
Abstract
Wei, Shuna, Xiaoju Liu. High-altitude environment and chronic obstructive pulmonary disease: epidemiology, pathological mechanisms and clinical management. High Alt Med Biol. 00:00–00, 2026
Background:
Chronic obstructive pulmonary disease (COPD) is a significant global health concern. Environmental factors such as low oxygen and temperature, along with poor living habits in high-altitude areas, contribute to regional variations in the occurrence and progression of COPD. There is currently a lack of systematic reviews on the relationship between high-altitude environments and COPD, which hinders effective prevention and treatment.
Methods:
This narrative review comprehensively sorts out and analyzes the research on COPD in high-altitude areas from three aspects: epidemiological characteristics, pathophysiological mechanisms, and clinical management.
Results:
Epidemiologically, COPD mortality increases with altitude; however, prevalence rates remain debated. Pathophysiologically, factors include hypoxia-inducible factor regulation, hemodynamic changes, air pollution particles promoting inflammation and oxidative stress, as well as gene mutations like PPARA and SERPINA1. Clinically managing COPD in high-altitude regions requires individualized approaches that consider environmental conditions.
Conclusion:
High-altitude environments exacerbate COPD through hypoxic stress, pollutant exposure, and genetic variations. Future efforts should focus on developing a risk prediction model for COPD that incorporates altitude parameters to enhance targeted prevention and treatment strategies in these areas.
Introduction
Chronic obstructive pulmonary disease (COPD) remains a major challenge to global public health, with a high prevalence and mortality rate, imposing a heavy burden on the economy and society. The global prevalence of COPD is ∼10.3% (Adeloye et al., 2015). With the rising smoking rates in low- and middle-income countries and the aging of the population, the prevalence is expected to increase further (Adeloye et al., 2022; Fallahzadeh et al., 2022). The World Health Organization points out that COPD is the third leading cause of death worldwide, with about 3 million deaths per year, and it is projected to exceed 5.4 million by 2060 (Mathers, 2022; WHO). These figures highlight the urgent need to strengthen the prevention and control of COPD in the global public health system.
The epidemiology of COPD differs markedly across geographic settings, particularly in high-altitude regions (Xiong et al., 2020). Globally, about 500 million people live at ≥1,500 m, 81.6 million at ≥2,500 m, and 14.4 million above 3,500 m (Tremblay and Ainslie, 2021). High-altitude environments—characterized by low barometric pressure, reduced oxygen partial pressure, cold temperatures, intense ultraviolet radiation, and aridity—induce physiological adaptations in residents, including alterations in lung volume and diffusing capacity, which may influence COPD patterns (Burtscher, 2014).In addition to altitude as a geographical factor, it is also closely related to multiple factors such as behavioral factors, occupational exposure, genetic susceptibility, socioeconomic differences, medical accessibility, and research methods. Studies have shown that the prevalence of COPD in high-altitude regions is ∼10%, and the prevalence is higher in Asia compared with Europe and the Americas (Xiong et al., 2020). However, there are still many controversies regarding the occurrence, development, and epidemiological characteristics of COPD in high-altitude environments.
In terms of clinical features, patients with COPD in high-altitude regions show significant differences from those in plain areas: the former are more prone to progressive dyspnea, cough, and increased sputum volume, and the severity of symptoms (CAT score ≥10) is significantly higher than that of the control group (p < 0.001) (Jiang et al., 2023); the incidence of nocturnal hypoxemia and apnea index increases (Furian, 2018); the prevalence of pulmonary hypertension is also significantly higher than that of plain area patients (60.2% vs. 31.3%) (Aguirre-Franco et al., 2024; Wang et al., 2023b), and the risk of concurrent hypertension (p = 0.001) and ischemic heart disease (p = 0.001) increases simultaneously (Jiang et al., 2023).
This narrative review examines how altitude influences COPD, covering epidemiological patterns, potential pathophysiological mechanisms, and clinical management in high-altitude settings.
Epidemiological characteristics of COPD in high-altitude regions
This section mainly summarizes the epidemiological characteristics of COPD in high-altitude regions from the aspects of mortality and prevalence.
Existing studies have identified a significant association between COPD mortality and altitude, with mortality generally increasing with altitude (Coté et al., 1993; Ezzati et al., 2023). Hwang et al. (2018) confirmed a positive correlation between altitude and respiratory disease mortality, particularly in regions with high COPD prevalence. Specifically, COPD mortality rises by 1 per 100,000 for every 95 m increase in altitude (Burtscher, 2014). Ezzati et al. (2023) further reported that COPD mortality in areas ≥1,000 m is 3–4 per 10,000 higher than at sea level, confirming adverse effects of high-altitude environments on patients with COPD. The underlying mechanism is thought to involve high-altitude hypoxia, which may exacerbate pulmonary hypertension and cor pulmonale, thereby impairing survival in patients with COPD (Ezzati et al., 2023; Pierson, 2000). Additionally, chronic mountain sickness (another key factor for increased COPD mortality risk; Vearrier and Greenberg, 2011) is closely linked to reduced alveolar ventilation. Delayed hypoxic ventilatory response leads to decreased arterial oxygen, elevated pulmonary artery pressure, and increased red blood cell count—pathophysiological changes that raise the risk of acute exacerbation and mortality in patients with COPD (Li et al., 2025a; Sevik et al., 2025).
The altitude–COPD prevalence relationship remains contentious, with studies reporting dichotomous associations—positive, negative, and nonsignificant correlations.
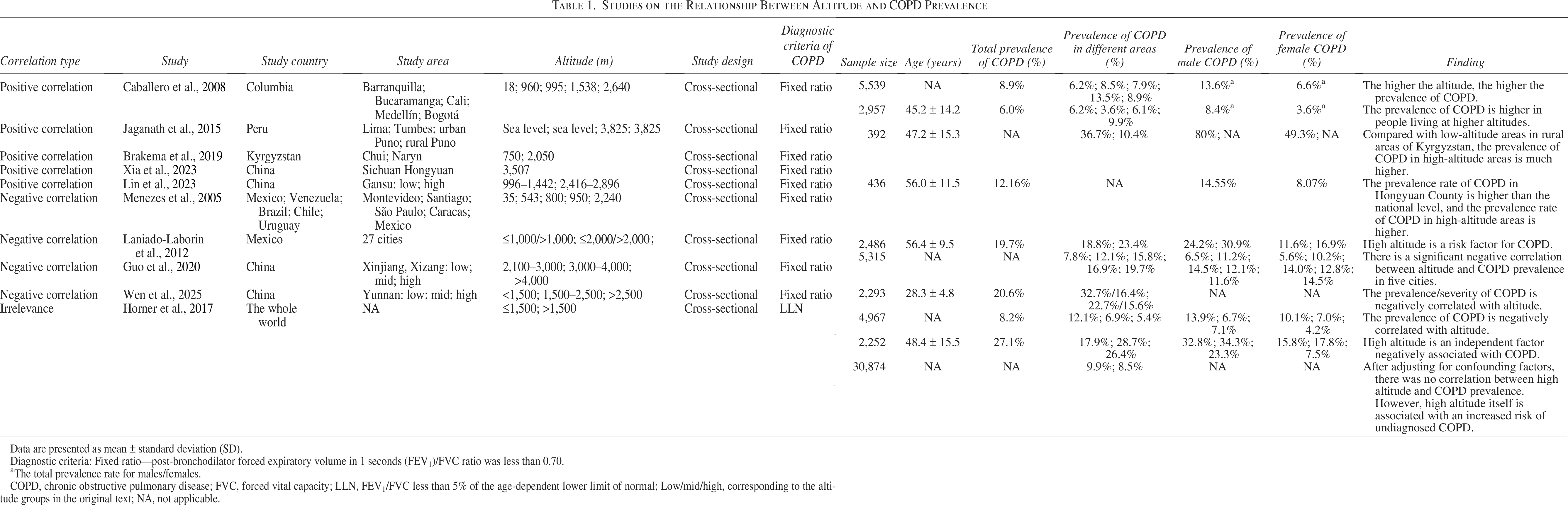
Studies supporting a positive correlation indicate that altitude may increase the risk of COPD through environmental exposures (Table 1). The survey across five Colombian cities showed a stepwise rise in COPD prevalence from 6.2% at 18 m (Barranquilla) to 13.5% at 1,538 m (Medellín) (Caballero et al., 2008). Similar patterns were reported in Peru (3,825 m) (Jaganath et al., 2015) and Kyrgyzstan (2,050 m) (Brakema et al., 2019), where prevalence was markedly higher than in low-lying areas. Chinese regional data corroborate these findings: Hongyuan County (3,507 m) reported a 12.16% prevalence versus the national 9.9% average (Xia et al., 2023); a Gansu cross-sectional study identified altitude as an independent risk factor (23.4% vs. 18.8% in low-altitude zones, p = 0.006) (Lin et al., 2023). And a study linked altitude to elevated PRISm rates (10.03% vs. 5.5% nationally) (Xia et al., 2025). Mechanistically, indoor air pollution from solid fuel combustion in high-altitude areas (Brakema et al., 2019; Yucra et al., 2014) (such as PM2.5 concentration of 5,822 μg/m³ in the Kyrgyzstan plateau, far exceeding the WHO standard; Basagaña, 2019), hypoxia-induced pulmonary arterial hypertension (Aguirre-Franco et al., 2024; Wang et al., 2023b), and increased risk of tuberculosis co-infection (Guo et al., 2020; Liang et al., 2021) may all contribute to the progression of COPD.
Studies on the Relationship Between Altitude and COPD Prevalence
Data are presented as mean ± standard deviation (SD).
Diagnostic criteria: Fixed ratio—post-bronchodilator forced expiratory volume in 1 seconds (FEV1)/FVC ratio was less than 0.70.
aThe total prevalence rate for males/females.
COPD, chronic obstructive pulmonary disease; FVC, forced vital capacity; LLN, FEV1/FVC less than 5% of the age-dependent lower limit of normal; Low/mid/high, corresponding to the altitude groups in the original text; NA, not applicable.
However, several studies have presented contrary conclusions, supporting a negative correlation or no association between altitude and COPD prevalence (Table 1). The PLATINO analysis of five Latin American cities found a strong inverse relationship between altitude and COPD prevalence (Spearman = −1.0); Mexico (2,240 m) had a prevalence of 7.8% versus 19.7% in Montevideo (35 m) (Menezes et al., 2005). Subsequent surveys in 27 Mexican cities (Laniado-Laborin et al., 2012) and large-scale studies in Xinjiang (Guo et al., 2020), and Yunnan (Wen et al., 2025) also reported lower COPD rates at higher elevations. A meta-analysis of 80 studies (2003–2014) concluded that high altitude exerts a protective effect on COPD, although the analysis was limited to national-level data (Aaron et al., 2016). Possible explanations include enhanced pulmonary function adaptability in high-altitude populations (such as increased forced vital capacity and forced expiratory volume in 1 second [FEV1]) (Ortiz-Prado et al., 2024; Spalgais et al., 2025b) and unique hypoxic adaptation characteristics—for instance, Xizang populations tend to achieve adaptation by inhibiting erythrocytosis and enhancing ventilatory efficiency (Richalet et al., 2024), while Andean populations primarily rely on elevated hemoglobin levels to improve oxygen-carrying capacity (Oak et al., 2025; Richalet et al., 2024); East African high-altitude populations, on the other hand, may maintain energy homeostasis by altering the efficiency of mitochondrial oxidative phosphorylation (Richalet et al., 2024; Storz and Cheviron, 2021).
Notably, a large-sample study, PREPOCOL-PLATINO-BOLD-EPI-SCAN, found that altitude itself has no significant impact on COPD prevalence (Horner et al., 2017). This study covered 30,874 participants from 44 countries/regions worldwide and found that the COPD prevalence in areas above 1,500 m and at or below 1,500 m was 8.5% and 9.9%, respectively (p < 0.005). However, after considering individual risk factors, it was concluded that living at high altitudes is not associated with differences in COPD prevalence but is associated with an increased risk of undiagnosed COPD (Horner et al., 2017).
The inconsistent conclusions on the prevalence of COPD among various studies may be influenced by multiple potential factors. First, lower socioeconomic status and scarce medical resources (Guo et al., 2020), as well as the lack of reference equations for spirometry at high altitudes (Li et al., 2025b), can increase the risk of missed diagnosis of COPD. Recently, reference equations for lung function in populations at altitudes ranging from 2,100 to 4,700 m have been established, but they have not been widely promoted (Li et al., 2025b). Second, ethnic groups living at high altitudes may carry genetic variations that adapt to hypoxic environments, which can indirectly affect lung function and COPD susceptibility (Maselli et al., 2019). Additionally, the use of different spirometry thresholds or self-reported questionnaires in various studies leads to inconsistent case definitions, thereby affecting the estimation of prevalence. Finally, significant differences in the definition of “high altitude” among studies directly affect the comparison of exposure intensity. Subsequently, based on altitude grades and in combination with long-term epidemiological monitoring data, the dynamic changes in the distribution of COPD at different altitude gradients can be explored.
According to the fixed ratio definition, there is a significant gender difference in the overall prevalence of COPD: the prevalence in males is 15.47%, significantly higher than that in females at 8.79% (Al Wachami et al., 2024). After summarization, it was found that the prevalence of COPD in males living at high altitudes is also higher than that in females (Table 1) (Guo et al., 2020; Lin et al., 2023; Menezes et al., 2005; Wen et al., 2025). This gender difference may be attributed to higher tobacco consumption in men and greater exposure to harmful particles such as dust and chemical fumes in occupational environments (Ntritsos et al., 2018).
Pathophysiological Mechanisms of COPD in High-Altitude Environments
Molecular mechanisms of hypoxia-inducible factors and their regulation
Hypoxia-inducible factors (HIFs) are oxygen-sensitive transcription factors that play a key role in cellular metabolic responses to hypoxia (Liu et al., 2020). The HIF family comprises HIF-1, HIF-2, and HIF-3, all heterodimeric protein complexes consisting of an oxygen-sensitive α subunit (HIF-α; with three subtypes: HIF-1α, HIF-2α, HIF-3α) and an oxygen-insensitive β subunit. The post-translational modification status of HIF-α is a key node regulating HIF transcriptional activity (Korbecki et al., 2021). Among them, HIF-2 serves as a key molecular hub in COPD, functioning as a molecular “switch” that regulates both the vascular and nonvascular phenotypes (including bronchitis/emphysema) of the disease and is also a potential therapeutic target for COPD (Myronenko et al., 2023). Additionally, elevated levels of HIF-1α have been confirmed as a diagnostic biomarker for COPD (Myronenko et al., 2023).
The HIF equilibrium is controlled by three enzymes: factors inhibiting HIFs (FIHs), prolyl hydroxylases (PHDs), and Von Hippel–Lindau protein (VHL) (McGettrick and O’Neill, 2020). Under normoxia, PHD1/2 hydroxylate HIF-1α at Pro402 and Pro564, while PHD3 modifies only Pro564. Hydroxylated HIF-1α is recognized by pVHL, ubiquitinated, and degraded by the proteasome (McGettrick and O’Neill, 2020). FIHs hydroxylate HIF-1α at Asn803, preventing its interaction with the co-activator p300/CBP and thus repressing target-gene transcription (Fig. 1). Under hypoxia, limited O2 suppresses PHD activity, preventing HIF-1α proteasomal degradation. Stabilized HIF-1α translocates to the nucleus, dimerizes with HIF-β, and binds hypoxia-response elements, activating genes that drive angiogenesis, cell proliferation, survival, and the expression of metalloproteinases, nitric-oxide synthase, erythropoietin, etc. (Fig. 1) (Greer et al., 2012; Hon et al., 2002; Pezzuto and Carico, 2018).
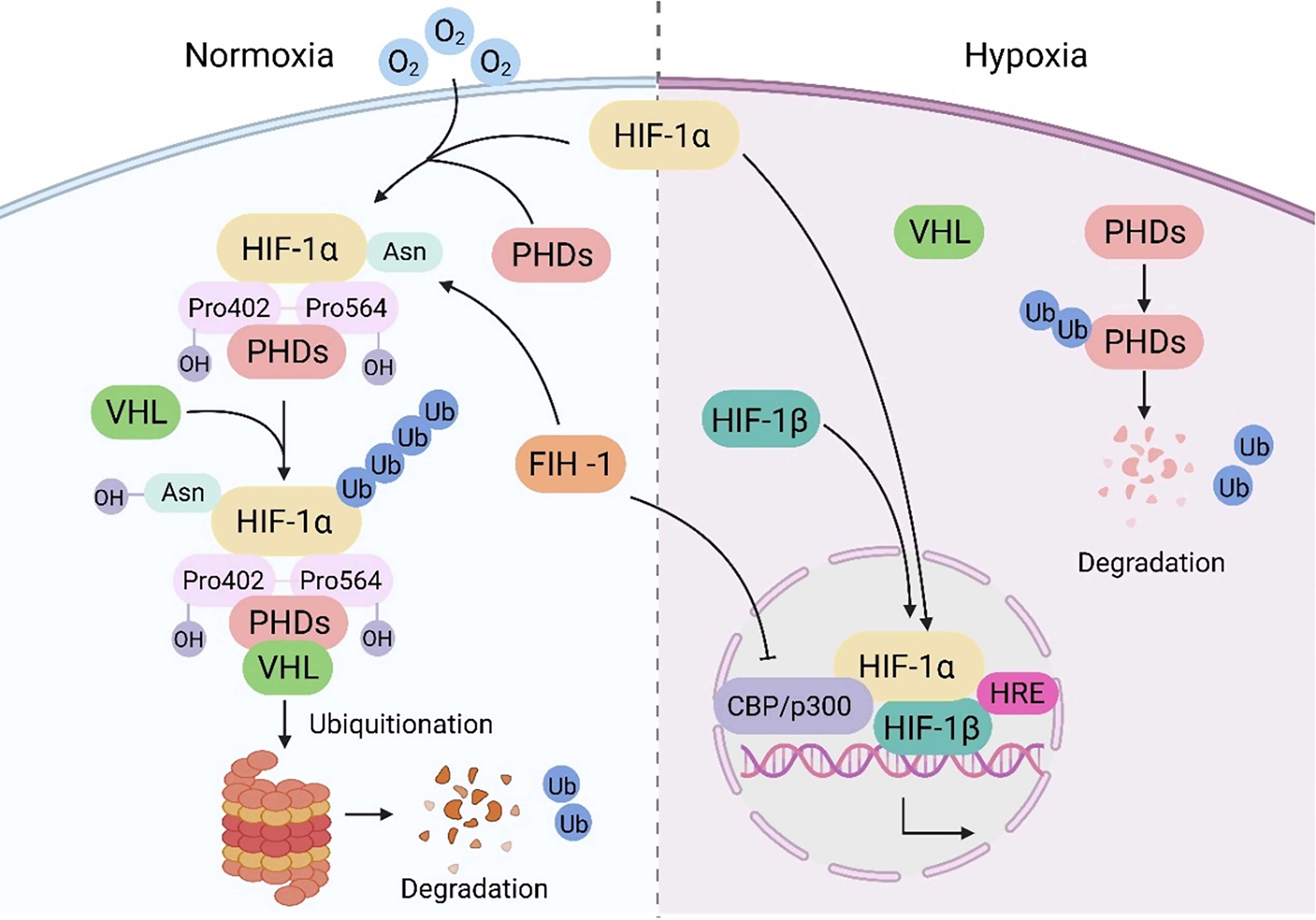
The signaling pathway of HIF under hypoxic and normoxic conditions. Under normoxic conditions, oxygen-dependent PHDs hydroxylate HIF-1α, which is then recognized and ubiquitinated by the VHL protein complex for degradation; under hypoxic conditions, the activity of PHDs is inhibited, the stability of HIF-1α increases, and it translocates to the nucleus to form a heterodimer with HIF-1β, thereby activating the transcription of downstream genes. HIF, hypoxia-inducible factor; VHL, Von Hippel–Lindau; PHDs, prolyl hydroxylases; FIH-1, factors inhibiting HIFs; HRE, hypoxia response elements. Created in https://BioRender.com. (Agreement number: IA29EFQG4C)
At high-altitude hypoxia, HIF signaling shows biphasic regulation: HIF-1α continuously induces erythropoietin, raising red blood cell count and hemoglobin (Sato and Takeda, 2023), and upregulates glucose transporter 1 to enhance glycolysis and preserve cellular energy homeostasis (Kierans et al., 2023). Conversely, excessive HIF-2α activation promotes pulmonary artery smooth muscle proliferation, causing pulmonary hypertension (Semenza, 2012), while HIF-1α synergizes with NF-κB to increase IL-6 and TNF-α, aggravating COPD (Jiang et al., 2010).
Changes in hemodynamics under hypoxic conditions
Long-term exposure to hypoxia at high altitudes can lead to progressive increases in pulmonary artery pressure and pulmonary vascular resistance (Hilty et al., 2016). Studies have shown that among the Xizang population living at altitudes above 4,000 m, the incidence of hypoxic pulmonary hypertension (HPH) and polycythemia is elevated (Groves et al., 1993). Additionally, HPH is commonly observed among the indigenous populations in the highlands of Ecuador and Bolivia (at altitudes of ∼3,500–4,000 m) as well as among children in Colorado, USA (at an altitude of about 3,100 m) (Sime et al., 1963). HPH is an important pathophysiological link in the development of chronic COPD and mainly consists of two stages: hypoxic pulmonary vasoconstriction (HPV) and hypoxic pulmonary vascular remodeling (Chai et al., 2022). HPV is the initiating and primary pathological process of HPH (Chai et al., 2022). HPV is a highly conserved physiological response that plays a crucial role in maintaining the balance of pulmonary ventilation and perfusion. However, continuous hypoxia exposure can lead to excessive activation of HPV, causing pulmonary edema, pulmonary hypertension, and pulmonary vascular remodeling, which in turn adversely affect right ventricular function (Leopold, 2022).
Hypoxia not only induces endothelial cells to release more vasoconstrictive mediators, such as endothelin-1 and platelet-activating factor, to vascular smooth muscle cells but also inhibits the synthesis of vasodilators such as nitric oxide and prostaglandins. It also leads to focal destruction of the endothelial cell basement membrane and increases pulmonary vascular permeability (Yang et al., 2025). In addition, hypoxia activates multiple signaling pathways, such as the MAPK pathway, Rho/ROCK pathway, BMP/TGF-β pathway, and NF-κB pathway, further promoting the proliferation and migration of smooth muscle cells (Mishra et al., 2015; Yang et al., 2025). Endothelial cell dysfunction has a significant impact on the increase in pulmonary vascular tone and vascular remodeling. Although HPV is regulated by the endothelium, pulmonary artery smooth muscle cells (PASMC) are the main effector cells of HPV (Archer et al., 2024).
The mitochondrial oxygen sensor in PASMC is located within the electron transport chain (ETC), particularly in complex I, where NDUFS2 is found. PASMC regulates changes in alveolar oxygen partial pressure by altering the production of reactive oxygen species (ROS) and hydrogen peroxide. Under anoxic conditions, the inhibition of ETC electron transfer leads to a decrease in ROS production, the inactivation of voltage-gated potassium channels (Kv), and the depolarization of PASMC, which promotes the opening of L-type calcium channels (CaL), and the influx of extracellular Ca2+ triggers vasoconstriction (Fig. 2) (Archer et al., 2024; Dunham-Snary et al., 2017; Firth et al., 2011).
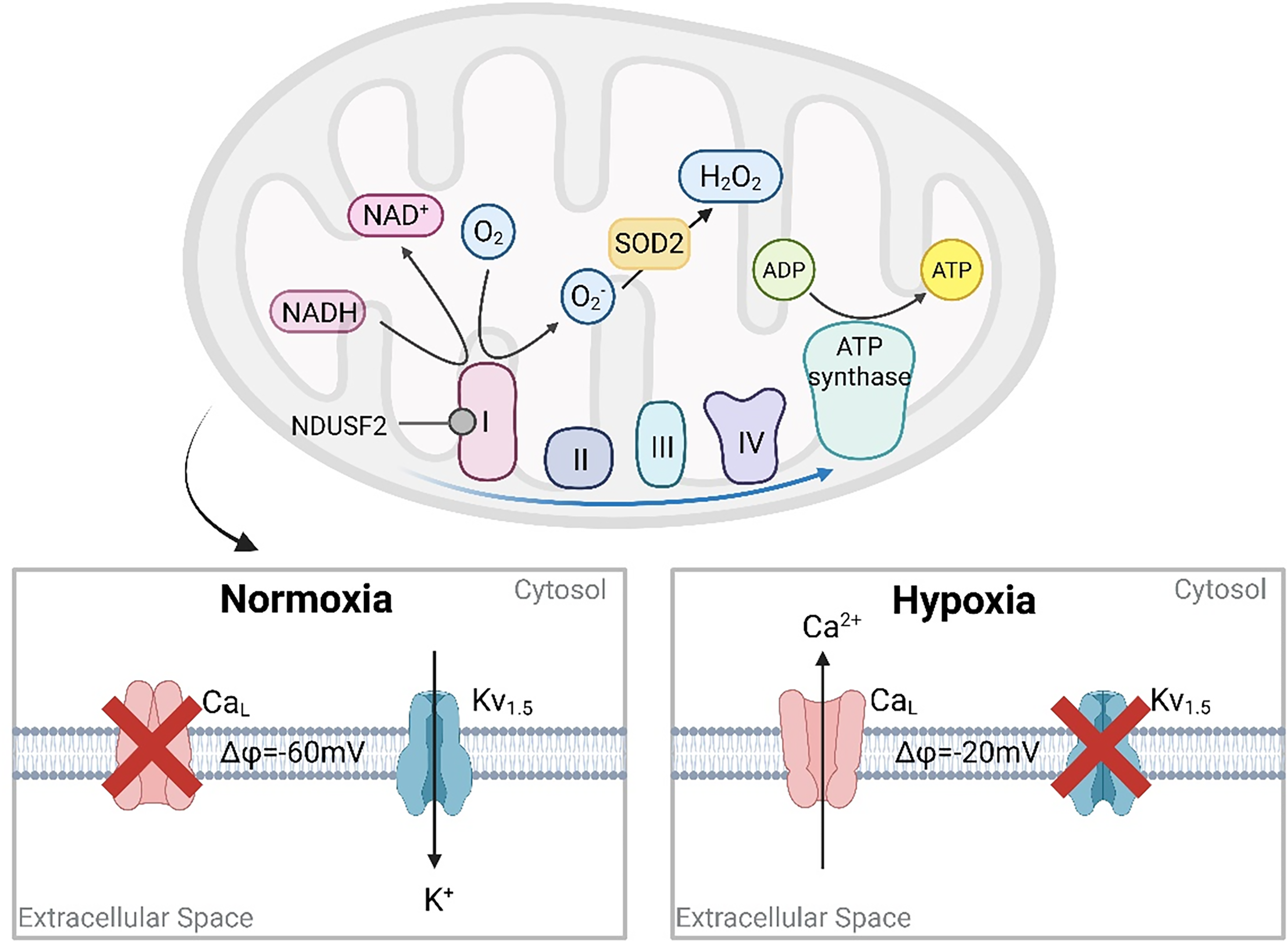
Schematic diagram of oxygen sensing in PASMC mitochondria. Under normoxia, NDUFS2 in mitochondrial ETC complex I generates superoxide, which is converted to H2O2 by SOD2. H2O2 oxidizes and opens Kv channels, allowing K+ efflux, maintaining the cell membrane potential (ΔΨ) at −60 mV, and inhibiting the opening of voltage-gated calcium channels (CaL). Conversely, under hypoxia, limited oxygen prevents H2O2 production, Kv channels close, K+ accumulation increases ΔΨ to −20 mV, stimulating CaL opening, Ca2+ influx, and triggering vascular contraction. PASMC, pulmonary artery smooth muscle cells; ETC, electron transport chain; NADH, nicotinamide adenine dinucleotide; NAD+, nicotinamide adenine dinucleotide; SOD2, superoxide dismutase 2. Created in https://BioRender.com.(Agreement number: HI29EFQG5O)
Furthermore, hypoxia directly increases the expression of vascular endothelial growth factor (VEGF) and EPO by upregulating HIF-1α, inducing angiogenesis and erythropoiesis, and accelerating hemodynamic changes in high-altitude environments (Ji et al., 2024). The aggregation of red blood cells and increased fibrinogen in circulation are important factors affecting blood viscosity, and the increase in blood viscosity reduces the deformability of red blood cells, directly increasing vascular resistance (Zeng et al., 2023). Therefore, the hypoxic environment at high altitudes significantly affects hemodynamics through multiple molecular and cellular mechanisms, leading to pathophysiological changes related to COPD.
Regulation of related genes
The unique low-pressure and hypoxic environment in high-altitude regions can induce gene expression regulation and participate in the pathological process of COPD (Prabhakar and Semenza, 2012). Abnormal expression or mutation of hypoxia-related genes can interfere with key physiological processes such as inflammatory regulation, pulmonary vascular remodeling, and vascular permeability, thereby accelerating the progression of COPD (Prabhakar and Semenza, 2012).
The peroxisome proliferator-activated receptor alpha (PPARA) gene is located on human chromosome 22q13-31 and belongs to the nuclear receptor transcription factor family. It is not only widely expressed in liver tissue but also plays important roles in alveolar epithelial cells, alveolar macrophages (AMs), and bronchial epithelial cells, with alveolar epithelial cells being the main source of PPARA mRNA (Kersten, 2014; Yaribeygi et al., 2020). Studies have found that mutations in PPARA susceptibility loci increase the risk of COPD (Li et al., 2024). During high-altitude adaptation, PPARA, as a downstream key target gene of the HIF pathway, can regulate erythropoiesis, angiogenesis, and oxygen metabolism by interacting with PHDs and HIF-2α, thereby reducing hypoxia-induced damage (Li et al., 2024; Watts and Walmsley, 2019). Specifically, under hypoxic conditions, the activity of PHDs is inhibited, leading to the accumulation of HIF-1α and HIF-2α proteins. After translocation to the nucleus, HIF-2α can upregulate the expression of PPARA and its downstream genes, maintaining cellular homeostasis and reducing the risk of COPD (Semenza, 2020). Research shows that the PPARA agonist WY14643 can activate PPARA, reduce mitochondrial ROS production, and significantly alleviate angiotensin II-induced oxidative stress and inflammatory responses (Liu et al., 2022).
In addition to PPARA, the polymorphism of the SERPINA1 gene is also closely related to the incidence of COPD in high-altitude regions. Sangeetha et al. (2022) analyzed the rs28929474 and rs17580 loci of the SERPINA1 gene and found that specific mutations in this gene were positively correlated with the incidence of COPD, with a more significant impact on high-altitude populations. The SERPINA1 gene is 12.2 kb in length and consists of six introns, four coding exons, and three noncoding exons. Its encoded product, alpha-1 antitrypsin (AAT), plays a crucial role in regulating pulmonary inflammation (Greene et al., 2016). When the lungs are infected or inflamed, neutrophils release elastase, which can degrade elastin in lung tissue and damage alveolar structure; AAT can promptly inhibit elastase activity, thereby maintaining the integrity of alveolar structure and function (Remih et al., 2021). If the SERPINA1 gene is dysfunctional or mutated, it will weaken the protective effect of AAT and increase the risk of COPD.
Genes such as PPARA and SERPINA1 play significant roles in the occurrence and development of COPD in high-altitude areas by regulating hypoxia adaptation, inflammatory responses, and tissue repair processes.
Pathogenic mechanism of indoor air pollution particulate exposure
Exposure to particulate matter (PM) from indoor biomass fuel combustion at high altitudes is a significant risk factor for COPD, especially in households with open stoves, no chimneys, or poor ventilation, and the impact is more pronounced on women (Basagaña, 2019). In areas at an altitude of ≥3,500 m, because of low temperatures, scarcity of wood, and high transportation costs, 63%−83.8% of households mainly use cow and sheep dung cakes as fuel (Duo et al., 2018). Moreover, the lower boiling point of water (e.g., ∼85°C at 3,900 m) necessitates prolonged cooking durations, and combined with incomplete fuel combustion, this results in significantly higher total exposure to indoor pollutants compared with areas at 1,500–3,500 m (Duo et al., 2018). Fine particles in PM can participate in the pathological process of chronic airway diseases by inducing oxidative stress and pulmonary inflammatory cascades (Olloquequi and Silva O, 2016). Toll-like receptors (TLRs), as key sensors of innate immune responses, play a central role in mediating PM immune recognition (Miyata and van Eeden, 2011). Toll-like receptor 2 (TLR2) and Toll-like receptor 4 (TLR4) have been confirmed to be involved in the immune response to PM. PM10 mainly activates AMs through TLR4, inducing the release of pro-inflammatory factors such as IL-6, while PM2.5 relies on TLR2 to mediate the secretion of IL-8 by bronchial epithelial cells (Shoenfelt et al., 2009).
TLRs can activate the MAPK and NF-κB pathways by recruiting the downstream adaptor protein myeloid differentiation marker 88 (MyD88) (Zeng et al., 2023). Studies have shown that PM activates the NF-κB/AP-1 transcriptional complex through the TLR4-MyD88 axis, thereby regulating the expression of downstream inflammation-related genes (Miyata and van Eeden, 2011). Meanwhile, the endotoxin or lipopolysaccharide contained in PM, as a potent activator of the NLRP3 inflammasome (Arias-Pérez et al., 2020), can mediate the maturation and release of IL-1β and IL-18 through the activation of caspase-1 (Sayan and Mossman, 2016). Different particle sizes of PM exhibit specific pro-inflammatory mechanisms: PM2.5 triggers systemic inflammatory responses by activating the NLRP3 inflammasome, significantly increasing the levels of TNF-α, MCP-1, and IL-1β (Allen et al., 2017), while PM10 promotes inflammatory cell infiltration in airway epithelial cells through the NLRP3 pathway and causes the accumulation of ROS by upregulating heme oxygenase-1 expression, ultimately leading to excessive production of inflammatory mediators (Bengalli et al., 2013).
Pathogenic mechanisms of outdoor air pollution exposure
Outdoor air pollution is a potential risk factor for reduced lung function and COPD (Bourbeau et al., 2022). At altitudes of 1,500–3,500 m, due to thin air and strong sunlight, ultraviolet radiation more readily drives photochemical reactions between nitrogen oxides and volatile organic compounds, generating more ozone (O3) (Dütsch, 1970; Wang et al., 2023a), and the O3 concentration shows an upward trend with increasing altitude, approximately increasing by 1 ppb for every 100 m rise (Chevalier et al., 2007), a conclusion also confirmed by the research of Yin et al. (2025). However, in the troposphere at or above 3,500 m, affected by the decrease in air pressure and the concentration of precursors, the O3 concentration enters a plateau or a decline phase (Dütsch, 1970).
As a strong oxidant, excessive exposure to O3 can cause multiple damages to the respiratory system. Studies have shown that O3 can lead to airway wall damage, airway hyperresponsiveness, airway inflammation, and emphysema, among other pathological changes (Sokolowska et al., 2019), and is considered a risk factor for COPD (Xing et al., 2023). Epidemiological data suggest that higher concentrations of O3 increase the number of hospital and emergency department visits for COPD (Hansel et al., 2016).
O3 induces oxidative stress and inflammatory responses through multiple molecular pathways. Wiegman et al. (2020) summarized that O3 exposure increases the release of inflammatory factors such as IL-1α, IL-6, IL-8, CXCL-12, CCL2, ICAM-1, KEAP-1, and macrophage migration inhibitory factor (MIF), and can activate MAPK pathways, TLR, NLRP3 inflammasomes, and NF-κB pathways, further exacerbating the inflammatory response. O3 can induce the gene expression levels of HIF-1α target genes, including histone deacetylase 2, VEGF, Kelch-like erythroid cell-derived protein with CNC homology (ECH)-associated protein 1, and MIF, and significantly increase the activity of nuclear erythroid 2-related factor 2 (Nrf2) (Wiegman et al., 2014). TLR4, MyD88, and toll-interleukin 1 receptor domain-containing adaptor protein may be involved in the inflammatory response induced by O3 (Li et al., 2011). In summary, the pathological effects of O3 can be amplified in high-altitude areas.
Furthermore, research indicates that exposure to toxic substances such as sulfur dioxide (SO2), carbon monoxide (CO), nitrogen dioxide (NO2), and PM significantly increases the outpatient visit rate for respiratory diseases in high-altitude areas (Ning et al., 2024) and can exacerbate the deterioration of COPD (Brunekreef et al., 2021; Cattani-Cavalieri et al., 2025). Among them, the concentrations of SO2 and NO2 released from industrial fuel combustion and vehicle exhaust emissions generally decrease with increasing altitude and approach background values at around 3,500 m (stratosphere) (KURIKO et al., 2009). However, the concentration of CO increases at altitudes between 1,500 and 3,500 m due to incomplete fuel combustion and the inhibition of CO’s chemical oxidation by low temperatures (Thakur et al., 2019) and remains at a high level in areas at or above 5,000 m (McGrath, 1988). The mechanisms by which these pollutants exacerbate COPD deterioration have been preliminarily clarified, involving the regulation of G protein-coupled receptor-mediated cyclic adenosine monophosphate signaling pathways (Cattani-Cavalieri et al., 2024), protein kinase C pathways (Aghaei-Zarch et al., 2023), calcium signaling (Cattani-Cavalieri et al., 2025), and the activation of TLR signaling pathways, which disrupt the lung’s homeostasis and thereby exacerbate COPD deterioration.
Clinical Management of Patients with COPD at High Altitudes
Prevention
At high altitudes, the prevention of COPD can be approached from multiple aspects, such as tobacco management, environmental exposure protection, infection prevention, and health education. First, in high-altitude areas at or above 3,500 m, special attention should be paid to the combustion products generated by residents’ use of solid fuels, while in the altitude range of 1,500–3,500 m, residents are mainly exposed to outdoor air pollution (Basagaña, 2019). To address this, measures such as actively promoting smoking cessation, improving stoves, promoting clean energy to reduce indoor pollution, wearing protective masks when going out, and conducting pollutant detection and early warning can be taken to lower outdoor pollution. Second, flu vaccination markedly lowers the risk of COPD exacerbation (Simon et al., 2023). Moreover, COPD education should be widely disseminated among high-altitude residents to boost awareness of risk factors and promote healthy living. Finally, encourage these residents to undergo pulmonary function testing and strengthen tuberculosis screening.
It is worth noting that long-term exposure to wood smoke from cooking and heating can lead to anthracosis and anthracofibrosis of the lungs and further accelerate the progression of COPD (Comert et al., 2012; Kim et al., 2014). Studies have confirmed that such complications are particularly common among residents living at altitudes above 11,000 feet (Spalgais et al., 2015, 2025a). Therefore, in addition to improving traditional stoves and optimizing the smoke exhaust system, targeted protective measures should also be taken for elderly women living at an altitude of ≥3,500 m (Pérez-Padilla et al., 2010).
Drug therapy and supportive treatment
The drug treatment for COPD mainly focuses on β2 receptor agonists and anticholinergic drugs. The Japanese Respiratory Society’s COPD guidelines recommend that for patients living long-term in high-altitude areas, the combination of long-acting anticholinergic drugs and long-acting β2 agonists (LABA) should be prioritized (Shibata et al., 2023). The Global Initiative for Chronic Obstructive Lung Disease (WHO, 2025) Report further indicates that on the basis of basic bronchodilator treatment, patients with COPD with blood eosinophil counts ≥300 cells/µl or with a history of frequent acute exacerbations should add inhaled corticosteroids (ICS); for patients with low blood eosinophil levels (<100 cells/µl), discontinuing ICS can reduce the incidence of pneumonia (WHO). In China’s high-altitude regions, ∼90% of patients with COPD use ICS-LABA dual therapy, and about 41% of patients use theophylline drugs (Zeng et al., 2023). The formation of this medication characteristic may be related to the preference of primary medical institutions for more economical and clinically experienced dual preparations.
When patients with COPD have chronic high-altitude pulmonary hypertension (HAPH) or elevated pulmonary artery pressure, drugs such as carbonic anhydrase inhibition (acetazolamide), phosphodiesterase-5 inhibitors (Sildenafil, tadalafil), prostacyclin analogs (iloprost, treprostinil), and endothelin receptor antagonists (macitentan, ambrisentan) can be used for treatment (Yang et al., 2025). Studies have confirmed that short-term treatment can reduce the mean pulmonary artery pressure by ∼6–7 mmHg and improve exercise capacity (Titz et al., 2024). And echocardiography is the most commonly used screening method. When the systolic pulmonary artery pressure assessed exceeds 50 mmHg, it is diagnosed as HAPH (Yang et al., 2025). Cardiac magnetic resonance imaging, with its advantages of noninvasiveness, radiation-free, and repeatability, plays a key role in the early diagnosis of HAPH (Chin et al., 2008).
Patients with COPD living in high-altitude areas may still face acute hypoxia stress risks due to short-term altitude changes (such as traveling to higher-altitude regions, traveling between high and low altitudes, etc.). When necessary, preventive acetazolamide and short-term use of dexamethasone can be given to prevent high-altitude pulmonary edema (Bloch et al., 2023). Studies have shown that acetazolamide can alleviate persistent and intermittent nocturnal cerebral hypoxia related to hypoxemia (Schmuziger et al., 2025); dexamethasone is most effective in areas above 4,000 m, with a recommended dose of 8–16 mg/day (Burtscher et al., 2025).
The hypoxic environment at high altitudes significantly affects drug absorption, distribution, and metabolism. First, hypoxia can lead to a decrease in blood flow to the gastrointestinal mucosa and delayed gastric emptying, thereby reducing the bioavailability of orally administered drugs (Szabo et al., 1985). Therefore, clinical efficacy monitoring needs to be strengthened. Second, under hypoxic conditions, blood viscosity and hematocrit increase, resulting in an increase in the apparent volume of distribution (Vd) of drugs (Siebenmann et al., 2017). Animal experiments further confirmed that the Vd of salbutamol increased by approximately twice after hypoxia (p < 0.05), and the area under the plasma concentration-time curve also significantly increased (p < 0.05), indicating that both the distribution and exposure levels of drugs in the body are affected (Perreault et al., 1995). In addition, hypoxia can also inhibit the activity of cytochrome P450 enzyme systems (such as CYP3A4 and CYP1A2), leading to a slower rate of drug metabolism and clearance. For example, in a high-altitude environment, the bioavailability of aminophylline can increase to 1.35 times its original level, and the clinical dose needs to be reduced accordingly to prevent adverse reactions such as arrhythmia caused by excessively high blood drug concentrations (Zizhao et al., 2020).
In terms of oxygen therapy, the high-altitude environment exacerbates the decline in nocturnal blood oxygen saturation (SpO2) in patients with COPD. Studies have confirmed that implementing nocturnal oxygen therapy (3 l/min) for patients with COPD living at an altitude of 2,048 m can increase SpO2 by 9% (Tan et al., 2020). For every increase of ∼500 m in altitude, the resting SpO2 of healthy adults decreases by an average of 1%–2%. Specifically, at 1,500 m, it is ∼96%, at 2,500 m, it is ∼94%, and at 3,500 m, it is ∼91% (Rojas-Camayo et al., 2018). Therefore, for patients with COPD living in high-altitude areas, the threshold for initiating oxygen therapy should be appropriately raised: within the range of 1,000–3,000 m, oxygen inhalation is recommended when SpO2 is below 90%–88%; at altitudes above 3,000 m, oxygen supplementation treatment should be initiated immediately when SpO2 is less than 85% (Avila-Hilari et al., 2024). The technical and resource requirements for treating COPD in high-altitude areas are highly consistent with the actual conditions in remote areas.
It is worth noting that high altitude is an important risk factor for polycythemia in patients with COPD (Zhang et al., 2021). Regular phlebotomy (about 300–500 ml each time) is an effective intervention for secondary polycythemia, which can reduce blood viscosity and improve microcirculation function. Studies have shown that after isovolemic hemodilution, blood viscosity decreases by ∼30%, hemoglobin decreases by about 14%, and flow-mediated dilation levels significantly increase, indicating that the reduction in blood viscosity has a reversible improvement effect on vascular function (Tremblay et al., 2019). Therefore, standardized phlebotomy can effectively alleviate the clinical symptoms of chronic mountain sickness and COPD by significantly reducing blood viscosity and improving cardiopulmonary load (Martinez et al., 1997; Villafuerte and Corante, 2016).
Rehabilitation therapy
The International Society of Physical and Rehabilitation Medicine includes COPD as an important component of pulmonary rehabilitation (PR) treatment. Studies have shown that implementing comprehensive PR (including exercise training, respiratory physiotherapy, climate therapy, etc.) for patients with COPD at high altitudes can significantly improve lung function, enhance exercise endurance, and alleviate breathing difficulties (p < 0.001) (Kubincová et al., 2018). Targeted training of respiratory muscles, especially inspiratory muscles, effectively enhances patients’ aerobic metabolic capacity, thereby improving gas exchange efficiency and alleviating breathing difficulties (Yu et al., 2021). At the same time, intervention in an oxygen-rich environment at high altitudes can significantly improve the partial pressure of oxygen and SpO2 during exercise in high-altitude populations by increasing the fraction of inspired oxygen (Cui et al., 2003).
However, in high-altitude environments, the reduced oxygen supply can exacerbate symptoms and limit exercise capacity, posing a challenge for patients to adhere to rehabilitation programs (Fan and Wang, 2025). Villamil-Parra’s (2024) research shows that in the hypoxic environment of high altitudes, the physical activity level of patients with COPD is significantly lower than that of healthy people at the same altitude, as indicated by a 61.32% decrease in hourly calorie consumption, a 9.64% reduction in hourly metabolic equivalent, and a 139.41% decrease in average daily steps. Relocation to low-altitude areas can significantly increase patients’ blood oxygen levels and enhance their exercise endurance. Therefore, personalized assessment of patients with COPD is necessary to develop individualized rehabilitation strategies, including low-to-moderate intensity aerobic exercise (Su et al., 2024), resistance training (Nolan and Rochester, 2019), high-intensity interval training (Gao et al., 2022), and nutritional support (Fan and Wang, 2025).
In addition, moving to a lower altitude is an effective measure for high-altitude patients with COPD to reduce pulmonary arterial hypertension, improve blood oxygen levels, and lower the risk of acute exacerbation (Stream et al., 2009). Studies have shown that on the second day after relocating high-altitude residents with a risk of pulmonary arterial hypertension from 3,250 m to 760 m, their blood oxygen content significantly increased (p < 0.001), and systolic pulmonary artery pressure (SPAP) and total pulmonary resistance decreased (p < 0.001), indicating that the HPV at low altitude is rapidly reversible (Vella et al., 2025). Although the effect of moving to a lower altitude is significant, individualized decisions should be made in combination with the patient’s social support system, medical accessibility, and psychological adaptability.
Conclusions
High-altitude environments, characterized by hypoxia, cold, and distinct pollution profiles, exert complex impacts on COPD. Epidemiologically, COPD mortality consistently rises with altitude, yet its prevalence shows conflicting associations (positive, negative, or nonsignificant), attributed to varied diagnostic criteria, genetic adaptations, and socioeconomic disparities. Pathophysiologically, hypoxia-driven mechanisms, hemodynamic alterations, genetic polymorphisms, and air pollution underpin COPD progression. Clinically, a comprehensive management approach combining prevention, medication, support, and rehabilitation should be adopted. However, the changes in drug metabolism and poor compliance with rehabilitation treatment remain urgent challenges to be addressed. Future research should further clarify its pathogenesis through multicenter collaboration, optimize prevention and treatment strategies to improve patient prognosis, and conduct systematic reviews based on altitude stratification to provide more solid evidence-based support for precise intervention.
Authors’ Contributions
S.W. was responsible for conceiving this review article. S.W. and X.L. participated in discussions and provided constructive feedback on the final version of the article. S.W. and X.L. reviewed and revised the review article for intellectual content and approved the final version for submission.
Footnotes
Author Disclosure Statement
The authors declare that this review was conducted without any financial interests. No personal interests to disclose.
Funding Information
This work was supported by the National Natural Science Foundation of China (82460009) and the Gansu Province Key Research and Development Program (22YF7FA083).