,000 ft (3,048 m) immediately (<72 hours) before arrival in Dallas for testing and were experienced high-altitude mountaineers with previous climbs >7,000 m. Following provision of informed consent, pre-participation health screenings were performed by the Hyperbaric Medicine Center at the Institute for Exercise and Environmental Medicine at Texas Health Presbyterian Hospital Dallas. Participants were free from any diagnosed chronic autonomic, cardiovascular, respiratory, metabolic, renal, or muscular diseases. Study approval was granted by the Institutional Review Board of The University of Texas Southwestern Medical Center (STU-2022-0235).
Study protocol
Participants completed one study visit (Fig. 1). The study team (study physician, safety officer, and researcher) and participant entered the hypobaric chamber, were fitted with an oxygen mask (United States Air Force mask), and began 120 minutes of oxygen pre-breathing (100% oxygen) to reduce the risk of altitude decompression sickness. During pre-breathing, all individuals completed exercise at low, medium, and high intensities to aid denitrogenation. The participant exercised for 1 hour, while the study team each exercised for 15 minutes. Final instrumentation and signal checks were performed at a Pb of 475 mmHg (4,000 meters). Thereafter, data were acquired at 2 altitudes with target Pb’s of 282 mmHg (8,100 meters) and 253 mmHg (8,848 meters) calculated from Pb using the West equation (1996, West et al., 1983).

Study Protocol. See methodology for detailed description.
Following pre-breathing, the chamber was decompressed (ascent) to 475 mmHg at a rate of 305 m/min. At this altitude, participants were fitted with a capillary line next to their mouth, attached to a mass spectrometer (MA Tech Services, Saint Louis, MO, USA) to measure gas fractions within the SUMMIT Standard System mask (Fig. 2A). Participants then used the SUMMIT mask and regulator connected in series to a 100% oxygen tank. The SUMMIT regulator is factory calibrated at sea level to provide flow rates between 0 and 6 L/min, and it was set to deliver 6 L/min of nominal supplemental oxygen. Participants were instrumented with a forehead pulse oximeter (Nellcor, Minneapolis, MN, USA) for continuous recording of SpO2 and heart rate via photoplethysmography. The expiration port of the SUMMIT mask was connected to a Universal Ventilation Meter (VacuMed) to measure expired volume and respiratory rate. The participant then began 4 minutes of exercise on a cycle ergometer (Lode Excalibur) to familiarize them with exercising with the SUMMIT mask and to confirm the quality of gas fraction waveforms.

Summit Standard System Oxygen Mask and example oxygen fraction waveform.
Thereafter, an ascent to 282 mmHg commenced at a rate of 305 m/min. At 365 mmHg (6,100 m), the ascent rate was reduced to 152.5 m/min until the target barometric pressure of 282 mmHg was reached. After stabilization, participants began 4-minute stages of decreases in supplemental oxygen at rest from 6 to 4, 2, 1, and 0 L/min (nominal flow) or until they reached the safety criteria of SpO2 <70% plus symptoms (lightheadedness, nausea, etc.). Participants and their vital signs were directly monitored continuously by study personnel inside the chamber, as well as outside the chamber via live video feed. Participants were assessed for alertness and symptoms throughout the protocol by qualified safety, medical, and research personnel. Following resting measurements, participants were returned to 6 L/min of supplemental oxygen, and once SpO2 was stable, participants began exercising at 60 Watts before the stepwise reductions in supplemental oxygen (6, 4, 2,1, and 0 L/min, nominal flow) were repeated until safety criteria were reached. Following recovery on 6 L/min, the exercise protocol was repeated at 120 Watts. Following adequate participant recovery, the chamber was decompressed (ascent) to 253 mmHg at a rate of 30 m/min while participants cycled at 60 Watts, breathing 6 L/min of supplemental oxygen. Once at 253 mmHg, the same stepwise reduction in supplemental oxygen was performed at rest. Upon completion of data collection, participants were returned to 6 L/min of supplemental oxygen, and the chamber was compressed to sea level at a rate of 600 m/min or at a rate that allowed participants to equalize their middle-ear pressure appropriately.
Data analysis
SUMMIT mask and regulator
The SUMMIT regulator settings of 0–6 L/min represent the nominal flow, which is calibrated at sea level (Pb 760 mmHg). As there are no available data regarding the measured flow of supplemental oxygen provided by the SUMMIT regulator at altitude, the volume of oxygen delivered by the regulator over three minutes was collected into Douglas Bags at 282 mmHg and 253 mmHg. Douglas bag volume was quantified using a 3-L calibration syringe at each altitude to calculate the actual flow at each barometric pressure.
Mask gas fractions
Continuous measurements of gas fractions were recorded at 250 Hz (BIOPAC Version 5.0, Goleta, CA, USA). During pilot testing, dynamic mixing of ambient air with supplemental oxygen was observed inside the mask, as well as a reservoir effect, which produced distinct patterns of oxygen fractions that were not suitable for standard assessments of FiO2; see Figure 2B for a typical waveform. The SUMMIT oxygen mask contains a 200 ml reservoir that fills with oxygen during expiration and three separate one-way valves for inspiration of oxygen, inspiration of ambient air, and expiration. Based on the measured waveform, we posit that upon inspiration, the one-way valve for the oxygen reservoir opens just before the valve for ambient air, likely due to higher pressure within the oxygen reservoir compared to the atmosphere. The sequential opening of the two inspiratory valves results in an initial peak in oxygen concentration from the reservoir, followed by a decline and eventual nadir at a lower inspired oxygen concentration once the ambient valve opens and mixes with the supplemental oxygen. Near the end of inspiration, the ambient inspiratory air valve closes first, while closure of the oxygen inspiratory valve is delayed due to continued pressure/flow from the regulator (Fig. 2B). Representative oxygen fraction waveforms across the nominal flow rates are shown in Figure 3. The time-averaged mean (TA-mean) oxygen fraction during inspiration and the end-tidal (∼alveolar) oxygen fraction in the final minute of each supplemental oxygen flow setting under each condition were calculated (Fig. 4).

Example of typical oxygen fraction waveforms collected at the mouth inside the SUMMIT mask at different nominal flow rates for a single participant. The blue-highlighted section represents the data used to calculate the time-averaged (TA) mean oxygen fraction during inspiration; the orange represents the data used to calculate the End-Tidal O2 fraction.
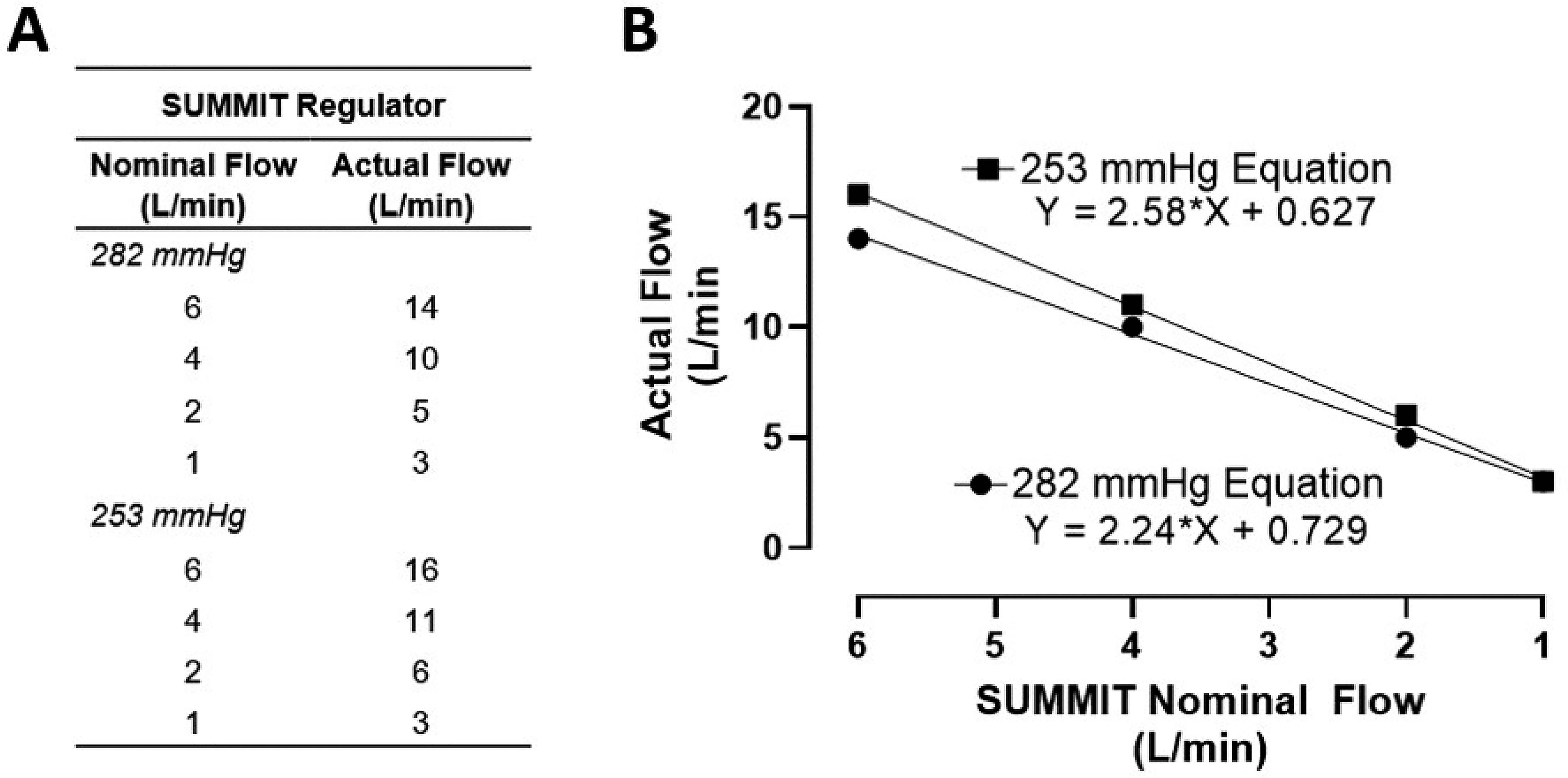
Nominal versus actual (measured) flow of supplement oxygen from the SUMMIT regulator at 282 mmHg and 253 mmHg
Equivalent altitude
Equivalent altitude was estimated by comparing our measured SpO2 at each flow setting and condition to the SaO2-Pb curves (second-order polynomial) generated from Operation Everest II data (Sutton et al., 1988). Three reference SaO2–Pb curves were created using previously published data collected in a hypobaric chamber at rest, 60 Watts, and 120 Watts across a range of altitudes: sea level (760 mmHg), 4,840 meters (428 mmHg), 6,500 meters (348 mmHg), 8,100 meters (282 mmHg), and 8,848 meters (240 mmHg) (Sutton et al., 1988). The best-fit equations are as follows:



Using these equations, Pb was calculated from measured SpO2 in each individual during each condition and converted to altitude using the West equation (1996). Any calculated Pb from SpO2 that was lower than the actual Pb (either 282 mmHg or 253 mmHg) is reported as the prevailing Pb, and an SpO2 of 98% or above was considered equivalent to sea level. All measurements taken at 0 L/min flow were input as the simulated altitude.
Statistical analyses
Data are presented as mean ± standard deviation. The relationship between nominal and measured flow using the SUMMIT Regulator was assessed with linear regression. The effect of supplemental oxygen flow rate at rest and during exercise, at 282 and 253 mmHg, was analyzed using a mixed-effects model for repeated measures. Due to missing data at the lower flow rates and higher exercise workloads, only times with more than two data points were included in our statistical analyses. Statistical analysis was conducted only within each condition to determine the effects of lowering the supplemental oxygen flow rate. The relationship between SpO2 and both TA-mean and the end-tidal oxygen fraction was analyzed using a one-phase exponential curve. Statistical analyses were performed with Prism v.10.0 (GraphPad Software, San Diego, CA, USA). A p < 0.05 was considered statistically significant for all tests.
Results
Nominal versus actual flow of supplemental O2
The actual flow rates of supplemental oxygen corresponding to each nominal flow on the SUMMIT Regulator at 282 mmHg and 253 mmHg of altitude are shown in Figure 4A, while their relationship across flow rates at both 282 mmHg (r2 = 1.00) and 253 mmHg (r2 = 1.00) is shown in Figure 4B. The measured flows were 2–3-fold greater than nominal at simulated altitudes >8,100 meters.
Oxygen saturation and heart rate
SpO2, heart rate, and nominal flow rate are shown for one individual during decreases in supplemental oxygen at rest at 282 mmHg in Figure 5. During rest at 282 mmHg, stepwise reductions in supplemental O2 flow rate caused decreases in SpO2 and a corresponding increase in heart rate (Table 1). This pattern of decreasing SpO2 and increasing heart rate with lowering of the supplemental oxygen flow rate was similar at 60 Watts of exercise and rest at 253 mmHg (Table 1). No change in HR was detected during 120 Watts at 282 mmHg with decreasing flow rates of supplemental oxygen (p = 0.471; Table 1); however, only one participant was able to exercise at 120 Watts on 1 L/min, and no participant could exercise at 120 Watts without supplemental oxygen. Therefore, the limited data reduces our statistical power for this condition.
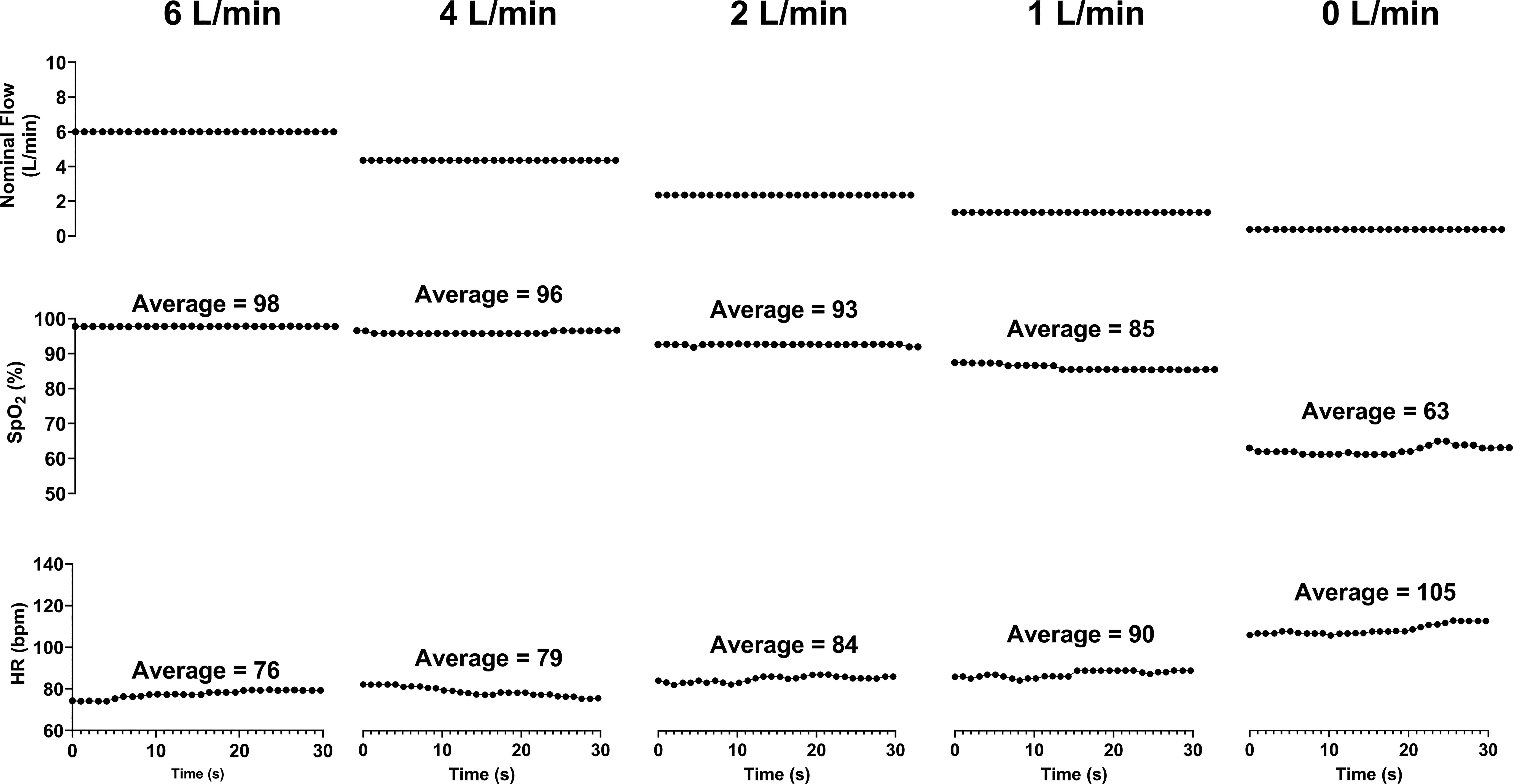
Heart rate (HR) and oxygen saturation (SpO2) during seated rest at 282 mmHg in one participant at different nominal flow rates of supplemental oxygen. Each stage was 4 minutes in duration and the data shown are from the final 30 seconds of each condition.
Physiological Responses to Lowering Supplement Oxygen Flow Rates
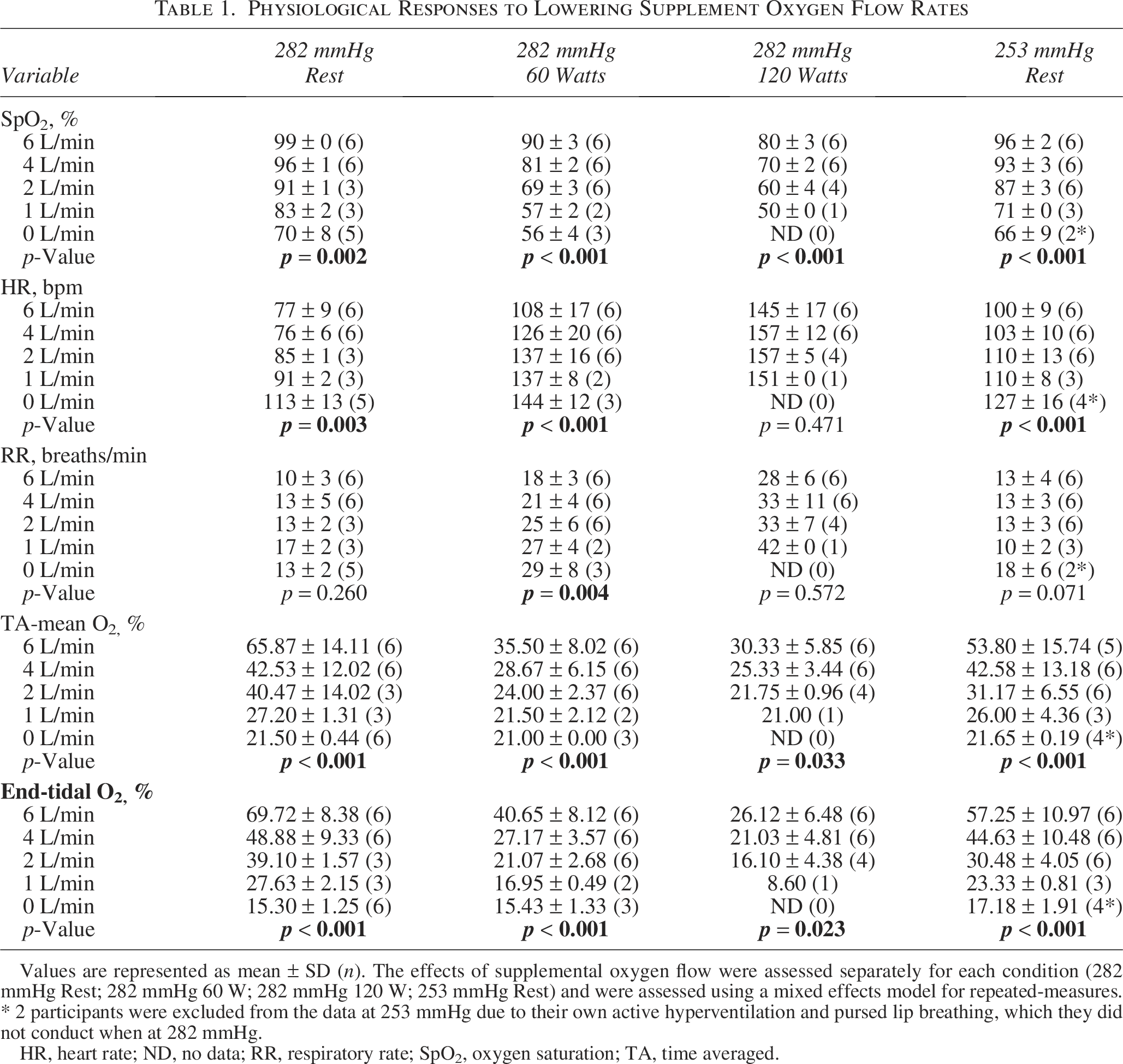
Values are represented as mean ± SD (n). The effects of supplemental oxygen flow were assessed separately for each condition (282 mmHg Rest; 282 mmHg 60 W; 282 mmHg 120 W; 253 mmHg Rest) and were assessed using a mixed effects model for repeated-measures. * 2 participants were excluded from the data at 253 mmHg due to their own active hyperventilation and pursed lip breathing, which they did not conduct when at 282 mmHg.
HR, heart rate; ND, no data; RR, respiratory rate; SpO2, oxygen saturation; TA, time averaged.
At rest, 1 L/min of supplemental oxygen offset the effects of hypoxemia at both 282 mmHg (SpO2: 83 ± 2%) and 253 mmHg (SpO2: 71 ± 1%), while 2 L/min of supplemental oxygen were necessary to maintain SpO2 above ∼60% (69 ± 3%) at 60 Watts of exercise, below which all but one participant reported effects of hypoxemia. At 282 mmHg, exercising at 120 W, participants required 4 L/min of supplemental oxygen to maintain SpO2 above ∼60% (70% ± 1%).
Respiratory rate
Resting respiratory rate was similar across flow rates of supplemental oxygen, both at 282 and 253 mmHg (Table 1), despite a trend for increasing respiratory rate at 253 mmHg without supplemental oxygen. During exercise at 282 mmHg, respiratory rate increased with stepwise reductions in supplemental oxygen during 60 Watts, while no change was observed at 120 Watts, likely because of loss of data points at lower (<2 L/min) flow rates (Table 1).
Mask gas fractions
As supplemental oxygen flow rates decreased during rest at 282 mmHg, there were stepwise reductions in TA-mean oxygen fraction and end-tidal oxygen fraction (Table 1). Similar stepwise decreases in both measures were observed at 60 Watts, 120 Watts, and at rest at 253 mmHg (Table 1). When all data were combined, there were exponential one-phase relationships between both TA-mean and end-tidal O2 fractions with SpO2 (r2 = 0.68 and r2 = 0.81, respectively; Fig. 6).

Exponential relationships between oxygen saturation and Time Averaged (TA)-mean oxygen fraction
Equivalent Altitude
The estimated equivalent altitude decreased as supplemental oxygen flow rates increased, with higher flow needed to reach a similar equivalent altitude during exercise compared to rest. At rest at 282 mmHg, 6 L/min of supplemental oxygen lowered the equivalent altitude to sea level, and 4 L/min of supplemental oxygen brought it to near or below Everest Base Camp altitude (5,364 meters) across all altitudes and exercise intensities (Fig. 7 and 8).

Equivalent altitude at different flow rates and conditions. Equivalent altitudes were calculated from SpO2, using data from the OEII study. Equivalent altitudes shown at 282 mmHg at rest

An illustration of the altitudes lowering effect of supplemental oxygen delivered by the SUMMIT oxygen mask at simulated altitudes during rest and exercise in unacclimatized adults.
Discussion
The primary findings of our study are: (1) Supplemental oxygen flow rates of 1 L/min at rest at 282 mmHg (8,100 meters) and 2 L/min at 253 mmHg (8,848 meters) were sufficient to maintain SpO2 above 60%, below which participants reported effects of hypoxemia; and (2) 4 L/min of supplemental oxygen decreased equivalent altitude to near or below Everest Base Camp altitude (5,364 meters) across all altitudes and exercise intensities. Therefore, in unacclimatized individuals exposed to extreme altitude, 2 L/min of supplemental oxygen may be sufficient to prevent symptoms of severe hypoxemia. Determining the minimum oxygen dose to keep reasonable blood oxygen saturation at extreme altitude in unacclimatized persons has important implications for oxygen strategies and logistics, especially when conserving supplemental oxygen is crucial (e.g., weather delays, queues).
The assessment of “mask altitude,” or the effective altitude within the mask, has been a topic of keen interest in the high-altitude community. The variety of masks with different technologies to provide more than 0.21 FiO2 has caused varying levels of altitude-lowering effects. The SUMMIT oxygen masks are among the most popular for extreme altitude. Our results indicate that the commonly used 4 L/min of nominal supplemental oxygen lowered the effective altitude from 8,100 meters to 2,000 meters at rest, 4,300 meters at 60 Watts, and 5,600 meters at 120 Watts, with similar reductions to 2,800 meters on 4 L/min at rest when on the summit of Mount Everest. Remarkably, 6 L/min at 8100 meters lowered the effective altitude to sea level. These altitude-lowering effects help explain why inexperienced climbers with limited acclimatization can reach extreme altitudes.
To better understand the effects of the SUMMIT mask, we aimed to measure the FiO2 produced at different supplemental oxygen flow rates. However, the unique design of this mask (Fig. 2A) made interpreting these gas fractions (Fig. 3) difficult, and calculating a true FiO2 or volume-averaged inspired oxygen concentration was not feasible without changing the mask’s function. As alternatives to calculating FiO2, we measured a time-averaged mean inspired oxygen concentration and an end-expiratory (∼alveolar) oxygen concentration. The TA-mean inspired oxygen concentration decreased with lower oxygen flow rates and higher minute ventilation, as expected (Table 1), and correlated with the resulting SpO2 (Fig. 6A). Thus, we consider these reasonable surrogates for FiO2 in the SUMMIT mask.
Methodological considerations
The primary methodological limitation of our study is the use of pulse oximetry to measure oxygen saturation and the chamber-based simulation of extreme altitude in unacclimatized adults. Although accurate within the range validated for FDA-approved pulse oximetry devices (i.e., 70%–100% saturation), any values below this threshold should be interpreted with caution. However, in one healthy male, we observed a strong correlation (r2 = 0.994, p < 0.001) between SpO2 and arterial blood oxygen saturation (SaO2, radial artery catheter) across a range of 60%–100%. Future studies with direct measurement of arterial blood gases are required to confirm our findings. As we performed an acute study in a hypobaric chamber, we cannot assess the effects of temperature, sustained high-altitude exposure and acclimatization, repeated high-intensity exercise efforts, dehydration, or high-altitude illness on the requirements for supplemental oxygen. Furthermore, we did not assess the effects of age, sex, or chronic disease, but we hypothesize that fitness, acclimatization and exertion will affect oxygen requirements. In particular, comparing our data to that of Sutton et al., which involved acclimatized individuals, is a limitation since acclimatization, raises SpO2 levels, meaning the equivalent altitude corresponding to our flow rates would likely be lower in acclimatized persons than in unacclimatized ones. These data provide a basis for determining the minimal supplemental oxygen flow rates required to counteract severe hypoxemia.
Conclusions
Supplemental oxygen flow rates lower than common practice (≥4 L/min) can offset the effects of arterial hypoxemia both at rest and during exercise at extreme simulated altitude in unacclimatized adults. Additional studies are needed to refine oxygen management strategies to hopefully lower morbidity, mortality, and waste when climbing to extreme altitude.
Footnotes
Acknowledgments
The authors would like to thank all participants who volunteered for this study. They would like to thank Don Bowie for his involvement in the design and execution of this study. Also, they acknowledge Dean Palmer, Adam Mottley, Jacob Moore, Birgitta Van Dooren, and Randy Gillmore for their technical, safety, and clinical support in running these studies. We want to acknowledge all the personnel at the IEEM who helped run the study. Finally, the authors thank Summit Oxygen for the provision of equipment to conduct the experiment.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
A donation by Chris and Elizabeth Wright.