
Abstract
Du, Tianjing, Haoqing Shi, Linlin Liu, and Zeyu Yang. The mediating role of cognitive function in the relationship between acute high-altitude stress and casualty care capability following rapid ascent. High Alt Med Biol. 00:00–00, 2026.
Background:
The impact of high-altitude rescue missions on medical personnel’s cognitive function and casualty care capabilities remains unclear.
Methods:
This multicenter, randomized, sham-controlled clinical trial established high-altitude intervention (HAI), high-altitude (HA), and sea level (SL) groups (n = 92 per group). The HAI group received an integrated cognitive-stress management training, and the HA group implemented a sham training regimen before rapid ascent to high altitude (RAHA). The SL group served as a blank control group. Primary outcomes included casualty care capability score, plasma cortisol level, and cognitive ability score. Longitudinal mediation analysis examined the role of cognitive function in stress and casualty care capabilities.
Results:
In the HA group, cognitive ability mediated strong negative indirect effects at 24 hours, alongside a positive direct effect of stress. At 48 hours, the negative indirect effect remained dominant, whereas the direct effect of stress was not significant. At 72 hours, the indirect effect weakened but remained significant, whereas the direct effect of stress became significantly negative. By 96 hours, the indirect effect disappeared, with the total effect explained by stress. In the HAI group, the total and indirect effects were significant at 24 and 48 hours, whereas the direct effects were not. At 72 and 96 hours, no effects were statistically significant.
Conclusion:
During the initial phase of RAHA, cognitive ability serves as a mediating factor through which stress impairs casualty care capabilities. Over time, the mediating effect of cognition gradually diminishes, while the direct negative impact of the stress response continues to strengthen. The integrated cognitive-stress training can effectively preserve cognitive function and mitigate the stress response, thereby enhancing medical personnel’s casualty care capabilities.
Introduction
Rapid ascent to high altitude (RAHA), defined as the swift movement of individuals from plains to regions >3,000 m (Pun, 2021; Burtscher et al., 2025), triggers psychological, physiological, cognitive, and behavioral alterations (Santangelo et al., 2024; Yu et al., 2016; Xu et al., 2025). During critical RAHA missions, a high-altitude environment may induce various stress-induced psychosomatic reactions characterized by diminished positive emotions and cognitive biases, along with enhanced negative emotions and cognitive bias indicators, thereby impairing individual capabilities (Schnaubelt et al., 2025; Beer et al., 2024; Muralt et al., 2025).
China’s high-altitude regions cover ∼26.8% of its total land area, with a resident population of >60 million living at >3,000 m. Additionally, a substantial number of plain-dwelling civilians engage in commercial and travel activities in these areas annually, whereas military personnel conduct operations. Natural disasters and localized military conflicts impart nationwide scope, urgency, mass casualty influx, and high severity to medical rescue operations in high-altitude regions. These features constrain and threaten the effective functioning of the local healthcare systems.
In military medicine, current research on cognitive function changes following RAHA focuses on new recruits or stationed military personnel (Muza, 2007; Luo et al., 2013). However, the patterns of change in cognitive function and casualty care capabilities among medical personnel during emergency RAHA rescue missions remain unclear. Particularly, systematic research on stress responses, cognitive function, and care capability dynamics of medical personnel undertaking RAHA missions is lacking. The harsh environmental conditions and scarce medical resources in high-altitude regions indicate that sudden events causing mass casualties, trauma, infectious disease outbreaks, or psychological illnesses would urgently require emergency support from plain-based medical teams. Therefore, the underlying mechanisms through which high-altitude, cold, and hypoxic environments affect the psychology, physiology, cognition, and behavior of health care personnel must be investigated. Moreover, the current early warning and regulation systems for stress among RAHA medical staff remain underdeveloped. Building upon a comprehensive understanding of the characteristics of stress responses, cognitive function, and casualty care capabilities, there is an urgent need to establish scientific, effective, and practical early warning indicator systems and intervention protocols. This would facilitate precise psychological support for personnel experiencing psychological crises and enhance their overall medical support capacity in extreme environments, thereby effectively reducing noncombat attrition and avoiding unnecessary losses of personnel and material resources.
Therefore, this study focused on medical personnel undergoing RAHA to comprehensively understand the impact of high-altitude stress on their cognitive function and casualty care capability. These findings provide a theoretical foundation to enhance these aspects and bolster the medical support capacity for RAHA operations.
Methods
Study population
This multicenter, randomized, sham-controlled clinical trial was conducted from February 1, 2023 to February 1, 2025 across three hospitals in China. The study protocol was approved by the Medical Ethics Committee of the General Hospital of Xinjiang Military Command (2023RR0130). All participants provided written informed consent before enrollment. We adhered to the Consolidated Standards of Reporting Trials guidelines.
This study employed purposive sampling to recruit physicians from three hospitals in China. Inclusion criteria were: (1) aged between 22 and 50 years; (2) absence of organic diseases in the circulatory, respiratory, urinary, or other systems; (3) permanent residency at or below 1,000 meters above sea level and first-time ascent to high altitudes; and (4) engagement in frontline clinical work for over 3 years. Exclusion criteria were: (1) inability to provide informed consent; (2) poor compliance and cooperation, displaying negative or resistant attitudes towards the study; and (3) inability to complete all tests.
Sample size calculation
Data analysis was performed using linear mixed-effects models. To estimate the sample size, a preliminary pilot experiment (n = 30) was first conducted. Based on the pilot data, a simulation-based power analysis was performed using the powerlmm package in R software (version 4.5.1). Model parameters were set as follows: significance level (α) at 0.025 and statistical power (1 − β) at 0.9. Analysis of the pilot data indicated an intraclass correlation coefficient of ∼0.52 for the primary outcome measures. The target effect size was set as a medium partial η2 = 0.06. With 3 groups and 5 measurement time points, the required sample size to detect a group × time interaction effect was 44 participants per group. To account for the burden of post hoc pairwise comparisons and an anticipated attrition rate of ∼15%, the sample size was appropriately increased to at least 56 participants per group. This study ultimately enrolled 92 participants per group.
Allocation and blinding
A central randomization system was used for participant allocation. An independent statistician, not involved in trial implementation, generated the random sequence using R software, setting a block length of 6 and allocating participants at a 1:1:1 ratio to the high-altitude (HA), high-altitude intervention (HAI), and sea level (SL) groups. After importing the random sequence into the central randomization system, investigators obtained participant group assignments through this system. The system incorporated stratification factors, with independent random blocks allocated to each center to ensure balanced baseline characteristics across groups. The allocation sequence was strictly confidential and stored under seal in the document management department.
This study employed a double-blind design. The intervention group used blue tablet devices preloaded with cognitive training programs, while the control group used red tablet devices preloaded with documentary viewing programs. All tablet devices had brand identifiers removed, maintained identical external appearances, and underwent customized system processing where all functions, except the program icons, were disabled. Participants were informed that the study aimed to compare two different high-altitude adaptation training methods, and all training instructions were standardized. Training venues were managed in separate zones: Zone A for blue device training and Zone B for red device training, with the two areas physically isolated. Training schedules were staggered, with the intervention group training in the morning and the control group in the afternoon.
Assessors were independent of the training implementation team and conducted their work in dedicated assessment areas. The assessment system displayed no group information, and assessors were strictly prohibited from communicating with trainers about participant details. A three-tier unblinding mechanism was established for emergencies: Individual unblinding was achieved via emergency letters stored in the central pharmacy; group unblinding was managed by the statistician holding the group code correspondence table; and complete unblinding was managed by the hospital safeguarding the master random sequence list. Unblinding occurred only in cases of serious adverse events requiring specific treatment, participant withdrawal from the study necessitating knowledge of the received treatment, and at study conclusion. All unblinding operations required documentation of the reason, time, and personnel involved and had to be reported to the ethics committee within 24 hours.
Device management was handled by dedicated personnel. All tablets were managed uniformly, assigned daily before training based on random IDs, and collected immediately after training with usage records cleared. Program integrity was checked weekly. All research staff signed confidentiality agreements and received regular training on maintaining blinding. A blinding violation reporting system was established, with monthly assessments of blinding effectiveness. Monitors regularly inspected blinding implementation, recording all potential unblinding events. At study conclusion, blinding effectiveness was assessed via questionnaires; participants and researchers separately completed questionnaires guessing the training type, and blinding success was evaluated by analyzing the difference between the correct guess rate and random chance.
Intervention measures
The SL group served as a blank control group, receiving no intervention and not entering the high-altitude environment.
The HAI group commenced daily training 7 days before entering the 3,500 m high-altitude area, concluding training 1 day before arrival. They entered the high altitude immediately after completing the 7-day training. Training occurred in soundproof rooms with ambient temperature maintained at 22 ± 2°C and illumination controlled between 300 and 500 lux. Uniform tablet models and noise-cancelling headphones were used, all calibrated to ensure a stable volume of 75 dB. The HAI group received a 3-day integrated cognitive-stress management training, comprising two daily modules: a computerized cognitive training module and a stress management training module. The computerized cognitive training module lasted 23 minutes and included three tasks: A dual N-back task required simultaneous memorization of visual positions (blue square changes in a 3 × 3 grid) and auditory letter sequences (letters A–K played via headphones), with difficulty adjusting dynamically based on performance (starting at 1-back, increasing after 3 consecutive correct responses, decreasing after 2 consecutive errors), lasting 10 minutes (Salminen et al., 2016; Soveri et al., 2017). A task-switching training required switching between judging digit magnitude or parity based on green or blue background cues, with stimuli presented for 1500 ms and a 2000 ms response window, totaling 120 trials (40% requiring rule switches), lasting 7 minutes. An Attention allocation training required simultaneous processing of central letter identification and peripheral target counting tasks, with stimuli lasting 500 ms and intervals of 1000 ms, comprising 70% single-task and 30% dual-task trials, lasting 6 minutes. The stress management training module lasted 15 minutes using audio-guided instructions. Diaphragmatic breathing training (Ma et al., 2017; Yadav et al., 2021) followed a 4-second inhalation, 2-second breath-hold, 6-second exhalation rhythm with alpha wave–inducing music background, lasting 5 minutes. Mindfulness meditation (Tang et al., 2015; Prakash, 2021; Zollars et al., 2019) involved body scan exercises focusing on breath awareness and somatic sensation awareness, lasting 5 minutes. Progressive muscle relaxation followed a sequence (right hand, right forearm, right upper arm, left upper limb, face, neck, shoulders, chest, abdomen, right lower limb, left lower limb) using 5-second tension, followed by 15-second relaxation cycles, lasting 5 minutes. All relaxation training was conducted in a semirecumbent position with room lighting dimmed to 100 lux.
The HA group implemented a sham training regimen, commencing daily training 3 days before entering the 3,500 m. high-altitude area and concluding training 1 day before arrival. They entered the high altitude immediately after completing the sham training. In the same environment and using identical devices, they watched documentaries for 30 minutes daily (video resolution 1080p, refresh rate 60 Hz), followed by completing 5 multiple-choice questions (four options each) based on the video content. A dedicated software interface displayed only completion status without providing correctness feedback.
Observation indicators
All three groups of participants were measured at five time points (preascent baseline, 24 hours, 48 hours, 72 hours, and 96 hours postascent) across multiple dimensions. Primary observation indicators included the casualty care capability score, plasma cortisol level, and cognitive function score. Secondary observation indicators included the two-back task accuracy rate, malondialdehyde (MDA) level, and norepinephrine (NE) level.
Blood sample collection and processing
All blood samples were collected in the morning at 6:30 under fasting conditions. A volume of 3 ml was drawn for each test item. Samples were immediately labeled with the time and stored in a 4°C icebox. All samples were centrifuged at 4°C and 1000g for 15 minutes within 30 minutes postcollection. After centrifugation, the upper serum or plasma was immediately aliquoted into 2 ml cryovials (0.5 ml per tube), avoiding repeated freeze-thaw cycles. Samples were rapidly transferred to a −80°C ultra-low temperature freezer for storage until batch testing. All blood collection tubes were from the same brand and batch. Centrifuges were calibrated weekly. Sample testing was completed using the same equipment in the same laboratory. Plasma cortisol concentration was measured using electrochemiluminescence. MDA was measured using the thiobarbituric acid method. NE concentration was determined using high-performance liquid chromatography with electrochemical detection.
Casualty care capability scores
Casualty care capability was assessed from three aspects, each scored out of 100 points: basic and advanced life support operations, case analysis, and basic knowledge assessment. The assessment of basic and advanced life support operations was conducted using a standardized scoring scale developed based on the 2021 European Resuscitation Council Guidelines (Olasveengen et al., 2021; Soar et al., 2021). This scale defines the specific steps, quality standards, and mark deduction criteria for each procedure. All skill-based assessments were performed via direct observation. Participants completed assigned tasks in simulated scenarios, and three uniformly trained examiners used the aforementioned scale to provide independent, real-time, and simultaneous scoring. The final score was calculated as the average of the three examiners’ ratings to ensure objectivity. All examiners were medical professionals who had been permanently stationed at high altitude and were fully acclimatized. They did not participate in the RAHA process of this study. Therefore, their physiological and cognitive states remained stable, and their scoring ability was not affected by acute high-altitude reactions, thereby ensuring the reliability of the assessment results. Prior to the study, all examiners received uniform training on the use of the scoring scale and passed a preassessment calibration exercise using simulated cases to ensure interrater reliability. The case analysis component was scored based on the written management plans submitted by the participants, while the theoretical knowledge component was assessed via a written examination.
Cognitive function assessment
To quantify overall cognitive function changes, a composite score was calculated for this study based on task completion outcomes from the Cogstate computerized battery (Lupu et al., 2022; Kuiper et al., 2017). First, using the initial test data (conducted 3 months before training began) as the baseline, individual indicators were standardized into unidirectional Z-scores. Subsequently, their arithmetic mean was calculated as the comprehensive Z-score, which was then converted into a score out of 30 via the cumulative distribution function. A higher score indicates better overall cognitive performance.
Two-back task test
Participants were required to judge whether the currently presented letter was identical to the letter presented two positions back. The test was administered via a computerized system for 100 trials, and the accuracy rate was recorded.
Statistical Analysis
Data analysis was performed using R software (version 4.5.1).
Missing data generated during longitudinal follow-up were handled using a multiple imputation method based on mixed-effects models. Using the participant ID as the hierarchical variable, an imputation model incorporating time variables, baseline covariates, and prior measurements was constructed to generate imputed datasets. For each complete dataset, analysis was performed separately using linear mixed-effects models. Parameter estimates and standard errors were ultimately pooled according to Rubin’s rules to ensure the accuracy of statistical inference.
We employed a linear mixed-effects model (Saigusa et al., 2022; Yang et al., 2025). The model included group, time, and their interaction as fixed effects, and a random intercept was set for each participant to account for the correlation among repeated measures data. Models were fitted using restricted maximum likelihood (Malik and Michoel, 2022; Grantham et al., 2022). The overall significance of fixed effects was first tested via Analysis of Variance (ANOVA). If a significant interaction effect was found, post hoc pairwise comparisons were further conducted using the emmeans package, applying the Tukey method for multiple comparison correction (Schaarschmidt et al., 2022; Zweifach, 2025). Post hoc comparisons included two aspects: (1) comparing intergroup differences at each time point; and (2) comparing differences between various time points and the baseline within each group.
This study employed a longitudinal mediation analysis framework based on linear mixed-effects models to examine the time-varying mediating role of cognitive function in the relationship between stress levels and casualty care capabilities. To control for initial individual differences, we included the baseline value from the first measurement as a covariate in the models. We established two linear mixed models: Model 1 examined the effect of stress level on cognitive function, and Model 2 examined the effects of both stress level and cognitive function on casualty care capability; both models included individual random intercepts to control for the inherent correlation of repeated measures data. An interaction term between stress and time was introduced into the models, allowing the strength of the mediation pathways to vary over time. We assessed the mediation effect at each time point by calculating the conditional indirect effect and used the parametric bootstrap method (2000 resampling iterations) to compute 95% confidence intervals and p-values for all effects in parallel. Finally, effect decomposition was performed to calculate the direct effect, indirect effect, total effect, and the proportion mediated.
Results
Participant characteristics
Across three hospitals, 318 participants were screened, and 276 eligible participants were enrolled (Fig. 1). In the HAI group, one participant was unable to complete the tests, and another left the high-altitude area early for personal reasons. In the HA group, one participant was unable to complete the tests and two participants left the high-altitude area early for personal reasons. No participants discontinued the study in the SL group. The participants’ demographic and clinical characteristics are shown in Table 1. The three groups showed no statistically significant differences in the baseline characteristics.
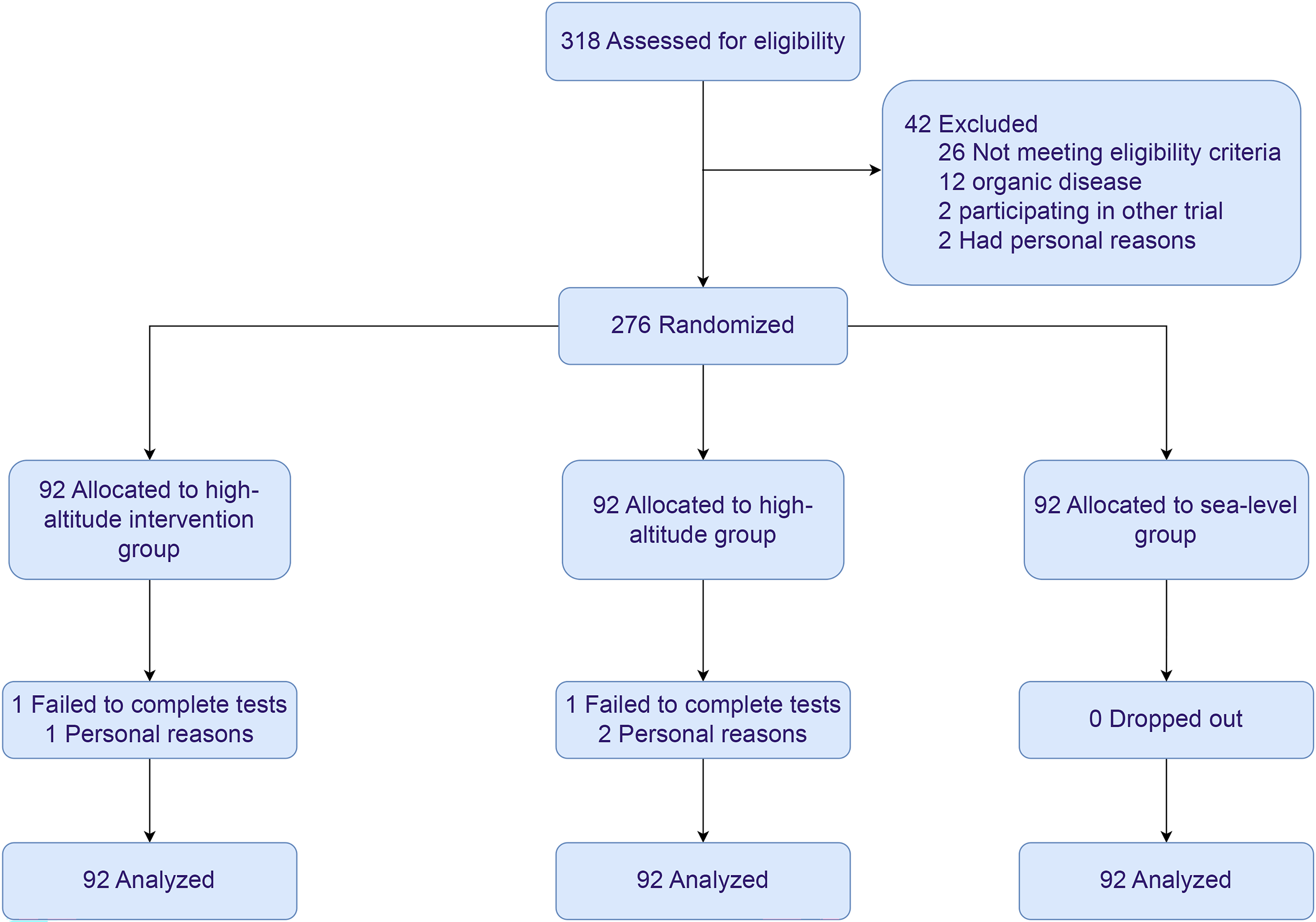
Study flowchart.
Baseline Characteristics of Participants
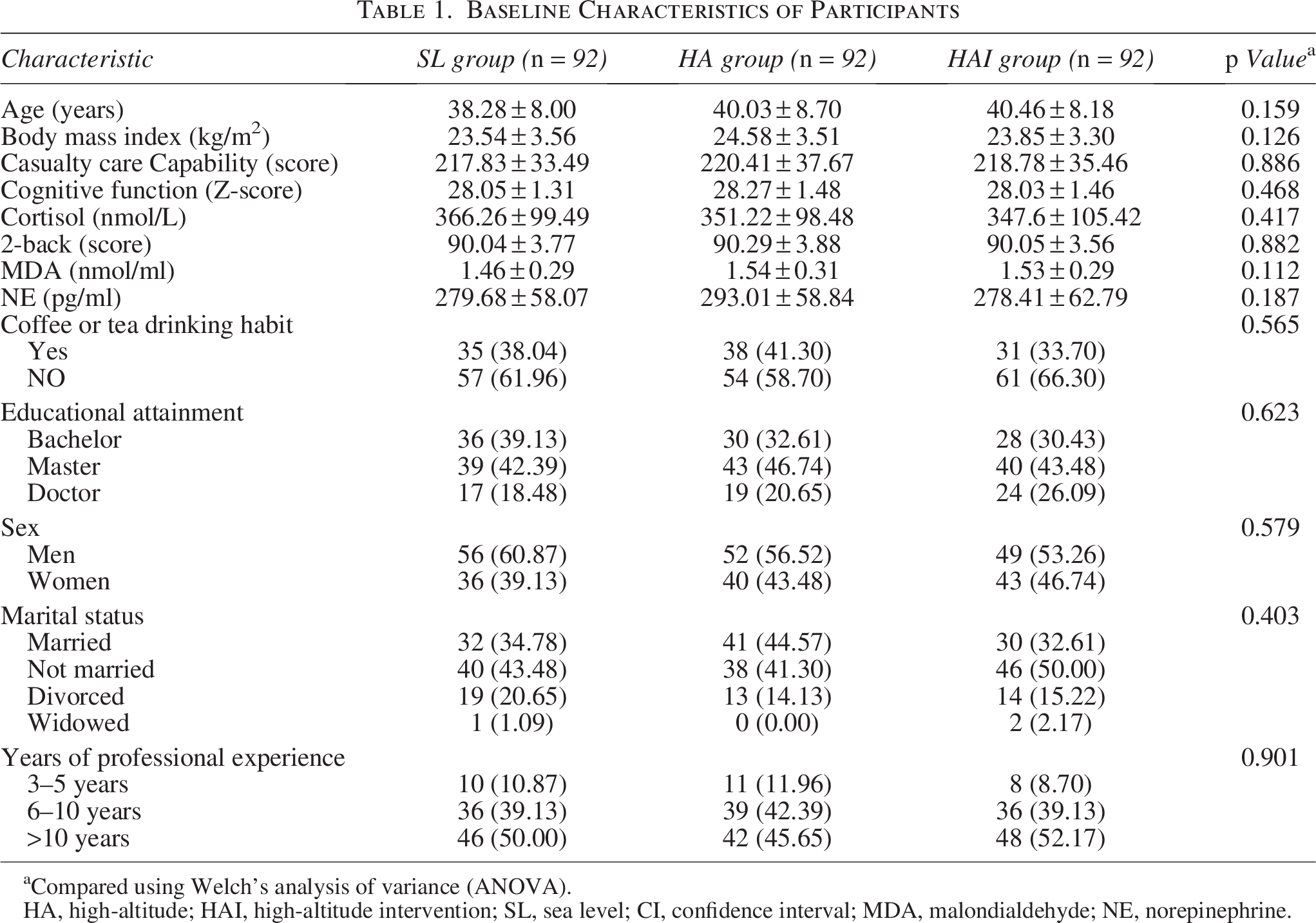
Compared using Welch’s analysis of variance (ANOVA).
HA, high-altitude; HAI, high-altitude intervention; SL, sea level; CI, confidence interval; MDA, malondialdehyde; NE, norepinephrine.
Changes in casualty care capability scores
The HAI group showed significantly lower casualty care capability scores than the SL group at all time posts after RAHA (p < 0.01). At 24 hours postascent, the decrease in casualty care capability scores did not differ significantly between the HAI and HA groups. However, from 72 to 96 hours, the reduction in scores was significantly smaller in the HAI group than in the HA group (p < 0.001). The largest difference between the HAI and HA groups occurred at 96 hours (difference: 64.01, 95% confidence interval [CI]: 52.85–75.18, Table 2). The changes in casualty care capability scores over time for all three groups are shown in Figure 2.
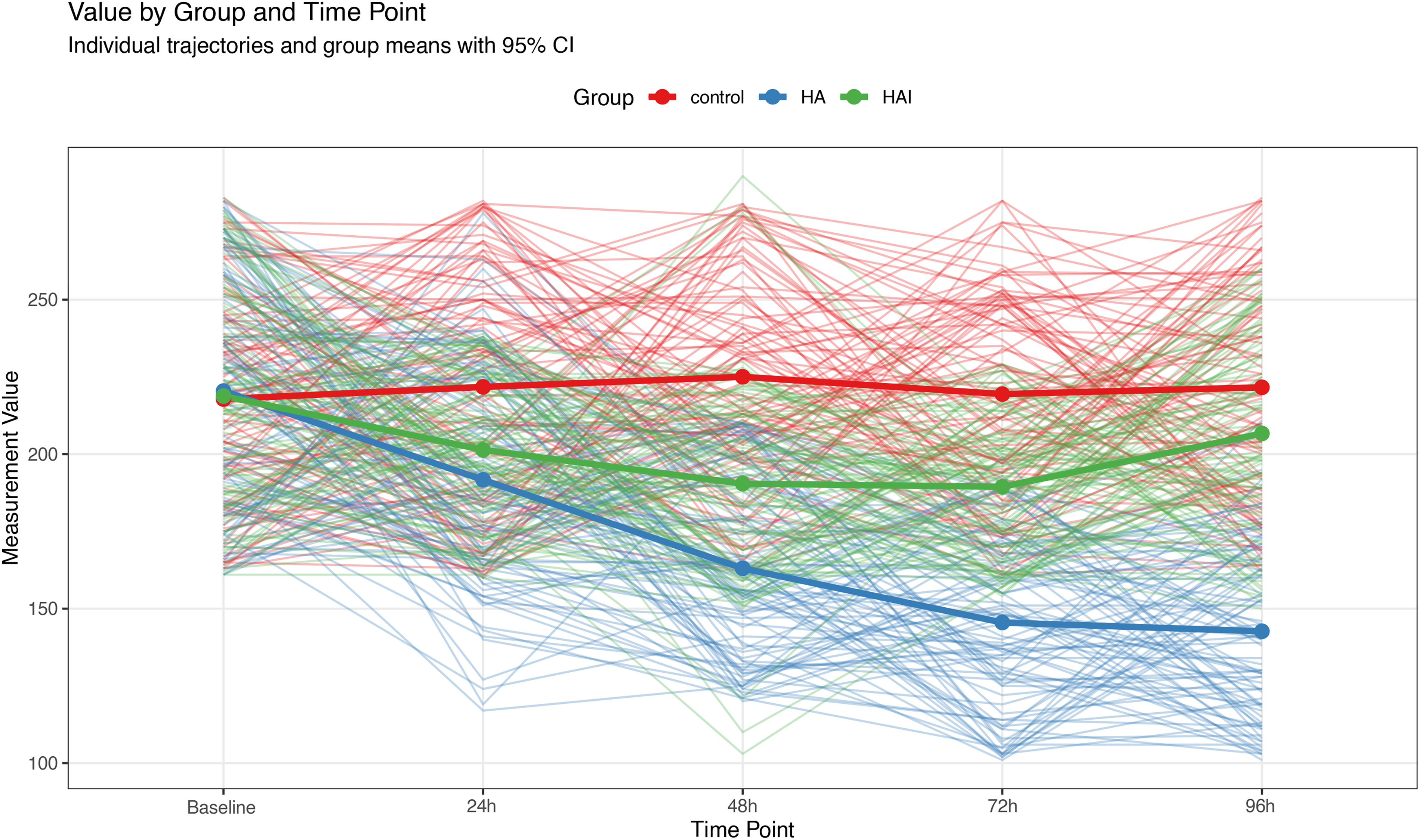
Changes in casualty care capability scores over time following rapid ascent to high altitude (RAHA), by group. Solid lines represent the mean change trajectories, thin lines represent individual change trajectories, and different colors indicate different groups.
Changes in Casualty Care Capability Scores Over Time Following RAHA, by Group (Score)

Scores range from 0 to 300, with higher scores indicating enhanced casualty care capabilities.
Compared using Tukey correction.
Changes in cognitive function scores
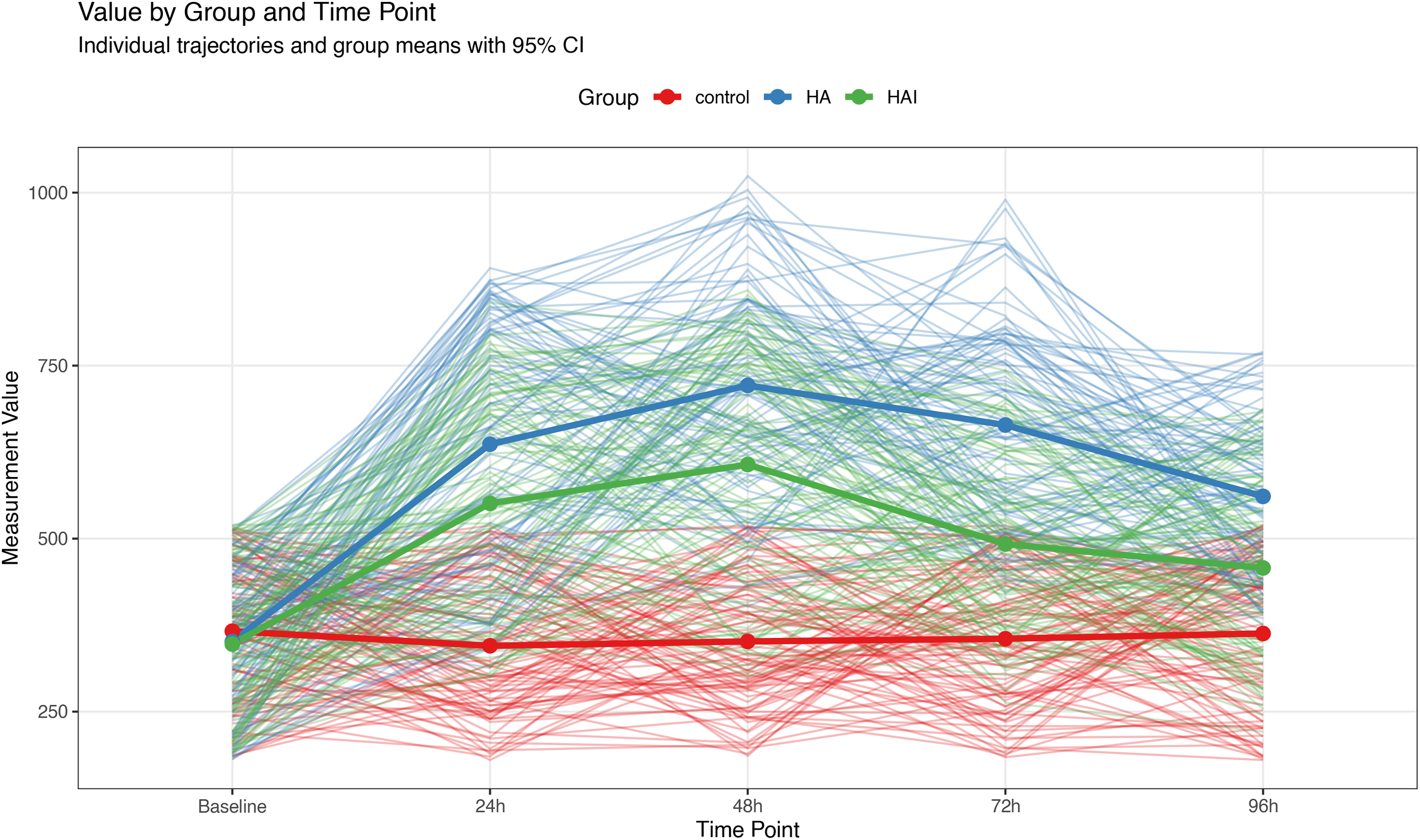
At 24–72 hours after RAHA, the HAI group demonstrated significantly lower cognitive function scores than the SL group (p < 0.001). At 96 hours, the cognitive function scores between the HAI and SL groups were no longer significantly different (p > 0.05). The reduction in cognitive function scores was significantly smaller in the HAI group than in the HA group at all time points after RAHA (p < 0.001). The largest difference in cognitive function scores between the HAI and HA groups occurred at 96 hours (difference: 3.96, 95% CI: 3.19–4.72, Table 3). The changes in cognitive function scores over time for all three groups are shown in Figure 3.
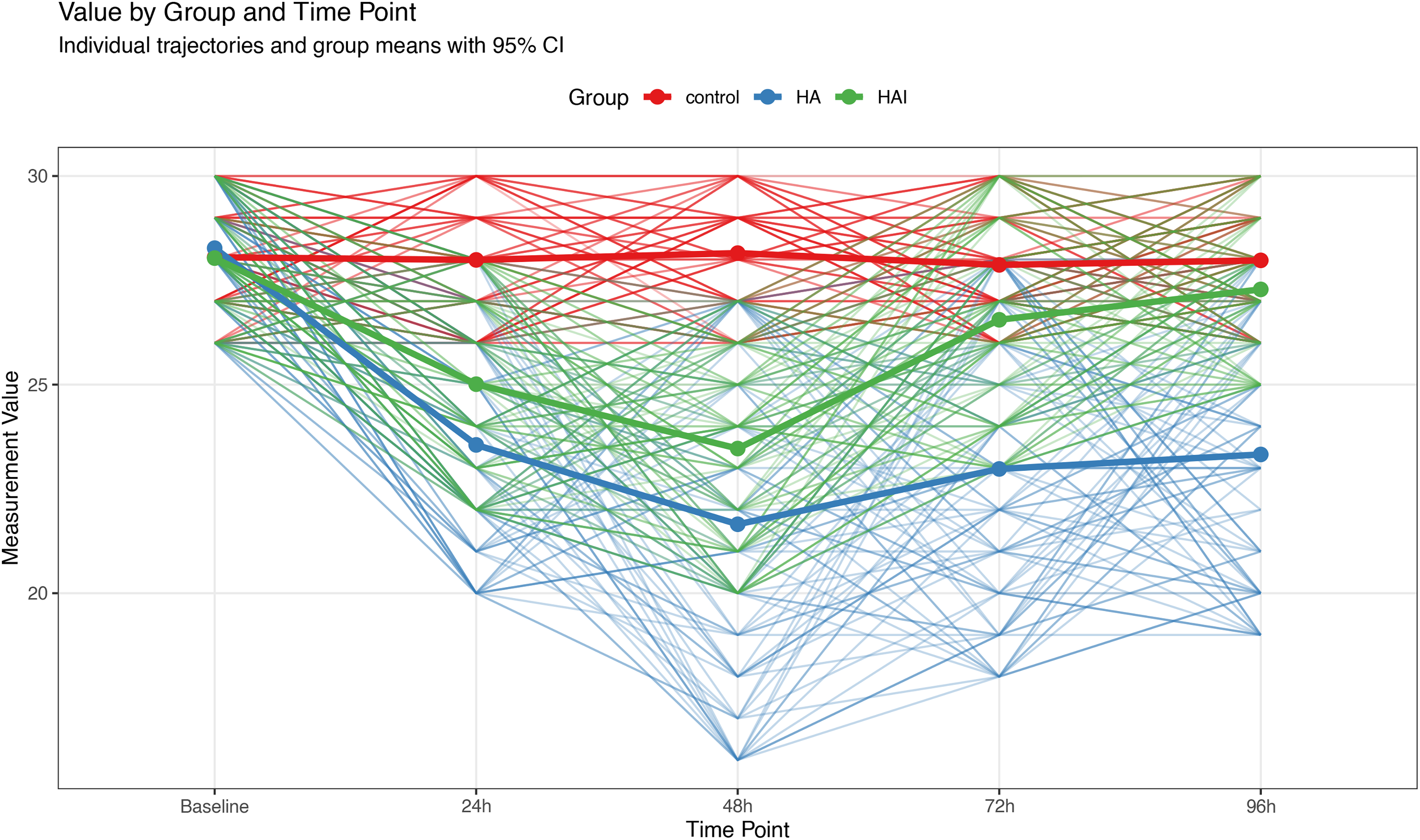
Changes in cognitive function scores over time following RAHA, by group. Solid lines represent the mean change trajectories, thin lines represent individual change trajectories, and different colors indicate different groups.
Changes in Cognitive Function Scores Over Time Following RAHA, by Group (Z-Score)
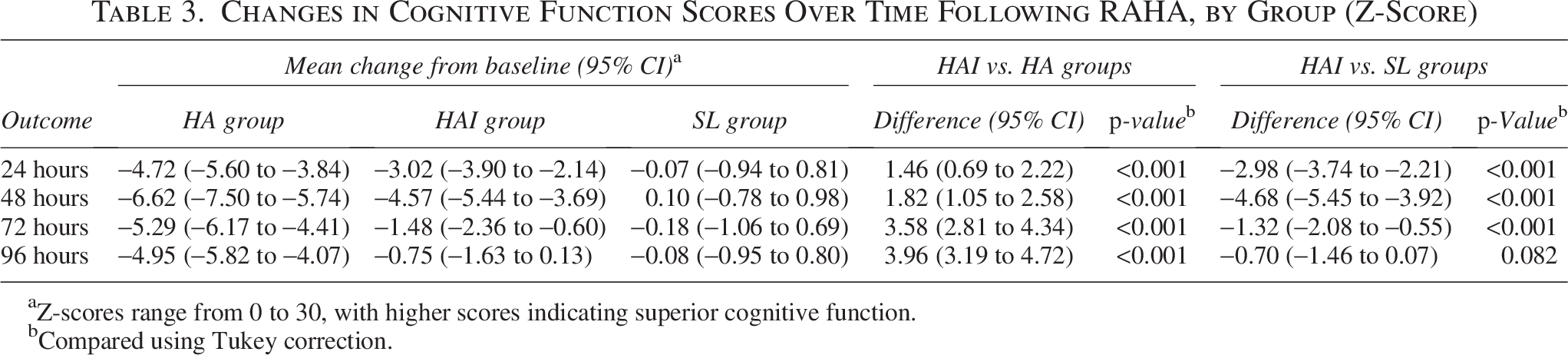
Z-scores range from 0 to 30, with higher scores indicating superior cognitive function.
Compared using Tukey correction.
Changes in stress response
The cortisol levels in the HAI group were significantly higher than those in the SL group at all time points after RAHA (p < 0.001). However, the magnitude of increase in cortisol levels was significantly smaller in the HAI group than in the HA group at all time points (p < 0.001). The largest difference in cortisol levels between the HAI and HA groups occurred at 72 hours (difference: −171.96, 95% CI: −216.23 – −127.68, Table 4). The changes in cortisol levels over time for all three groups are shown in Figure 4.
Changes in cortisol levels over time following RAHA, by group. Solid lines represent the mean change trajectories, thin lines represent individual change trajectories, and different colors indicate different groups.
Changes in Cortisol Levels Over Time Following RAHA, by Group (nmol/L)

aCompared using Tukey correction.
Changes in secondary outcomes
The two-back scores in the HAI group were significantly lower than those in the SL group at all time points (p < 0.001); however, the magnitude of score reduction was significantly smaller in the HAI group than in the HA group (p < 0.001). The maximum difference between the HAI and HA groups was observed at 48 hours (difference: 14.22, 95% CI: 11.42–17.02). MDA levels in the HAI group were significantly higher than those in the SL group at all time points (p < 0.001); however, the magnitude of MDA increase was significantly smaller in the HAI group than in the HA group (p < 0.001). The largest difference in MDA levels between the HAI and HA groups was observed at 48 hours (difference: −2.23, 95% CI: −2.44 – −2.02). NE levels in the HAI group were significantly higher than those in the SL group at all time points (p < 0.01), whereas the magnitude of NE increase was significantly smaller in the HAI group than in the HA group (p < 0.001). The maximum difference in NE levels between the HAI and HA groups was found at 48 hours (difference: −484.71, 95% CI: −529.46 – −439.95). These results are summarized in Table 5.
Changes in Secondary Outcomes Over Time Following RAHA, by Group
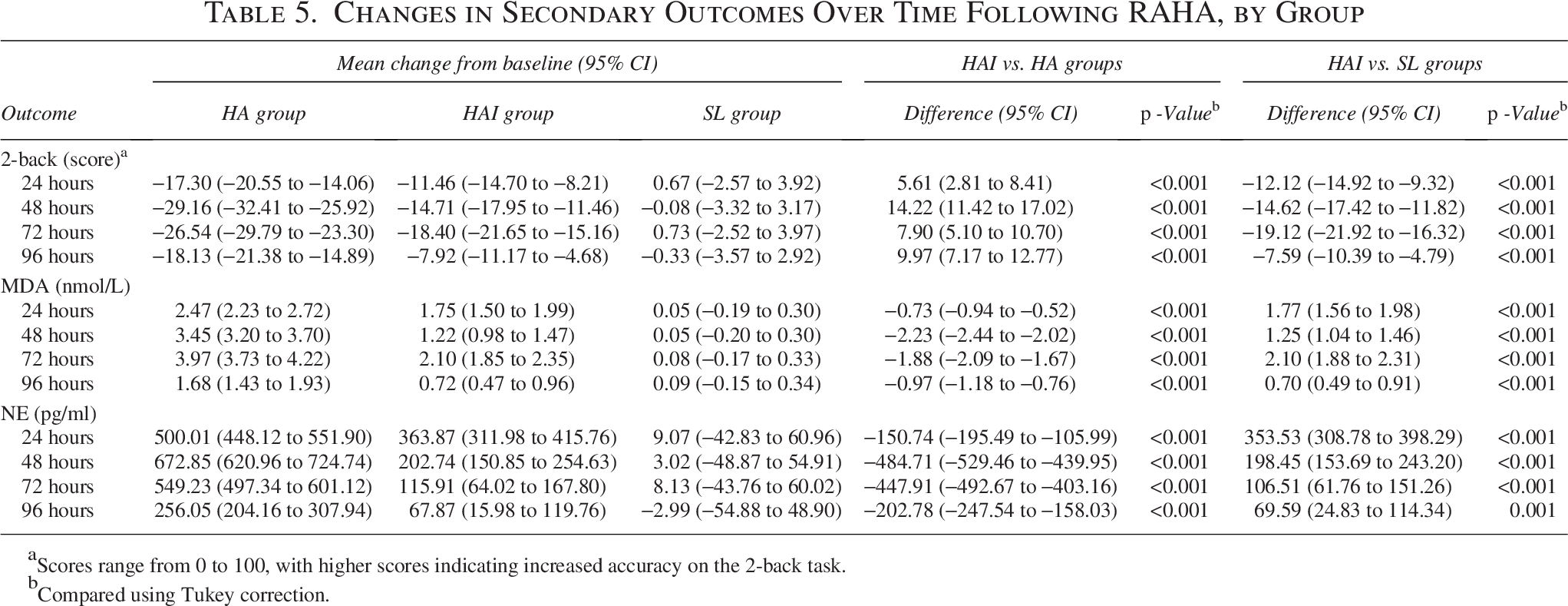
Scores range from 0 to 100, with higher scores indicating increased accuracy on the 2-back task.
Compared using Tukey correction.
Mediation analysis of the stress-cognitive function-casualty care capability pathway across groups
Mediation analysis of the stress-cognitive function-casualty care capability pathway in the HA group revealed a dynamically evolving mechanism over time (Table 6, Fig. 5). A significant suppressive effect was observed at 24 hours. A strong negative indirect effect of cognitive function (β = −0.106, p < 0.001) coexisted with a positive direct effect of stress (β = 0.058, p = 0.006). At 48 hours, the influence remained dominated by a negative indirect effect of cognitive function (β = −0.047, p < 0.001), whereas the direct effect of stress was not significant (β = 0.014, p = 0.263). By 72 hours, the cognitive function–mediated indirect effect weakened but remained significant (β = −0.012, p = 0.001), and the stress-mediated direct effect became significantly negative (β = −0.029, p = 0.018). At 96 hours, the cognitive function–mediated indirect effect disappeared (β = −0.007, p = 0.847), and the total effect was entirely explained by the stress-mediated direct effect (β = −0.073, p < 0.001).
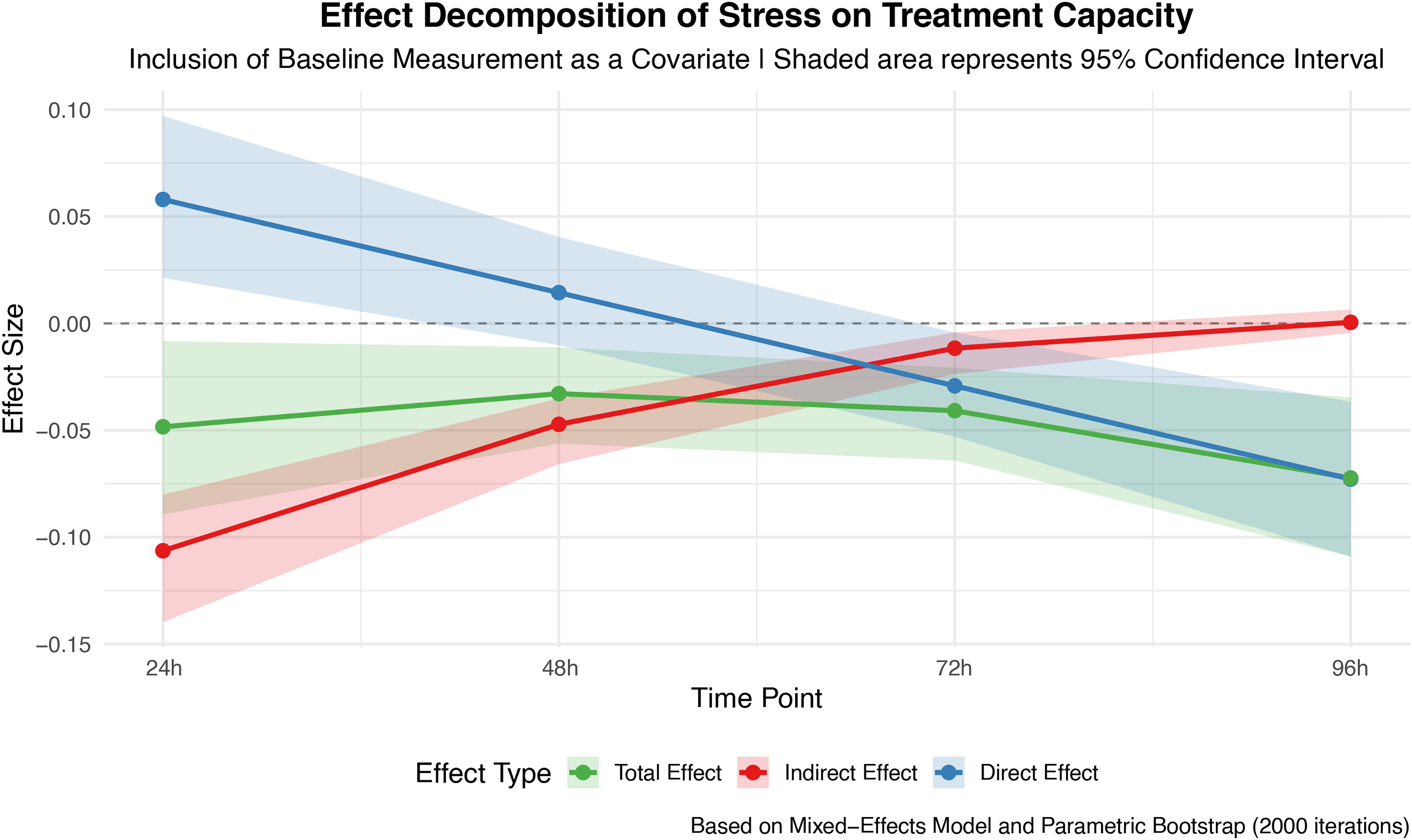
Mediation analysis of the stress-cognitive function-casualty care capability pathway in the high-altitude (HA) group. Lines represent change trajectories of effect sizes, and shaded areas indicate confidence intervals.
Mediation Analysis of the Stress-Cognitive Function-Casualty Care Capability Pathway in the HA Group

aBased on linear mixed-effects models and parametric bootstrapping with 2,000 repetitions.
In the HAI group, the mediating effect of stress on casualty care capabilities through cognitive function was only observed in the early stages. At 24 and 48 hours, the total (24 hours: β = −0.068, p < 0.001; 48 hours: β = −0.028, p = 0.029) and indirect effects (24 hours: β = −0.037, p = 0.006; 48 hours: β = −0.015, p = 0.001) were significant, whereas the direct effects were not significant, with mediation proportions 54.3% and 54.5%, respectively, indicating that cognitive function is crucial in complete mediation. At 72 and 96 hours, neither the total, indirect, nor direct effects were statistically significant (p > 0.05). The results are presented in Table 7 and Figure 6.
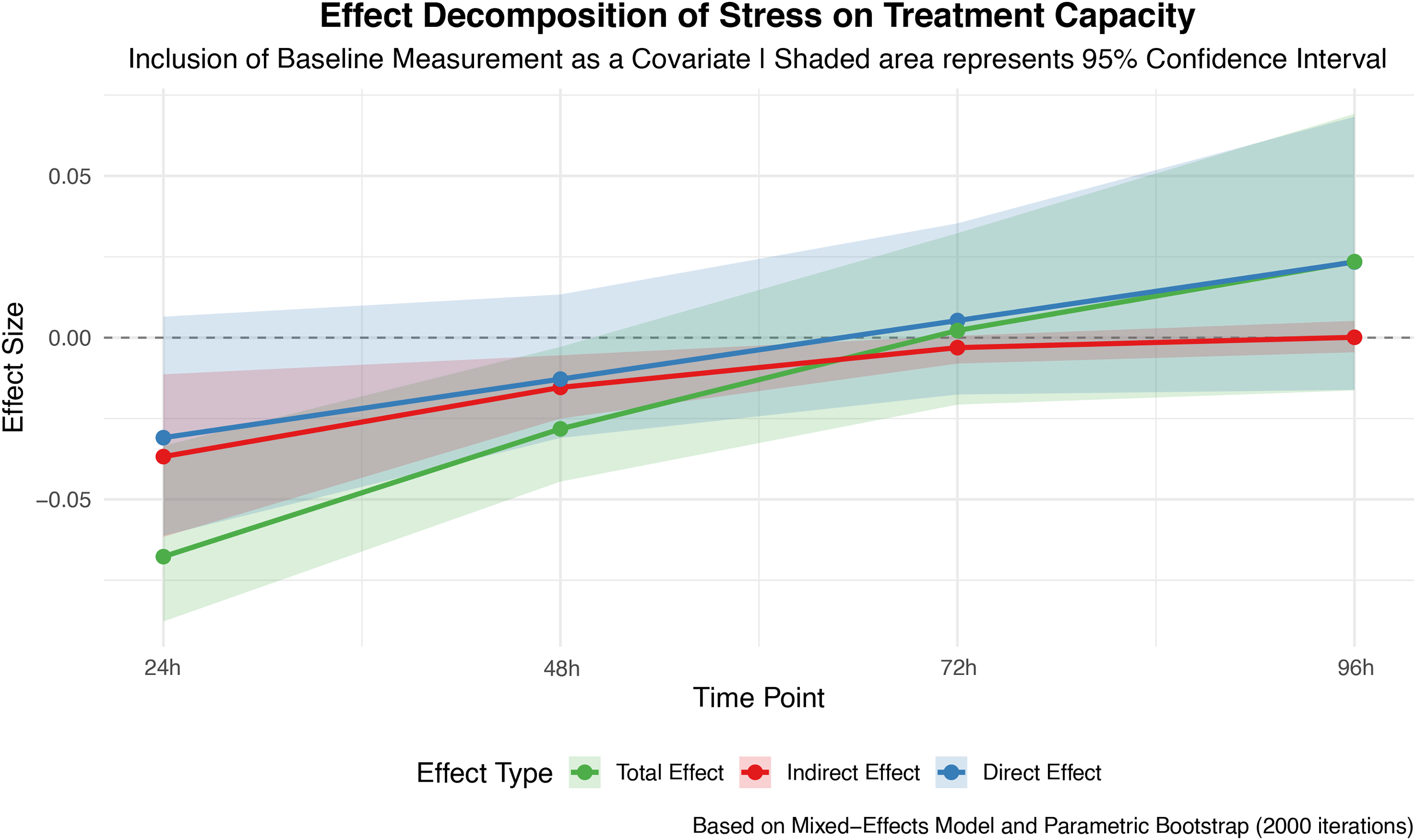
Mediation analysis of the stress-cognitive function-casualty care capability pathway in the high-altitude intervention (HAI) group. Lines represent change trajectories of effect sizes, and shaded areas indicate confidence intervals.
Mediation Analysis of the Stress-Cognitive Function-Casualty Care Capability Pathway in the HAI Group
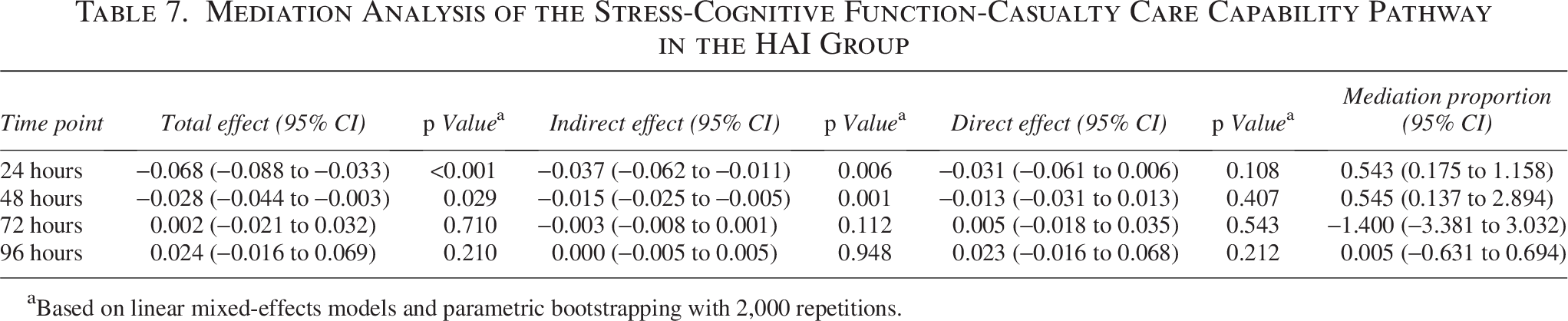
Based on linear mixed-effects models and parametric bootstrapping with 2,000 repetitions.
Discussion
This study systematically evaluated the multifaceted effects of an intervention on organismal function and stress response in RAHA. Mediation analysis further elucidated the cognitive pathway mechanism through which stress impairs casualty care capability and the blocking effect of the intervention on this pathway.
Regarding casualty care capabilities, the intervention demonstrated a significant time-dependent protective effect. Although the degree of score reduction did not differ significantly between the HAI and HA groups at 24 hours, the protective effect in the HAI group became prominent after 48 hours and peaked at 72 hours. This indicates a lag in the impact of the intervention on casualty care capabilities, which requires time to fully exert its rescue effect. Notably, the pattern of cognitive function changes closely mirrored that of casualty care capability. At 24–72 hours, cognitive function scores in the HAI group, although lower than those in the SL group, decreased significantly less than those in the HA group. By 96 hours, their cognitive function had recovered to a level comparable to that of the SL group. This suggests that the preservation of cognitive function may be a crucial foundation for an intervention’s ability to maintain comprehensive casualty care capability.
Cortisol, a key stress hormone, significantly increased in the HA group, whereas the increase was significantly smaller in the HAI group, with the maximum difference observed at 72 hours. This coincided with the largest intergroup difference in cognitive function during the same period, implying that the intervention may buffer the release of stress hormones, thereby mitigating the damage caused by excessive stress to central cognitive function and executive capacity (Balasamy et al., 2024; Stephens and Wand, 2012; Roberts and McWade, 2021). The magnitude of the increase in MDA (oxidative stress marker) and NE (sympathetic nervous activity marker) was significantly lower in the HAI group than in the HA group, suggesting that the intervention may exert protective effects via multiple pathways, including reducing oxidative damage and modulating the autonomic nervous system balance (Cordiano et al., 2023; Czerska et al., 2015; Zuin et al., 2022; Nestel et al., 2017).
In the HA group, mediation analysis revealed a clear and dynamically evolving impairment mechanism. In the initial phase of rapid ascent, a strong negative indirect effect of cognitive function coexisted with a positive direct effect of stress. The stress response from a rapid ascent impairs cognitive function, leading to decreased casualty care capabilities, while simultaneously activating compensatory mechanisms that attempt to directly sustain casualty care capabilities. However, the powerful negative effect of cognitive impairment was completely suppressed and masked this potential protective effect, ultimately manifesting as a significant negative total effect. By 48 hours, the cognition-mediated indirect effect remained the primary source of the total effect, whereas the positive direct effect of stress became nonsignificant, suggesting a depletion of the initial compensatory mechanism. At 72 hours, although the cognitive-mediated indirect effect weakened significantly, it remained important (mediation proportion; 28%), and a significant negative direct effect of stress emerged. With prolonged exposure, noncognitive factors, such as fatigue and physical exhaustion, begin to directly contribute to impaired casualty care capabilities. By 96 hours, the mediating role of cognitive function disappeared completely, and the total effect was entirely explained by the strong negative direct effect of stress. Under sustained stress, the initial “stress-cognitive function-casualty care capability” pathway had collapsed and was no longer the core mechanism, replaced by direct damage dominated by systemic physiological dysfunction. At 96 hours, stress levels decreased, and cognitive function recovered in the SL group; however, casualty care capabilities declined. This could be because the cumulative nature of stress-induced damage to the organism and lag in the recovery of casualty care capabilities. Alternatively, after the depletion of the cognitive pathway, recovered cognitive function may no longer be able to positively protect casualty care capability. In a high-altitude environment, the mechanism by which the stress response affects casualty care capabilities evolves dynamically. In the early phase, it is primarily indirect via cognitive mediation, accompanied by a suppression effect. In the mid-phase, it transitions to a combination of cognitive mediation and direct physiological effects. In the later phase, it manifests entirely as a direct physiological effect of stress. This explains the reason changes in the various variables are a dynamic process with fluctuations, rather than simply linear.
Compared to the HA group, the mediation effect pattern in the HAI group underwent a fundamental change, characterized by substantial weakening and earlier disappearance of the effect, including early blockade and complete mediation. In the intervention group, significant mediation effects were observed only at 24 and 48 hours. Although the total and indirect effects remained significant, the indirect effect values were far lower than those in the HA group at the same time points. The direct effect was not significant, and the mediation proportion remained stable at ∼54%. The intervention did not completely eliminate the early impact of stress but successfully confined its influence to a single pathway of cognitive mediation, achieving complete mediation. Notably, in the early stage of RAHA in the HAI group, we did not observe a direct positive regulatory effect of stress on casualty care capabilities, likely related to the intervention’s reduction in the stress response itself. At 72 and 96 hours, the entire “stress-cognition-casualty care capabilities” pathway became nonsignificant in the intervention group. This aligns with the recovery trends observed in casualty care capabilities and Cogstate scores. The protective effect of the intervention strengthened and expanded over time, almost completely offsetting the negative effects of high-altitude stress on cognitive function and casualty care capabilities. Its mechanism of action extends beyond mere cognitive protection, encompassing the mitigation of oxidative stress and stabilization of neuroendocrine responses, thereby dismantling the entire network of stress-induced damage. The intervention employed in this study demonstrates multistage, multitarget protective characteristics; it primarily targets the preservation of cognitive function, acting as a “buffer” that confines stress-induced damage to a single pathway (early phase) and functions as a “comprehensive protective net,” maintaining multisystem homeostasis and preventing the stress response from effectively establishing any significant damaging pathways (later phase).
In the mid-to-late stages of rapid ascent, the cognitive mediation effect disappeared in the HA and HAI groups. However, the “nonsignificance” of this effect carries diametrically opposite meanings in the two groups. In the HA group, its disappearance is a “catastrophe,” representing the destruction and exhaustion of the cognitive pathway, loss of its buffering role, leading to stress directly attacking core capabilities, and collapse of casualty care capabilities. In the HAI group, its disappearance is a “victory,” representing the protection and transcendence of the cognitive pathway, in which individuals are no longer constrained by the fragile chain of stress-cognition-ability, having established greater overall resilience. Casualty care capabilities became stable. Therefore, the core mechanism of this intervention is to progressively buffer, weaken, and ultimately sever this negative mediating pathway, thereby protecting an individual’s casualty care capabilities from erosion by stress.
The integrated cognitive-stress management intervention program employed in this study consists of two core components. The cognitive training component focuses on three key executive function domains: working memory, cognitive flexibility, and attentional allocation. The “dual N-back” task was selected because it is a classical paradigm for working memory training, which not only enhances working memory capacity but also produces near-transfer effects (e.g., improved attentional control) and far-transfer effects (e.g., enhanced fluid intelligence). This provides a theoretical basis for maintaining information processing capacity in complex, unfamiliar high-altitude environments. Task-switching training directly targets cognitive flexibility—a critical ability for rapidly shifting thinking and behavioral strategies in response to environmental changes. Attentional allocation training aims to strengthen the ability to distribute limited cognitive resources among multiple tasks, which may be particularly important in high-altitude environments where individuals must simultaneously cope with physiological discomfort and environmental monitoring demands. The stress management component integrates diaphragmatic breathing, mindfulness meditation, and progressive muscle relaxation techniques. These techniques were chosen based on their respective, empirically supported pathways for modulating stress responses: diaphragmatic breathing directly regulates autonomic balance by increasing parasympathetic nervous system activity; mindfulness meditation enhances emotional and cognitive regulation in stressful situations by fostering nonjudgmental awareness of present-moment experiences; and progressive muscle relaxation reduces overall physiological arousal by systematically relieving physical tension. The combination of these three techniques is designed to act synergistically across physiological, cognitive, and emotional levels, constructing a multitarget stress-buffering system. Therefore, the design of this intervention program is not an arbitrary combination but aims to systematically enhance individuals’ comprehensive adaptive capacity to high-altitude stress by specifically strengthening executive functions and building multidimensional stress resistance.
This study employed linear mixed-effects models to analyze the repeated measures data. Linear mixed-effects models are powerful tools in modern statistics for handling complex data, with their core advantage lying in the ability to model both fixed effects and random effects simultaneously. Their strengths are primarily manifested in the following aspects: (1) They can effectively analyze repeated measures, longitudinal data, or data with a nested structure, accounting for correlations among observations within the same group and avoiding bias caused by violating the independence assumption inherent in traditional regression. (2) By incorporating random intercepts and random slopes, they can capture heterogeneity among different individuals or groups while allowing for the investigation of the overall trend of fixed effects, making the results more generalizable and accurate. (3) In studies with unequal sample sizes or inconsistent measurement time points, linear mixed-effects models can still effectively integrate information, reduce information loss, and enhance statistical power. (4) By appropriately specifying the random effects structure, the model can control for within-group correlations while avoiding the misattribution of random differences as fixed effects, thereby yielding more reliable inferences. Therefore, the main findings of this study are based on a more robust statistical framework that better aligns with the intrinsic structure of the data, strengthening the reliability of the conclusions.
This study had several limitations. First, the cognitive function assessment tools were limited. Although Cogstate is a widely used cognitive screening tool, its ability to evaluate specific cognitive domains, such as executive function and working memory, is limited. Future research should incorporate neurobehavioral tests, electroencephalography, or functional near-infrared spectroscopy to provide a more comprehensive and objective assessment of cognitive changes and their underlying neural mechanisms. Second, long-term follow-up data were lacking. This study primarily focused on dynamic changes within 96 hours of rapid ascent and did not assess the long-term protective effects of the intervention or functional recovery after returning to the plains. Subsequent studies could extend the observation period to explore whether the intervention sustains its benefits. Third, not all potential confounding variables were controlled. Multiple stressors present in high-altitude environments, such as hypoxia, cold, and ultraviolet radiation, may collectively influence outcomes. Although several physiological indicators were included, unmeasured variables, such as sleep quality and nutritional status, may have interfered with the results. Finally, although in this study, “documentary viewing” served as an active control task, with its content strictly screened to achieve emotional and cognitive neutrality, it must be acknowledged that this design still has certain limitations. The narrative structure and audiovisual content of the documentary may unintentionally evoke specific cognitive processes or subtle emotional modulation. While this differs in nature from the cognitive training mechanisms of primary interest in the experiment, the potential influence of these factors on the baseline state of the control group cannot be entirely ruled out. Future studies could employ more passive audiovisual stimuli or conduct standardized measurement and matching of the emotional and cognitive load of control content to further refine the design of control conditions.
Conclusion
High-altitudes environment causes damage through a dynamic “stress-cognition-casualty care capabilities” pathway, initially dominated by cognitive mediation and eventually shifting to direct physiological effects. The core mechanism of the integrated cognitive-stress management training was progressive weakening, which ultimately severed this pathologically mediated pathway. The intervention acts early as a “buffer,” confining damage to the cognitive pathway, and in the mid-to-late stages, serves as a “comprehensive protective net,” disrupting the formation of stress-induced damage pathways through multisystem stabilization, thereby effectively protecting casualty care capabilities.
Authors’ Contributions
Z.Y. initiated and supervised the project. Z.Y. and L.L. Designed and performed the analysis. Z.Y. and T.D. Wrote the article. T.D., H.S., and L.L Revised the article. All authors read and approved the article.
Footnotes
Acknowledgment
The authors would like to acknowledge all participants.
Author Disclosure Statement
All authors declare no conflicts of interest.
Funding Information
This study was not supported by any funding.
Consent for Publication
All authors agreed to publish the article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available because they contain protected personally identifiable information. In accordance with the approval granted by the Medical Ethics Committee of the General Hospital of Xinjiang Military Command and the hospital’s data protection policies, the raw data cannot be shared publicly. However, in compliance with ethical and legal standards, partially deidentified data necessary for replicating the findings are available from the corresponding author upon reasonable request.