
Abstract
Barg, Taylor, Jaclyn Walker, Samara Levine, David Ryan Ormond, and James P Maloney. Altered Mental Status at High Altitude: Obstructive Hydrocephalus Mimicking High Altitude Cerebral Edema (HACE). High Alt Med Biol. 00:00–00, 2025.—A 29-year-old female presented to a Colorado emergency department with amnesia, headache, confusion, and dysarthria after rapidly ascending a 4,404 m (14,267 ft) peak. Head CT revealed cerebral edema and hydrocephalus. She was hypotensive and required vasopressors prior to evacuation to a lower-altitude intensive care unit and received initial treatment for high-altitude cerebral edema (HACE) with dexamethasone. Imaging and clinical workup revealed obstructive hydrocephalus due to a colloid cyst with minimal radiographical evidence of cerebral edema except due to the compressive effects of hydrocephalus. She transiently developed stress-induced cardiomyopathy and mixed neurocardiogenic shock. This case emphasizes the importance of considering HACE mimics at high altitude triggered by hypoxia-mediated increases in intracranial pressure.
Keywords
Introduction
High-altitude exposure causes a range of hypoxia-induced pathologies. Acute mountain sickness (AMS) typically manifests within 6–12 hours of ascent to moderate (>8,000 ft, 2,438 m) and higher altitudes with nonspecific symptoms such as headache, malaise, fatigue, dizziness, insomnia, nausea, and anorexia (Luks et al., 2017). AMS can progress to severe syndromes, including high-altitude cerebral edema (HACE), a rare but potentially fatal condition. HACE typically affects individuals who rapidly ascend to elevations above 3,000 m (Hackett et al., 1998), with an incidence of 0.5%–1% at elevations above 4,000 m (Luks et al., 2017). Rapid descent, oxygen, and corticosteroids are critical for HACE recovery. HACE symptoms include confusion, headaches, lassitude, and ataxia. Given the risk for rapid decompensation, clinicians must recognize both risk factors for HACE and alternative diagnoses that can mimic its presentation to ensure timely and appropriate treatment (Buttner et al., 1997).
Hypoxia increases intracranial pressure (ICP) through cerebral vasodilation and vasogenic edema, placing individuals with preexisting intracranial abnormalities at risk. Patients with intracranial masses or hydrocephalus are particularly vulnerable—even minor increases in ICP can cause deterioration, as they are living near the limits of neurovascular autoregulation. Neurological decline at altitude has been reported with chronic hydrocephalus even during intermediate altitudes of commercial aircraft flight (Kutty et al., 2020; Nelson and Haymaker, 1957).
Colloid cysts are benign epithelial-lined lesions typically located in the third ventricle at the foramen of Monro, comprising ∼2% of primary brain tumors. Though colloid cysts are often asymptomatic, they may intermittently obstruct cerebrospinal fluid (CSF) flow, causing hydrocephalus and sudden neurological symptoms (Lawley et al., 2016). Obstruction may follow any situation that increases ICP. Environmental triggers like altitude and air travel have been associated with symptom onset (Kutty et al., 2020). While deaths linked to asymptomatic colloid cyst-related hydrocephalus during commercial and military air travel are documented (Nelson and Haymaker, 1957), there are no known published reports of hydrocephalus due to colloid cysts mimicking HACE during a mountain ascent.
We present a case of a young woman who was initially diagnosed with HACE after developing acute neurological symptoms at high altitude. However, she was found to have obstructive hydrocephalus from a colloid cyst. This case underscores the importance of maintaining a broad differential diagnosis when evaluating altered mental status at high altitudes.
Case Presentation
A 29-year-old woman presented to a rural emergency department in the Colorado Rocky Mountains at 1,780 m after rapidly ascending Castle Peak (4,349 m) and developing confusion, dysarthria, headache, nausea, and vomiting. She lived at 1,707 m and had camped overnight at 2,438 m before her first-ever >4,000 m summit. She and her companion left camp and summited in 7 hours, after which she described feeling “drunk.” After descending to 2,438 m, she briefly napped and awoke confused with slurred speech and headache and vomited. She had no prior medical history and denied alcohol or drug use. Her symptoms had not resolved upon descent to the emergency department.
On exam, her blood pressure was 85/61 mmHg, heart rate 100 bpm, and respiratory rate 26. She was afebrile with an SpO2 of 99% on room air. Neurological examination showed dysarthria and mild confusion without visual field deficits, papilledema, cranial nerve palsies, or focal deficits. Initial labs showed a white blood cell (WBC) count of 20,300 cells/ul, an elevated anion gap, but otherwise unremarkable findings on chemistries, urine drug screen, serum pregnancy test, urinalysis, chest radiograph, and respiratory viral panel. She received norepinephrine via a central line due to progressive hypotension and was started on intravenous (IV) antibiotics for possible sepsis.
A CT scan of the head (Fig. 1) demonstrated dilated lateral ventricles and suspected cortical edema with an Evans index of 0.35, including enlargement of the normal slit-like temporal horns (the Evans index is defined as the ratio of the maximal width of the frontal horns to the maximum inner parietal zone skull diameter; the normal value is ≤0.25). A lumbar puncture after the CT scan (hydrocephalus was not initially appreciated) revealed WBC of 11 cells/ul, red blood cells of 8,650 cells/ul without xanthochromia, and normal protein. CSF PCR studies for common viral and bacterial pathogens were later negative. Opening pressure was not recorded. In the case of high RBC counts and/or xanthochromia, the differentiation between subarachnoid hemorrhage and traumatic LP is still not reliable (Zinganell et al., 2023); a consulting neurologist recommended brain magnetic resonance imaging/arteriography (MRI/MRA). However, given that this evaluation occurred at a rural hospital in a high-altitude environment, where HACE is considered a high-priority, “do-not-miss” diagnoses, this context likely influenced the clinical decision-making at the time to consider HACE. Although the CT showed hydrocephalus (diagnosis only made by a delayed radiologist interpretation), motion artifact and apparent sulcal effacement were interpreted as consistent with cerebral edema, prompting empirical treatment for HACE with IV dexamethasone and immediate transfer to a tertiary care center at a lower altitude.
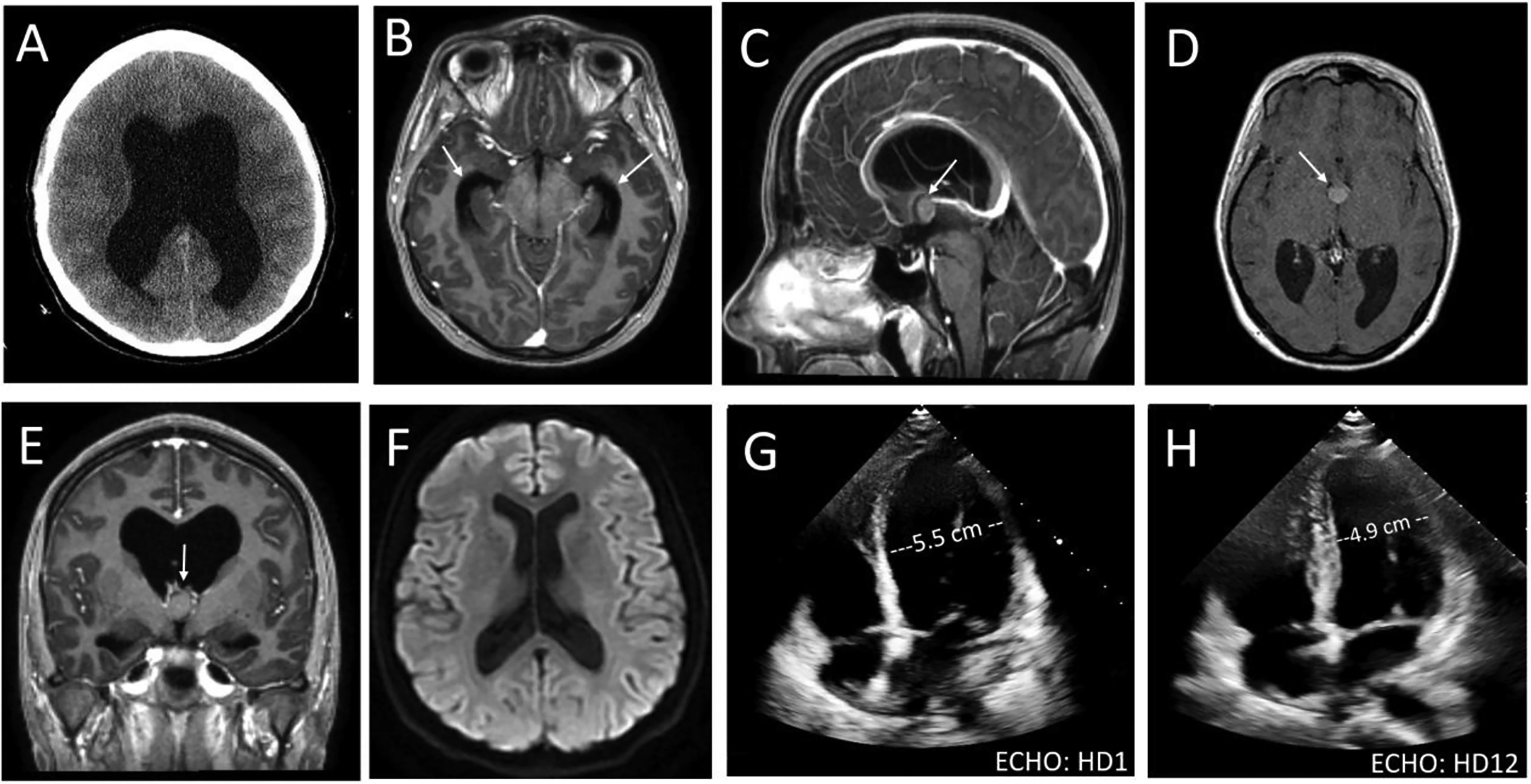
On arrival at the University of Colorado Hospital in Denver, a repeat head CT (Fig. 1) showed obstructive hydrocephalus and a 1.3 cm colloid cyst at the Foramen of Monro. A subsequent MRI/MRA confirmed this diagnosis (Fig. 1). Dexamethasone was continued, IV fluids were stopped, and the head of the patient’s bed was elevated. Serial EKG and telemetry demonstrated diffuse T-wave inversions but no arrhythmias. Further evaluation for the etiology of shock included a transthoracic echocardiogram (TTE), which was notable for a reduced left ventricular ejection fraction of 35% with mid-left ventricular hypokinesis and dilation with apical sparing (Fig. 1), consistent with stress cardiomyopathy. Troponin and brain natriuretic peptide were elevated. Cardiology was consulted and recommended coronary CT angiography; however, given her youth, the patient and her family decided to forgo further cardiac testing. Cardiology attributed stress cardiomyopathy due to a neurogenic cause, namely the increased ICP and resulting hydrocephalus. Due to agitation, she was transferred to neurosurgery and had an extra-ventricular drain (EVD) placed in the right frontal horn on hospital day 2 (HD2). Her initial ICP was 18 cm H20. Agitation resolved, and the neurological exam thereafter was abnormal only for slowly improving hypoactive delirium. The repeat TTE on HD3 was unchanged. Oral captopril and metoprolol were started after vasopressors were stopped on HD5. On HD5, she underwent a right frontal endoscopic resection of the cyst. Pathology confirmed a colloid cyst. Norepinephrine was weaned off, and hypoactive delirium resolved on HD 12. On HD 12 the EVD was clamped, and a repeat TTE showed full resolution of the stress cardiomyopathy (Fig. 1). The patient was discharged on HD 15 with goal-directed medical therapy for stress-induced cardiomyopathy and levetiracetam for seizure prophylaxis. Imaging at 5 months showed resolved cortical compression and hydrocephalus (Fig. 1). She returned to work with mild short-term memory deficits that later resolved. She provided written consent for publication of her case, which was IRB-approved.
Discussion
With growing participation in high-altitude activities, understanding serious complications like HACE is vital. This case demonstrates how typical and atypical symptoms of HACE can be mimicked by other pathologies. Although the patient’s rapid ascent and neurological symptoms suggested HACE, imaging revealed obstructive hydrocephalus, and atypical symptoms such as slurred speech could be a sign of alternative diagnoses (Table 1). HACE pathophysiology involves vasodilation, increased cerebral blood flow, and vasogenic edema. The “tight fit hypothesis” suggests that individuals with limited intracranial compliance are more susceptible to developing cerebral edema (Gareth et al., 2008). In patients with preexisting lesions, like a colloid cyst, altitude-related hypoxia can increase ICP and worsen obstruction. Our patient likely had chronic partial obstruction that became acutely worse when increased ICP from hypoxia further restricted CSF flow. Similar episodes have been reported in patients with colloid cysts triggered by air travel or other minor fluctuations in ICP (Kutty et al., 2020; Gareth et al., 2008). Our patient did not have hallucinations or psychotic features, which may occur in more extreme environments (Hüfner et al., 2023).
Differential Diagnosis for Altered Mental Status at High-Altitude and Atypical Symptoms and Signs of HACE
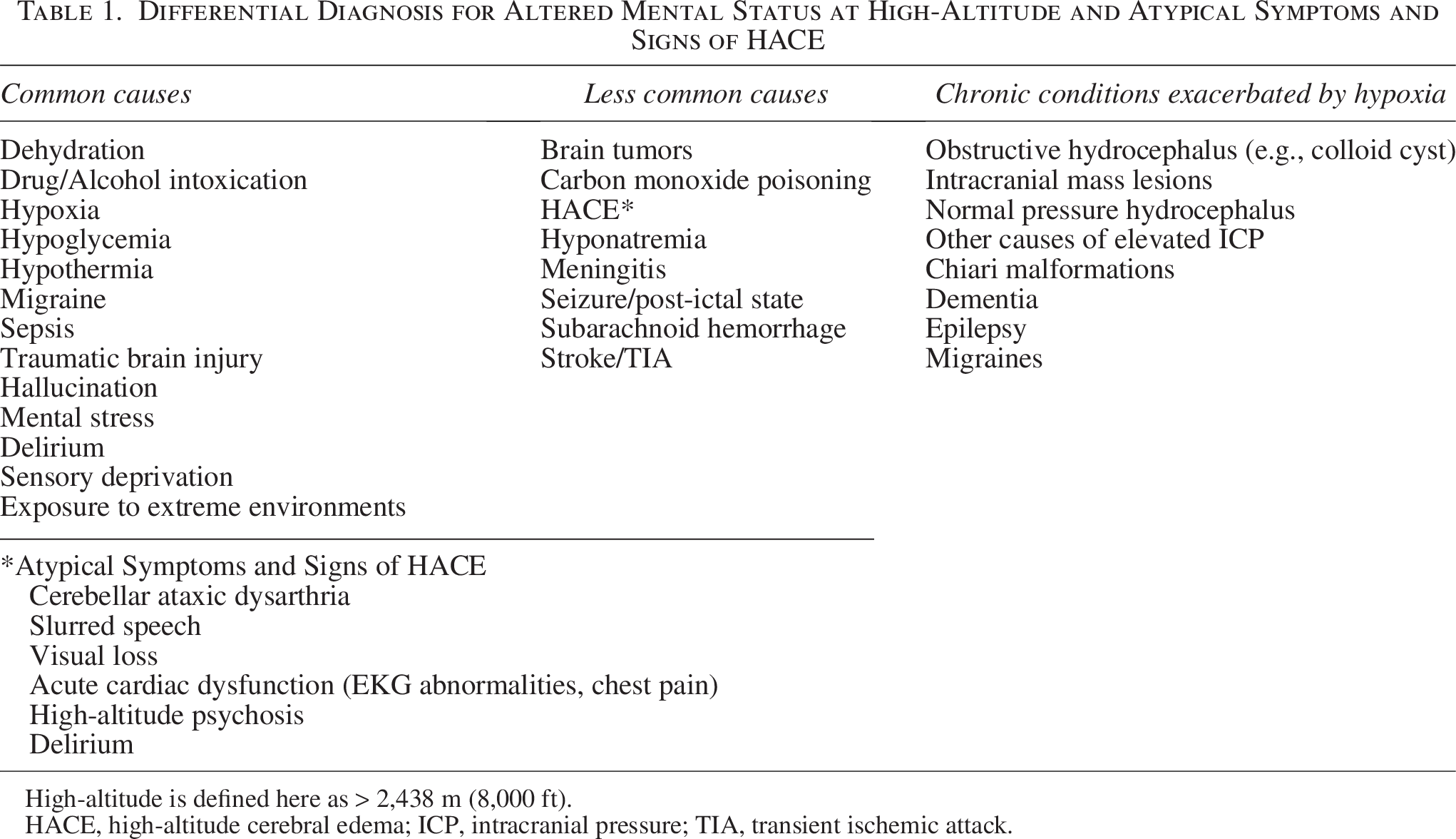
High-altitude is defined here as > 2,438 m (8,000 ft).
HACE, high-altitude cerebral edema; ICP, intracranial pressure; TIA, transient ischemic attack.
The patient also developed stress cardiomyopathy, likely precipitated by elevated ICP. Multiple studies have documented Takotsubo-like cardiomyopathy because of neurological insults like subarachnoid hemorrhage, traumatic brain injury, and even seizures (Finsterer and Wahbi, 2014; Cheah et al., 2017; Pelliccia et al., 2017). Clinically, this case emphasizes the importance of a broad differential diagnosis for altered mental status at altitudes (Table 1). Brain CT scanning, while readily available in most alpine resort areas, can be problematic in suspected HACE as this imaging technique lacks high sensitivity for the early stages of brain edema and may miss subtle findings (Luks et al., 2019); MRI is more sensitive for detecting the white matter changes characteristic of HACE, though it is less accessible in alpine or rural emergency care settings and should not delay descent or definitive care (Hackett et al., 1998). Hydrocephalus is not typical of HACE; thus, when identified, it should drive consideration of alternative diagnoses. Prompt imaging, descent, and initiation of appropriate therapy, including surgical intervention for hydrocephalus, is essential.
Conclusions
Clinicians should consider HACE mimics in patients with severe neurological symptoms at altitude. Obstructive hydrocephalus can present similar to HACE due to rapid elevations in ICP due to hypoxia. Early brain imaging is essential to differentiate HACE from such alternative diagnoses. The finding of hydrocephalus suggests HACE is unlikely and should trigger transfer to a lower-altitude facility with neurosurgery support.
Authors’ Contributions
T.B.: Data curation, validation, visualization, writing—review and editing (lead); J.W.: Conceptualization, data curation, validation, writing—original draft, review and editing; S.L.: Conceptualization, data validation, writing—review and editing; D.R.O.: Data curation, resources, writing—review and editing; J.P.M.: Supervision, data curation, validation, visualization, and writing—review and editing.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.