
Abstract
Zhang, Fengying, Yang Zhong, Qiuyue Li, Doudou Hao, Zhiyou Shi, Suying Zhu, Qian Zhang, and Yunhong Wu. Does Hydrogen-Rich Water Reduce Oxidative Stress in Patients with Chronic Mountain Sickness? A Randomized, Blinded, Controlled Trial. High Alt Med Biol. 00:00–00, 2025.
Background:
Oxidative stress is implicated in the pathogenesis of chronic mountain sickness (CMS), providing a rationale for antioxidant therapies. This study evaluated the safety and efficacy of hydrogen-rich water (HRW) as a potential antioxidant in individuals with CMS.
Methods:
We conducted an 8-week, randomized, blinded, placebo-controlled trial at the Tibetan Hospital of Nagqu, China. Adults with untreated CMS (defined by Qinghai score) were randomly assigned (1:1) to receive 990 ml/day of HRW or placebo using a dynamic minimization method. Participants, clinicians, and investigators were blinded to treatment allocation. The primary efficacy endpoint was change in oxidative stress biomarkers from baseline to week 8, including catalase, glutathione, malondialdehyde (MDA), superoxide dismutase, 8-hydroxy-2’-deoxyguanosine, and total antioxidant capacity (T-AOC). Safety was assessed by adverse event reporting. This trial has been completed and is registered at chictr.org under the identifier ChiCTR2400082685.
Results:
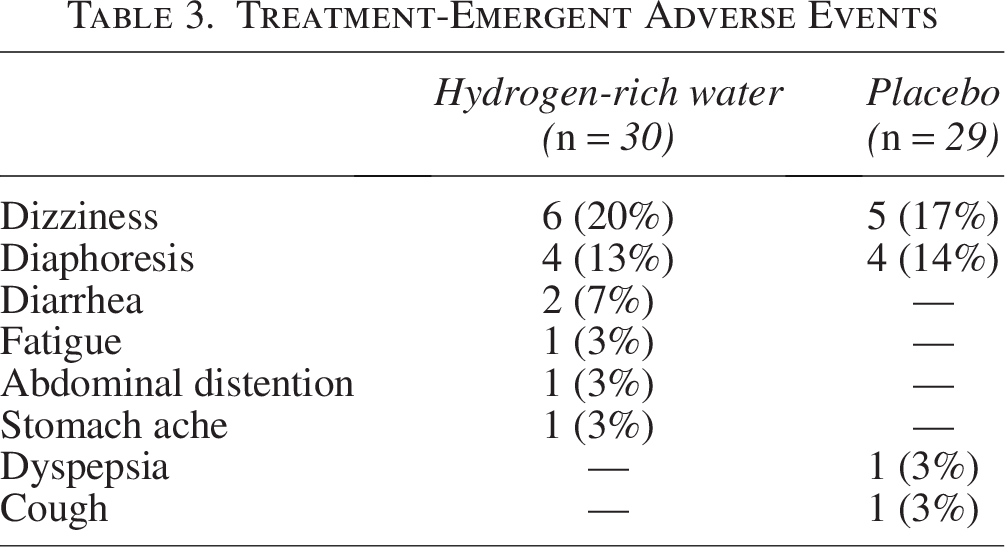
From July 3 to December 24, 2024, 60 participants were randomized; one in the placebo group did not receive treatment and was excluded from the analysis. At week 8, HRW produced greater changes in MDA and T-AOC compared with placebo: MDA, +2.11 (95% CI: 1.13–3.09; p < 0.001); T-AOC, +2.86 (95% CI: 0.09–5.64; p = 0.043). In participants with body mass index (BMI) ≥24, the increase in MDA was more pronounced (Δ+2.57; p = 0.02 for interaction). Adverse events occurred in 50% (15/30) of the hydrogen group and 37% (11/29) of the placebo group; dizziness was the most common.
Conclusion:
HRW demonstrated both pro-oxidative and antioxidative effects in CMS. However, it did not reduce oxidative stress-induced damage and may increase oxidative risk in individuals with higher BMI.
Keywords
Introduction
Chronic mountain sickness (CMS) is a clinical syndrome affecting long-term residents or natives living above 2,500 meters, presenting with a spectrum of physiological symptoms including headache, dizziness, insomnia, fatigue, poor concentration, and memory impairment (León-Velarde et al., 2005). Although those symptoms relief can be achieved by descending to lower altitudes, recurrence is common upon re-exposure to high-altitudes environments. Therefore, developing therapies targeting the disease’s underlying mechanisms to prevent high-altitudes symptom onset remains critical.
CMS pathogenesis is closely linked to chronic hypoxia-induced oxidative stress (Pena et al., 2022; Jefferson et al., 2004). Sustained hypobaric hypoxia leads to excessive production of reactive oxygen species (ROS), which overwhelms endogenous antioxidant defense systems, including enzymatic (e.g., superoxide dismutase [SOD], catalase [CAT]) and non-enzymatic (e.g., glutathione [GSH]) pathways (Gaur et al., 2021; Bailey et al., 2019; Maimaitiyiming et al., 2014). Previous studies have demonstrated that patients with CMS exhibit marked alterations in oxidative stress biomarkers, characterized by elevated malondialdehyde (MDA) levels and reduced activities of key antioxidant enzymes, including SOD and GSH peroxidase, reflecting a disruption of redox homeostasis under chronic hypoxic conditions (Pena et al., 2022). This redox imbalance contributes to lipid peroxidation, oxidative DNA damage, and mitochondrial dysfunction—factors that promote vascular endothelial injury, inflammation, and maladaptive erythropoiesis (Penna and Pagliaro, 2025; Wang and Zennadi, 2021; Bissinger et al., 2019). Concurrently, proteomic analyses in CMS patients highlight upregulated pathways linked to ROS metabolism, hydrogen peroxide catabolism, and acute inflammatory responses (Zhang et al., 2021). These mechanisms not only exacerbate clinical manifestations such as polycythemia and pulmonary hypertension but also accelerate disease progression. As such, oxidative stress is increasingly recognized not only as a hallmark of CMS but also as a viable therapeutic target. Targeting these oxidative pathways and restoring redox balance may offer therapeutic strategies to mitigate CMS progression.
Other antioxidant strategies have been investigated in CMS and high-altitude-related conditions. Supplementation with antioxidant vitamins (e.g., vitamins C and E) and N-acetylcysteine has shown partial attenuation of hypoxia-induced oxidative damage, although the effects remain inconsistent and limited by poor bioavailability (Dhar-Mascareño et al., 2005; Mariacher et al., 2013). Pharmacological agents with antioxidant or vasodilatory properties, such as acetazolamide and certain flavonoids, have demonstrated some benefit in reducing hypoxemia or oxidative burden, but their application is often restricted by side effects, tolerance issues, or non-specific actions (Kushwaha and Saraswat, 2024). These limitations underscore the need for more selective and safer antioxidant approaches.
Hydrogen-rich water (HRW), known for its selective antioxidant activity, has emerged as a promising candidate for modulating oxidative stress-related conditions. Molecular hydrogen (H2), the active component in HRW, has been shown to selectively reduce hydroxyl radicals and peroxynitrite—highly cytotoxic species implicated in hypoxia-induced cellular injury—without disturbing beneficial redox signaling pathways (Ohsawa et al., 2007; Ostojic, 2021). Preclinical and clinical studies in other oxidative stress-associated diseases have demonstrated the potential of HRW to alleviate inflammation, improve mitochondrial function, and enhance overall redox homeostasis (Meng et al., 2025; LeBaron et al., 2020; Liang et al., 2023). Given the central role of oxidative stress in CMS pathogenesis, HRW represents a biologically plausible and potentially safe adjunctive intervention.
In this study, we conducted a blinded, randomized, placebo-controlled trial to evaluate the effects of an 8-week HRW intervention on oxidative stress in patients with CMS. We aimed to assess both the efficacy and safety of HRW in this high-altitude population, and to explore its potential role as a therapeutic strategy targeting redox imbalance in CMS.
Methods
Study design
We conducted a randomized, blinded, placebo-controlled, single-center study that evaluated the efficacy and safety of HRW on oxidative stress in people with untreated CMS. The trial was conducted at the Tibetan Hospital of Nagqu (Tibetan, China). The study has received approval from the Institutional Review Board of Hospital of Chengdu Office of People’s Government of Tibetan Autonomous Region (No.: 2024-73, Supplementary Appendix A1–A2) and is registered at the Chinese Clinical Trial Register Center (Identifier: ChiCTR2400082685). The Consolidated Standards of Reporting Trials (CONSORT) reporting guideline and the corresponding checklist for randomized clinical trials was followed to report this study (Supplementary Appendix A3–A6) (Schulz et al., 2010).
Participants
All patients provided written informed consent (Supplementary Appendix A7–A14). Eligible patients were aged 18–65 years and met the diagnostic criteria for CMS based on the Qinghai score, proposed by the International Society for Mountain Medicine at the VI World Congress on Mountain Medicine and High Altitude Physiology. Body mass index (BMI) ranging from 18 to less than 28 kg/m2 and a self-reported residence history in the survey area for 3 years were also required. Patients were excluded if they had a history of HRW consumption or hydrogen inhalation, were diagnosed with true erythrocytosis, chronic lung disease, or organic sleep disorders, had severe hepatic or renal insufficiency, or were pregnant or breastfeeding women.
Randomization and masking
Eligible participants were randomly assigned to either the HRW or placebo group in a 1:1 ratio using a dynamic minimization method, stratified by gender, ethnicity, and CMS severity (mild, moderate, severe). The randomization scheme was prepared by an independent statistician not involved in patient care or data analysis using the R (4.1.3) procedure. Individual randomization codes were sealed in opaque envelopes and delivered to the study site. Blinding was ensured by supplying HRW and placebo in identical aluminum cans, matched for taste, color, shape, and packaging. Participants, health care providers, data collectors, outcomes assessors, and data analysts were masked to treatment assignments throughout the study. Only the independent statistician retained access to the randomization codes until the study database was locked.
Study termination criteria were defined a priori. Participants could be withdrawn if they experienced adverse events deemed severe or intolerable, if they relocated to low-altitude areas during the intervention period, or if adherence fell below protocol requirements. The trial itself would be terminated early if unexpected safety concerns emerged or if continuation was judged inappropriate by the Institutional Review Board.
Procedures
At the screening visit, all candidates underwent a complete blood count (CBC) test and an evaluation based on the Qinghai diagnostic criteria for CMS. A professional endocrinologist further assessed participants for suitability and eligibility. Eligible participants were subsequently randomized to receive either HRW or placebo. Study visits were conducted at baseline (week 0), 4 weeks, and 8 weeks. At each visit, participants underwent a physical examination, completed standardized questionnaires (Fatigue Scale-14 [FS-14], Pittsburgh Sleep Quality Index [PSQI], and 36-Item Short Form Survey [SF-36]), and provided urine and blood samples. Blood samples were analyzed for routine hematological parameters, biochemical indices, and oxidative stress markers.
Application of HRW and placebo
Participants assigned to the HRW group received aluminum-canned HRW, while those in the placebo group received identically packaged plain water matched for taste, color, and appearance. The administration protocol was based on previous preclinical and clinical studies demonstrating both safety and measurable biological effects with a daily hydrogen intake of ∼4–5 ppm (Russell et al., 2021). Accordingly, participants were instructed to consume three bottles daily (990 ml each; total daily hydrogen dose ∼4.84 ppm), and to finish each opened bottle within 1 hour to ensure hydrogen stability and bioavailability. The aluminum can packaging was chosen to minimize hydrogen loss and to maintain masking integrity, since placebo water was prepared and packaged identically. Both HRW and placebo were supplied by Weifang Jinfang Qiling Mineral Water Co., Ltd. No additional dietary or lifestyle restrictions were imposed during the intervention period. Empty bottles were collected at each visit to evaluate adherence (calculated as [recycled empty bottles/assigned bottles × 100%]).
CBC and biochemical blood tests
Following an overnight fasting, venous blood samples were collected from all participants between 08:00 and 10:00. Whole blood was drawn into ethylenediaminetetraacetic acid-coated tubes for CBC analysis and into serum-separating tubes for biochemical assays. All samples were processed within 30 minutes of collection. Serum was isolated by centrifugation at 3,000×g for 15 minutes at 4°C, aliquoted, and immediately stored at −80°C until further analysis. To ensure stability, all assays were performed according to the manufacturer’s instructions, and no samples underwent more than one freeze–thaw cycle.
Oxidative stress biomarkers
To evaluate the impact of HRW on oxidative stress in patients with CMS, we quantified a series of antioxidant and oxidative damage biomarkers, including CAT, GSH, MDA, SOD, 8-hydroxy-2′-deoxyguanosine (8-OHdG), and total antioxidant capacity (T-AOC). CAT activity (U/ml) was assessed using a commercial catalase assay kit (E-BC-K031-M, Elabscience, Houston, TX, USA) following the manufacturer’s instructions. GSH concentration was determined using a GSH colorimetric assay kit (E-BC-K030-M, Elabscience) according to the kit protocol. Lipid peroxidation was measured via the MDA content using a colorimetric assay kit (E-BC-K025-M, Elabscience), with absorbance recorded at 532 nm. SOD activity (μmol/L) was evaluated using a specific SOD activity assay kit (E-BC-K020-M, Elabscience) per the manufacturer’s guidelines, with absorbance read at 550 nm. 8-OHdG levels were determined (in ng/ml) using an Enzyme-Linked Immunosorbent Assay kit (E-EL-0028, Elabscience), and absorbance was measured at 450 nm using a microplate reader. T-AOC (U/ml) was quantified using a colorimetric assay kit (E-BC-K136-M, Elabscience), with one unit of antioxidant capacity defined as a 0.01 increase in absorbance per minute per milliliter of sample at 37°C.
Outcomes
The primary efficacy endpoint assessed the change from baseline to week-8 in oxidative stress biomarkers. These biomarkers represent well-established, widely utilized indices for evaluating systemic oxidative-antioxidant equilibrium and quantifying oxidative stress. Specifically, SOD, CAT, and GHS were selected as core components of endogenous antioxidant defense mechanisms; MDA and 8-OHdG served as established indicators of lipid peroxidation and DNA oxidative damage, respectively; and T-AOC provided a comprehensive assessment of cumulative antioxidant potential.
Secondary endpoints were changes from baseline to week 8 in routine blood test result, blood biochemistry, 36-item SF-36, FS-14, PSQI. Safety was assessed with documentation of adverse events collected at in-person and telephone visits, vital signs, and physical examination. Adverse events were graded as mild, moderate, or severe and judged for relatedness to the study intervention.
Statistical analysis
We calculated that a sample size of ∼58 participants per group would provide more than 90% power to detect a 0.89-point difference between either treatment group or placebo in mean change from baseline in MDA with an SD of 0.80, two-sided α of 0.05, and 20% dropout assumption. The 0.89-point difference was based on the previous performance of HRW in an 8-week study (0.79-point difference in MDA) and expectation that MDA would decline by about 0.1 point over 8 weeks in a population with untreated CMS (Kura et al., 2022).
Descriptive statistics was used to express quantitative data in the form of mean ± standard deviation and qualitative data in the form of [n (%)]. To test for normal distribution of continuous variables, we used the Shapiro–Wilk test. The Levene’s test was applied to evaluate the homoscedasticity of data.
The primary analysis was conducted following the modified intention-to-treat (mITT) principle. mITT was defined as participants who were randomly allocated and received at least one bottle of the intervention. Statistics were calculated using a restricted maximum likelihood mixed model for repeated measures analysis, with fixed effects for treatment group, time (0, 4, 8 weeks), and treatment by week interaction, and associated baseline values as covariate. Within-subject variability was modelled using an unstructured covariance matrix and denominator degrees of freedom calculated using the Kenward–Roger approximation. Secondary endpoints were treated as exploratory. The secondary endpoints, including routine blood test result, blood biochemistry, SF-36, FS-14, and PSQI, were analyzed using a mixed model for repeated measures. Results are presented as an adjusted treatment effect and the associated 95% CI.
Analyses of the primary endpoint were also conducted on per protocol and completer populations and prespecified subgroups (age, sex, ethnicity, BMI, and CMS criteria score). The per-protocol population was all mITT participants who had no major protocol deviations (adherence >85%) with respect to the primary outcome measure. Completers were all mITT participants who completed all protocol specified tests and observations and completed treatment as per the protocol. The safety analysis was conducted on all randomly allocated participants who received at least one bottle of the intervention.
For missing data, multiple imputation was employed using the chained equations method with random forest matching. The imputation model included baseline demographic variables (age, sex, ethnicity, BMI, and residence history), treatment assignment, baseline outcome values, and available repeated outcome measures (hematology, biochemistry, and oxidative stress biomarkers) to preserve associations between covariates and outcomes. Five complete datasets were generated and pooled using Rubin’s rules. Variables with more than 20% missingness were not included in the imputation model.
All statistical analyses were performed using Python 3.8.1, with the packages of “mice” for multiple imputation and “statsmodels” for mixed-effects model.
Results
This study was conducted from July 3, 2024, to December 24, 2024, at Tibetan Hospital of Nagqu. A total of 124 individuals were screened, of whom 64 were deemed ineligible. Sixty eligible participants were randomly allocated to study groups, with 30 people allocated per group (Fig. 1). One participant who was randomly assigned to placebo did not receive study treatment and was not included in the mITT analysis. Baseline characteristics were similar across groups (Table 1).
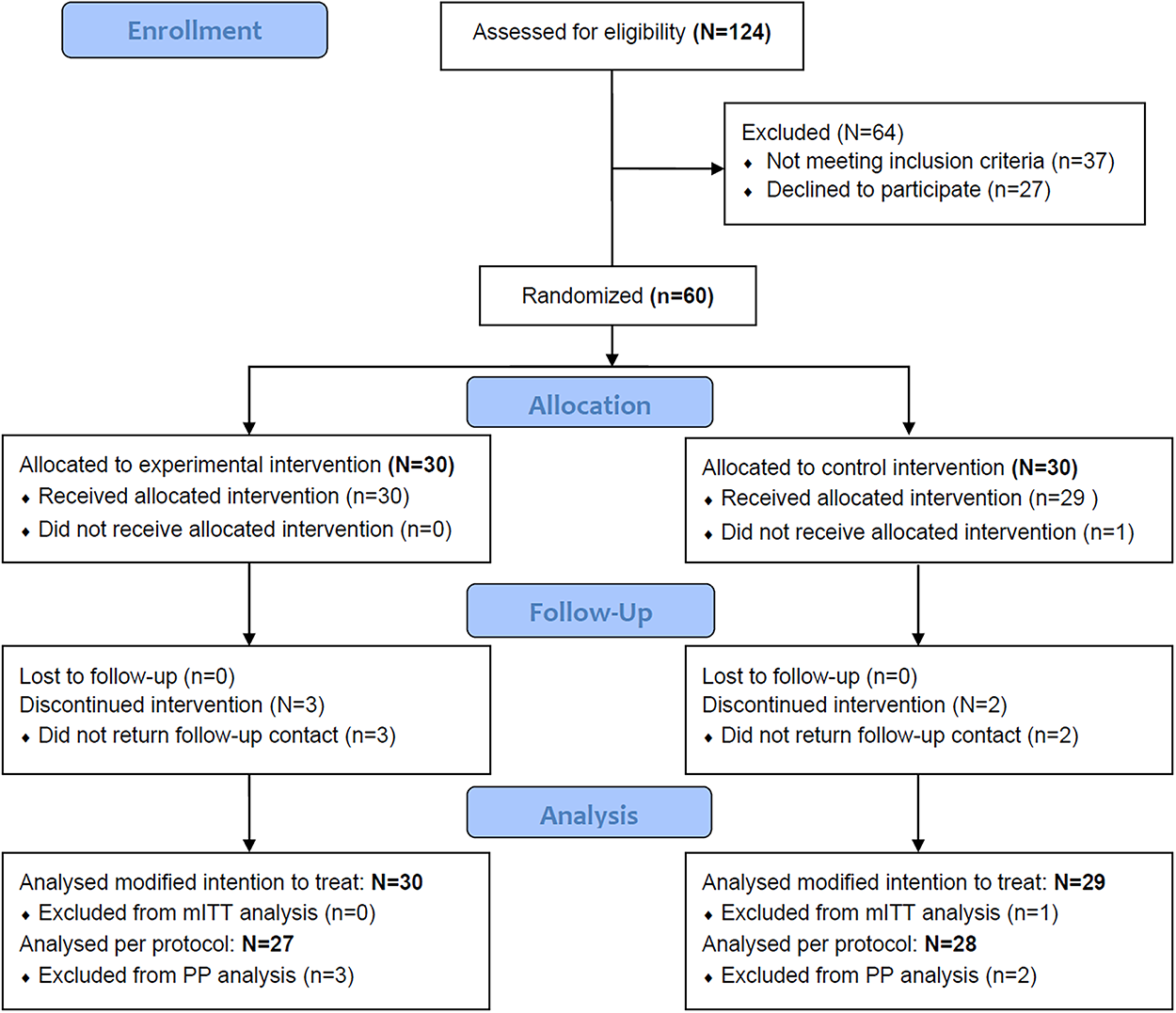
CONSORT flow diagram.
Demographics and Disease Characteristics at Baseline in the Modified Intention-to-Treat Population
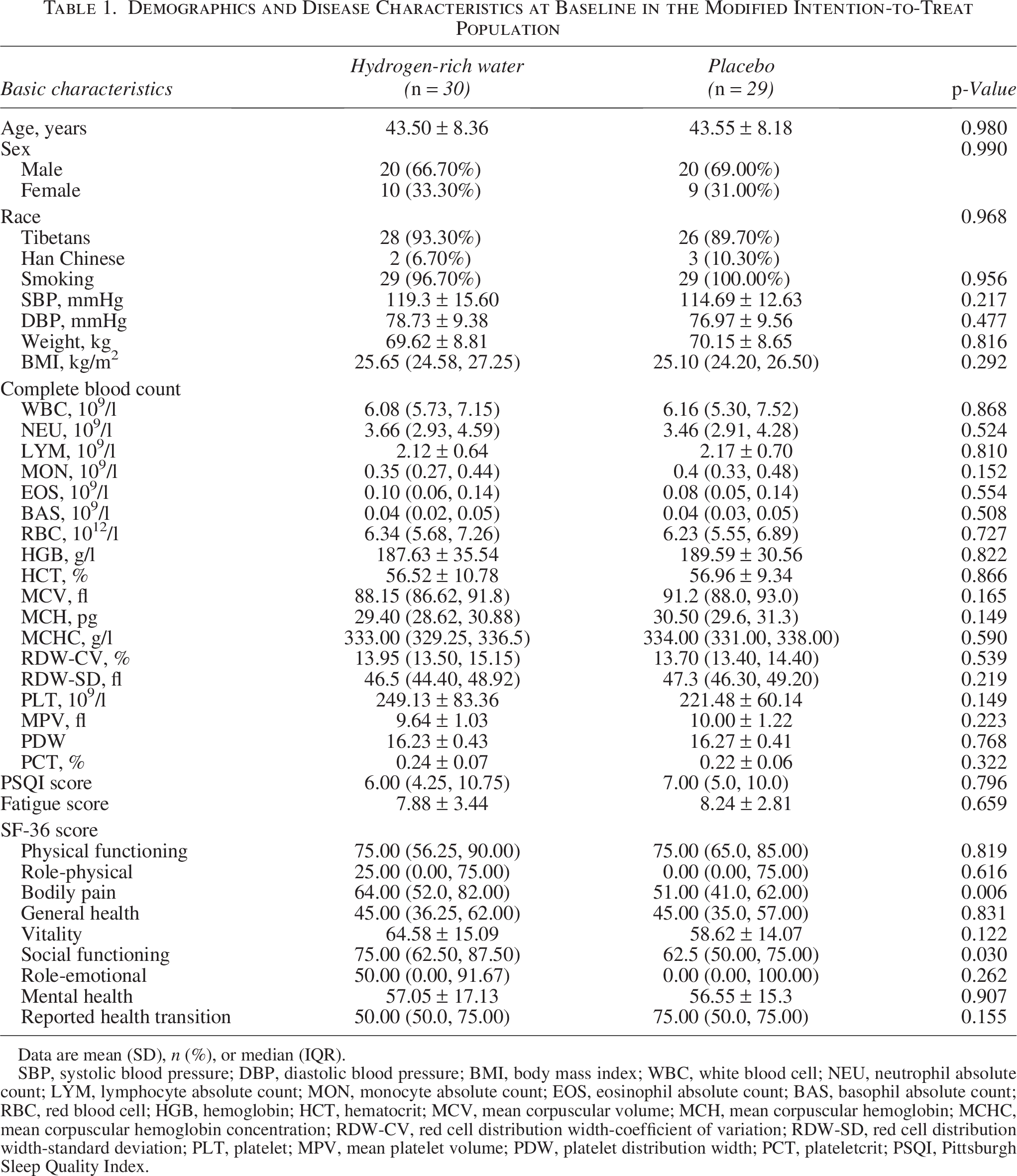
Data are mean (SD), n (%), or median (IQR).
SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; WBC, white blood cell; NEU, neutrophil absolute count; LYM, lymphocyte absolute count; MON, monocyte absolute count; EOS, eosinophil absolute count; BAS, basophil absolute count; RBC, red blood cell; HGB, hemoglobin; HCT, hematocrit; MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; RDW-CV, red cell distribution width-coefficient of variation; RDW-SD, red cell distribution width-standard deviation; PLT, platelet; MPV, mean platelet volume; PDW, platelet distribution width; PCT, plateletcrit; PSQI, Pittsburgh Sleep Quality Index.
Fifty-four (92%) participants completed the 8-week treatment period. Five (8%) people discontinued treatment (three in the HRW group and two in the placebo group). The most common reason for discontinuation was relocation from high to lower altitudes (one in the HRW group, and two in the placebo group). Compliance with study treatment, as determined by recycled empty bottles, was 90% for placebo and 85% for HRW group.
The primary endpoint demonstrated statistically significant in the T-AOC and MDA levels after 8-week HRW compared with placebo (Table 2, Fig. 2). The adjusted between-group differences at endpoint for MDA was 2.11 (95% CI: 1.13–3.09, p < 0.001), while for T-AOC it was 2.86 (95% CI: 0.09–5.64, p = 0.043). No significant intergroup differences were observed in CAT, GSH, SOD, and 8-OHdG. In both the per protocol and completers analysis, MDA levels remained significantly elevated, with an adjusted between-group difference of 1.38 (95% CI: 0.33–2.44, p = 0.01) and 1.81 (95% CI: 0.85–2.77, p < 0.001), respectively. No significant differences were detected for CAT, GSH, SOD, 8-OHdG, or T-AOC in either analysis (Supplementary Appendix A15).
Changes from Baseline in Primary and Secondary Outcome Measures at Week 8 in the mITT Population
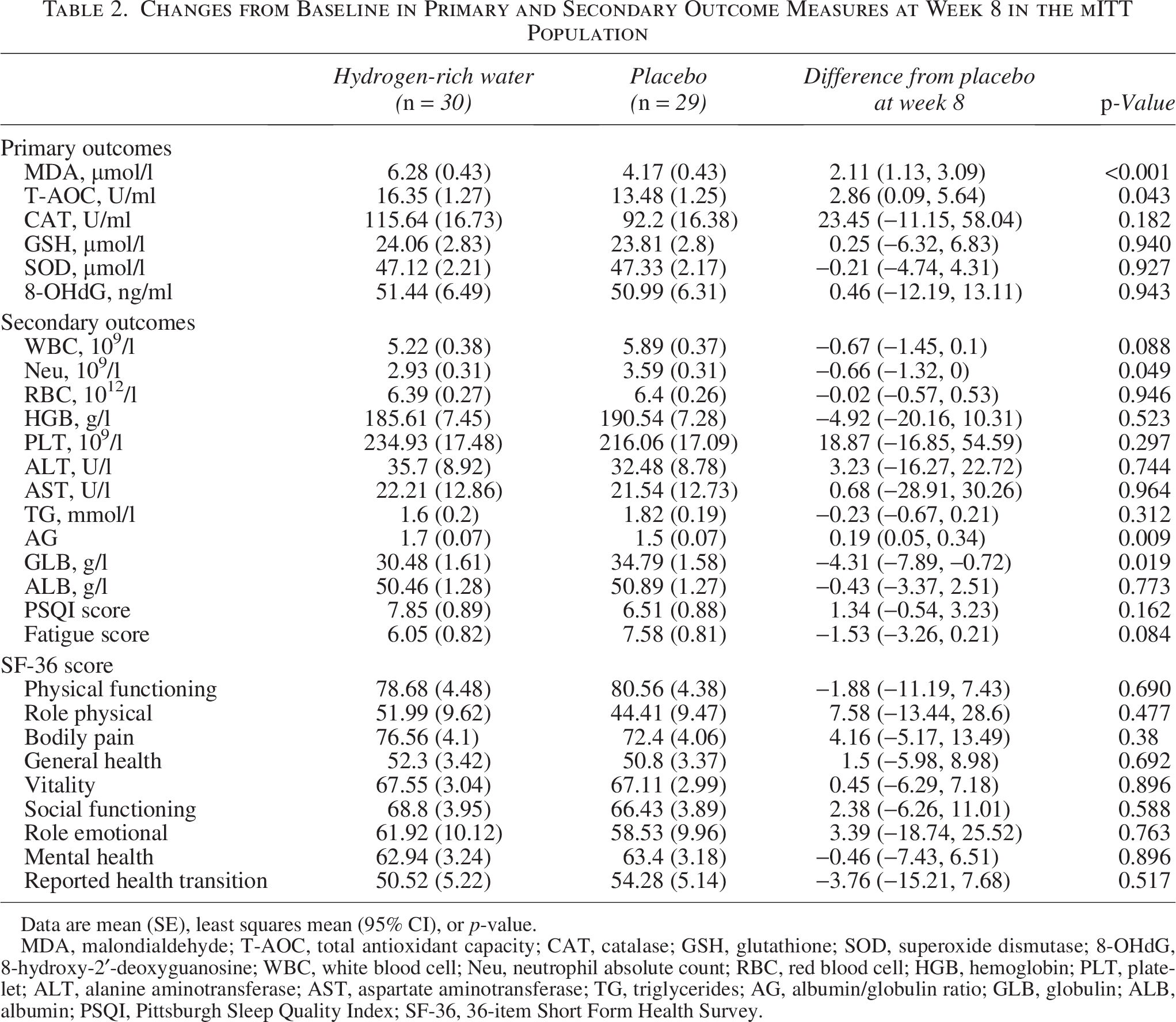
Data are mean (SE), least squares mean (95% CI), or p-value.
MDA, malondialdehyde; T-AOC, total antioxidant capacity; CAT, catalase; GSH, glutathione; SOD, superoxide dismutase; 8-OHdG, 8-hydroxy-2′-deoxyguanosine; WBC, white blood cell; Neu, neutrophil absolute count; RBC, red blood cell; HGB, hemoglobin; PLT, platelet; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TG, triglycerides; AG, albumin/globulin ratio; GLB, globulin; ALB, albumin; PSQI, Pittsburgh Sleep Quality Index; SF-36, 36-item Short Form Health Survey.
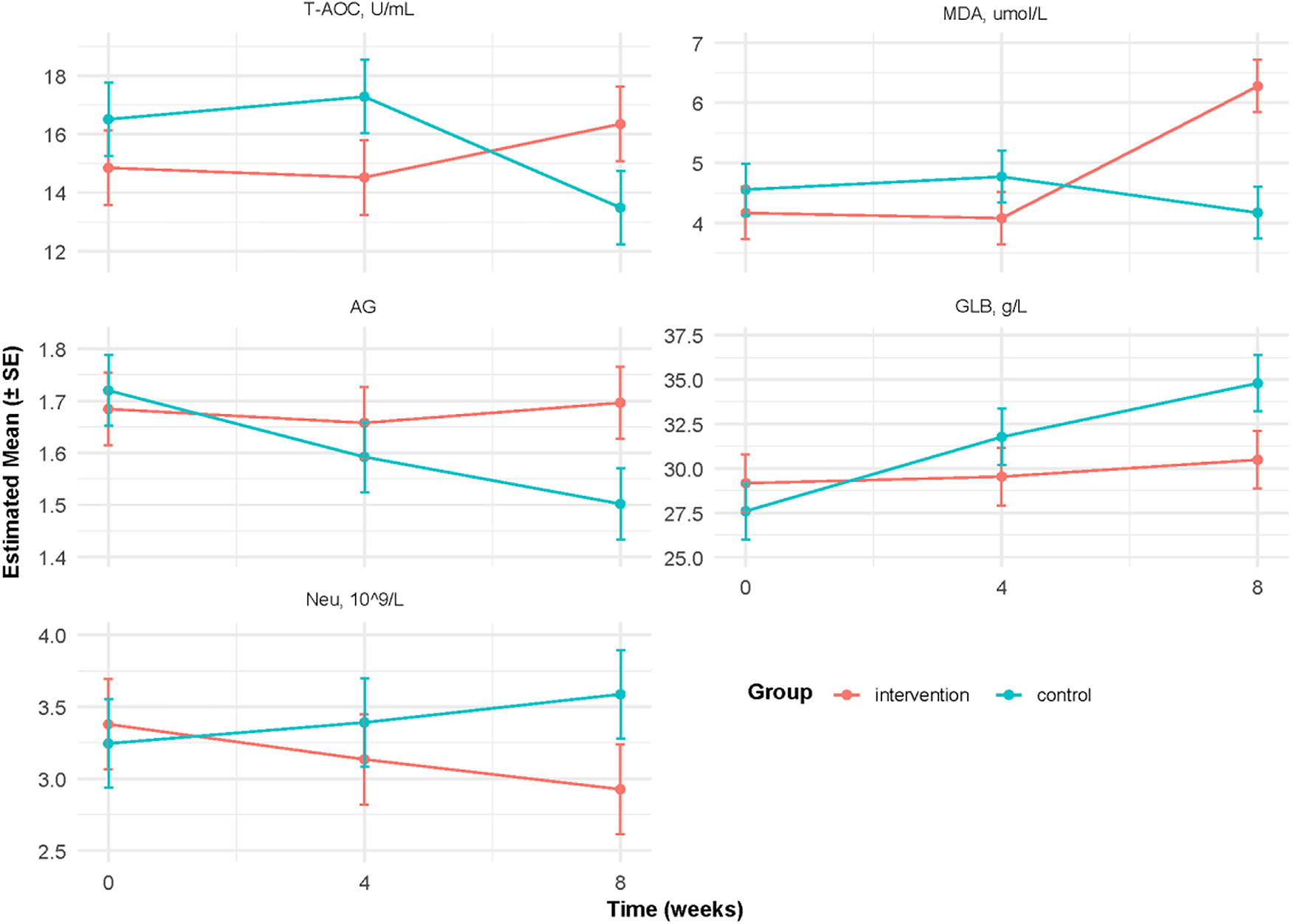
Changes from baseline in primary and secondary outcome measures during the treatment period in the mITT population. Primary and secondary outcome measures were assessed at week 8. Datapoints represent absolute mean changes; error bars represent standard errors. MDA, malondialdehyde; T-AOC, total antioxidant capacity; AG, albumin/globulin ratio; GLB, globulin; Neu, neutrophil absolute count.
Secondary outcome analysis revealed significant between-group differences in neutrophil count (Δ−0.66, 95% CI: −1.32–0.00, p = 0.049), anion gap (Δ + 0.19, 95% CI: 0.05–0.34, p = 0.009), and globulin (Δ−4.31, 95% CI: −7.89–0.72, p = 0.019) (Table 2). No statistically significant intergroup differences were observed in other hematological parameters, biochemical profiles, SF-36, FS-14, and PSQI scores (Table 2, Supplementary Appendix A16–A17).
The results regarding the MDA levels did not show significant heterogeneity in analyses of the 4 subgroups, with one exception (Fig. 3). The effect of HRW appeared to be enhanced in patients with a BMI ≥24 (Δ + 2.57, 95% CI: 1.51–3.64, p = 0.02 for the interaction).

Subgroup analysis of changes from baseline in MDA level by Gener, BMI, race, age, and CMS degree. CMS, chronic mountain sickness; BMI, body mass index.
HRW was generally well tolerated, with most adverse events being mild in severity (Table 3). The most frequently reported adverse events were dizziness and diaphoresis, with comparable incidence rates observed across both groups.
Treatment-Emergent Adverse Events
Discussion
In this blind, randomized, placebo-controlled trial, we evaluated the efficacy and safety of HRW in patients with CMS under high-altitude hypoxic conditions, revealing both pro-oxidative and antioxidative effects. Specifically, following 8-week intervention, HRW significantly increased plasma MDA levels (Δ2.11, 95% CI: 1.13–3.09, p < 0.001) and T-AOC levels (Δ2.86, 95% CI: 0.09–5.64, p = 0.043) compared with placebo. Notably, the elevation in MDA was more pronounced among participants with BMI ≥24 (Δ + 2.57; 95% CI: 1.51–3.64; p = 0.02 for interaction). HRW was generally safe and well tolerated.
Interestingly, despite the HRW intervention led to an increase in T-AOC, a paradoxical elevation in MDA, a well-established marker of lipid peroxidation, was also observed. Classical enzymatic antioxidants (including CAT, GSH, and SOD) as well as the DNA oxidative damage marker 8-OHdG, did not show significant changes. This pattern provides information in three aspects. First, contrary to conventional antioxidant expectations, the elevation in T-AOC may not reflect a comprehensive enhancement of the endogenous antioxidant defense system but rather a partial or compensatory increase in non-enzymatic antioxidant components. HRW may selectively enhance certain low-molecular-weight antioxidants (e.g., uric acid, ascorbic acid, or other redox-active metabolites), which contribute to the t-AOC measurement but do not strongly impact lipid peroxidation under sustained hypoxic conditions (Meng et al., 2025; Kawakami et al., 2022). Second, elevated levels of MDA indicate enhanced lipid peroxidation and suggest an increased burden of oxidative stress. HRW may paradoxically amplify lipid peroxidation through hypoxia-specific mechanisms, such as transient disruption of mitochondrial electron transport chain function (He et al., 2025). This effect could be further intensified by hydrogen’s interaction with redox-active metal ions (e.g., free Fe2+), potentially amplifying the generation of hydroxyl radicals (·OH) under hypoxic conditions (Murphy, 2009). Third, in the context of chronic hypoxia, where ROS generation is continuous and multifactorial, the upregulation of non-enzymatic antioxidant defenses may be inadequate to neutralize oxidative damage (Behn et al., 2007).
The coexistence of both pro-oxidant and antioxidant effects observed in our trial may therefore reflect context-dependent mechanisms unique to chronic hypoxia. On the one hand, HRW selectively scavenges highly ROS such as hydroxyl radicals and peroxynitrite, which may explain the modest increase in T-AOC. On the other hand, hydrogen may interact with hypoxia-driven alterations in mitochondrial electron transport or with redox-active metal ions, thereby facilitating secondary generation of reactive species and amplifying lipid peroxidation. Moreover, the discrepancy between T-AOC and MDA highlights the limitations of biomarker interpretation: T-AOC predominantly reflects non-enzymatic antioxidants and does not necessarily indicate reduced oxidative damage, whereas MDA specifically captures lipid peroxidation.
Beyond oxidative markers, several hematological and biochemical changes after HRW intervention may signify a multifaceted immunomodulatory response under chronic hypobaric hypoxia. The observed reduction in neutrophil counts—key effectors in oxidative and inflammatory pathways—suggests a potential anti-inflammatory action of HRW. This decrease may be attributed to suppression of pro-inflammatory signaling pathways, such as Nuclear Factor-Kappa B activation or NOD-Like Receptor Family Pyrin Domain Containing 3 inflammasome signaling, leading to diminished neutrophil recruitment and activation—a mechanism that aligns with previously reported anti-inflammatory effects of molecular hydrogen (Fu et al., 2022; Zhang et al., 2022; Ren et al., 2016). Concurrently, decreased serum globulin levels—potentially reflecting reduced immunoglobulin or acute-phase protein production—could compromise antioxidant buffering capacity, as globulins participate in free radical scavenging and metal ion chelation(Sitar et al., 2013; Gulhar et al., 2018). This may, in part, explain the paradox of increased T-AOC with persistent MDA elevation. Additionally, the observed increase in anion gap may signal a subclinical accumulation of unmeasured anions or organic acids, such as lactate, because altered mitochondrial function and incomplete oxidative metabolism under chronic hypoxic stress. These changes suggest that HRW may influence metabolic and inflammatory parameters without fully restoring oxidative balance.
Subgroup analysis highlights that individuals with BMI ≥24 exhibited disproportionately higher levels of MDA compared with those with lower BMI. This observation is biologically plausible, as adiposity is strongly linked to oxidative stress through multiple molecular pathways. Excess adipose tissue promotes chronic low-grade inflammation characterized by increased secretion of pro-inflammatory cytokines such as Tumor Necrosis Factor-alpha and IL-6, which stimulate ROS production and lipid peroxidation (Fernández-Sánchez et al., 2011). In parallel, adipose tissue expansion is associated with mitochondrial dysfunction and reduced efficiency of the electron transport chain, further increasing ROS leakage (Masschelin et al., 2020). Obesity is also known to impair the activity of key enzymatic antioxidants, including SOD and CAT, thereby weakening endogenous defenses against oxidative stress (Cecerska-Heryć et al., 2022). Moreover, adipocytes themselves can serve as both a source and target of ROS, amplifying redox imbalance and accelerating lipid peroxidation in cell membranes (Olivares-Vicente and Herranz-López, 2025). Sensitivity analyses, including per protocol and completers analysis, showed a significant increase in MDA, reinforcing the primary result that HRW did not mitigate oxidative lipid injury. Interestingly, in these restricted populations, the increase in T-AOC was no longer statistically significant, suggesting that the observed T-AOC increase in the m-ITT analysis may have been influenced by protocol deviations or attrition-related bias.
Moreover, adipocytes themselves can serve as both a source and target of ROS, amplifying redox imbalance and accelerating lipid peroxidation in cell membranes. These mechanisms collectively provide a rationale for why participants with higher BMI may be more vulnerable to the paradoxical pro-oxidant effects of HRW under hypoxic conditions. This highlights the importance of considering metabolic phenotype in the design and interpretation of antioxidant interventions in high-altitudes populations.
These findings collectively suggest that HRW exerts complex and context-specific effects under sustained hypoxia rather than functioning as a uniformly protective antioxidant. For future studies, more comprehensive redox profiling—including mitochondrial function, iron metabolism, and a broader panel of oxidative biomarkers—will be required to clarify the dual actions of HRW. Stratified analyses based on metabolic phenotype (e.g., BMI, adiposity, or baseline oxidative status) may also help identify subgroups most likely to benefit or experience paradoxical responses.
Our study has several limitations. First, although we aimed for inclusivity in recruitment, the study population was predominantly Tibetan, which limits the generalizability of our findings and our ability to assess potential ethnic variations in response to HRW. Future studies should include participants from different ethnic backgrounds and geographical regions as well as lowland residents, to determine whether the observed effects of HRW are consistent across genetic and environmental contexts. Second, lifestyle factors such as dietary intake, nutritional supplementation, physical activity, alcohol consumption, and smoking status—which may strongly influence oxidative stress levels—were not comprehensively measured or controlled in this study, introducing possible confounding. Future research should collect and adjust for these variables to reduce bias and enhance the reliability of observed effects. Finally, the biological mechanisms underlying the paradoxical increase in both T-AOC and MDA remain unclear. Further mechanistic studies and longer-term interventions are needed to explore HRW’s effects under varying physiological and environmental conditions—such as differences in oxygen levels, altitudes, and metabolic states—to elucidate its precise role in redox regulation and clinical outcomes.
Conclusions
In conclusion, HRW was generally safe and well tolerated, but demonstrated limited systemic antioxidant effects. Further mechanistic studies and longer-term interventions are needed to determine the reproducibility and clinical significance of these findings.
Footnotes
Acknowledgments
The authors thank all study participants, families, and health care providers, as well as the data collectors and outcomes assessors who contributed to this project.
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
This study was supported by a grant from the science and technology department of Tibet, “Unveiling and Commanding” project (No. XZ202303ZY0011G), and the Hospital of Chengdu Office of People’s Government of Xizang Autonomous Region project (No. 2023-YJ-5 and 2024-YJ-2).
Data Availability
Data will be made available upon request.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.