
Abstract
Background:
This study examined the effects of chronic high-altitude hypoxic exposure on attention networks in indigenous primary school students, integrating cardiovascular indices to explore underlying physiological mechanisms.
Methods:
Three real-world altitude groups were established: low (2,200 m), mid (3,200 m), and high (4,200 m). Cardiovascular function was assessed via systolic blood pressure, diastolic blood pressure, and heart rate. Attentional performance was evaluated using the Attention Network Test (ANT), which provides measures of alerting, orienting, and executive control efficiency.
Results:
Cardiovascular indices followed a nonlinear pattern across altitudes, with systolic blood pressure, diastolic blood pressure, and heart rate being significantly higher at mid-altitude compared to both low and high altitudes. In contrast, attention performance exhibited an opposite trend: alerting and executive control efficiency were relatively reduced at mid-altitude but were comparable between the low- and high-altitude groups. Orienting efficiency did not differ significantly across the three altitude groups.
Conclusions:
The findings reveal a dissociation between physiological regulation and cognitive performance under chronic hypoxia. To explain these results, we propose a U-shaped model of cardiovascular adaptation, where mid-altitude represents an incomplete compensatory state, while prolonged exposure at higher altitudes leads to stabilized cardiovascular function and preserved attentional performance. This integrative framework underscores the crucial role of physiological adaptation in shaping cognitive outcomes in high-altitude environments.
Keywords
Introduction
Attention refers to the mental process by which individuals selectively direct and sustain cognitive resources toward specific objects or events, thereby enabling clearer perception, more accurate responses, and goal-directed behavior (Peng, 2023). It constitutes a fundamental psychological prerequisite for knowledge acquisition, skill learning, and the successful execution of complex cognitive and practical activities (Peng, 2023). From an information-processing perspective, attention involves the active selection, enhancement, and processing of task-relevant information while suppressing irrelevant or distracting inputs (Peng, 2023).
Early theoretical accounts often conceptualized attention as a unitary system; however, such models proved insufficient to explain the diversity and complexity of attentional phenomena observed in behavioral and neurophysiological research. To address this limitation, Posner and colleagues proposed the attention network model, which posits that attention consists of three functionally and anatomically dissociable but interacting subnetworks: alerting, orienting, and executive control (Fossella et al., 2002; Posner and Petersen, 1990). The alerting network supports the maintenance of a vigilant state and readiness to respond to incoming stimuli; orienting refers to the ability to direct attention to target stimuli; and the executive control network is responsible for conflict monitoring, response inhibition, and top-down regulation of behavior. The coordinated operation of these subnetworks determines overall attentional efficiency (Posner and Petersen, 1990).
Importantly, these three attention subnetworks differ in their neural substrates and metabolic demands. The alerting and executive control networks rely heavily on frontal–parietal and prefrontal–cingulate circuits that are densely interconnected and energetically costly (Posner and Petersen, 1990; Ma et al., 2017), whereas the orienting network primarily involves posterior parietal regions with comparatively lower metabolic requirements (Posner and Petersen, 1990). This neurofunctional heterogeneity suggests that attention subnetworks may exhibit differential vulnerability to physiological stressors—particularly chronic hypoxia—which disproportionately affects brain regions with high oxygen and energy demands. Based on Posner’s model, Fan et al. developed the Attention Network Test (ANT), which integrates cueing and flanker paradigms to quantify the efficiency of each attention subnetwork within a single experimental framework (Fan et al., 2002). The ANT has been widely validated as a reliable and sensitive tool for assessing attentional function across developmental and clinical populations (Wang et al., 2015).
From a medical and physiological perspective, altitude is defined primarily by its effects on oxygen availability. Empirical evidence indicates that at altitudes below ∼2,500 m, arterial oxygen saturation typically remains above 92%, whereas oxygen saturation declines progressively at higher elevations, increasing the likelihood of hypoxia-related physiological stress (Luks and Hackett, 2022). Accordingly, regions above 2,500 m are commonly classified as high-altitude environments in medical research (Xiao, 2004), with altitude ranges often categorized as low altitude (500–1,500 m), moderate altitude (1,500–2,500 m), high altitude (2,500–4,500 m), very high altitude (4,500–5,500 m), and extreme altitude (>5,500 m) (Ge, 1997). As a highly metabolically active organ, the brain consumes ∼20%–25% of the body’s total oxygen supply at rest, a proportion that can exceed 25% during cognitively demanding tasks (Williams and Leggett, 1989). This pronounced oxygen dependence raises a critical question: How does chronic exposure to high-altitude hypoxia influence cognitive functioning, particularly attention?
Evidence from acute and simulated high-altitude exposure studies consistently indicates that hypoxic environments at high altitude adversely affect multiple cognitive domains, including attention (Virués-Ortega et al., 2004; Stivalet et al., 2000), memory (de Aquino Lemos et al., 2012), thinking (Evans and Witt, 1966), and executive control (An et al., 2017). Moreover, these cognitive impairments tend to become more pronounced with increasing altitude and greater hypoxic severity (Meng et al., 2023; Wang et al., 2015). In contrast, studies focusing on long-term high-altitude residents have reported mixed findings. Some investigations have found no significant cognitive differences between indigenous high-altitude populations and low-altitude controls. For example, Hogan et al. observed comparable visual memory performance in adolescents living at 3,700 m and those at low altitude (Hogan et al., 2010), while Richardson et al. reported no differences in overall cognitive abilities between high- and low-altitude adolescents (Richardson et al., 2011). Similarly, Barkaszi et al. found that after a 6-week stay at 3,233 m, participants exhibited no significant changes in attention network efficiency as measured by the ANT, suggesting functional adaptation to chronic hypoxic exposure (Barkaszi et al., 2016). Neurophysiological evidence further supports the possibility of compensatory mechanisms under chronic hypoxia. For instance, Wang et al. (2020) reported that young adults residing at 3,650 m for 3 years exhibited bilateral occipital activation and reduced hemispheric lateralization during early attentional processing, in contrast to unilateral activation patterns observed in low-altitude controls. This bilateral recruitment was interpreted as a compensatory neural strategy to meet task demands under hypoxic stress (Wang et al., 2014).
Taken together, existing research presents an apparent paradox: While acute or short-term hypoxic exposure often impairs attention, long-term residence at high altitude may be associated with preserved or compensated attentional functioning. However, several critical gaps remain. First, much of the literature emphasizes acute or simulated exposure, whereas fewer studies have examined chronic hypoxia under natural living conditions. Second, children—whose brains are undergoing rapid structural and functional development and may be particularly sensitive to environmental stressors—have received comparatively little attention. Third, most studies focus exclusively on behavioral or neural outcomes, with limited integration of physiological systems that are central to hypoxic adaptation.
In addition to its direct effects on cognition, chronic high-altitude hypoxia places sustained demands on the cardiovascular system. Long-term exposure has been shown to alter heart rate regulation and blood pressure through sympathetic activation and adaptive cardiovascular remodeling, processes that may influence cerebral perfusion and oxygen delivery. A substantial body of research indicates that indigenous high-altitude populations develop distinctive cardiovascular adaptations to chronic hypoxia, including modulation of hypoxia-inducible factor (HIF) pathways, enhanced nitric-oxide-mediated vasodilation, and more efficient oxygen transport mechanisms (Beall, 2007; Simonson et al., 2010). These adaptations are thought to attenuate excessive sympathetic activation and stabilize blood pressure and heart rate under sustained hypoxic stress. Yet, few studies have examined attention network functioning and cardiovascular regulation within a unified framework, particularly among indigenous children living at different altitudes under natural conditions. To address these limitations, the present study established three real-world altitude groups—low (2,200 m), moderate (3,200 m), and high (4,200 m)—and employed the ANT to dissociate alerting, orienting, and executive control functions (Fan et al., 2002). By integrating behavioral measures of attention with cardiovascular indicators, this study aimed to systematically investigate how chronic high-altitude exposure across distinct altitude gradients influences attention network efficiency and its physiological correlates in indigenous high-altitude primary school students.
Methods and Procedures
Participants
A total of 300 fourth-grade students were initially recruited from three high-altitude regions in Qinghai Province, China: Zhiduo County (Yushu Prefecture; 4,200 m), Gangcha County (Haibei Prefecture; 3,200 m), and Guide County (Hainan Prefecture; 2,200 m). For convenience, the three groups are hereafter referred to as the low-altitude (2,200 m), mid-altitude (3,200 m), and high-altitude (4,200 m) groups. All participants were indigenous Tibetan children who were born and raised locally and attended ethnic boarding elementary schools in their respective regions. To ensure data quality, participants whose overall task accuracy in the ANT was more than three standard deviations below the grand mean accuracy (calculated across all participants) were excluded from further analysis. Based on this criterion, 28 participants were excluded (Guide County: 11; Gangcha County: 8; Zhiduo County: 9). The final sample therefore consisted of 89 students in the low-altitude group, 92 in the mid-altitude group, and 91 in the high-altitude group. Geographical characteristics and demographic information for the final sample are presented in Table 1. All participants were right-handed and physically healthy. None reported a history of neurological disorders, psychiatric conditions, or sensory impairments. Right-handedness was required to reduce potential variability related to hemispheric lateralization in attentional processing. The study was approved by the local education authorities and school administrations. Written informed consent was obtained from parents or legal guardians, and all participants provided assent prior to participation.
Basic Information of Participants

All participants were indigenous Tibetan children born and raised in their respective regions.
Cardiovascular indicators and ANT
Before the ANT, the Chinese version of the Standard Raven’s Progressive Matrices (SPM; Set A–E) was administered to assess general nonverbal cognitive ability, along with participants’ blood oxygen saturation, blood pressure, and heart rate. The Chinese standardized version was used in accordance with age-appropriate norms for primary school students. Blood pressure and heart rate were assessed using a portable electronic blood pressure monitor (Yuwell, Jiangsu Yuyue Medical Equipment & Supply Co., Ltd., China). Measurements were conducted in a quiet room under standardized conditions. Participants were instructed to sit quietly for at least 5 minutes before measurement. Blood pressure and heart rate were measured three consecutive times at 1–2 minute intervals on the right upper arm in a seated position, and the mean of the three readings was used for subsequent analyses.
The ANT was programmed and administered using E-Prime 3.0 (Psychology Software Tools, Pittsburgh, PA). The experimental procedure followed the standard ANT paradigm described by Fan et al. (2002), and the workflow is illustrated in Figure 1. Each trial began with a central fixation cross presented continuously throughout the experiment. Cue stimuli (no-cue, central-cue, or spatial-cue) were presented for 200 ms. Following a random stimulus-onset asynchrony of 300–1,450 ms between cue offset and target onset, the target stimulus appeared and remained on the screen until a response was made or until a maximum response window of 2,000 ms elapsed. The experimental design included three cue types (no-cue, central-cue, spatial-cue) and two stimulus types (congruent and incongruent). In the congruent condition, all five arrows pointed in the same direction; in the incongruent condition, the central arrow pointed in the opposite direction to the flanking arrows.
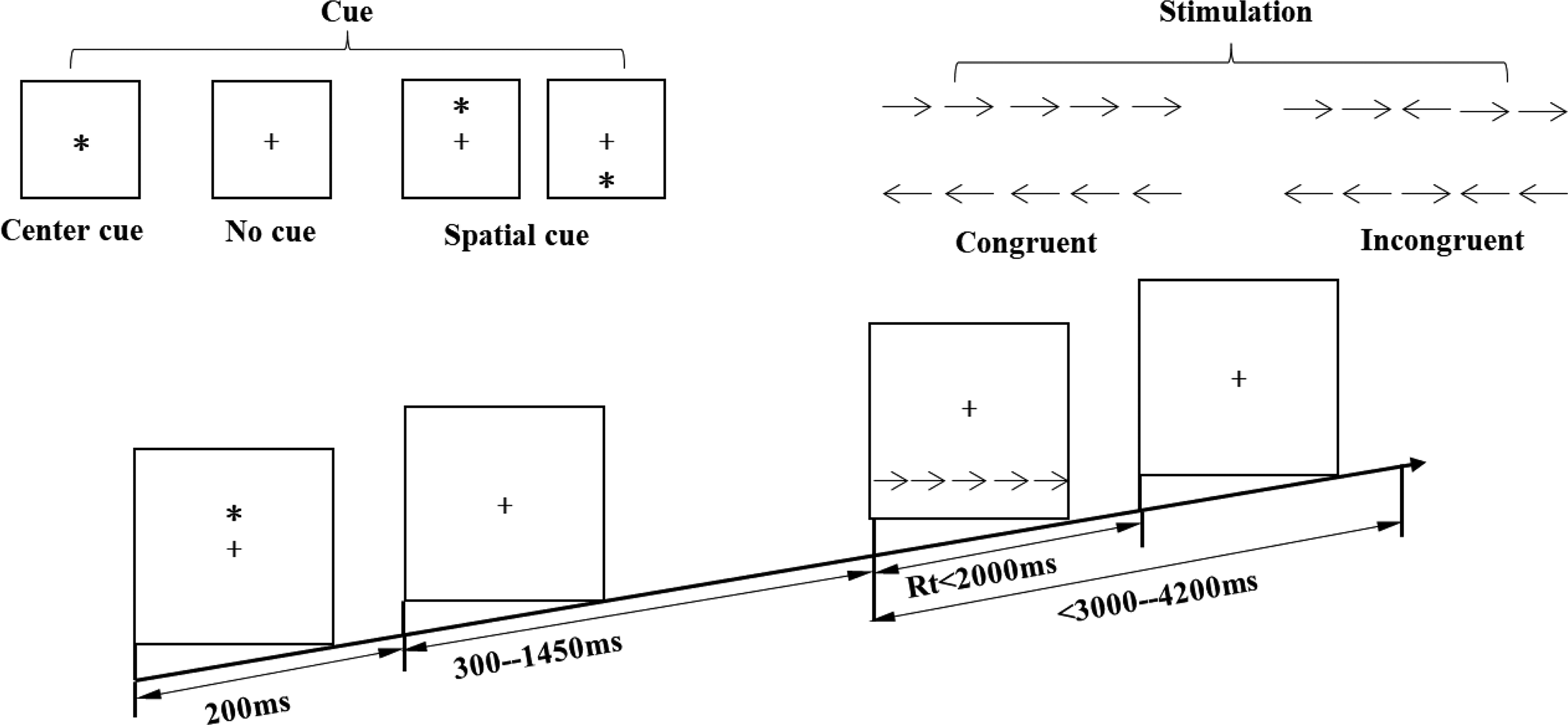
Experimental flowchart of the attention network test.
All stimuli were presented on a uniform gray background, with arrows displayed in white. Visual angles were calculated based on a fixed viewing distance of ∼60 cm. The visual angle of a single arrow was 0.58°, the spacing between adjacent arrows subtended 0.06°, and the entire five-arrow array subtended 3.27° of visual angle. The arrow array was presented either 1.06° above or below the central fixation point and pointed either left or right. Stimuli were displayed on a 19-inch LCD monitor with a screen resolution of 1,920 × 1,080 pixels and a refresh rate of 60 Hz. Participants were tested individually in a quiet room under standardized lighting conditions. The experiment adopted a block design consisting of six experimental conditions (3 cue types × 2 stimulus types), which appeared with equal probability within each block. The task comprised two blocks of 108 trials each, yielding a total of 216 trials. Participants were instructed to respond as quickly and accurately as possible to the direction of the central arrow by pressing the “F” key for left-pointing arrows and the “J” key for right-pointing arrows. Prior to the formal experiment, participants completed a practice session consisting of 24 trials covering all cue and stimulus conditions. Participants were allowed to proceed to the formal experiment once they demonstrated an understanding of the task and achieved an accuracy rate of at least 80% during practice.
Attention network scores were calculated as follows: alerting score = mean reaction time (RT) in the no-cue condition minus RT in the central-cue condition (larger values indicate better alerting efficiency); orienting score = RT in the central-cue condition minus RT in the spatial-cue condition (larger values indicate better orienting efficiency); executive control score = RT in the incongruent condition minus RT in the congruent condition (smaller values indicate better executive control efficiency) (Fan et al., 2002).
Statistical methods
Statistical analyses were conducted using SPSS Statistics 27.0 (IBM, Somers, NY, USA). Descriptive statistics are reported as mean ± standard error. The significance level was set at p < 0.05 (two-tailed). Prior to statistical analysis, RT data were screened to remove outliers following standard procedures in attention research. Trials with incorrect responses were excluded. For correct trials, RTs shorter than 200 ms or longer than 2,000 ms (corresponding to the predefined response window) were discarded. Altitude group served as the between-subjects independent variable. Cardiovascular indicators (blood oxygen saturation, heart rate, systolic and diastolic blood pressure) and the efficiency scores of the three attention networks (alerting, orienting, and executive control) were treated as dependent variables. One-way analysis of variance (ANOVA) was conducted separately for each cardiovascular indicator and each attention network efficiency score. When a significant main effect of altitude was observed, post hoc pairwise comparisons were performed using the Bonferroni correction to control for multiple comparisons (Zhou et al., 2011). Associations between cardiovascular indicators and attention network efficiency scores were examined using Pearson’s product–moment correlation coefficients, as all variables satisfied assumptions of normality and linearity. Correlation strength was interpreted according to conventional criteria: |r| ≈ 0.10 was considered small, |r| ≈ 0.30 moderate, and |r| ≥ 0.50 large. Where appropriate, effect sizes (partial η2 for ANOVA) were reported to quantify the magnitude of group differences.
Results
Results of Standard Raven’s Progressive Matrices
The results of the Standard Raven’s Progressive Matrices indicated that the mean scores for the low-, mid-, and high-altitude groups were 29.50 ± 4.80, 29.10 ± 4.60, and 28.90 ± 5.10, respectively. A one-way ANOVA revealed no significant difference in Raven’s scores among the three groups, F(2, 269) = 0.58, p = 0.56, ηp2 = 0.004, indicating that the participants were homogeneous in terms of general cognitive ability.
Results of cardiovascular indicators
Cardiovascular indicators of blood oxygen saturation, blood pressure, and heart rate for the three altitude groups are presented in Table 2. One-way ANOVA on cardiovascular indicators across the three altitude groups revealed the following (Fig. 2):
Participants’ Cardiovascular Indicators in the Three-Altitude Groups (M ± SD)
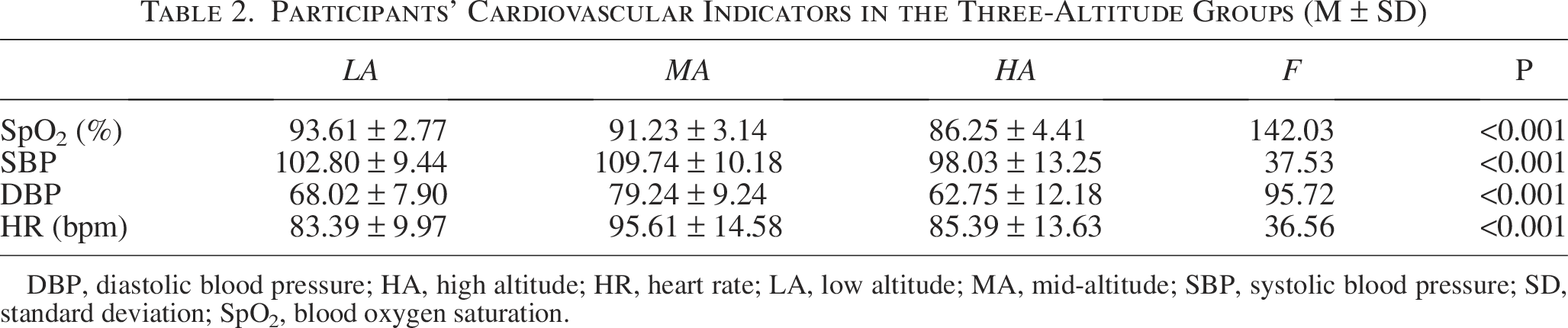
DBP, diastolic blood pressure; HA, high altitude; HR, heart rate; LA, low altitude; MA, mid-altitude; SBP, systolic blood pressure; SD, standard deviation; SpO2, blood oxygen saturation.
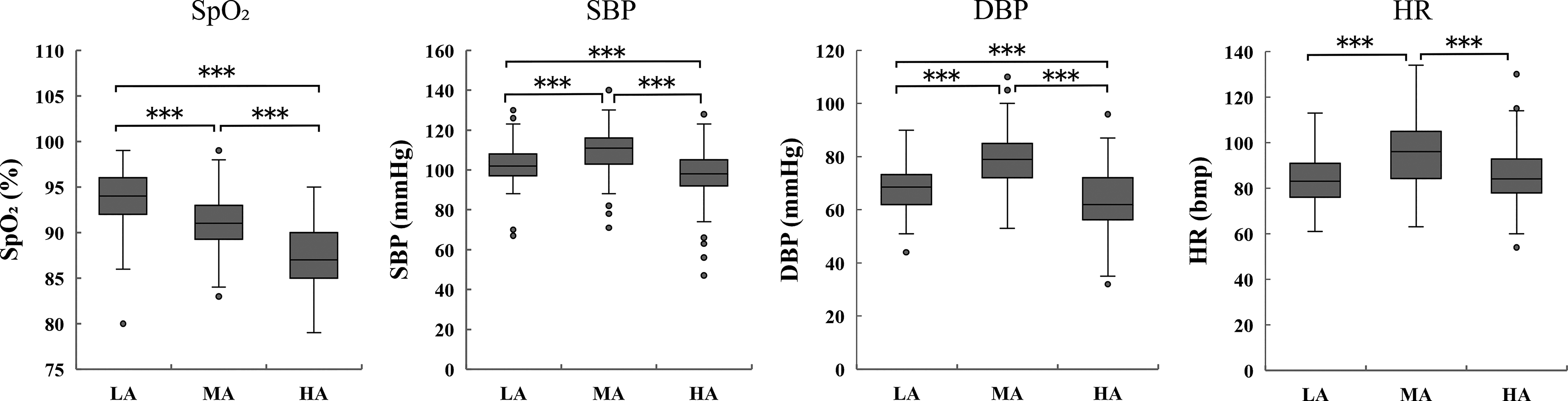
Cardiovascular indicators comparisons across high-, mid-, and low-altitude groups.
Results of attention network
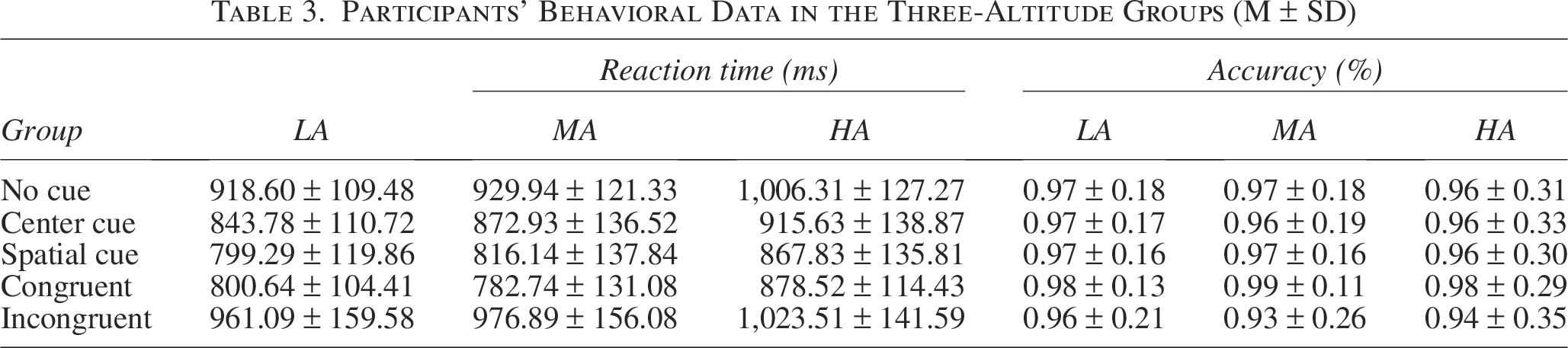
The mean RTs and accuracy rates for each experimental condition are shown in Table 3, and the efficiency scores of the three attention subnetworks are presented in Table 4. One-way ANOVA on the attention network efficiency scores across the three altitude groups revealed the following (Fig. 3):
Participants’ Behavioral Data in the Three-Altitude Groups (M ± SD)
Participants’ Attention Network Scores in the Three-Altitude Groups (M ± SD)


Attentional network performance: comparative analysis of alerting, orienting, and executive control across high-, mid-, and low-altitude groups.
Correlations between cardiovascular indicators and attention network scores
Results from cardiovascular indicator analysis showed that blood pressure (diastolic and systolic) and heart rate all exhibited a nonlinear “higher in the mid-altitude, lower at low and high altitudes” pattern, with the mid-altitude group significantly higher than the other two groups. Analysis of attention network functions revealed a contrasting nonlinear distribution for alerting and executive control functions, characterized by “lower in the mid-altitude, higher at low and high altitudes”—this suggests a potential negative association between cardiovascular indices and alerting/executive control functions. To validate this association, we conducted correlation analyses between cardiovascular indicators and network efficiency scores (Table 5). Results showed that diastolic blood pressure, systolic blood pressure, and heart rate were all positively correlated with executive control network scores, while diastolic blood pressure was significantly negatively correlated with alerting network scores.
Correlations Between Cardiovascular Indicators and Attentional Network Scores
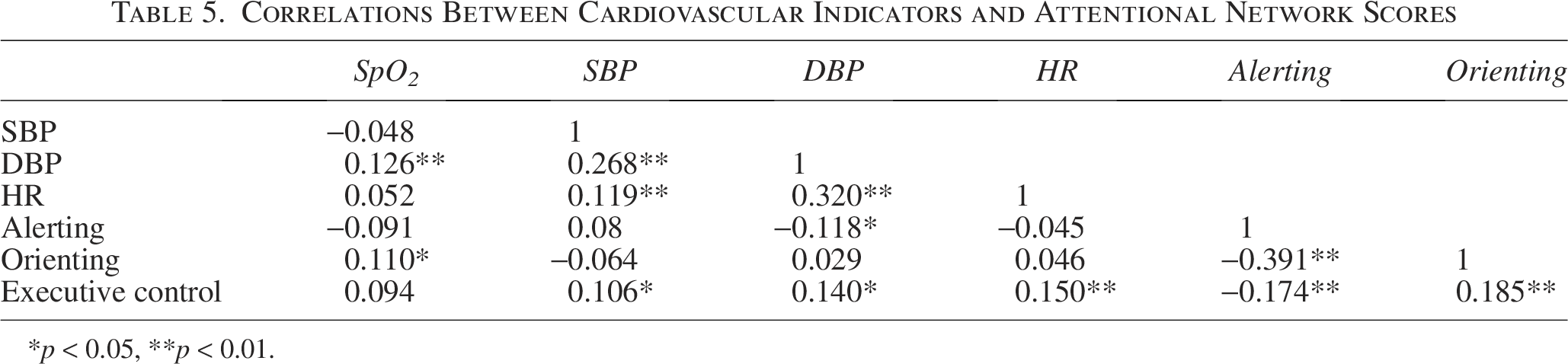
*p < 0.05, **p < 0.01.
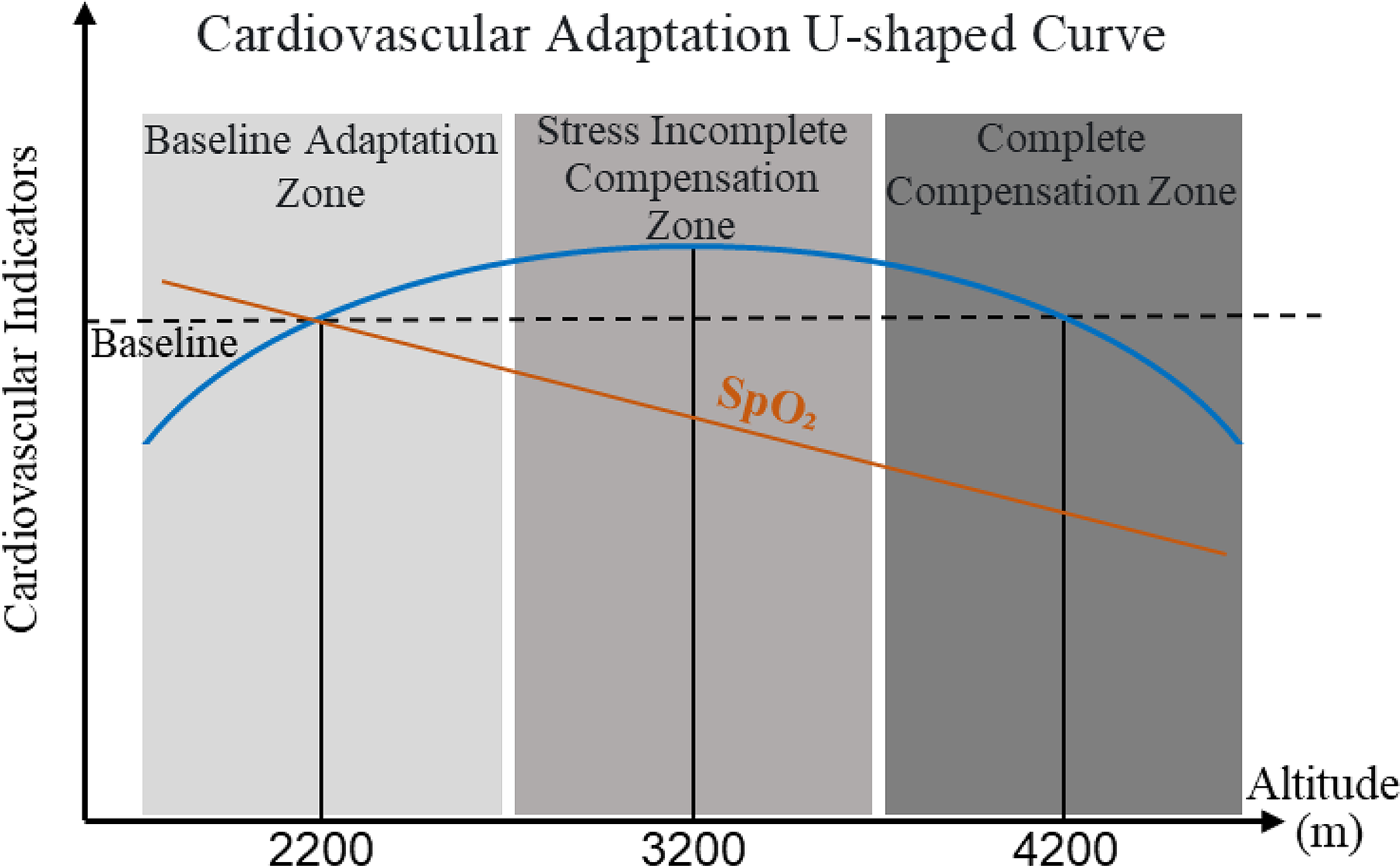
Schematic diagram of the U-shaped curve for cardiovascular adaptation.
Discussion
By establishing three real-world altitude groups—low (2,200 m), mid (3,200 m), and high (4,200 m)—the present study integrated physiological indices with the ANT paradigm to examine how chronic high-altitude hypoxic exposure shapes cardiovascular regulation and attention network functioning in indigenous high-altitude primary school students. A central contribution of this study is the identification of a nonlinear, U-shaped pattern of cardiovascular regulation across altitude, which provides a physiological framework for interpreting the observed patterns of attentional performance under chronic hypoxic stress.
Discussion of cardiovascular indicators: a U-shaped model of cardiovascular regulation
Physiological analyses revealed that blood oxygen saturation declined monotonically with increasing altitude across the three groups, which is consistent with well-established principles of high-altitude hypoxic physiology and previous empirical findings (Pang et al., 2023). In contrast, systolic blood pressure, diastolic blood pressure, and heart rate exhibited a clear nonlinear pattern, characterized by significantly higher values in the mid-altitude group compared with both the low- and high-altitude groups, forming an inverted U-shaped distribution across altitude.
Previous research indicates that sympathetic nervous system activity increases markedly within the altitude range of ∼3,000–4,000 m as an acute and subacute response to hypoxic stress, aiming to preserve oxygen delivery through increased cardiac output and vascular tone. However, when such sympathetic activation is not accompanied by sufficiently efficient oxygen transport or vascular adaptation—such as increases in hemoglobin concentration or improvements in microvascular regulation—it may fail to counteract hypoxia effectively and instead increase cardiovascular load, leading to elevated blood pressure and heart rate (Virués-Ortega et al., 2004; Simonson et al., 2010). Within this framework, the significantly higher cardiovascular indices observed in the mid-altitude group likely reflect an incomplete compensatory state, characterized by heightened physiological stress but limited regulatory efficiency. By contrast, indigenous high-altitude populations have been shown to exhibit genetic and phenotypic adaptations that support long-term cardiovascular stabilization under chronic hypoxic conditions. These adaptations include altered HIF signaling (e.g., EPAS1-related pathways), nitric-oxide-mediated vasodilation, and attenuation of excessive sympathetic tone, all of which contribute to more efficient oxygen delivery and reduced cardiovascular strain (Beall, 2007; Simonson et al., 2010). Although genetic, hematological, or biochemical markers (e.g., hemoglobin concentration, erythropoietin levels) were not directly measured in the present study, the comparatively lower blood pressure and heart rate observed in the high-altitude group—despite lower blood oxygen saturation—are consistent with a state of more efficient long-term physiological compensation. This interpretation should be regarded as a plausible explanation derived from the observed physiological patterns rather than as direct evidence of specific genetic mechanisms.
Based on these findings, we propose a U-shaped model of cardiovascular regulation under chronic hypoxic exposure, in which cardiovascular indicators such as blood pressure and heart rate show an inverted U-shaped relationship with altitude (Fig. 4):
Overall, the proposed U-shaped model captures the dynamic and nonlinear nature of cardiovascular adaptation to chronic hypoxic environments. Importantly, this physiological framework provides a coherent basis for interpreting the altitude-related patterns observed in attention network performance, which are discussed in the following section. At the same time, the model should be viewed as a hypothesis grounded in converging physiological evidence and warrants further validation using direct genetic, hematological, and neurophysiological measures in future studies.
Discussion of attention network results in light of the U-shaped model
Using the ANT, the present study examined altitude-related differences in the efficiency of the orienting, alerting, and executive control networks. In line with the physiological findings described above, both the alerting and executive control networks exhibited a nonlinear pattern across altitude groups, whereas the orienting network remained relatively stable. These findings suggest differential sensitivity of attention subnetworks to chronic hypoxic stress and its associated cardiovascular regulation.
Taken together, the ANT results indicate that chronic hypoxic exposure is not associated with a uniform decline across all attention subnetworks. Instead, alerting and executive control functions show a shared nonlinear pattern characterized by relatively reduced efficiency at mid-altitude, whereas orienting remains resilient across altitude levels. When interpreted in light of the U-shaped cardiovascular regulation model, these findings suggest that attentional performance in children living at different altitudes may be shaped not solely by oxygen availability per se, but by the efficiency of physiological and cardiovascular compensation to chronic hypoxic stress. Importantly, these interpretations remain tentative and should be tested in future studies incorporating direct neurophysiological and hematological measures.
Relationships between cardiovascular indices and attention networks
Across the three altitude groups, cardiovascular indices and attention network performance exhibited opposite nonlinear patterns. Specifically, systolic blood pressure, diastolic blood pressure, and heart rate were highest in the mid-altitude group and lower at both low and high altitudes, whereas alerting and executive control efficiency showed relatively reduced performance at mid-altitude and higher performance at both ends. This complementary pattern suggested a potential association between cardiovascular strain and attentional efficiency. To examine this possibility, correlation analyses were conducted. The results revealed that blood pressure and heart rate were positively correlated with executive control scores and that diastolic blood pressure was negatively correlated with alerting efficiency. Because higher executive control scores reflect poorer conflict monitoring and resolution performance, these associations indicate that higher cardiovascular indices were related to less efficient alerting and executive control functions. This perspective is supported by prior research; for example, Li et al. found that hypertensive patients showed poorer executive and memory functions, with prefrontal activation intensity 25% lower than the control group and a reduced activation range, indicating that insufficient blood flow limits neuronal activity (Li et al., 2017; Wang et al., 2017).
Importantly, however, the magnitude of these correlations was modest, indicating that cardiovascular variables accounted for only a limited proportion of variance in attentional performance. Accordingly, these findings should be interpreted with caution and do not support direct causal inferences. Rather than suggesting that cardiovascular dysregulation directly causes attentional impairment, the results indicate that sustained cardiovascular strain and reduced attentional efficiency may co-occur under chronic hypoxic stress, particularly within the mid-altitude range identified as an incomplete compensation zone in the proposed U-shaped model. The relatively weak associations further suggest that cardiovascular indicators may not exert a uniform or direct influence on attention network efficiency. Instead, the relationship between systemic cardiovascular regulation and cognitive performance is likely mediated by additional physiological mechanisms not measured in the present study, such as cerebral blood flow regulation, neurovascular coupling efficiency, oxidative stress processes, and individual differences in autonomic nervous system balance. Moreover, chronic hypoxic adaptation may involve multi-level compensatory adjustments, whereby cardiovascular regulation partially offsets reduced oxygen availability, thereby attenuating linear correlations between resting cardiovascular indices and attentional performance. Thus, the modest correlation coefficients observed here likely reflect the complexity of physiological–cognitive interactions rather than the absence of meaningful relationships.
Previous studies have shown that moderate elevations in heart rate and systolic blood pressure may transiently enhance alertness by improving cerebral perfusion (Moonen et al., 2021). However, long-term or excessive elevations in blood pressure reduce cerebrovascular compliance and impair the brain’s ability to regulate blood flow in response to metabolic demand (Iadecola et al., 2016). When blood pressure exceeds the adaptive regulatory range, regions with high metabolic demand—such as the prefrontal cortex—are especially vulnerable to hypoperfusion and metabolic stress, potentially compromising executive and attentional functions (Elias et al., 1993; Bai et al., 2022).
In the present study, diastolic blood pressure in the low- and high-altitude groups remained within a relatively moderate range (∼60–70 mmHg), whereas the mid-altitude group exhibited significantly higher diastolic pressure (79.24 ± 9.24 mmHg). Although this observation alone does not establish a pathological threshold, it suggests that children in the mid-altitude group experienced a level of sustained cardiovascular load that may exceed optimal adaptive regulation. From this perspective, the relatively reduced alerting and executive control efficiency observed at mid-altitude may be associated with prolonged cardiovascular stress rather than with arterial oxygen saturation per se. Integrating the physiological, behavioral, and correlational findings, one plausible interpretation is that mid-altitude exposure represents a transitional state in which hypoxic stress exceeds baseline tolerance but has not yet triggered efficient long-term physiological adaptation. In contrast, despite lower blood oxygen saturation, children in the high-altitude group appear to maintain both cardiovascular stability and attention network efficiency, consistent with more effective compensatory regulation. These results suggest that the cognitive impact of chronic high-altitude exposure in children may depend less on oxygen saturation alone and more on the efficiency of cardiovascular and systemic adaptation to hypoxic stress.
Conclusions, Limitations, and Future Research Directions
By establishing three real-world altitude groups—low (2,200 m), mid (3,200 m), and high (4,200 m)—and integrating cardiovascular indices with the ANT paradigm, the present study systematically examined the effects of chronic high-altitude hypoxic exposure on attention network functioning in indigenous high-altitude primary school students under natural living conditions. The results demonstrated that cardiovascular indices (blood pressure and heart rate) followed a nonlinear pattern characterized by higher values at mid-altitude and lower values at both low and high altitudes, whereas attention network performance—specifically alerting and executive control—exhibited an opposite pattern, with relatively reduced efficiency at mid-altitude and comparable performance at low and high altitudes. In contrast, orienting network efficiency remained stable across altitude levels. To account for these findings, we proposed a U-shaped model of cardiovascular regulation under chronic hypoxia. Within this framework, the low-altitude zone represents a physiological baseline state with minimal hypoxic stress and no need for compensatory regulation. The mid-altitude zone constitutes an incomplete compensation state, in which intensified hypoxic stress elicits heightened sympathetic activation but insufficient regulatory efficiency, resulting in elevated blood pressure and heart rate alongside relatively reduced attentional efficiency. The high-altitude zone reflects a complete compensation state, in which long-term physiological and phenotypic adaptations stabilize cardiovascular function and help preserve attention network performance despite further reductions in blood oxygen saturation. Importantly, these findings indicate that arterial oxygen saturation alone did not directly determine attentional outcomes. Instead, attentional efficiency appeared to be more closely associated with the effectiveness of systemic cardiovascular regulation under chronic hypoxic stress. This observation challenges strictly linear models that attribute cognitive impairment primarily to reduced oxygenation and highlights the importance of adaptive physiological processes in shaping cognitive outcomes in high-altitude children.
Despite the coherence of this integrative framework, several limitations should be acknowledged. First, the proposed U-shaped cardiovascular regulation model is derived from cross-sectional behavioral and physiological data and therefore remains inferential. Genetic, hematological, and neurophysiological markers (e.g., hemoglobin concentration, erythropoietin levels, cerebral blood flow, or neural activation patterns) were not directly measured. Consequently, the model should be regarded as a plausible explanatory hypothesis rather than definitive evidence of causal mechanisms. Future studies employing biochemical assays, neuroimaging, or electrophysiological methods are needed to directly test the proposed compensatory pathways. Second, although cognitive homogeneity across altitude groups was carefully controlled using the Standard Raven’s Progressive Matrices, other environmental and contextual factors were not quantitatively assessed. Socioeconomic status, school quality, parental education, nutritional status, and home learning environments may co-vary with altitude and influence attentional development. While participants were recruited from public boarding primary schools serving indigenous communities with broadly similar educational structures and curricula, these factors remain potential confounders and should be explicitly measured in future research. Third, the sample consisted exclusively of indigenous high-altitude children, which precluded examination of interactions between altitude, duration of exposure, migration status, and developmental stage. Longitudinal designs and cross-population comparisons involving both indigenous residents and migrant children across multiple age groups would be particularly valuable for clarifying the time-dependent and developmental dynamics of cognitive adaptation to chronic hypoxia.
Despite these limitations, this study provides novel evidence that chronic high-altitude exposure does not exert uniform or monotonic effects on attention networks in children. Instead, attentional outcomes appear to reflect the balance between hypoxic stress and the efficiency of cardiovascular and systemic adaptation. By highlighting cardiovascular regulation as a key contextual factor, the present findings contribute to a more nuanced understanding of cognitive development under chronic hypoxic conditions and offer important theoretical insights with potential implications for health management, educational planning, and individualized interventions in high-altitude regions. To our knowledge, this study is the first to systematically integrate cardiovascular regulation and attention network function in indigenous high-altitude primary school students across three ecologically valid altitude gradients under natural living conditions, thereby providing a novel developmental perspective on chronic hypoxic adaptation.
Data and Materials Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement and Informed Consent
The research protocol was approved by the Ethics Committee of Qinghai Normal University (QHNU2024LS-09 and April 7, 2024).
Authors’ Contributions
W.G.: Conceptualization, methodology, investigation, formal analysis, writing—original draft. X.C.: Investigation, data curation, formal analysis. X.L.: Investigation, formal analysis, visualization. X. L.: Investigation, data curation. X.W.: Investigation, data curation. X.C.: Investigation, data curation. C.Z.: Conceptualization, methodology, resources, supervision, funding acquisition, writing—review and editing. C.F.: Conceptualization, methodology, resources, supervision, funding acquisition, writing—review and editing. All authors reviewed and approved the final version of the manuscript.
Footnotes
Author Disclosure Statement
The authors declared no conflicts of interest with respect to the authorship or the publication of this article.
Funding Information
This work was supported by the National Natural Science Foundation of China (Grant/Award Number: 32260203), the Qinghai Provincial Basic Research Program in Science and Technology (Grant Number: 2025-ZJ-957M), and the Major Science and Technology Special Projects of Qinghai Province (Grant/Award Number: 2024-SF-A2).