
Abstract

Normobaric hypoxic sleeping systems are increasingly utilized as a preacclimatization strategy by both professional mountaineers and climbers guided commercially. However, their efficacy in improving subsequent terrestrial high-altitude performance remains debated (Fulco et al., 2011). We report an opportunistic observational case study of 37-year-old male monozygotic twins (confirmed by whole-genome sequencing; Participants A and B) who undertook markedly different passive normobaric hypoxic preacclimatization regimens before a successful ascent of Mount Everest in May 2024.
Both participants showed almost identical baseline fitness confirmed by incremental treadmill cardiopulmonary exercise testing (maximal oxygen uptake [VO2max]: 56.8 vs. 56.1 ml·kg−1·min−1; lactate thresholds and maximum heart rates). Both had comparable high-altitude experience, having previously summited Aconcagua (6,961 m) in January 2018 and Denali (6,190 m) in June 2019, with no prior use of normobaric hypoxic conditioning systems.
During the 39 days before departure, Participant A slept in a commercial normobaric hypoxic tent for 351 hours. The fraction of inspired oxygen (FIO2) was progressively manually titrated from 0.150 to 0.105 based on intermittent overnight oxygen saturation as (SpO2) checks via pulse oximetry (Nonin 3150, Plymouth, MN). Conversely, Participant B completed a minimal protocol of only 30 hours of exposure (FIO2: 0.137–0.122) in the 5 days preceding departure (Fig. 1).
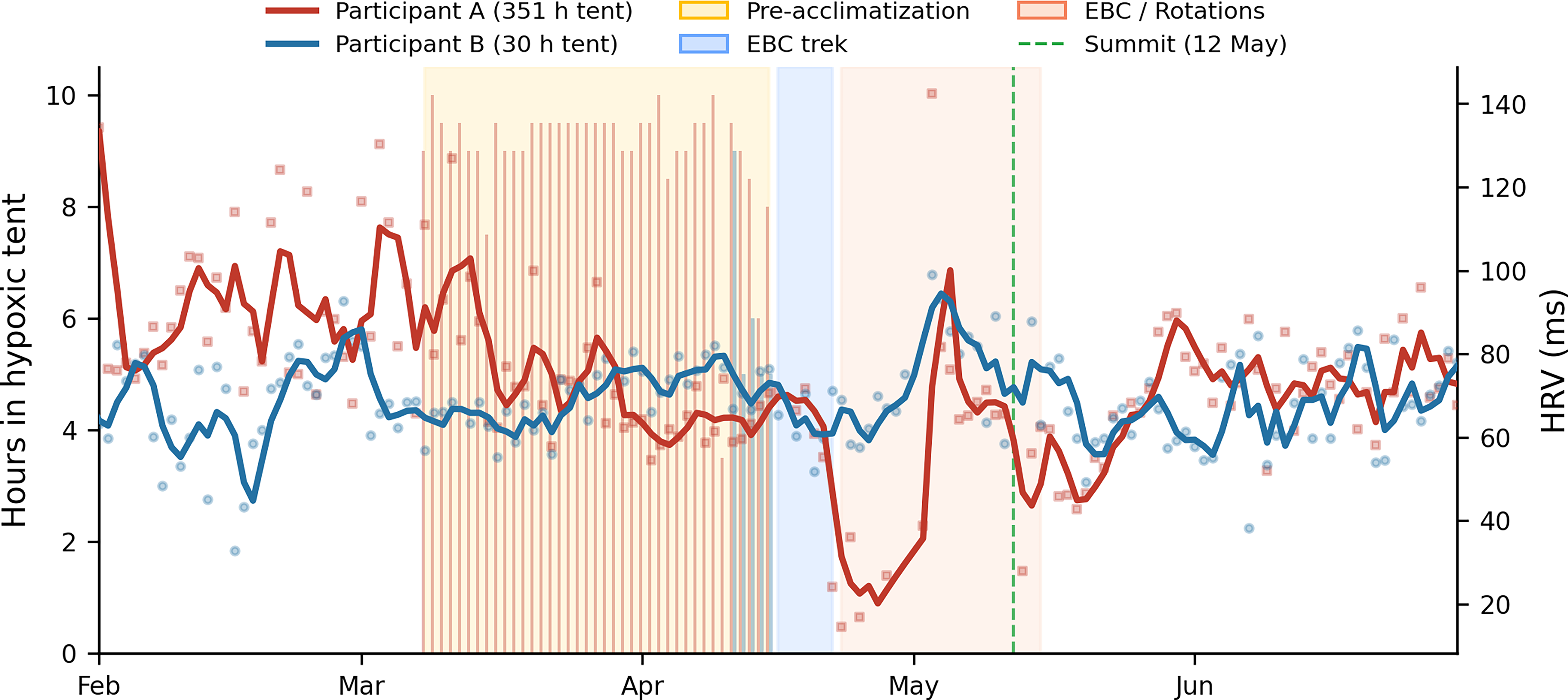
Normobaric hypoxic tent exposure and heart rate variability (HRV) for Participant A (red) and Participant B (blue) (February–June 2024). Bars (left axis) show nightly hours spent in the hypoxic tent. Bold lines (right axis) show HRV as 3-day rolling averages with linear interpolation across gaps of ≤3 days; individual data points are shown as markers (squares = Participant A, circles = Participant B). Shaded regions indicate as follows: yellow = preacclimatization intervention; blue = EBC trek; orange = EBC/rotations. Green dashed line = summit day (12 May 2024). Note the progressive decline in HRV in Participant A during the preacclimatization period despite the 11.7-fold greater hypoxic exposure. EBC, Everest Base Camp.
Longitudinal physiological data were collected daily using commercial wearable sensors (Fitbit Luxe, San Francisco, CA) to track resting heart rate (RHR), heart rate variability (HRV; nightly root mean square of successive differences derived from photoplethysmography during sleep), and resting respiratory rate (RR).
During the preacclimatization intervention, Participant A exhibited an observable progressive decline in HRV (Fig. 1) and Fitbit-derived sleep scores compared to Participant B, suggesting mild physiological strain. Despite this 11.7-fold difference in preexpedition hypoxic exposure, both participants demonstrated nearly indistinguishable adaptation profiles upon arrival in the Himalaya.
During the standard 7-day approach trek to Everest Base Camp (EBC, 5,364 m), both participants exhibited an immediate, synchronized increase in RHR and RR. Similarly, SpO2 values recorded via point-of-care pulse oximetry at EBC and Camp 2 (6,500 m) were similar and consistent with standard physiological adaptation (Grocott et al., 2009). An observable decline in HRV in Participant A during rotations between EBC and higher camps was related to a minor viral illness. Following a standard acclimatization rotation, both participants successfully summited Everest on May 12, 2024, using identical supplemental oxygen flow rates and reporting comparable exertion levels.
The principal observation of this twin case study is that 351 versus 30 hours of passive normobaric hypoxic exposure conferred no observable advantage in on-mountain performance. We hypothesize two principal explanations. First, the standard 7-day hypobaric trek to EBC likely provided a potent and sufficient primary acclimatization stimulus, effectively overriding any baseline advantage. Second, innate physiological traits, such as closely matched resting RR profiles in both twins, may exert a stronger influence on high-altitude tolerance than passive hypoxic preconditioning (Canouï-Poitrine et al., 2014; Luks et al., 2017).
We acknowledge the inherent limitations of this report, such as low power, the use of commercially available wearables, the field study environment, and the lack of pre- and post-expedition blood tests assessing hematological response.
Despite these limitations, this unique genetically matched observation suggests that success at “real-life” extreme altitudes was not affected by passive normobaric hypoxic preacclimatization.
These findings highlight the need for further adequately powered studies into widely commercially available normobaric preacclimatization systems and protocols to determine their efficacy and close the existing evidence gap.
Footnotes
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
No funding was received for this article.