
Abstract
Hill, Adam D. Slow symptom resolution of acute altitude illness upon rapid descent. High Alt Med Biol. 00:00–00, 2026.—Acute mountain sickness (AMS) effects roughly one-quarter to more than three-quarters of persons travelling to elevations greater than 2,500 m. Treatment relies primarily on descent or a stoppage of further ascent (with or without pharmacologic therapy) to allow for acclimatization. In the latter approach, acclimatization as heralded by improvement of symptoms can take anywhere from 12 hours to 4 days. The timeline for symptom resolution when descent takes place, however, is not clearly defined. A case is presented of a hiker who suffered from persistent symptoms of AMS for nearly 24 hours despite descending rapidly to sea level.
Introduction
Acute mountain sickness (AMS) occurs in an estimated 20–85% of individuals traveling at high altitudes (>2,500 m) (Beidleman et al., 2013; Cameron et al., 2026; Pradhan et al., 2009), with rates being influenced by various factors, including speed of ascent, absolute altitude achieved, and individual susceptibility, among others (Hackett et al., 2017; Imray et al., 2011). Descent is the best treatment option among several (Luks et al., 2024), but the anticipated timing of symptom resolution upon reaching lower elevations is not well defined or documented. A case is presented here that describes a hiker experiencing mild AMS after summiting Maunakea with prolonged symptoms for nearly 24 hours despite rapid descent to sea level.
Case Presentation
A 37-year-old experienced female hiker was part of a group climbing Maunakea (4,205 m) on the island of Hawai’i in the United States of America. Having arrived the evening before, they spent the night in a hotel near sea level (0 m). The group included two medical professionals—myself (a physician) and the hiker herself (a physician associate). While her living altitude was close to sea level, she had spent 7 days sleeping and travelling at or above 2,600 m 1 week prior to this climb. She had no prior medical history, was of South Asian descent, had a body mass index of 21, and her only medication was oral contraceptive pills. Of note, she had experienced no prior episodes of AMS when travelling above 2,500 m.
The group embarked just after sunrise, driving to the Maunakea Visitor Information Station (2,804 m), where they began the hike. Roughly 4 hours into the hike (∼3,700 m) and a total time above 2,500 m of ∼5.5 hours, the aforementioned hiker began experiencing a dull, throbbing headache and mild nausea. Believing she had mild AMS, she self-administered 400 mg ibuprofen and 4 mg ondansetron orally for symptom relief. After a short rest period, she opted to continue. She never exhibited any fatigue, weakness, confusion, lethargy, or ataxia. The group successfully summited, but during the descent the hiker expressed a worsening of her headache and nausea and took 1,000 mg of acetaminophen orally. Upon reaching the visitor station 10 hours after starting the hike, she began having frequent bouts of emesis and was immediately driven back to sea level.
The emesis persisted over 12 hours while the nausea and headache lasted close to 24 hours. Standard pharmacologic therapeutics for AMS, such as acetazolamide or dexamethasone, were not available without presentation to a medical facility, so the hiker took an additional dose of 4 mg ondansetron as well as 400 mg ibuprofen with 1,000 mg acetaminophen for the nausea and headache, respectively, during this period. She was examined by me and found to have no signs of respiratory distress or increased respiratory rate, had a nontender abdomen, exhibited no lower extremity edema, and had a grossly normal neurologic examination with a steady gait and no signs of confusion, lethargy, or ataxia. Detailed vital signs such as temperature, heart rate, respiratory rate, blood pressure, and pulse oximetry were either not obtained due to a lack of supplies or not formally recorded. She reported no abdominal pain, diarrhea, flank pain, fevers, chest pain, or shortness of breath. No one else in the climbing party had similar symptoms. Despite recommendations by the other group members, she declined to seek advanced medical care. At nearly 24 hours after descending, the hiker reported full resolution of her symptoms (Fig. 1) and ultimately sought no further medical evaluation related to this event upon return home.
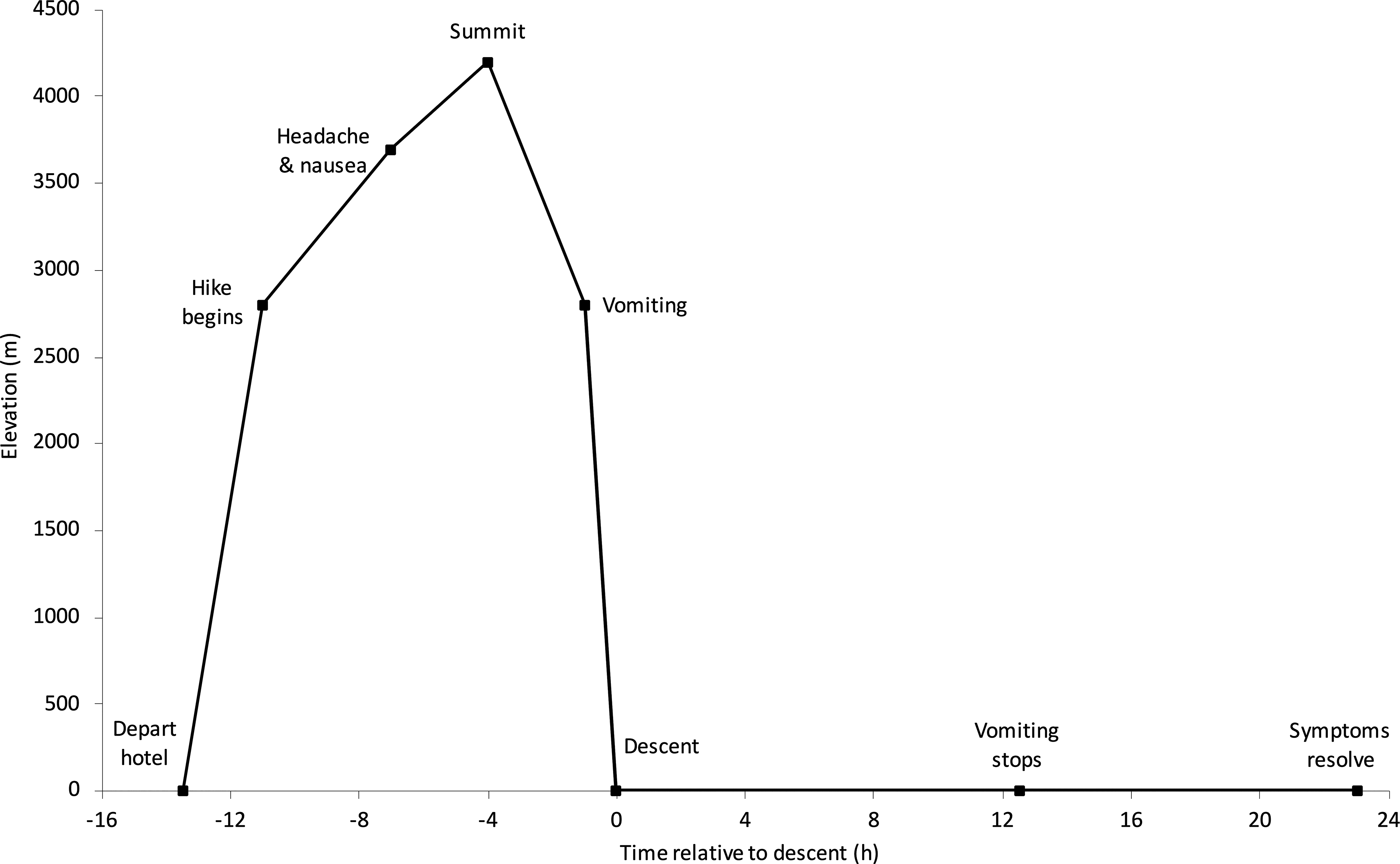
Events in relation to elevation and time from descent.
Discussion
AMS is one of several distinct syndromes related to high-altitude travel (Luks et al., 2024). Prior research has placed the incidence of AMS among travelers to Maunakea at 30% (Onopa et al., 2007). Its management depends on factors unique to each patient and situation. Both descent and stopping further ascent (with or without pharmacologic therapy) are accepted practices per current Wilderness Medical Society guidelines (Luks et al., 2024). When holding further ascent without medication assistance, symptoms typically resolve within 12 hours to 4 days (Hackett et al., 2017). What is not well established is the anticipated time to resolution of AMS in a patient who descends. An understanding of the pathophysiology would suggest it to be decreased in an individual who descends compared to one who maintains altitude, but there are no data to definitively support that statement. While commenting on descent as the definitive treatment, many texts and information resources use statements such as “quickly” (Strickland, 2024) and “rapidly” (Hackett and Shlim, 2025) when referring to expected timing.
In the above case, the hiker had a Lake Louise Scoring System (LLSS) number corresponding to mild AMS (mild headache with moderate nausea, LLSS = 3) and attempted to manage the symptoms with oral medications (Roach et al., 2018). Despite descending from 4,205 m at the summit to 2,804 m at the visitor station, her symptoms worsened (moderate headache with severe nausea and vomiting, LLSS = 5). This can likely be explained by the typical 6–12 hour delay in symptom onset combined with her continued climb (Imray et al., 2011; Roach et al., 2018). Active ascent has been shown to hasten the onset of AMS, so it is plausible that an active descent could worsen or sustain symptoms (Beidleman et al., 2023; Fabries et al., 2025). Returning to the visitor station was, however, a descent of nearly 900 m from the altitude at which symptoms began—at the upper end of the recommended 300–1,000 m for treating AMS (Luks et al., 2024). This prompted the other group members to recommend advanced care as they expected improvement, if not resolution, of the symptoms after achieving such a decrease in elevation.
Possible explanations for the hiker’s slow symptom resolution are many. It may have been related to the anticipated delay in symptom onset coupled with exertional ascent and descent, as previously described. Alternatively, instead of AMS, she may have actually had undiagnosed early high-altitude cerebral edema, which would require a longer resolution time (Hackett et al., 2017). High altitude deacclimatization syndrome—wherein exposure to higher atmospheric pressures and oxygen levels (such as during or after descent) causes a myriad of symptoms, including headache, fatigue, decreased appetite, and abdominal pain, to name a few—is also possible though less likely, given it is predominantly linked to individuals who are acclimatized and have resided at altitude for extended periods of time (He et al., 2013). The lack of other symptoms or sick members within the group leans against a non-altitude-related diagnosis such as acute gastroenteritis or viral syndrome. Ultimately, it may be a case of the hiker’s unique individual susceptibility and response to AMS causing her to be an outlier from the commonly anticipated course of illness.
This case highlights the importance of information relating to descent and AMS. While studies have evaluated the occurrence of AMS after descent in acclimatized individuals (Beidleman et al., 2017; Subudhi et al., 2014), and the International Headache Society has defined the resolution of high-altitude headache to occur within 24 hours of descent (Olesen et al., 2018), a literature review found limited information describing a more detailed hourly time course for AMS resolution in symptomatic patients. Such information could prove useful to clinicians caring for patients with a suspected diagnosis of AMS who have descended. Due to the overlap with other diagnoses (hyponatremia, migraine headache, viral illness, gastroenteritis, etc.), a patient whose symptoms persist past an anticipated timeline could prompt clinicians to expand their differential and pursue additional treatment modalities or diagnostic testing.
Conclusion
Expected time to resolution of AMS symptoms after descent is typically rapid, but a more detailed and definitive timeframe is unknown. Future studies and observations examining altitude-related disorders would benefit from additional information related to this missing data. Such knowledge could better guide patient management in suspected cases of AMS.
Author’s Contributions
A.D.H.: Conceptualization, investigation, writing—original draft, writing—review and editing, visualization.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.