
Abstract
Pena, Eduardo, Samia El Alam, Juliane Hannemann, and Rainer Böger. Compliance and genetic variability are determinants of the success of
Background:
Asymmetric dimethylarginine (ADMA) is a risk biomarker of high-altitude pulmonary hypertension (HAPH). ADMA is inactivated by dimethylarginine dimethylaminohydrolase (DDAH)1 and 2. Single nucleotide polymorphisms in these genes contribute to genetic predisposition for HAPH. Supplementation with
Methods:
Twenty male volunteers were randomly assigned to receive 6 months of A/C or placebo; PAP was assessed by echocardiography.
Results:
Conclusion:
Our data show that A/C supplementation may offer an opportunity to alleviate the altitude-induced increase in PAP; however, long-term compliance and genetic factors may affect outcome.
Keywords
Introduction
Hypoxic pulmonary vasoconstriction (HPV) is a major mechanism contributing to high altitude pulmonary hypertension (HAPH) during chronic-intermittent hypobaric hypoxia (CIH) (Brito et al., 2018; Böger and Hannemann, 2020). Having been discovered as a physiological mechanism in the 1940s (von Euler and Liljestrand, 1946; Blakemore et al., 1955), we now know that signal transduction pertaining to endothelium-derived nitric oxide (NO) is involved. NO is a potent vasodilator; its reduced production and/or biological action in the hypoxic pulmonary vasculature have been demonstrated (Böger and Hannemann, 2020).
Asymmetric dimethylarginine (ADMA) is an endogenous inhibitor of NO synthesis (Böger et al., 2000, Böger et al., 2004); ADMA concentration is increased in individuals exposed to chronic hypobaric hypoxia (CH) or CIH (Lüneburg et al., 2017; Brito et al., 2018; Verratti et al., 2020). In a previous study, we demonstrated the progressive increase in ADMA plasma concentration during 6 months of exposure to CIH in a young, healthy, male Chilean population. We also found that ADMA is a biomarker predicting the risk of HAPH (Siqués et al., 2019). This finding offers an opportunity to assess an individual’s risk of HAPH before ascent to high altitude; it also has a therapeutic perspective: ADMA exerts its effects by competitively displacing
We therefore hypothesized that dietary supplementation with
We have previously shown that a combination of
We performed the present clinical pilot study to test whether administration of an oral
Patients and Methods
Study participants and study protocol
We included 20 healthy male army draftees; none of them had been exposed to high altitude before. Written informed consent was obtained from all study participants before the study. The protocol was approved by the Ethical Committee of Universidad de Tarapacá, Arica, Chile (N°08/2023).
During the study period of 6 months, the participants adhered to a shift regimen of 5 days at high altitude (HA; 3,550 m) followed by 2 days of recovery at sea level (SL). Their daily routine at high altitude comprised moderate physical activity and a standardized diet (3,000 kcal daily). The supplements were handed to the participants in containers that contained supply for 1 month each, that is, each participant received six containers with supplements during the study. Compliance was expressed as a percentage of unopened containers returned by participants relative to the total supplied.
Measurements were taken at baseline (month 0; complete investigation incl. echocardiography), month 1 (sampling of dried blood spots only), and month 6 (complete investigation incl. echocardiography).
Preparation and administration of supplements
Dietary supplements contained a mixture of
Analysis of l -arginine and its metabolites by UPLC-MS/MS in dried blood spots
Isolation of DNA from dried blood and genotyping
DNA was isolated from dried blood spots using a salting-out procedure as reported previously (Hannemann et al., 2021b). DNA concentration was determined using a nanophotometer NP60 (Implen, Munich, Germany). Genotyping of single nucleotide polymorphisms (SNPs) was performed using single-tube human TaqMan SNP Genotyping Assays (Thermofisher Scientific, Dreieich, Germany) as described before (Hannemann et al., 2021a). We genotyped two SNPs in the ARG1 gene (rs2246012 and rs2781667), ARG2 gene (rs3742879 and rs2759757), and DDAH2 gene (rs805304 and rs2272592), and three SNPs in the DDAH1 gene (rs1241321, rs480414, and rs233112), respectively, after having excluded SNPs that were in strong linkage disequilibrium with each other by checking the LDLink database of the National Cancer Institute, USA (https://ldlink.nci.nih.gov/). In order to test for the combined effects of DDAH1 and DDAH2 on ADMA concentration and the combined effects of ARG1 and ARG2 on
Echocardiography
Echocardiography was performed by trained cardiologists according to the standards set forth in the 2010 guideline of the American Society of Echocardiography (Rudski et al., 2010). Left ventricular ejection fraction (LVEF) was measured using the standard Simpson method. The diameter and respiratory variability of the inferior vena cava was measured to estimate right atrial pressure (RAP). Right ventricular pressure gradient (RVPG) was calculated from the peak velocity of the tricuspid regurgitation using the simplified Bernoulli equation; systolic pulmonary artery pressure (sPAP) was calculated as RVPG + RAP (Yock and Popp, 1984; Rudski et al., 2010). Mean pulmonary artery pressure (mPAP) was calculated from the formula: mPAP = (0.61 × sPAP) + 2 (Chemla et al., 2004). Due to small numbers of echocardiographic investigations at month 6, no formal statistical analyses were performed on echocardiographic data.
Calculations and statistical analyses
From biomarker concentrations measured, we calculated the
Results
Baseline characteristics of the study population
We recruited 20 healthy, male study participants aged 20.0 ± 1.8 years. They had a mean body mass index of 24.8 ± 3.6 kg/m2 and no concomitant chronic or acute diseases. All study participants had cardiac dimensions and function parameters within the normal range of healthy individuals in the baseline echocardiographic assessment with no significant differences between both groups (Table 1). Concentrations of
Baseline Characteristics of the Study Population
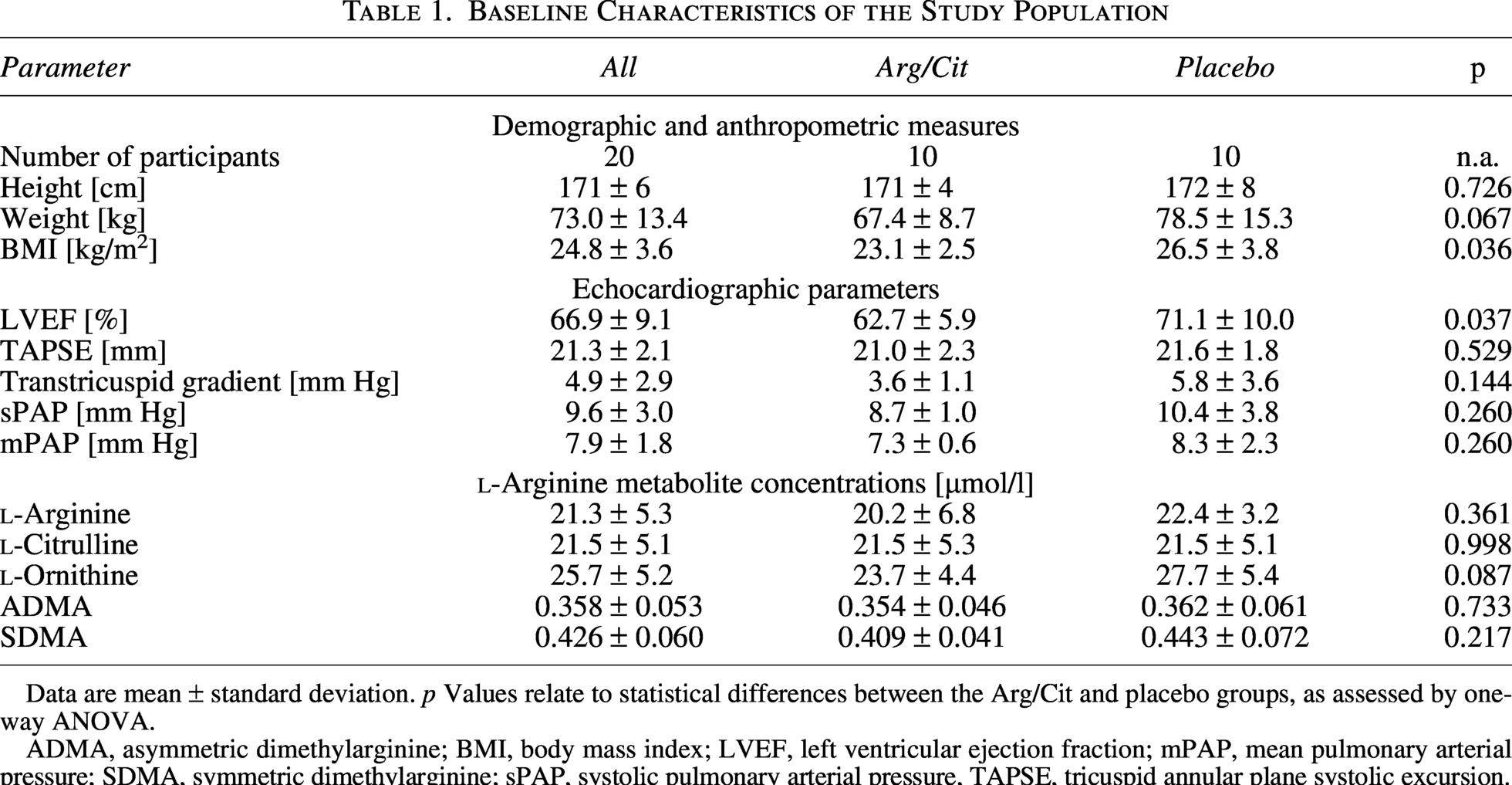
Data are mean ± standard deviation. p Values relate to statistical differences between the Arg/Cit and placebo groups, as assessed by one-way ANOVA.
ADMA, asymmetric dimethylarginine; BMI, body mass index; LVEF, left ventricular ejection fraction; mPAP, mean pulmonary arterial pressure; SDMA, symmetric dimethylarginine; sPAP, systolic pulmonary arterial pressure, TAPSE, tricuspid annular plane systolic excursion.
Effects of high altitude exposure and l -arginine supplementation on blood metabolite concentrations
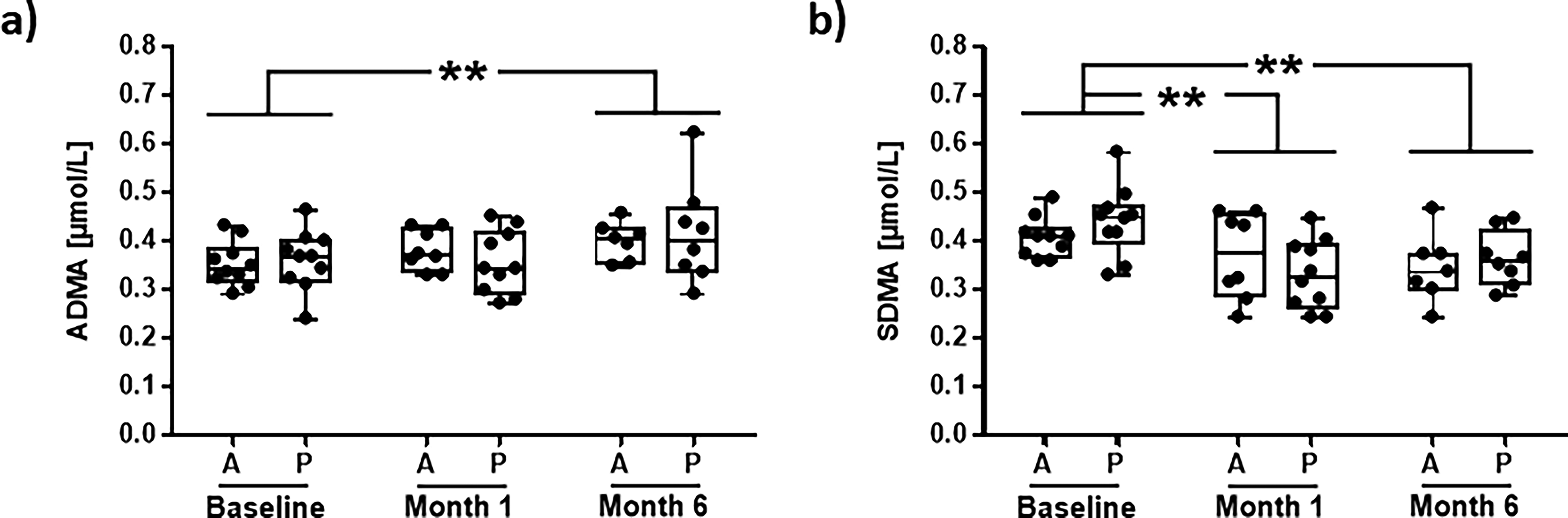
ADMA concentration increased slightly but significantly, with no significant difference between both intervention groups during exposure to CIH (0.36 ± 0.06 to 0.41 ± 0.08 µmol/l; p = 0.0015), whereas SDMA concentration was significantly reduced (0.44 ± 0.06 to 0.36 ± 0.06 µmol/l; p = 0.0011; Fig. 1a and b).
Concentrations of
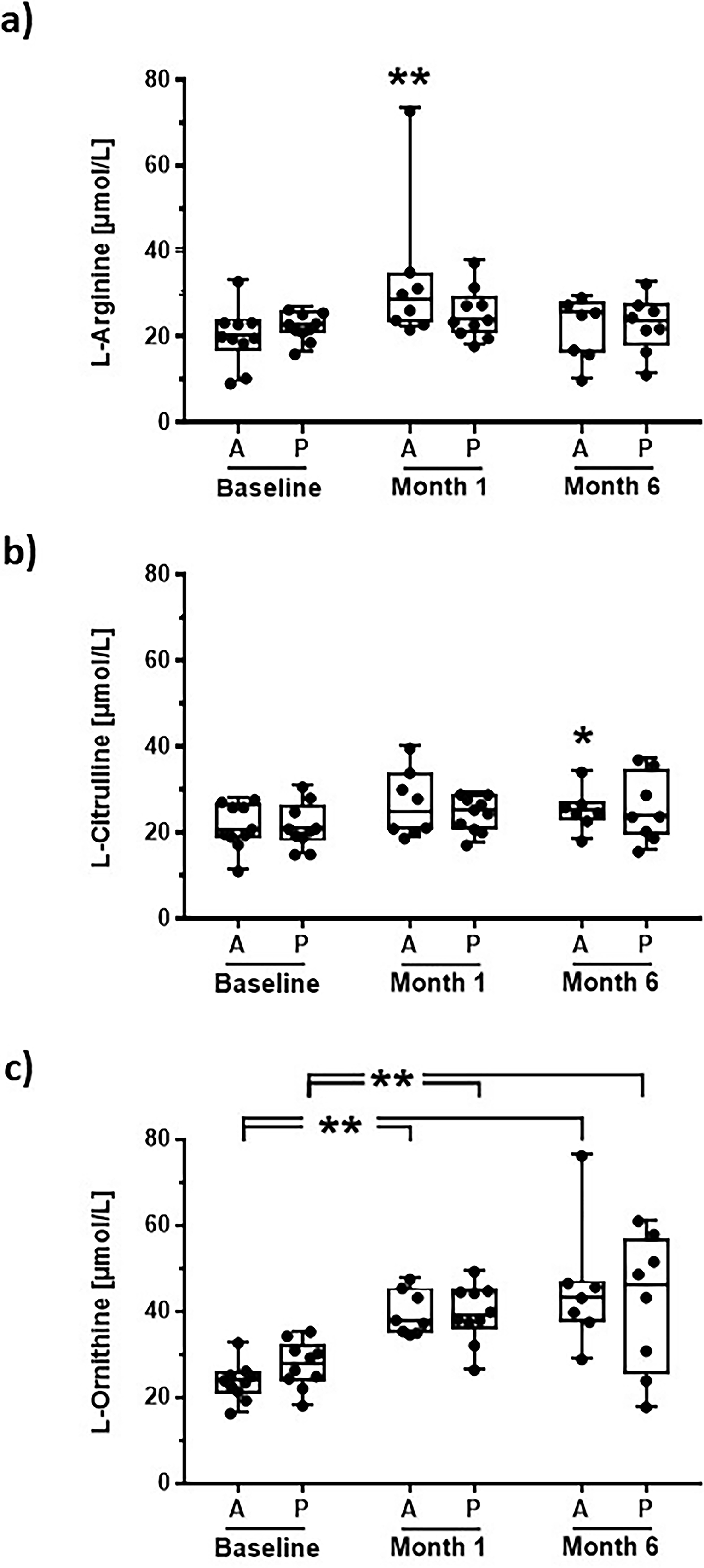
In month 1 of the study, we observed a significant 60% increase in mean
Concentrations of
Compliance of study participants with supplement intake
Under the conditions of a fully voluntary study participation with no infrastructural means of maintaining compliance of study participants at the high-altitude site during the 6 months’ duration of this pilot trial, 18 individuals agreed to provide dried blood spots for metabolite measurements at month 1, but only 12 participants (60% of the initial study group of 20 participants) participated in the 6 months’ follow-up investigation, which included clinical parameters and echocardiography.
Based on quantification of
Consistent with the above, at the end of the study, the mean adherence in the A/C group was 80.6%. Specifically, three participants consumed all six containers (100% adherence), one participant consumed five containers (83.3%), and two participants consumed three containers (50%). Overall, 66.7% of participants in this group achieved adherence ≥80%. In contrast, the placebo group showed a mean adherence of 66.7%. Within this group, three participants consumed all six containers (100%), one participant consumed four containers (66.7%), and two participants consumed three containers (50%). Consequently, only 50% of participants in the placebo group reached adherence ≥80%.
Association of arginase gene polymorphisms with blood l -arginine and l -ornithine concentrations
None of the ARG1 SNPs were significantly associated with
To assess the influence of both arginase genes on
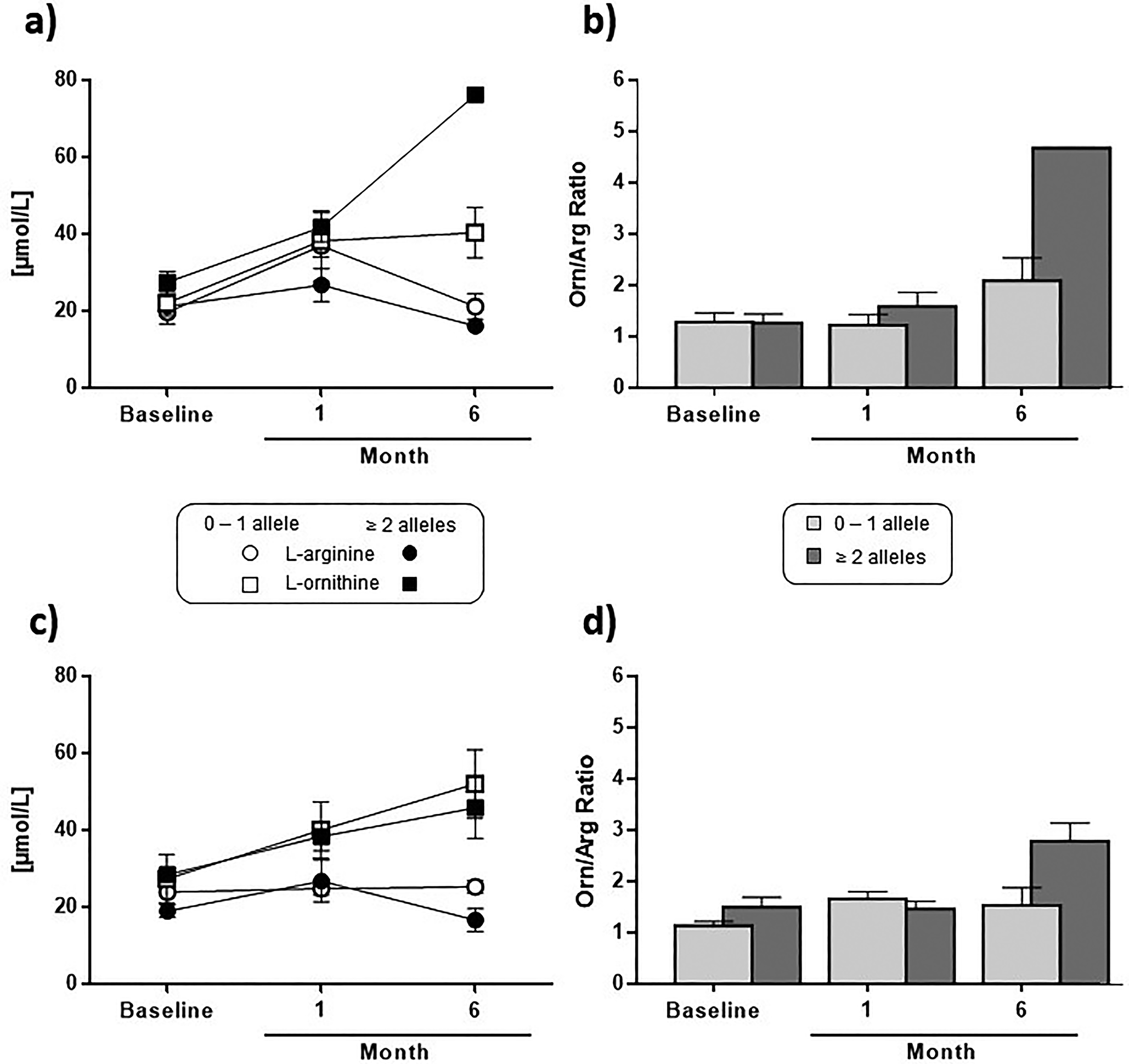
None of the ARG1 nor ARG2 SNPs showed significant associations with
Association of DDAH gene polymorphisms with blood ADMA concentrations
SNPs in the DDAH1 and DDAH2 genes were not significantly associated with ADMA blood concentrations in this study. However, a previously described DDAH1/DDAH2 haplotype (Hannemann et al., 2021a) was significantly associated with ADMA concentration: Carriers of two or more alleles of the haplotype had a significantly higher ADMA concentration at 6 months of CIH exposure, whereas carriers of less than two alleles showed no significant increase in ADMA (Fig. 4).

ADMA concentration in dried blood spots at baseline and at 6 months of chronic intermittent hypoxia in carriers of 0–1 active allele or 2 or more active alleles of the combined DDAH1/DDAH2 haplotype. Data represent median and interquartile range, with whiskers extending to the range of measurements. **p < 0.01 for comparison with baseline values.
Echocardiographic assessment of cardiac function after CIH exposure
In our exploratory analysis of echocardiographic data, we observed no significant change in mean LVEF from month 0 to month 6 in either of the two groups (Fig. 5a). However, we noted trends toward a higher increase in parameters of right ventricular pressure in the placebo group as compared to the A/C group (Fig. 5b–d). Whilst we performed no formal test for statistical significance due to missing data, there was a clear and uniform trend toward an alleviated increase in right ventricular pressure in the A/C group.
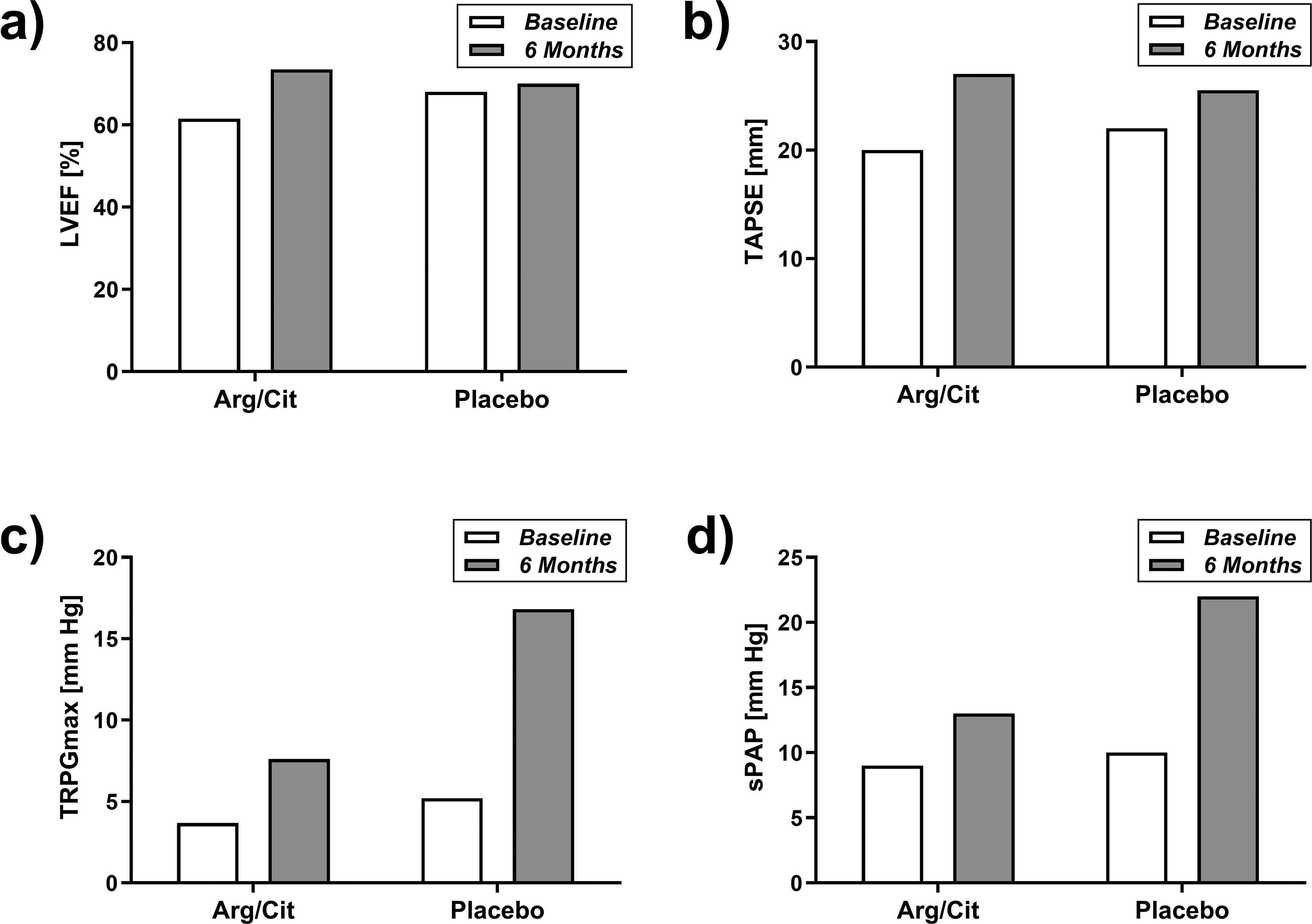
Echocardiographic parameters of left and right ventricular function and pulmonary artery pressure at baseline and at 6 months of chronic intermittent hypoxia. (
Incidence of acute mountain sickness
The Lake Louise Score was 2.8 ± 2.1 immediately after the first ascent to high altitude with no significant difference between both groups. It was 2.2 ± 2.3 after 1 month and declined to 1.2 ± 1.7 after 6 months (Table 2).
Lake Louise Score of Acute Mountain Sickness
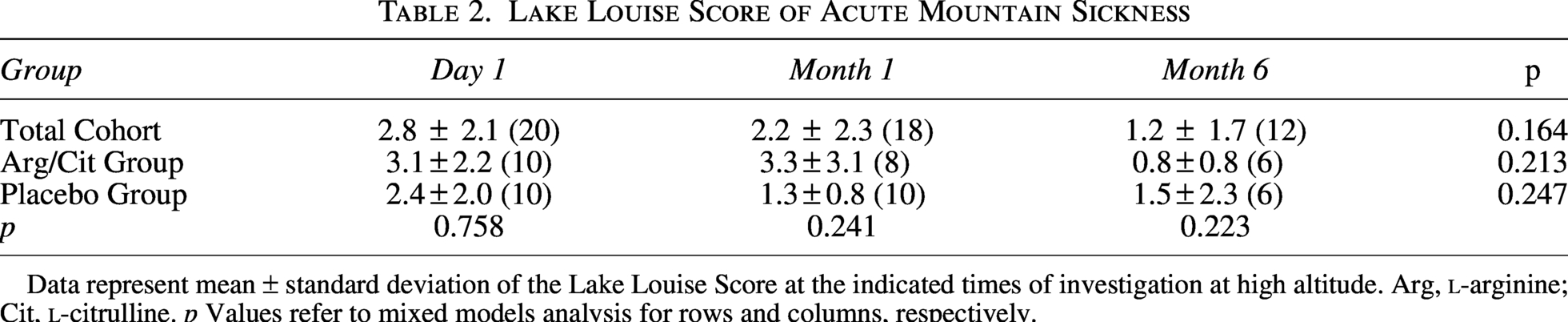
Data represent mean ± standard deviation of the Lake Louise Score at the indicated times of investigation at high altitude. Arg,
Discussion
We performed this pilot study to assess conditions that affect the conduct and outcome of an interventional trial under the conditions of high-altitude exposure. Although direct results from this study are difficult to interpret due to the small number of participants, our principal findings are as follows:
Supplementation of study participants with A/C during high altitude exposure is feasible and bears promising potential as a measure of prevention of increased PAP and, consequently, HAPH. The major factors influencing variability of outcome data are genetic variability between study participants and limited compliance of participants with intake of study product(s). Adherence of study participants to present at follow-up visits strongly depends on measures of study management to maintain contact, send reminders, and clearly define appointments in line with individual work schedules.
Biological plausibility and interindividual variability
Studies have assessed HPV, which results in an increased PAP and, when extended over prolonged periods of time, may lead to pulmonary hypertension (Siqués et al., 2019; Hannemann et al., 2020). For example, HAPH may be considered a cause of long-term morbidity and mortality among workers at high altitude in the Andean region, who often maintain an intermittent regimen of several days of work at high altitude, followed by some days of recovery at SL (Brito et al., 2018; Yang et al., 2025). Our group has previously reported the prevalence of manifest HAPH to be as high as 9% among long-term high-altitude mining workers in Chile (Brito et al., 2018). Given the high number of workers undergoing such CIH work schedules (Brito et al., 2007; Reveco et al., 2026), this is also a matter of health concern for the Andean countries’ health systems, as follow-up cost and loss of work ability are enormous (Reveco et al., 2026).
In previous studies our group has identified upregulation of the endogenous inhibitor of NO synthesis, ADMA, to be a prospective marker of the risk of HAPH (Siqués et al., 2019). Amongst other experimental proof, a causal involvement of ADMA in HPV was suggested by enhanced pulmonary arterial vasoconstriction in DDAH1 k.o. mice (Leiper et al., 2007; Wang et al., 2019). Reversely, DDAH1-overexpressing mice showed decreased HPV as compared to wild-type littermates (Bakr et al., 2013). As we have shown before that the biological effects exerted by ADMA can be overcome by increasing availability of
Another issue that must be considered in studying A/C supplementation in HAPH-prone individuals is the genetic makeup of study participants. Our previous data showed that DDAH1 and DDAH2 SNPs, which affect enzyme activity and/or expressional regulation of these enzymes, have a strong association not only of blood ADMA concentration but also of HAPH risk (Hannemann et al., 2021a). Specifically, in this study two SNPs in the DDAH1 and DDAH2 genes (rs233112 and rs805304) were significantly associated with ADMA concentration and HAPH incidence. Therefore, our present data, although generated in a very small group of participants in this pilot study, is consistent with our previous finding by showing that a DDAH1/DDAH2 haplotype combining these two SNPs was significantly associated with high ADMA concentration after 6 months of CIH. Our present study also supports the prior finding that SNPs in the arginase genes affect individuals’ responses to
Notably, we observed that
Compliance as a central determinant of interpretability
A key finding of this study is the progressive reduction in adherence to the study supplement throughout follow-up, which fundamentally shaped the interpretability of our results. High initial adherence likely enabled the detection of short-term biological effects, such as early increases in
Limitations
Considering this drawback of our pilot study, we have refrained from plotting standard deviations and performing statistical tests for echocardiographic outcome variables. Nonetheless, our current data present a promising picture of the potential effect of the dietary intervention on the pulmonary circulation. We observed no trend of any differences in LEVF, neither over time of high-altitude exposure nor between treatment groups. By contrast, the tricuspid annular plane systolic excursion trended to increase more in A/C-supplemented individuals than in those allocated to placebo. Most intriguingly, the maximal tricuspid regurgation pressure (TRPGmax) showed a steep increase during high altitude exposure in the placebo group (in fact, it almost tripled), whereas this increase was attenuated in the A/C group. The same was true for systolic and mPAP, which both increased more strongly in the placebo group than in the A/C group. As mentioned above, we interpret these differences between treatment groups with considerable caution. Nonetheless, the observed trends provide a reasonable basis to anticipate that a future, adequately powered interventional trial may have the potential to demonstrate a preventive effect on PAP elevation and, possibly, on HAPH incidence in individuals exposed to CIH. Finally, we did not assess systemic blood pressure because the study enrolled young, healthy, normotensive participants and was not powered to detect systemic hemodynamic changes. For this reason, our conclusions are restricted to pulmonary responses. Nonetheless, it is important to acknowledge that prior evidence indicates a link between ADMA, high-altitude exposure, and systemic blood pressure regulation, as demonstrated by Verratti et al. (2020), which further supports the physiological relevance of the ADMA–NO pathway in hypoxic environments.
Implications for future trials
Our findings, which align with previous observations from our group and others, highlight several methodological considerations that should guide the design of future interventional trials. Beyond informing sample size calculations, this pilot study underscores the need for active, continuous participant engagement to maintain adherence—an essential determinant of interpretable outcomes. We therefore recommend that a dedicated study team member remain available throughout the entire study period to maintain regular contact with participants, not only at scheduled follow-ups but also between visits, to enhance compliance and retention. Furthermore, coherent echocardiographic data require consistent acquisition across time; relying on clinical personnel who must balance routine duties with research tasks is insufficient. Instead, future trials should incorporate an experienced echocardiographer as part of the study team to ensure standardized image acquisition by the same observer and to guarantee availability for all planned assessments. These measures will strengthen data completeness, reduce variability, and ultimately improve the reliability of long-term outcomes in CIH intervention research.
Footnotes
Acknowledgments
The authors gratefully thank Alina Haack for excellent technical assistance, Natalia Bazaes for her collaboration in the project, and the Chilean Army for their logistical support during fieldwork.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was in large part funded by the co-authors’ academic institutions and partially supported by the project funded by FIC GORE-TARAPACÁ (grant BIP-400187737-0). In addition, both research groups are joint members of the DECIPHER Institute for Research on Pulmonary Hypoxia, which was initiated with funds provided by the German Federal Ministry of Education and Research. RB is the recipient of an ERC Advanced Grant by the European Research Council (grant 101096706–NO PRESSURE). Views and opinions expressed are, however, those of the author(s) only and do not necessarily reflect those of the European Union or the European Research Council. Neither the European Union nor the granting authority can be held responsible for them.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.