
Abstract
Brillhart, Aaron, Molly Enenbach, Javier Seufferheld, Bernabé Abramor, Peter Callas, Rodrigo Duplessis, Ian Guertin, Theodore A Hartridge, Roxana Pronce, Ana Saravia, and Scott E. McIntosh. Medical screening of climbers who later develop high-altitude pulmonary edema on Aconcagua. High Alt Med Biol. 00:00–00, 2026.
Introduction:
On Aconcagua (6,961 m), high-altitude pulmonary edema (HAPE) is the most frequent reason for medical evacuation. This study aimed to compare medical screening data of climbers who developed HAPE with those who did not and to identify trends to aid in illness prevention and climber safety.
Methods:
De-identified medical screening data of Aconcagua climbers from 2024 to 25 were retrospectively reviewed, comparing climbers who developed HAPE with those who did not.
Results:
Fifty-three of 2,336 climbers developed HAPE (2.3%). Asymptomatic climbers screened at 4,300 m who later developed HAPE had lower mean oxygen saturation than controls (80% vs. 85%, p < 0.001) and higher mean heart rate (96 vs. 87 bpm, p < 0.001). Nonsignificant trends were noted with guided status (74% vs. 61%, p = 0.06), and prophylactic acetazolamide use (34% vs. 21%, unadjusted: p = 0.02, odds ratio [OR] 1.92, adjusted: p = 0.08, OR 1.74).
Conclusions:
On Aconcagua, certain vital sign parameters, including oxygen saturation below 80% and tachycardia during asymptomatic screening at 4,300 m, could raise concern for later developing HAPE. Future research could clarify any association between HAPE, certain climber groups such as guided clients, ascent rate, and medication use. Gradual ascent should continue to be emphasized to facilitate acclimatization and prevent life-threatening altitude illness such as HAPE.
Introduction
Mount Aconcagua (6,961 m) in Argentina is the highest peak in the Americas and attempted by thousands of climbers annually. On Aconcagua, high-altitude pulmonary edema (HAPE) occurs in over 2% of climbers, is the most common life-threatening medical illness encountered, the most common reason for rescue evacuation, and has been associated with death on the mountain (Brillhart et al., 2025b, 2025a; Westensee et al., 2013). The medical service of Aconcagua Provincial Park (APP) performs medical clearance control checks on all climbers during ascent at the base camps of Plaza de Mulas (4,300 m, Normal Route), Plaza Argentina (4,200 m, Vacas Valley approach), and Confluencia (3,400 m, Normal Route). The APP medical service also oversees the medical aspects of all rescue evacuations on Aconcagua, including all climbers who develop HAPE.
A recent Aconcagua study surveyed 17 HAPE patients and found that HAPE was associated with ascending with unresolved symptoms of acute mountain sickness (AMS), fewer days spent acclimatizing at 4,300 m base camp, and a non-significant trend of increased acetazolamide use compared with 42 healthy controls (47% vs. 19%, p = 0.05) (Park et al., 2025). That survey did not include medical screening data. To date, medical screening data of climbers who subsequently develop HAPE have never been analyzed nor published in the medical literature. This study aimed to compare medical screening data of climbers who developed HAPE with those who did not and to identify trends that may aid in high-altitude illness prevention and climber safety.
Materials and Methods
Retrospective de-identified medical service data were reviewed from an electronic database for all climbers attempting to summit Aconcagua via the Horcones Valley Normal Route and who underwent mandatory medical clearance checks at Plaza de Mulas base camp during the November 2024–March 2025 climbing season. Similarly, retrospective deidentified data for all climbers who were diagnosed with HAPE and evacuated from the Normal Route (all from Plaza de Mulas) over the same timeframe were reviewed and compared to the control population of those climbers who did not develop HAPE. Diagnosis of HAPE was made clinically by physicians of the APP medical service based on symptoms such as dyspnea and/or cough, rales on pulmonary auscultation, and decreased peripheral oxygen saturation. Data collected by the medical service included climber demographics, country of origin, guided status, existing symptoms, vital signs, pulmonary exam, and medication. Medication use specified whether the climber was taking prophylactic acetazolamide to facilitate acclimatization and prevent AMS, rather than for treating symptoms of AMS. These data did not include ascent rate, as the medical service does not currently track or record it.
If climbers ascended via the Vacas Valley approach through Plaza Argentina base camp but were later evacuated for HAPE from Plaza de Mulas on the Normal Route, they were included in the dataset of Plaza de Mulas HAPE patients. Climbers who did not attempt Aconcagua via the Horcones Valley Normal Route and who were not evacuated via the Normal Route for HAPE were not included in the current study.
Statistical analyses were performed using two-sample t tests for continuous variables and chi-square tests for categorical variables, with differences in means and odds ratios computed for effect sizes. Logistic regression was used to further examine the relationship between acetazolamide and HAPE, adjusting for age, sex, guided status, and continent. Data were analyzed using SAS 9.4 (Cary, NC: SAS Institute Inc.).
This study was approved by the Institutional Review Board of the University of Utah. Permission to conduct the study was granted by the medical service of APP.
Results
Over the study period, 53 of 2,336 climbers on the Aconcagua Normal Route developed HAPE, and all were evacuated from the Plaza de Mulas (4,300 m) base camp. The incidence of HAPE in the study population was 2.3% (95% confidence interval [CI] 1.7 to 3.0). Of those 53 climbers, 35 had a routine asymptomatic mandatory medical clearance check at 4,300 m base camp with vital sign records prior to developing HAPE, and 18 had not yet undergone their routine medical clearance check prior to developing HAPE. None had reported a history of prior HAPE. Four of the 53 climbers with HAPE evacuated from the Normal Route had ascended via the alternate Vacas Valley and were included. The medical service performed an initial mandatory medical clearance check with vital signs on 2,283 other climbers at Plaza de Mulas who did not develop HAPE (control group).
As shown in Table 1, climbers who underwent an asymptomatic initial mandatory medical check at 4,300 m but later developed HAPE (n = 35) had a 5% lower oxygen saturation on their initial asymptomatic evaluation than those climbers who did not develop HAPE (80% vs. 85%, p < 0.001, 95% CI −7% to −4%, sensitivity 31.4%, specificity 91.4%, PPV 5.4%, NPV 98.8%). These climbers also had higher heart rates (96 vs. 87 bpm, p < 0.001) and respiratory rates (15.5 vs 14.7/min, p = 0.005). Blood pressures did not differ. Climbers who developed HAPE did not differ from controls in age, sex, guided status, or continent of origin (other than Africa, which included less than 1% of total climbers). There were non-significant trends towards more guided clients developing HAPE than independent climbers (74% vs. 61%, p = 0.06) and more North American climbers developing HAPE versus those from other continents (28% vs. 22%, p = 0.29).
Climbers Who Developed High-Altitude Pulmonary Edema (HAPE) on Aconcagua versus Climbers Who Did Not Develop HAPE. Vital Signs Are Displayed from the First Asymptomatic Medical Clearance Check at 4,300 m Base Camp (n = 35/53 for Climbers Who Later Developed HAPE). N = 2,039 for the Prophylactic Acetazolamide Control Group Only
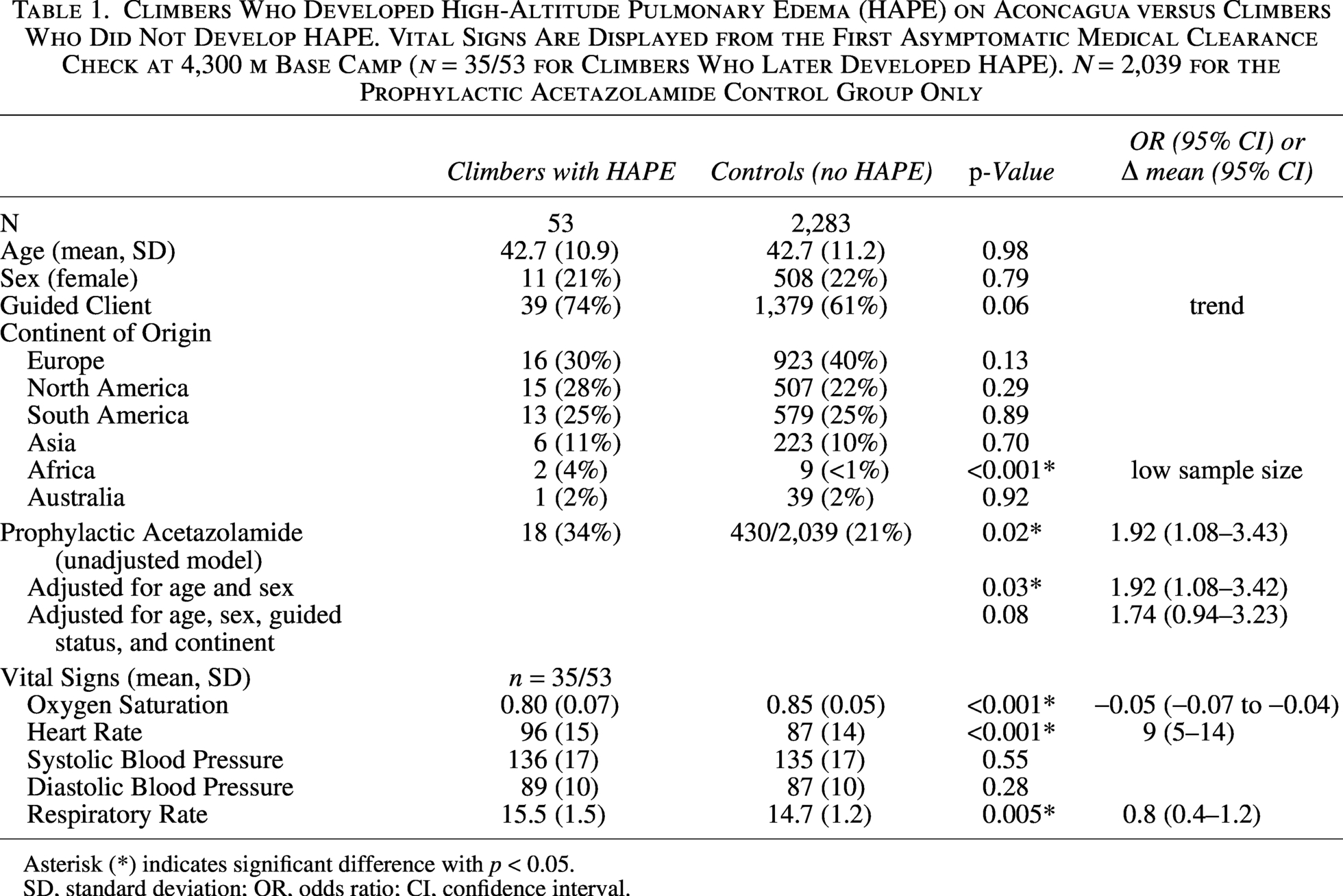
Asterisk (*) indicates significant difference with p < 0.05.
SD, standard deviation; OR, odds ratio; CI, confidence interval.
Of all climbers with documentation regarding whether they were taking prophylactic acetazolamide, 21% (n = 448/2,092) confirmed taking acetazolamide for this purpose (with >99% at the 125 mg BID dose). In an unadjusted model, more climbers who developed HAPE were taking prophylactic acetazolamide than controls (34% vs. 21%, p = 0.02, OR 1.92, 95% CI 1.08–3.43). When adjusting for age, sex, guided status, and continent of origin, the result became a nonsignificant trend (p = 0.08, OR 1.74, 95% CI 0.94–3.23). Table 2 displays demographic and vital sign characteristics for climbers who took prophylactic acetazolamide on Aconcagua versus those who did not, grouped by climbers who developed HAPE and the control group of those who did not. Among controls (and all climbers), acetazolamide use was more common in guided clients (73% vs. 55%, p < 0.001) and climbers from North America (39% vs. 18%, p < 0.001), and less frequent in climbers from South America (8% vs. 29%, p < 0.001). Among climbers who developed HAPE, female climbers comprised a greater proportion of the group taking prophylactic acetazolamide compared with those not taking acetazolamide (44% vs. 9%, p = 0.002). Oxygen saturation was marginally increased in the control group taking acetazolamide (86% vs. 85%, p = 0.02).
Characteristics of Climbers Who Took Prophylactic Acetazolamide on Aconcagua versus Those Who Did Not. Climbers Are Grouped by Those Who Developed High-Altitude Pulmonary Edema (HAPE) and Controls. Vital Signs Are from the First Asymptomatic Medical Check at 4,300 m Base Camp (Difference in Total n Due to Missing Values)
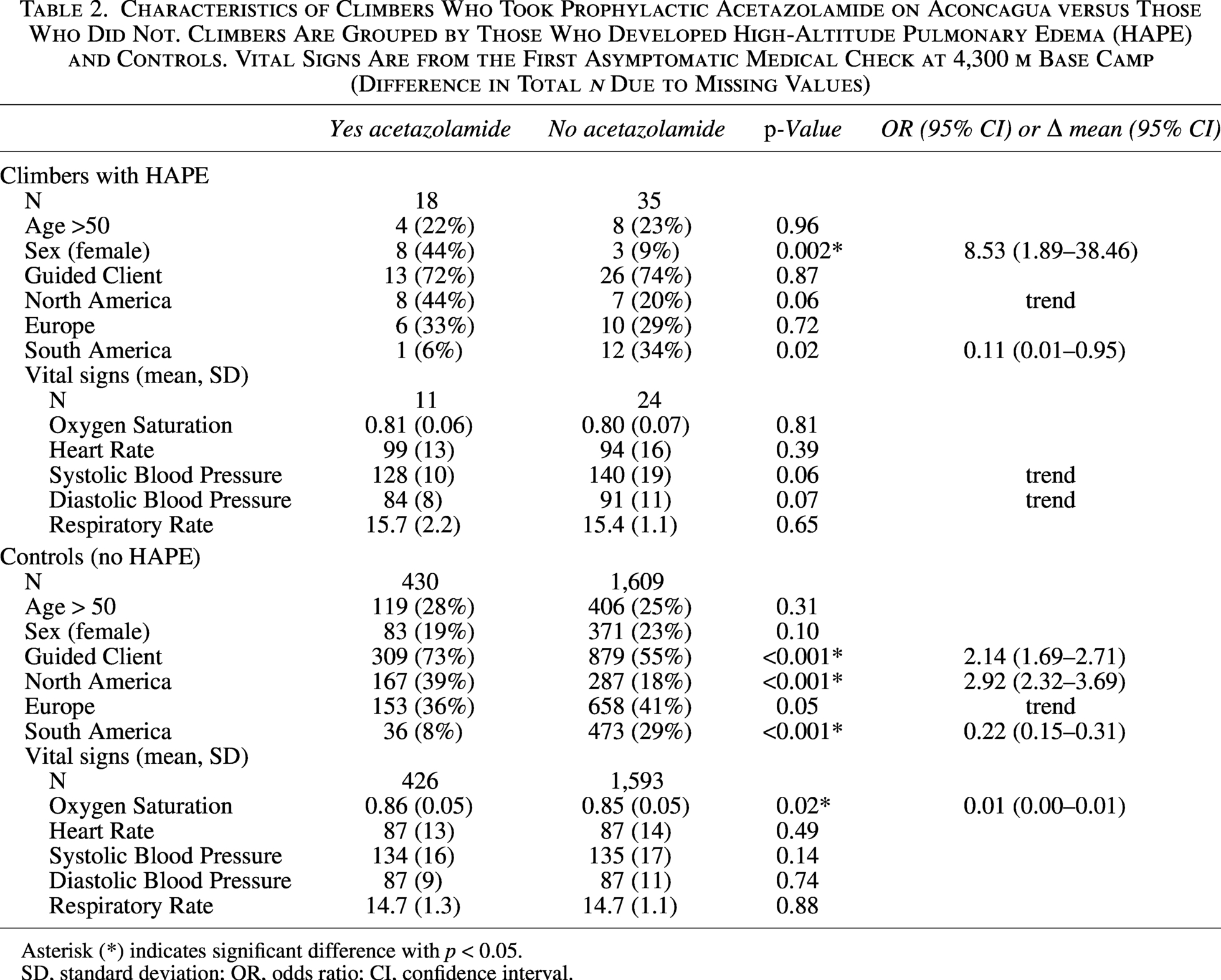
Asterisk (*) indicates significant difference with p < 0.05.
SD, standard deviation; OR, odds ratio; CI, confidence interval.
During diagnosis and evacuation for HAPE, the climber’s (patient’s) mean vital signs for this evacuation medical encounter at the 4,300 m base camp were as follows: oxygen saturation 69% (SD 14%), heart rate 105 bpm (SD 15 bpm), systolic blood pressure 131 mmHg (SD 19 mmHg), diastolic blood pressure 85 mmHg (SD 11 mmHg), and respiratory rate 22.1 breaths per minute (SD 6.2 breaths/min).
Discussion
Aconcagua mountaineers who were screened at 4,300 m and later developed HAPE had lower oxygen saturations and higher heart rates compared to controls. This study represents the first large study to compare the medical screening data of expedition mountaineers who developed HAPE with a control population. This study furthers understanding of HAPE on Aconcagua, which is more common than on other Seven Summit peaks such as Denali or Everest (Brillhart et al., 2025b).
At 4,300 m, oxygen saturation of 85% and heart rate in the 80s appear to be average among all mountaineers. Oxygen saturation below 80% with tachycardia above the upper 90s should raise concern that HAPE could develop, and more days acclimatizing may be warranted before further ascent. However, the sensitivity and positive predictive value remain low for this 80% oxygen saturation cutoff due to the relative rarity of climbers diagnosed with HAPE among the total population of climbers and other clinical factors besides oxygen saturation that contribute to the diagnosis of HAPE. Tachypnea over 15 breaths per minute during asymptomatic medical screening may also be concerning for the subsequent development of HAPE, though the small significant increase found of 1 breath per minute is of marginal clinical value.
Notably absent from medical service data was rate of ascent data, due primarily to the early screening that climbers receive at Aconcagua base camps before sleeping over 4,300 m. Aconcagua climbers have been documented to have rapid average ascent rates over 600 m/day (Pesce et al., 2005). As gradual ascent is recommended as the primary method to prevent HAPE (Luks et al., 2024), future ascent rate research is indicated to better understand HAPE risks among Aconcagua climbers. Ascent rate research could also specifically evaluate questionably at-risk groups such as guided clients, those from North America, and those taking acetazolamide. Certain climber groups may ascend faster, and medication could mask AMS symptoms, allowing climbers to ascend more rapidly. The medical service could also consider methods to track ascent rate and therefore potential risk of developing high-altitude illness among climbers undergoing medical screening in future climbing seasons, though this task is not currently mandated by APP.
Other HAPE contributors could be considered as potential confounders in future studies. Inflammatory contributors such as from viral exposure are debated and may play a role in the development of HAPE, in addition to genetic predisposition and strenuous exercise. (Femling et al., 2025; Miserocchi, 2025; Swenson, 2020) Climbers who developed HAPE trended toward increased prophylactic acetazolamide use, though this result was not significant in a multivariate adjusted model.
Acetazolamide has minimal adverse effects and is generally recommended to facilitate acclimatization and prevent AMS in climbers at moderate and high risk of AMS (Luks et al., 2024). However, acetazolamide has not been shown to prevent HAPE in climbers and is not recommended for specific treatment or prophylaxis of HAPE (Berger et al., 2022; Luks et al., 2024). The questionable association between prophylactic use of acetazolamide and HAPE in the current study does not suggest causation, nor that any change in clinical practice is warranted. Rather, further research into ascent rate and acetazolamide use is indicated to better understand any association that may exist. Climbers on Aconcagua should remain aware that acetazolamide does not prevent life-threatening high-altitude illness such as HAPE and continue to adhere to a principal of gradual ascent. As Aconcagua climbers have been shown to have relative inexperience with high-altitude (Borm et al., 2011), APP educational initiatives to prevent altitude illness such as HAPE could be further explored.
Limitations
Study limitations include a retrospective design. Some climbers in the control population did not have complete records such as all screening vital signs or documentation of acetazolamide use. The ascent profile was not collected nor identifiable by medical service data. Medication use was self-reported, dosing was not standardized, and the study did not control for all prophylactic medications. The clinical diagnosis of HAPE depended on individual physicians, which could have affected results.
Conclusions
This study is the first to review a detailed medical screening database of over 2,000 expedition mountaineers for trends in the development of HAPE. Asymptomatic screening of climbers at 4,300 m with peripheral blood oxygen saturation below 80% and tachycardia greater than 96 bpm should raise concern for subsequent development of HAPE. Gradual ascent should continue to be emphasized to facilitate acclimatization and prevent life-threatening high-altitude illness such as HAPE on Aconcagua. These findings may be used to aid in future climber education, safety initiatives, and prevention of life-threatening high-altitude illness such as HAPE among expedition mountaineers.
Authors’ Contributions
Conceptualization, methodology, investigation, validation, writing review and editing: A.B., M.E., J.S., B.A., R.D., I.G., T.H., A.S., R.P., and S.M. Investigation, validation, formal analysis, writing review and editing: P.C. Supervision, formal analysis, and original draft preparation: A.B.
Ethical Considerations
This study was approved by the Institutional Review Board of the University of Utah. Permission to conduct the study was granted by the medical service of APP.
Data Availability
Data were made available only to the research team by the medical service of APP.
Footnotes
Acknowledgments
The authors acknowledge the medical service of Aconcagua Provincial Park for their screening and care of climbers on Mount Aconcagua, and for their permission to conduct this study.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article, other than B.A., R.D., R.P., A.S., and J.S. work for the medical service of APP.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.