
Abstract
Ramírez, Esteban, C Alejandro Luzardo, Daniel F Namen, Juan D Rivera, Lina Pérez, Daniela Mora, Nicolás Moncada, Santiago Lopez, and Jaime Guiza. Heart rate variability in adults from low- and high-altitude origins residing in a high-altitude city: A cross-sectional comparison. High Alt Med Biol. 00:00–00, 2026.
Background:
Heart rate variability (HRV) is used to assess autonomic regulation, reflecting autonomic nervous system activity through heartbeat interval analysis. HRV can be evaluated using time-domain, frequency-domain, and nonlinear methods. Although acute high-altitude exposure has been studied, the effects of chronic exposure remain less well understood.
Methods:
This study compared HRV in adults from altitudes ≥2,500 m (group 1) and <1,500 m (group 2), with both groups residing in Bogotá, Colombia (2,600 m) for more than 6 months. HRV was assessed using time domain, frequency domain, and nonlinear metrics.
Results:
Participants from low-altitude regions (group 2) exhibited higher resting heart rates (p = 0.002) and lower time domains (standard deviation of normal-to-normal intervals, root mean square of successive differences, number of pairs of successive normal-to-normal intervals differing by more than 50 ms, percentage of NN50 [%]; p < 0.05), frequency domain (total power, high-frequency power; p ≤ 0.004), and nonlinear measures (triangular interpolation of the NN interval histogram, standard deviation of instantaneous beat-to-beat variability, short-term fractal scaling exponent; p < 0.05) than those from high-altitude regions. These results indicate a lower HRV in individuals from low-altitude regions.
Conclusion:
Adults raised at low altitudes showed lower HRV when living in Bogotá compared with those raised at high altitudes, suggesting an association with long-term autonomic differences potentially related to early-life altitude exposure, rather than a direct causal effect of chronic hypoxia during childhood. These findings may have physiological and clinical implications, particularly in countries with diverse geography. Further prospective, longitudinal research is needed to confirm these associations and clarify their cardiovascular relevance and the potential contribution of genetic and environmental factors.
Introduction
Heart rate variability (HRV) is a physiological indicator used to assess the function of the autonomic nervous system as it reflects the dynamic interaction between sympathetic and parasympathetic influences on the sinoatrial node through the analysis of interval between consecutive R waves (R–R) intervals in the electrocardiogram (Veloza et al., 2019). A reduction in HRV is associated with increased cardiovascular risk, whereas an increase in HRV is linked to better autonomic and cardiovascular health (Sessa et al., 2018; Shaffer and Ginsberg, 2017).
Acute exposure to hypobaric hypoxia at high altitudes triggers sympathetic activation, which, in turn, leads to a decrease in HRV. In contrast, chronic exposure allows acclimatization processes that promote recovery and even enhance parasympathetic activity and HRV (Cornolo et al., 2004; Lizamore et al., 2016). This phenomenon has been described by Contador et al. in athletes exposed to real hypoxia and by Lizamore et al. in populations subjected to simulated hypoxia. However, most of these studies have focused exclusively on the acute or subacute effects (Boos et al., 2022; Contador et al., 2020).
There is limited evidence regarding whether exposure to high altitudes during early life is associated with autonomic adaptations that persist after migration to high-altitude environments. In Colombia, this scenario is particularly relevant, as many individuals from low-altitude regions (<1,500) immigrate to Bogotá, the capital city, which is located at 2,640 m. To date, it remains unclear whether the place of origin influences HRV after prolonged residence in a hypoxic environment.
The aim of this study was to compare HRV between adults from low-altitude (<1,500 m) and high-altitude (≥2,500 m) regions who currently reside in Bogotá (2,640 m). HRV was assessed in the time, frequency, and nonlinear domains to explore potential differences related to chronic cardiovascular adaptations to hypoxia. A better understanding of these differences may provide valuable insights into the mechanisms of cardiovascular adaptation to altitudes and their implications for the health of urban populations chronically exposed to hypoxia.
Methods
Study design
This cross-sectional observational study was conducted between 2021 and 2024 at the Physiology Laboratory of Universidad El Bosque, Bogotá, Colombia (2,640 m). The study aimed to assess HRV in adults.
Participants
The participants were recruited through an open call, a convenience sampling approach in Bogotá, Colombia. Eligible individuals were healthy adults aged 18–35 years who had resided in the city for at least 6 months and had provided written informed consent.
In accordance with the recent literature that has operationally used elevations of 2,500 m and above to characterize significant hypobaric exposure (Tremblay et al., 2024), participants were stratified into two groups based on their self-reported altitudes of residence during the first 10 years of life, as recorded on a standardized questionnaire completed before electrocardiogram recording:
Group 1 (high altitudes): ≥2,500 m. Group 2 (low altitudes): <1,500 m.
The intermediate range of 1,500–2,500 m was deliberately excluded to avoid potential confounding from moderate hypobaric exposure during childhood. Of the 201 individuals screened, 189 met all eligibility criteria and were included in the final analysis (127 in Group 1 and 62 in Group 2). The unequal group sizes reflect participant availability rather than selective recruitment (Fig. 1). No participants reported childhood residence above 3,000 m, precluding further altitude-based stratification.
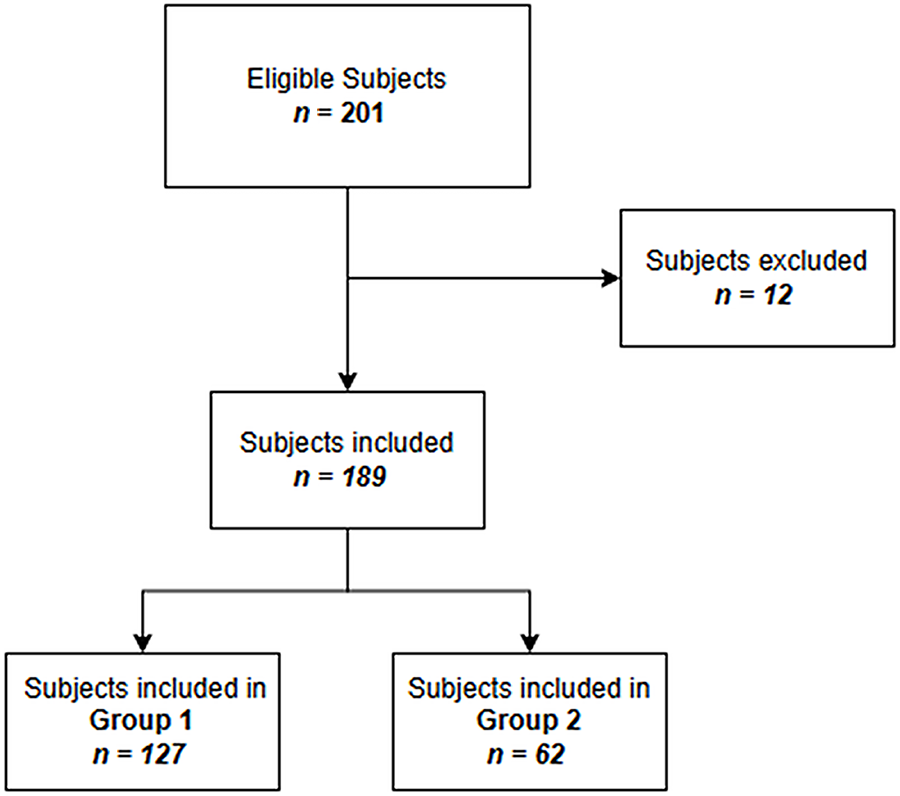
Flowchart of participant selection and allocation. A total of 201 individuals were screened; from these, 12 were excluded and 189 were included in the analysis 127 in Group 1 and 62 in Group 2.
Eligibility criteria
Participants were adults aged 18–35 years who had resided in Bogotá (2,640 m) for at least 6 months and who provided written informed consent. Individuals were excluded if they were high-performance athletes, had slept less than 6 hours the night before the evaluation, or reported consumption of caffeine, nicotine, energy drinks, or other stimulants on the day of the recording. Additional exclusion criteria included alcohol consumption within 48 hours before testing, a history of alcoholism or psychoactive substance abuse, or engagement in physical activity within 1 hour before the evaluation. Participants were also excluded if they presented with chronic conditions, such as hypertension; diabetes mellitus; hypothyroidism; respiratory, cardiovascular, or cerebrovascular disease; cancer; autoimmune disorders; or active infections. Other exclusion criteria were obesity (body mass index [BMI] ≥30), underweight (BMI <18.5), diagnosed psychiatric disorders (including depression, anxiety, schizophrenia, or bipolar disorder), food intake within 2 hours before the evaluation, or the use of any medication within the 24 hours preceding the test.
Procedure
All evaluations were performed in a controlled environment during a single session. Participants remained seated at rest for 30 minutes, followed by a 15-minute supine period for electrocardiogram (ECG, Lead II) acquisition while awake, motionless, and silent. ECG signals were recorded using a PowerLab® system (ADInstruments, Sydney, Australia) and LabChart® software (ADInstruments).
HRV analysis was performed using the Kubios HRV® Standard software (version 3.5.0) (Tarvainen et al., 2014). The R–R intervals were extracted after automatic artifact correction using validated algorithms. Breathing was spontaneous and not controlled during ECG acquisition, and respiratory rate was not directly measured. To reduce potential confounding, participants fasted for at least 2 hours before testing, abstained from alcohol and stimulants, and avoided physical activity during the 24 hours preceding the evaluation.
Variables
The primary outcome was HRV, assessed across three domains:
Time domain: Standard deviation of normal-to-normal intervals (SDNN), root mean square of successive differences (RMSSD), number of pairs of successive normal-to-normal intervals differing by more than 50 ms (NN50), percentage of NN50 (pNN50). Frequency domain: Total power, high-frequency (HF) power (absolute, percentage, and logarithmic units), low-frequency (LF) power (absolute, percentage, and normalized units [n.u.]), and very-low-frequency (VLF) power (logarithmic units). Frequency bands were defined as follows: VLF (0.05–0.078 Hz), LF (0.05–0.15 Hz), and HF (0.15–0.35 Hz). Nonlinear domain: Standard deviation of instantaneous beat-to-beat variability (SD1), triangular interpolation of the NN interval histogram (TINN), short-term fractal scaling exponent, and long-term fractal scaling exponent (alpha 2).
Minimum heart rate was included as an additional parameter.
The main independent variable was the altitudes of residence during childhood (<1,500 m or ≥2,500 m). Demographic and clinical variables (sex, age, BMI, blood pressure, and resting heart rate) were also recorded to describe the study population.
Statistics
Data distribution was assessed using a test of normality. Variables with a non-normal distribution were compared using the Mann–Whitney U test, whereas normally distributed variables were analyzed using Student’s t-test. Comparative analyses were conducted between groups defined by the altitudes of residence during childhood. Given the exploratory nature of this study, no multivariate analyses or adjustments were performed to control for potential confounders.
Ethical approval
The study protocol was reviewed and approved by the Ethics Committee of the Universidad El Bosque (approval no. 016–2023, July 18, 2023). All procedures were conducted in accordance with the ethical principles of the Declaration of Helsinki (World Medical Association, 2013).
Results
Characterization of the study population
The study population comprised 189 participants: 127 in Group 1 (altitudes ≥2,500 m) and 62 in Group 2 (<1,500 m). No statistically significant differences were observed between the groups in sex, age, height, weight, BMI, or blood pressure, indicating comparable baseline characteristics (p > 0.05; Table 1).
Baseline Characteristics According to Altitude of Origin
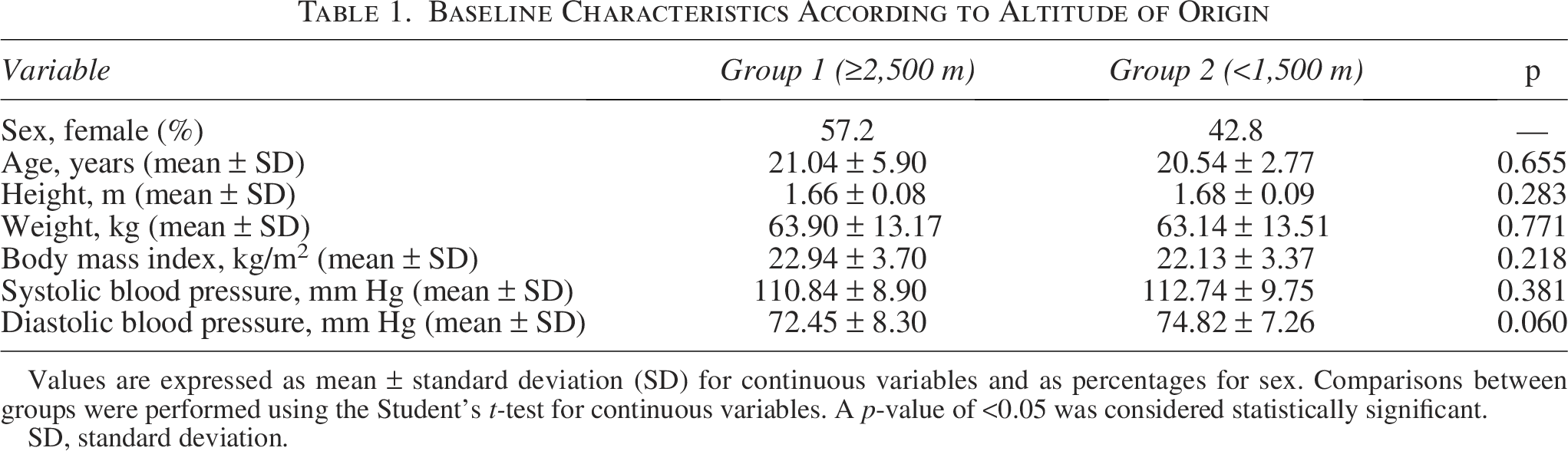
Values are expressed as mean ± standard deviation (SD) for continuous variables and as percentages for sex. Comparisons between groups were performed using the Student’s t-test for continuous variables. A p-value of <0.05 was considered statistically significant.
SD, standard deviation.
HRV parameters by altitudes of origin
The HRV parameters were analyzed in the time, frequency, and nonlinear domains. Time-domain HRV parameters are presented in Table 2, whereas frequency-domain and nonlinear HRV parameters are presented in Table 3. Statistical comparisons were performed using Student’s t-test or the Mann–Whitney U test.
Heart Rate Variability Parameters in the Time Domain According to Childhood Altitude Category (≥2,500 m vs. <1,500 m)
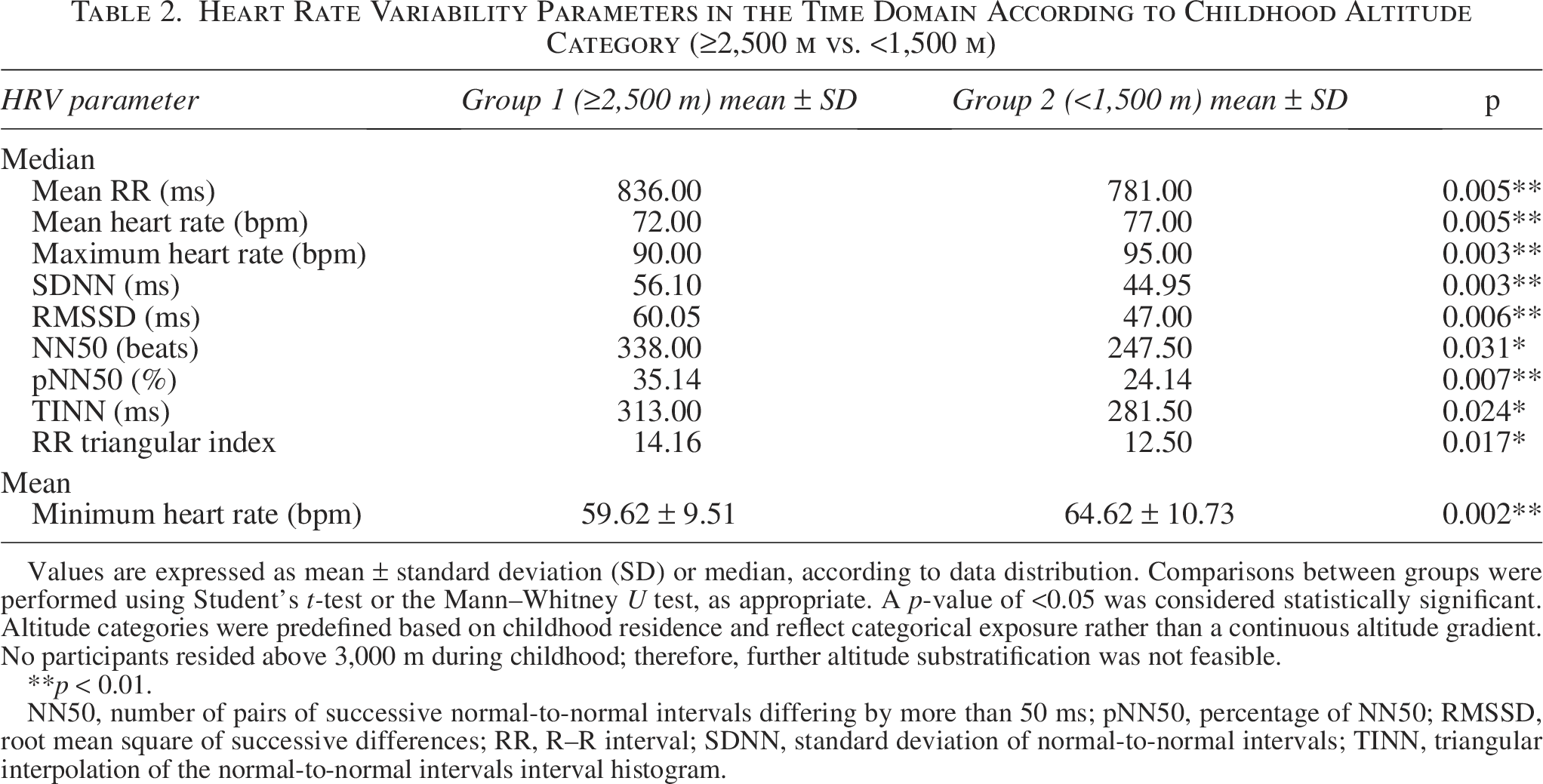
Values are expressed as mean ± standard deviation (SD) or median, according to data distribution. Comparisons between groups were performed using Student’s t-test or the Mann–Whitney U test, as appropriate. A p-value of <0.05 was considered statistically significant. Altitude categories were predefined based on childhood residence and reflect categorical exposure rather than a continuous altitude gradient. No participants resided above 3,000 m during childhood; therefore, further altitude substratification was not feasible.
**p < 0.01.
NN50, number of pairs of successive normal-to-normal intervals differing by more than 50 ms; pNN50, percentage of NN50; RMSSD, root mean square of successive differences; RR, R–R interval; SDNN, standard deviation of normal-to-normal intervals; TINN, triangular interpolation of the normal-to-normal intervals interval histogram.
Heart Rate Variability Parameters According to Childhood Altitude of Origin—Frequency-Domain and Nonlinear Measures

Values are expressed as mean ± standard deviation (SD) or median, according to data distribution. Comparisons between groups were performed using Student’s t-test or the Mann–Whitney U test, as appropriate. A p-value of <0.05 was considered statistically significant. Frequency-domain bands were defined as very-low frequency (VLF: 0.003–0.04 Hz), low frequency (LF: 0.04–0.15 Hz), and high frequency (HF: 0.15–0.40 Hz). Absolute power values (ms2) and logarithmic transformations reflect total spectral power, whereas percentages (%) and normalized units (n.u.) represent relative contributions within the spectrum.
**p < 0.01.
alpha 1, short-term fractal scaling exponent; alpha 2, long-term fractal scaling exponent; HF, high-frequency; LF, low-frequency; SD1, standard deviation of instantaneous beat-to-beat variability; SD2, standard deviation of long-term variability (Poincaré plot); VLF, very-low-frequency.
In the frequency domain, statistically significant differences were observed in total power (log; p = 0.001) and HF power (log; p = 0.001), both of which were higher in Group 1. In contrast, minimum heart rate (p = 0.002) and long-term fluctuations (alpha 2; p = 0.003) were higher in Group 2 (Table 2 and Table 3, respectively).
Several indices showed significant differences between the groups for variables with non-normal distributions. In the time domain, Group 1 presented higher values for the mean R–R interval (RR) (p = 0.005), SDNN (p = 0.003), RMSSD (p = 0.006), NN50 (p = 0.031), pNN50 (p = 0.007), TINN (p = 0.024), and RR triangular index (p = 0.017), whereas Group 2 showed higher values for the stress index (p = 0.007). In the frequency domain, the total power (ms2; p = 0.004), LF power (ms2; p = 0.003), LF power (log; p = 0.005), and HF power (ms2; p = 0.003) were greater in Group 1, whereas the VLF power (%) was higher in Group 2 (p = 0.020). Regarding nonlinear measures, SD1 (p = 0.007) and SD2 (p = 0.003) were significantly higher in Group 1 (Table 3).
Discussion
This study revealed significant differences in HRV between adults originating from altitudes above 2,500 m and those from altitudes below 1,500 m, after more than 6 months of residence in Bogotá (2,640 m). Unlike previous studies that focused on acute exposure to altitudes (Cornolo et al., 2004; Lizamore et al., 2016), our findings indicate that these HRV differences persist in the long term, suggesting a sustained cardiovascular modulation associated with prior altitude exposure that has not been previously described (Aldavero Muñoz, 2017; Gallagher et al., 2021).
Heart rate–related parameters (mean RR, mean, minimum, and maximum heart rate) were consistently higher in the low-altitude group, reflecting a shift toward greater sympathetic influence and lower overall HRV, as previously described (Boos et al., 2022; Cygankiewicz and Zareba, 2013). In contrast, the high-altitude group exhibited higher time-domain parameters (SDNN, RMSSD, NN50, and pNN50%), which are commonly interpreted as reflecting greater parasympathetic-related heart rate modulation and are associated with better cardiovascular health, as reported in prior studies (Hill et al., 2018; Lizamore et al., 2016; Sessa et al., 2018; Shaffer and Ginsberg, 2017; Veloza et al., 2019).
These findings are partially consistent with studies in athletic populations, such as that of Contador et al., who observed transient decreases in HRV among soccer players during acute exposure to high altitudes in La Paz (3,650 m) (Contador et al., 2020). Our study contributes a novel perspective by examining longer-term cardiovascular modulation beyond the initial acclimatization phase, rather than acute responses alone (Cornolo et al., 2004; Gallagher et al., 2021).
Additionally, the elevated stress index and increased very-low-frequency (VLF) power observed in the low-altitude group are consistent with a pattern suggestive of greater sympathetic-related influence, as reported previously (Boos et al., 2022; Cygankiewicz and Zareba, 2013). Such autonomic imbalance could have adverse consequences for cardiovascular regulation and overall homeostasis (Sessa et al., 2018).
In our study, frequency-domain analysis showed higher total power and HF values in the high-altitude group, which have been commonly interpreted as reflecting greater parasympathetic-related heart rate modulation at rest (Hill et al., 2018; Lizamore et al., 2016; Shaffer and Ginsberg, 2017; Veloza et al., 2019). Although this group also exhibited higher LF values, which could suggest a sympathetic contribution, such an interpretation is limited by the study design (short-term, supine recordings) and the lack of baroreceptor challenge maneuvers (Boos et al., 2022; Cornolo et al., 2004). Because VLF and LF power were largely similar between groups, the observed differences in total power were mainly driven by HF components. Given that HF power may be influenced by respiratory patterns, breathing was spontaneous and not controlled in either group, and both groups were evaluated under identical resting conditions; therefore, major systematic differences in respiratory influence between groups cannot be excluded but are considered unlikely. Nonlinear analysis, increasingly recognized as a valuable tool in the study of cyclical physiological phenomena, revealed higher TINN, SD1, and short-term fluctuation short-term scaling exponent (alpha-1) of detrended fluctuation analysis values in the high-altitude group, reinforcing the evidence of a more robust HRV in this population (Cygankiewicz and Zareba, 2013; Shaffer and Ginsberg, 2017). In contrast, the elevated standard deviation of long-term variability (Poincaré plot) (SD2) observed in the low-altitude group may reflect a greater contribution of long-term variability mechanisms, which have been associated with increased sympathetic-related influence, consistent with an autonomic profile shifted toward sympathetic predominance (Sessa et al., 2018).
These findings support the hypothesis that long-term residence at high altitudes during childhood is associated with long-term differences in autonomic-related cardiovascular regulation, potentially reflecting both early-life altitude exposure and genetic or familial factors, which may confer cardiovascular benefits in such environments (Aldavero Muñoz, 2017; Cornolo et al., 2004; Gallagher et al., 2021). However, due to the observational design of this study, causality cannot be inferred. Future longitudinal and interventional studies are needed to determine whether the observed HRV differences translate into a reduced incidence of chronic cardiovascular disease (Sessa et al., 2018; Shaffer and Ginsberg, 2017).
This study has certain limitations that should be acknowledged. First, due to its cross-sectional design, causal relationships between altitudes of origin and HRV cannot be established. The relatively moderate sample size and the absence of extended recordings also limit the scope of interpretation, as longer recordings would have allowed a more comprehensive assessment of baroreceptor modulation (Hernández and Velasco-Mondragón, 2000). In addition, respiratory rate was not directly monitored during HRV recordings, and because several HRV indices, particularly those in the high-frequency domain, are influenced by respiratory patterns, variability in breathing may have affected some of the observed autonomic responses. The study also did not include information regarding the genetic background of participants, and genetic adaptations associated with long-term high-altitude ancestry could influence autonomic regulation and cardiovascular responses to hypoxia, potentially contributing to the differences observed between groups. Finally, although participants had resided in Bogotá for more than 6 months, variability in duration of residence and previous altitude exposure may also influence autonomic adaptation. Future studies incorporating respiratory monitoring, assessment of genetic background, larger samples, and longitudinal designs would help clarify these mechanisms.
In summary, our findings suggest that early-life residence at high altitudes is associated with higher HRV and greater parasympathetic modulation, even after long-term residence in Bogotá. In contrast, individuals from low-altitude regions showed lower HRV values, a pattern that warrants further investigation to clarify its potential long-term cardiovascular implications.
Authors’ Contributions
C.A.L.: Investigation, data curation, and writing—original draft. D.F.N., J.D.R., L.P., D.M., N.M., S.L., and J.G.: Investigation and data curation. E.R.: Conceptualization, methodology, formal analysis, supervision, writing—review and editing, and project administration.
Footnotes
Acknowledgments
The authors would like to thank the Physiology Laboratory of Universidad El Bosque for providing facilities and technical support for conducting this study. The authors are also grateful to all participants for their valuable contributions.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
The authors received no specific funding for this work.