
Abstract
Zhuoga Danzeng, Luobu Gesang, Yangzong Suona, Yuansheng Wang, Yangjin Baima, Bai Ci, Ju Huang, Zhuoma Ciren, Rui Zhang, Binyun Liu, and Quzong Zhaxi. Establishing Early Intervention Thresholds for High-Altitude Polycythemia: Evidence from a Cross-Sectional Study of Tibetan Residents. High Alt Med Biol. 00:00–00, 2026.
Background:
High-altitude polycythemia (HAPC), defined by elevated hemoglobin levels, is a key feature of chronic mountain sickness, yet the “intermediate zone” preceding overt HAPC remains poorly understood. This cross-sectional study aimed to define evidence-based thresholds for early intervention in high-altitude populations.
Methods:
A total of 2,819 indigenous Tibetan residents (≥18 years) living at altitudes ≥ 4,500 m were classified into three groups based on hemoglobin levels: normal (males: 130–175 g/l; females: 115–150 g/l), intermediate (males: 175–210 g/l; females: 150–190 g/l), and HAPC (males: ≥210 g/l; females: ≥190 g/l). We assessed clinical phenotypes, organ function, and metabolic parameters through questionnaires, physical exams, biochemical analyses, and echocardiography. Logistic regression identified health risks for each group.
Results:
Revealed that participants in the intermediate and HAPC groups exhibited significant abnormalities compared with the normal group: increased waist circumference (p < 0.001), elevated low-density lipoprotein cholesterol (LDL-C; p < 0.001), and higher uric acid levels (p < 0.001), with an increased risk of hyperuricemia (OR = 2.077, p < 0.001). Additionally, SpO2 was lower in the intermediate (83%) and HAPC (80%) groups, indicating worsening hypoxia (p < 0.001). Organ function abnormalities included elevated ALT levels (p < 0.001) and right ventricular wall thickness (p = 0.025).
Conclusion:
These findings suggest that individuals in the intermediate zone exhibit early signs of organ dysfunction, indicating a “pre-HAPC state.” We advocate for a risk-stratified approach to early intervention in high-altitude illness.
Background
High-altitude polycythemia (HAPC) is the most representative maladaptive disease induced by chronic high-altitude hypoxia, with its core pathological feature being compensatory hemoglobin (Hb) elevation to improve tissue oxygen supply (Villafuerte et al., 2022). Current clinical diagnostic criteria (Hb ≥ 210 g/l for males, ≥190 g/l for females; León-Velarde et al., 2005). Effectively identify typical cases but overlook the significant population with Hb levels between normal upper limits and diagnostic thresholds—the “intermediate zone.” This population constitutes a significant proportion of high-altitude residents, yet their potential health risks remain systematically unevaluated, creating a blind spot in high-altitude medicine research.
Recent studies suggest that pathological effects of Hb do not begin at diagnostic thresholds but accumulate dynamically across concentration gradients (León-Velarde et al., 2000; Pillai et al., 2024). Even when Hb levels do not meet HAPC criteria, elevated blood viscosity can lead to microcirculatory disorders and induce subclinical cardiovascular remodeling (e.g., right ventricular hypertrophy, pulmonary arterial pressure elevation) and metabolic disorders (insulin resistance, lipid abnormalities) (Liu et al., 2024; Ouyang et al., 2024; Savina et al., 2024). More concerningly, intermediate zone individuals commonly exhibit occult hypoxemia (SpO2 <90%), potentially activating inflammation-oxidative stress cascade reactions through hypoxia-inducible factor (HIF) pathways, accelerating multiorgan dysfunction (Gesang et al., 2019; Painschab et al., 2015). However, existing evidence primarily focuses on diagnosed HAPC patients, while systematic phenotypic analysis and mechanistic exploration of the intermediate zone remain severely lacking, causing clinical interventions to lag behind pathological progression.
This study targets indigenous Xizangan populations living at altitudes above 4,500 meters, focusing on the “intermediate zone” population based on Hb levels. We conducted comprehensive assessments of physiological indicators, biochemical markers, cardiovascular imaging, and multiorgan function. For the first time, we discovered that “intermediate zone” individuals already demonstrate metabolic abnormalities, worsening hypoxia, and multiorgan functional changes, revealing a pre-HAPC state characterized by significant metabolic abnormalities and various pathophysiological alterations before HAPC onset, providing a basis for early intervention.
Methods
Study design
This cross-sectional study employed a stratified cluster sampling approach, enrolling 2,819 indigenous Tibetan residents aged ≥18 years from 51 villages across 8 townships in Nyima, Amdo, and Shuanghu counties of Nagqu Prefecture, Xizang, China. The average altitude of the study locations was ∼4,850 m (range: 4,500-5,200 m). The study population was derived from the Health Improve of Very High Altitude (HI-VHA) study, with clinical trial registration number (CHICTR2200061812). The study was approved by the Ethics Committee of People’s Hospital of Xizang Autonomous Region (approval number: ME-TBHP-21-028). All subjects provided informed consent and received privacy protection.
Study population and sampling method
This study primarily targets residents from three counties scheduled for relocation. A stratified sampling method was employed to recruit participants, with a total sample size exceeding 2,556. To account for a potential loss to follow-up rate of <10%, the minimum required sample size was determined to be 2,840. Participants were stratified into 36 subgroups based on residence (three counties), age (7–20, 20–30, 30–40, 40–50, 50–60, and ≥60 years), and gender (male/female) (3 × 6 × 2 stratification). Each stratum was required to contain at least 10% of the total sample.
Sample size calculation
The sample size estimation was based on the largest standard deviation (SD) observed among primary outcome measures, specifically platelet count (PLT). Using data from prior literature, the SD for PLT intervals in high-altitude populations ranges between 40 × 109/L and 60 × 109/L; a conservative value of 50 × 109/L was selected for this study. The minimum sample size per stratum was calculated using the formula:
Based on international consensus standards (León-Velarde et al., 2005) and target population characteristics, participants were categorized by Hb levels into three groups: Normal group: males 130–175 g/l, females 115–150 g/l; Intermediate group: males 175–210 g/l, females 150–190 g/l; HAPC group: males >210 g/l, females >190 g/l. Inclusion criteria: (1) age ≥18 years; (2) Xizang residents living at high altitudes (≥4,500 m) for at least three generations; (3) voluntary participation with signed informed consent. Exclusion criteria: (1) recent (within 6 months) acute illness or infection, Acute disease or infection was defined as any condition meeting one or more of the following criteria within the 6 months before enrollment: (a) hospitalization for any acute illness; (b) prescription of systemic antibiotics, antivirals, or corticosteroids; (c) self-reported fever (body temperature ≥38.0°C) lasting ≥3 days; or (d) laboratory evidence of active infection (white blood cell count >10 × 109/L and/or C-reactive protein >10 mg/l), confirmed by medical records or structured participant interview.; (2) previously diagnosed severe cardiovascular disease (e.g., chronic heart failure, coronary heart disease) or chronic lung disease (e.g., chronic obstructive pulmonary disease); (3) medication affecting Hb or metabolic indicators (e.g., erythropoietin, glucocorticoids); (4) pregnant or lactating women.
Data collection and measurements
Clinical indicators
All subjects underwent standardized questionnaire surveys and physical examinations, collecting: demographic information (age, sex, smoking history, alcohol consumption, tea drinking habits, residence altitude and duration); physiological indicators including height, weight (calculating body mass index [BMI = weight(kg)/height2(m2)]), waist circumference, hip circumference (calculating waist-to-hip ratio [WHR = waist/hip]); blood pressure (measured twice on the right upper arm after 10 minutes of rest, averaging the values); oxygen saturation measurements including blood oxygen saturation (SpO2) measured at rest using a pulse oximeter (Nonin Onyx 9590, USA) on the left index finger; and cerebral oxygen saturation (rSO2) measured using near-infrared spectroscopy (INVOS 5100 C, USA) in the left and right prefrontal cortical regions.
Biochemical indicators
After 8–12 hours of fasting, 5–10 ml venous blood was collected by professional medical staff, divided into Ethylene Diamine Tetraacetic Acid [EDTA] anticoagulation tubes and coagulation tubes, promptly centrifuged, stored at 4°C, and tested within 24 hours. The following parameters were measured using an automated biochemical analyzer (Cobas 8000, Roche, Switzerland): liver function indicators (alanine aminotransferase [ALT], aspartate aminotransferase [AST], total protein [TP], albumin [ALB], GLO, total bilirubin [TBIL], direct bilirubin [DBIL], indirect bilirubin, [IBIL]); renal function indicators (blood urea nitrogen [BUN], Cr, uric acid [UA], estimated glomerular filtration rate [eGFR] calculated using the Chronic Kidney Disease Epidemiology Collaboration [CKD-EPI] formula); lipid metabolism (total cholesterol [TC], triglycerides [TG], high-density lipoprotein-cholesterol [HDL-C], LDL-C); inflammation and metabolism-related indicators (high-sensitivity C-reactive protein [Hs-CRP], homocysteine [HCY], Fasting Plasma Glucose [FPG]); complete blood count (CBC) including red blood cells (RBC), HGB, hematocrit [HCT], mean corpuscular volume [MCV], mean corpuscular hemoglobin [MCH], mean corpuscular hemoglobin concentration [MCHC], red cell distribution width [RDW], white blood cells [WBC], and differential, PLT.
Echocardiography
All subjects underwent transthoracic echocardiography (TTE) examination (GE Vivid E95, USA). The examinations were conducted by two experienced echocardiographers (each with >5 years of experience) who were blinded to subject grouping. Each subject was examined by one of the two physicians, and no duplicate measurements were performed for consistency testing. The following cardiac structural and functional parameters were assessed: (1) Right ventricular function: right ventricular wall thickness (RVWT), right ventricular anteroposterior diameter (RVAPD), right ventricular pre-ejection period (RPEP), right ventricular ejection time (RVET); (2) Left ventricular function: left ventricular end-diastolic diameter (LVEDd), left ventricular end-systolic diameter (LVESd), left ventricular ejection fraction (LVEF), interventricular septal thickness (IVST), left ventricular posterior wall thickness (LVPWT); (3) Pulmonary circulation pressure: main pulmonary artery diameter (MPA), pulmonary artery acceleration time (AcT), right ventricular outflow tract diameter (RVOT); (4) Atrial measurements: right atrial diameter (RAD), left atrial diameter (LAD); (5) Right heart function assessment: tricuspid annular plane systolic excursion (TAPSE).
Outcome indicators
Health outcomes were defined using the following criteria: (1) hypertension (HTN): systolic blood pressure (SBP) ≥140 mmHg or diastolic blood pressure (DBP) ≥90 mmHg, or diagnosed HTN currently taking antihypertensive medication; (2) Liver dysfunction: ALT > 40 U/L or AST >40 U/L or TBIL > 27 μmol/L (male)/22 μmol/L (female); (3) Renal dysfunction: eGFR < 60 ml/min/1.73m2 or creatinine >97 μmol/L (male)/73 μmol/L (female) or proteinuria > 2+; (4) Hyperuricemia: uric acid > 420 μmol/L (male)/360 μmol/L (female); (5) Dyslipidemia: TC > 5.2 mmol/L or LDL-C > 3.0 mmol/L or TG > 1.7 mmol/L or HDL-C < 1.0 mmol/L (male)/1.3 mmol/L (female); (6) Inflammatory state: Hs-CRP > 3 mg/l; (7) Hypoxic state: SpO2 <85%.
Statistical analysis
SPSS 25.0 (IBM, USA) was used for statistical analysis. Continuous variables were presented as mean ± SD (normal distribution) or median (interquartile range) (non-normal distribution), and categorical variables as frequency (percentage). For group comparisons, normally distributed data were analyzed using one-way analysis of variance with Least Significant Difference post-hoc tests; non-normally distributed data using Kruskal–Wallis H tests with Dunn–Bonferroni post-hoc tests; categorical variables using χ2 tests or Fisher’s exact tests. Adjusted odds ratios (OR) and 95% confidence intervals (CI) for various health outcomes were calculated using logistic regression analysis. Gender-stratified analysis was performed due to different diagnostic criteria for HAPC between males and females. Statistical significance was set at two-sided p < 0.05. For multiple comparisons, Bonferroni correction was applied, with adjusted p-value threshold of p < 0.017 (0.05/3, pairwise comparisons among three groups).
Results
Basic characteristics of the study population
This study included 2,819 indigenous Xizang adults living at high altitudes (≥4,500 m), comprising 1,302 males (44.6%) and 1,517 females (55.4%). Based on Hb levels, Among male participants (n = 1,302), 366 (28.1% of males) were in the normal group (Hb: 130–175 g/l), 744 (57.1% of males) in the intermediate group (Hb: 175–210 g/l), and 192 (14.8% of males) in the HAPC group (Hb: ≥210 g/l). Among female participants (n = 1,517), 1,126 (74.2% of females) were in the normal group (Hb: 115–150 g/l), 363 (23.9% of females) in the intermediate group (Hb: 150–190 g/l), and 28 (1.8% of females) in the HAPC group (Hb: ≥190 g/l). Age distribution showed no statistically significant difference between groups (p > 0.05), with males averaging 41 years (32–51 years) and females averaging 40 years (32–50 years).
Weight indicators and blood pressure changes
Physical indicators showed an increasing trend with rising Hb levels (Table 1, all p < 0.001). In males, BMI increased significantly across groups (normal vs. intermediate vs. HAPC: 22.1 vs. 23.9 vs. 25.8 kg/m2, p < 0.001); females showed a similar trend (21.6 vs. 23.3 vs. 26.0 kg/m2, p < 0.001). Waist circumference and WHR increased significantly in the intermediate group (male waist: 83.0 vs. 77.5 cm, p < 0.001; female waist: 75.5 vs. 72.0 cm, p < 0.001).
Demographic and Clinical Characteristics of Study Participants Stratified by Sex and Hemoglobin Level Groups
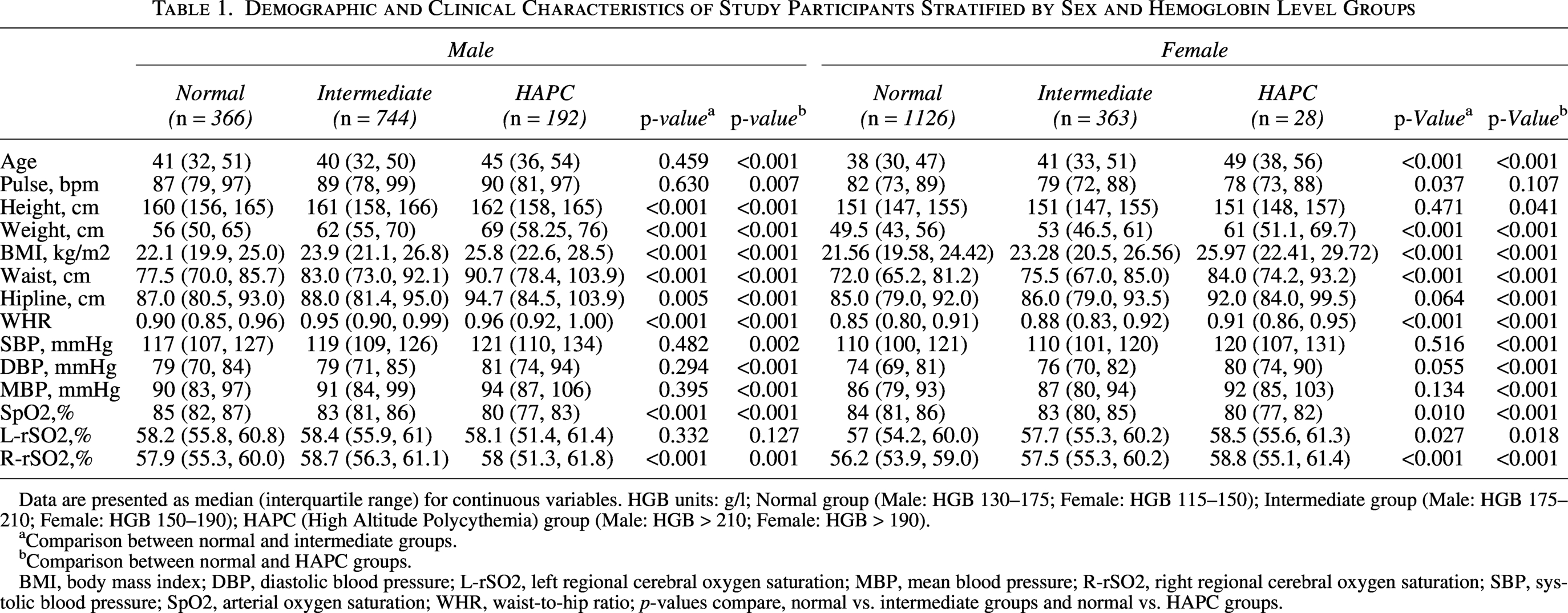
Data are presented as median (interquartile range) for continuous variables. HGB units: g/l; Normal group (Male: HGB 130–175; Female: HGB 115–150); Intermediate group (Male: HGB 175–210; Female: HGB 150–190); HAPC (High Altitude Polycythemia) group (Male: HGB > 210; Female: HGB > 190).
aComparison between normal and intermediate groups.
bComparison between normal and HAPC groups.
BMI, body mass index; DBP, diastolic blood pressure; L-rSO2, left regional cerebral oxygen saturation; MBP, mean blood pressure; R-rSO2, right regional cerebral oxygen saturation; SBP, systolic blood pressure; SpO2, arterial oxygen saturation; WHR, waist-to-hip ratio; p-values compare, normal vs. intermediate groups and normal vs. HAPC groups.
Regarding blood pressure, females in the intermediate group showed a trend toward increased DBP (76 vs. 74 mmHg, p = 0.055), with significant elevation in the HAPC group (80 mmHg, p < 0.001). Male SBP was significantly higher in the HAPC group compared with the normal group (121 vs. 117 mmHg, p = 0.002), but the intermediate group showed no significant change (119 mmHg, p = 0.482). Multivariate logistic regression analysis showed that, after adjusting for age, BMI, and other factors, HTN risk was significantly higher in the HAPC group (OR = 2.566, p < 0.001), but not significantly increased in the intermediate group (OR = 1.018, p = 0.905).
Blood oxygen saturation and cerebral oxygen saturation
SpO2 gradually decreased with increasing Hb levels (Table 1, all p < 0.001). Male SpO2 decreased from 85% in the normal group to 83% in the intermediate group (p = 0.001) and further to 80% in the HAPC group (p < 0.001); females showed similar trends (84% vs. 83% vs. 80%, p < 0.001). Cerebral oxygen saturation (rSO2) showed no significant decrease in males in the intermediate group, but L-rSO2 was significantly reduced in the HAPC group (p = 0.018), while females showed a significant reduction even in the intermediate group (p = 0.027).
Biochemical indicator changes
As shown in Table 2, the intermediate group already displayed significant abnormalities in multiple biochemical indicators (p < 0.01).
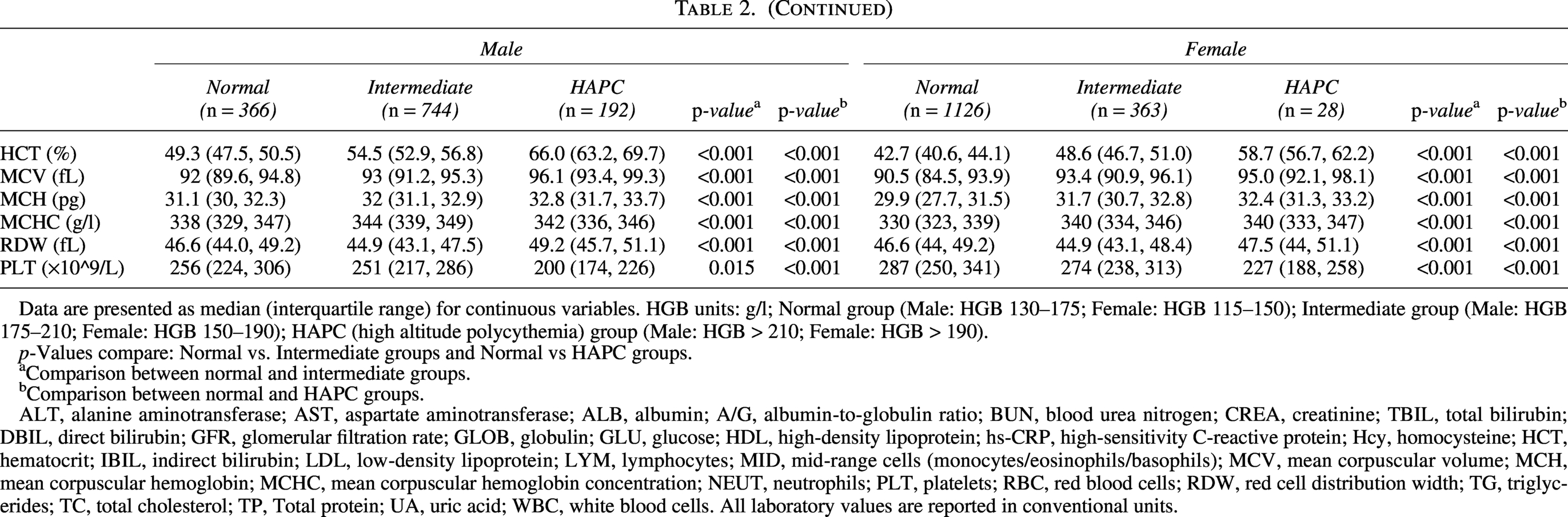
Biochemical and Hematological Parameters Stratified by Sex and Hemoglobin Level Groups
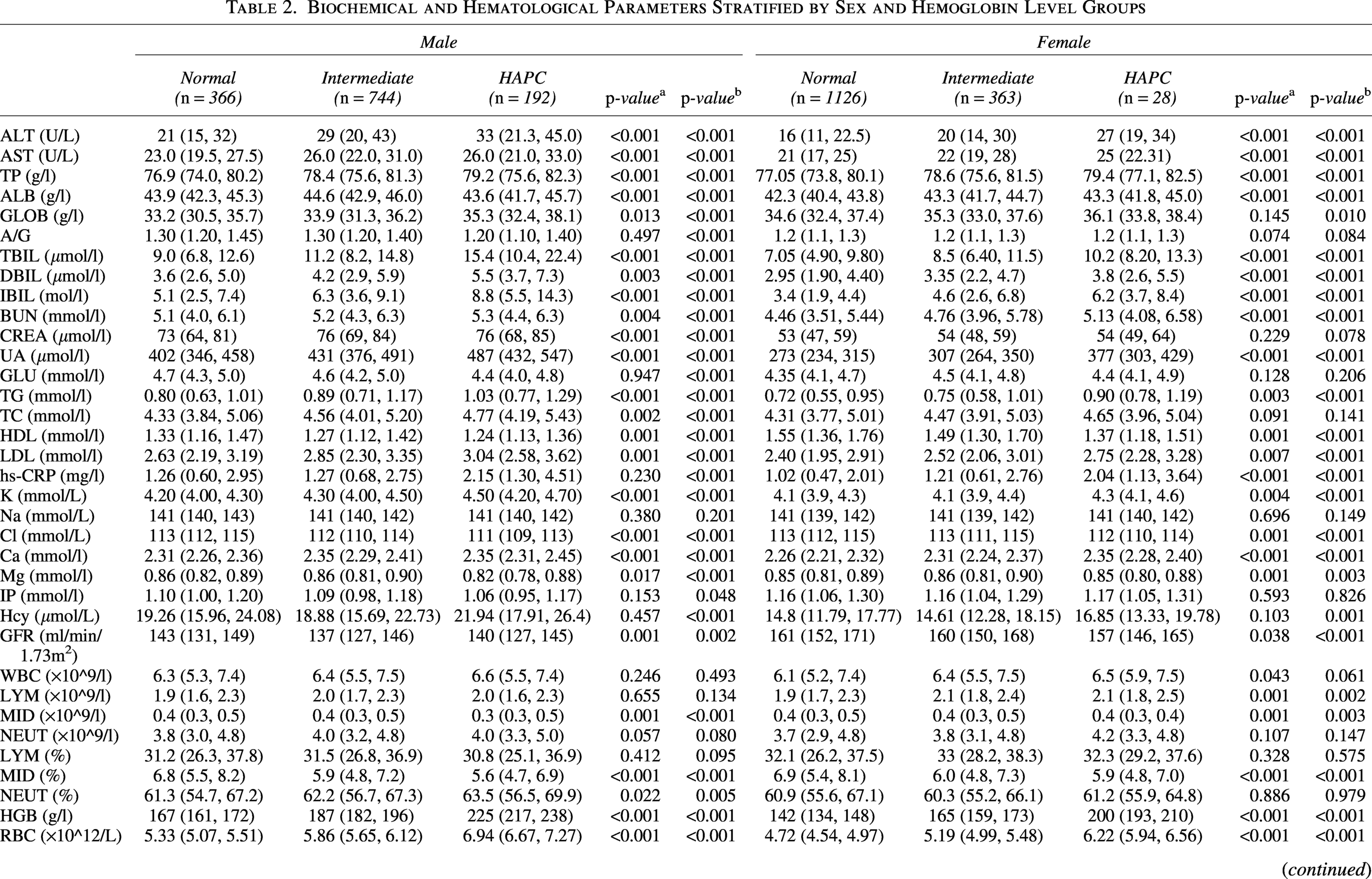
Data are presented as median (interquartile range) for continuous variables. HGB units: g/l; Normal group (Male: HGB 130–175; Female: HGB 115–150); Intermediate group (Male: HGB 175–210; Female: HGB 150–190); HAPC (high altitude polycythemia) group (Male: HGB > 210; Female: HGB > 190).
p-Values compare: Normal vs. Intermediate groups and Normal vs HAPC groups.
Comparison between normal and intermediate groups.
Comparison between normal and HAPC groups.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; ALB, albumin; A/G, albumin-to-globulin ratio; BUN, blood urea nitrogen; CREA, creatinine; TBIL, total bilirubin; DBIL, direct bilirubin; GFR, glomerular filtration rate; GLOB, globulin; GLU, glucose; HDL, high-density lipoprotein; hs-CRP, high-sensitivity C-reactive protein; Hcy, homocysteine; HCT, hematocrit; IBIL, indirect bilirubin; LDL, low-density lipoprotein; LYM, lymphocytes; MID, mid-range cells (monocytes/eosinophils/basophils); MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; NEUT, neutrophils; PLT, platelets; RBC, red blood cells; RDW, red cell distribution width; TG, triglycerides; TC, total cholesterol; TP, Total protein; UA, uric acid; WBC, white blood cells. All laboratory values are reported in conventional units.
continued
Liver function
Male ALT levels were significantly elevated in the intermediate group (29 vs. 21 U/L, p < 0.001), with further increases to 33 U/l in the HAPC group (p < 0.001); females showed similar trends (20 vs. 16 U/l, p < 0.001). The HAPC group had significantly increased risk of liver dysfunction (OR = 3.110, p < 0.001).
Lipid metabolism
Male LDL-C levels were significantly elevated in the intermediate group (2.85 vs. 2.63 mmol/l, p = 0.001), with further increases in the HAPC group (3.04 mmol/l, p < 0.001); females showed similar trends (2.52 vs. 2.40 mmol/l, p = 0.007). The intermediate group had a significantly increased risk of dyslipidemia (OR = 1.397, p = 0.028), with further elevation in the HAPC group (OR = 1.710, p = 0.006).
UA levels
Male UA levels were significantly higher in the intermediate group compared with the normal group (431 vs. 402 μmol/l, p < 0.001), with further increases in the HAPC group (487 μmol/l, p < 0.001); females showed similar significant increases (307 vs. 273 μmol/l, p < 0.001). Logistic analysis showed significantly increased hyperuricemia risk in the intermediate group (OR = 2.077, p < 0.001), with further elevation in the HAPC group (OR = 6.978, p < 0.001).
Inflammation levels
Hs-CRP was significantly elevated in females in the intermediate group (1.21 vs. 1.02 mg/l, p < 0.001), with further increases in the HAPC group (2.04 mg/l, p < 0.001); males showed significant elevation only in the HAPC group (p < 0.001). The HAPC group had a significantly increased inflammatory state (OR = 2.372, p < 0.001).
Echocardiographic analysis
As shown in Table 3, the intermediate group already showed trends of right ventricular hypertrophy and pulmonary arterial pressure elevation, with more pronounced cardiac structural changes in the HAPC group.
Echocardiographic Parameters Stratified by Sex and Hemoglobin Level Groups
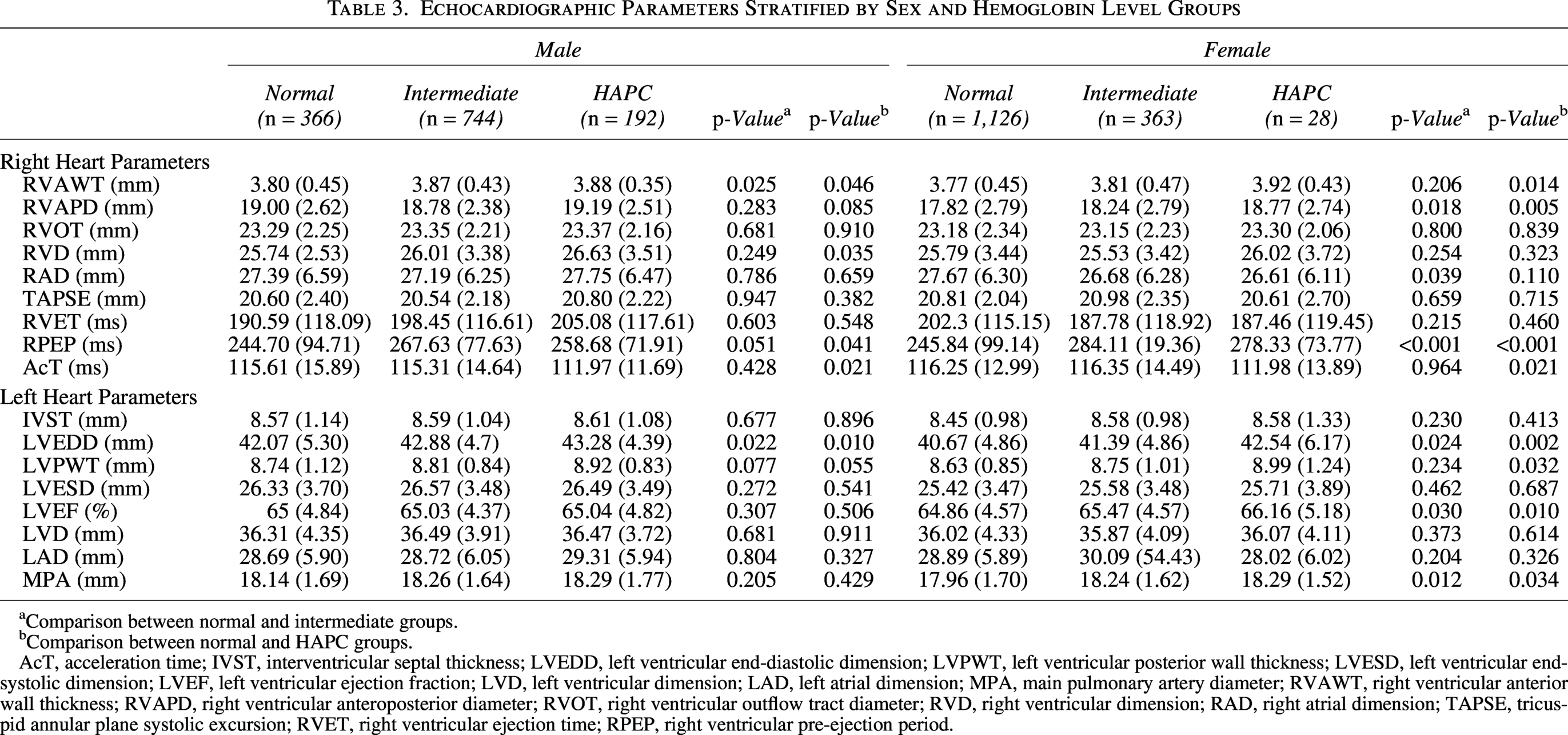
aComparison between normal and intermediate groups.
bComparison between normal and HAPC groups.
AcT, acceleration time; IVST, interventricular septal thickness; LVEDD, left ventricular end-diastolic dimension; LVPWT, left ventricular posterior wall thickness; LVESD, left ventricular end-systolic dimension; LVEF, left ventricular ejection fraction; LVD, left ventricular dimension; LAD, left atrial dimension; MPA, main pulmonary artery diameter; RVAWT, right ventricular anterior wall thickness; RVAPD, right ventricular anteroposterior diameter; RVOT, right ventricular outflow tract diameter; RVD, right ventricular dimension; RAD, right atrial dimension; TAPSE, tricuspid annular plane systolic excursion; RVET, right ventricular ejection time; RPEP, right ventricular pre-ejection period.
Right ventricular function: Male RVWT increased in the intermediate group compared to the normal group (3.87 vs. 3.80 mm, p = 0.025), with females showing more significant increases in the HAPC group (3.92 vs. 3.77 mm, p = 0.014). RVAPD increased significantly in males in the HAPC group (p = 0.035), while females showed significant increases even in the intermediate group (p = 0.018).
Pulmonary circulation pressure: Male pulmonary artery acceleration time (AcT) showed no significant change in the intermediate group but was significantly shortened in the HAPC group (111.97 vs. 115.31 ms, p = 0.021); females showed significant shortening in the HAPC group (111.98 vs. 116.35 ms, p = 0.021), suggesting elevated pulmonary arterial pressure.
Left ventricular function: Male LVEDd significantly increased in the intermediate group compared with the normal group (42.88 vs. 42.07 mm, p = 0.022), with females showing similar trends (41.39 vs. 40.67 mm, p = 0.024). Female LVEF showed an increasing trend in the intermediate group (p = 0.03), suggesting enhanced cardiac compensatory function (Fig. 1).
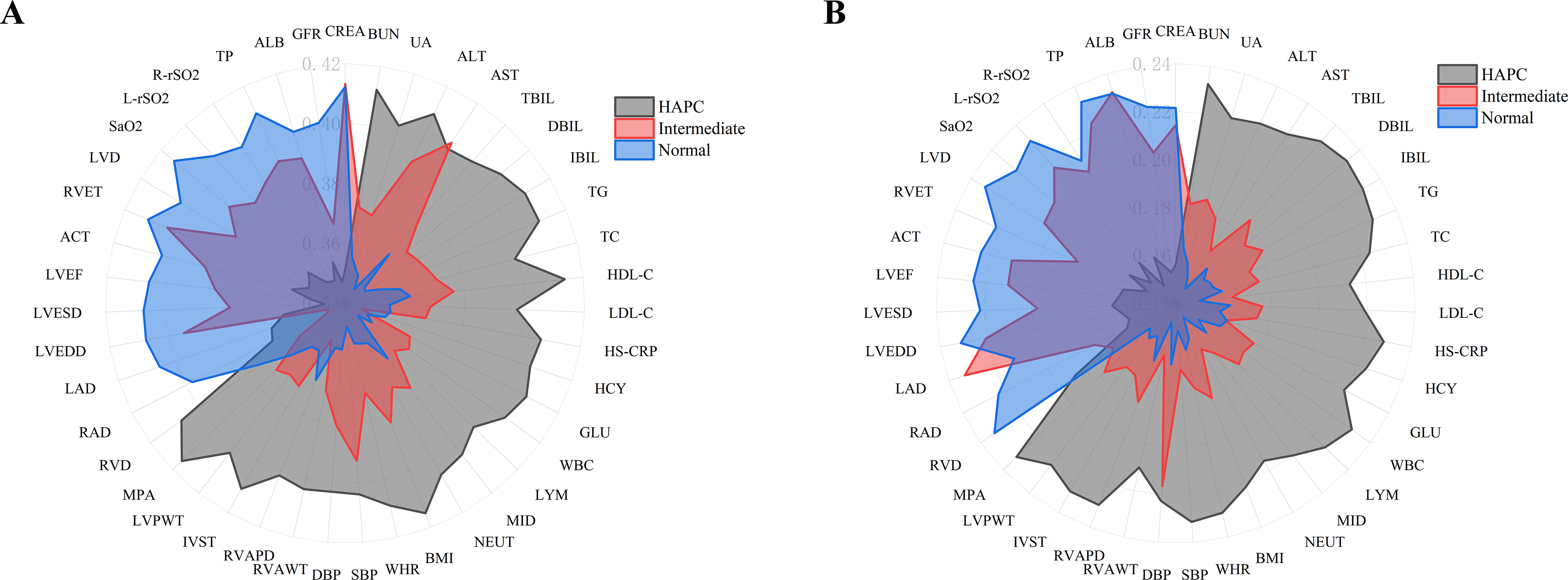
Radar chart illustrating the multidimensional clinical phenotype across hemoglobin-stratified groups in male
Association between hemoglobin levels and health risks
Logistic regression analysis assessing the impact of different hemoglobin levels on health outcomes showed (Fig. 2):

Adjusted ORs and 95% CIs for HAPC/pre-HAPC risk factors in male
Hypertension: Male intermediate group did not show significantly increased hypertension risk (OR = 1.018, 95% CI: 0.761–1.361, p = 0.905), but the HAPC group showed significant elevation (OR = 2.566, 95% CI: 1.842–3.574, p < 0.001); female HAPC group also showed significant increases (OR = 3.231, 95% CI: 2.145–4.867, p < 0.001).
Liver dysfunction (elevated ALT): The HAPC group showed significantly increased risk (OR = 3.110, 95% CI: 2.241–4.315, p < 0.001), with an increasing trend in the intermediate group that did not reach statistical significance (OR = 1.153, 95% CI: 0.913–1.455, p = 0.230).
Renal dysfunction (decreased eGFR): The HAPC group showed significantly increased risk (OR = 4.861, 95% CI: 3.282–7.198, p < 0.001), but the intermediate group showed no significant changes (OR = 1.175, 95% CI: 0.898–1.537, p = 0.239).
Dyslipidemia (elevated LDL-C): The intermediate group already showed significantly increased risk (OR = 1.397, 95% CI: 1.037–1.882, p = 0.028), with further increases in the HAPC group (OR = 1.710, 95% CI: 1.166–2.507, p = 0.006).
Hyperuricemia: The intermediate group already showed significantly increased risk (OR = 2.077, 95% CI: 1.602–2.693, p < 0.001), with further elevation in the HAPC group (OR = 6.978, 95% CI: 5.013–9.716, p < 0.001), representing the most significantly increased risk indicator among all health outcomes.
Chronic inflammation (elevated Hs-CRP): The HAPC group showed significantly increased risk (OR = 2.372, 95% CI: 1.714–3.282, p < 0.001), but the intermediate group showed no significant changes (OR = 1.063, 95% CI: 0.865–1.307, p = 0.557).
Gender differences: This study found that females in the intermediate group already showed more significant metabolic abnormalities, decreased blood oxygen, and increased right heart load. Compared with males, females in the intermediate group early on showed: significant elevation in DBP (p = 0.055 vs. male p = 0.294); significant decrease in cerebral oxygen saturation (p = 0.027 vs. male p = 0.332); significant elevation in hs-CRP levels (p < 0.001 vs. male p = 0.230); and increased RVAPD (p = 0.018 vs. male p = 0.283). These results suggest that females may be more sensitive to hypoxic environments in the pre-HAPC state (Fig. 2).
Discussion
Based on a large-sample stratified cluster sampling study in Xizang at altitudes ≥4,500 m, this study systematically reveals, for the first time, the pathophysiological characteristics of the pre-HAPC state (i.e., individuals with Hb levels between normal upper limits and HAPC diagnostic thresholds in the “intermediate zone”). Results show that even before Hb levels reach HAPC diagnostic criteria, intermediate group individuals already demonstrate metabolic abnormalities, worsening hypoxia, and trends of multiorgan functional changes, suggesting this state may be a precursor stage of HAPC. This finding breaks through the traditional binary diagnostic model of HAPC and supports establishing a hemoglobin gradient-based “risk stratification-early intervention” strategy.
Clinical significance of the Pre-HAPC state
Current clinical diagnostic criteria for HAPC use Hb concentration as the sole criterion (≥210 g/l for males, ≥190 g/l for females) (León-Velarde et al., 2005). While effective for identifying typical cases, these criteria overlook the significant population with intermediate Hb levels. Our study found that intermediate group individuals already demonstrate significant health risks, including metabolic abnormalities (increased BMI and waist circumference, dyslipidemia, hyperuricemia), decreased blood oxygen (reduced SpO2), improved cardiovascular load (right ventricular hypertrophy, elevated pulmonary arterial pressure), and liver and kidney dysfunction. These changes suggest that the intermediate group is not in a completely healthy state but may be in an early stage of HAPC.
The HAPC diagnostic criteria proposed by León-Velarde et al. (2005) have become an international consensus, but Villafuerte et al. (2022) noted that this single-threshold Hb-based diagnostic criterion may not reflect the continuous nature of the disease. Previous research has considered high-altitude adaptation a continuous physiological process, with Hb elevation representing a compensatory adjustment to hypoxic environments (Simonson et al., 2015). However, our study reveals that before HAPC diagnosis, Hb elevation already affects multiple organ systems, supporting HAPC as a gradually developing pathological process rather than a single-threshold mutation disease. The diagnostic model of HAPC establishes a paradigm shift in clinical assessment, transitioning from the conventional “binary classification” system (normal vs. HAPC) to a “gradient risk stratification” framework. This innovative approach enables dynamic risk quantification and offers a theoretical foundation for implementing timely identification of subclinical abnormalities and tailored preventive strategies in presymptomatic populations.
Relationship between Pre-HAPC state and metabolic disorders
Our study found that intermediate group individuals show significantly increased BMI, waist circumference, and WHR, with significantly increased risks of dyslipidemia (elevated LDL-C, OR = 1.89) and hyperuricemia (males OR = 3.02, females OR = 2.08), suggesting the pre-HAPC state may be closely related to metabolic syndrome. Previous studies have indicated that high-altitude hypoxic environments can influence lipid metabolism, insulin sensitivity, and UA metabolism through HIF pathways, thereby increasing metabolic disease risk (Hao et al., 2015; Hopkins et al., 1996).
Elevated uric acid levels may be one of the earliest metabolic abnormalities in the pre-HAPC state. Our study found significantly elevated UA levels in intermediate group males (431 vs. 402 μmol/l, p < 0.001) and females (307 vs. 273 μmol/l, p < 0.001), suggesting that hypoxia may lead to hyperuricemia by promoting purine metabolism and reducing UA excretion. This is consistent with findings by Jefferson et al.(Jefferson et al., 2002), who found that HAPC positively correlates with hyperuricemia, proteinuria, and HTN. Hyperuricemia is associated not only with gout but also with endothelial dysfunction, chronic inflammation, and oxidative stress, further increasing cardiovascular disease risk (Borghi et al., 2020).
Additionally, our study found that metabolic disorders are more pronounced in the HAPC stage, but glucose levels don’t change significantly in the intermediate group, suggesting that high-altitude hypoxia-induced metabolic disorders may initially manifest as lipid and UA metabolism abnormalities. Savla et al. (2018) found that hypoxia through HIF-1α activation can affect lipid metabolism enzyme expression, leading to lipid abnormalities. Therefore, intermediate group individuals should receive routine monitoring of lipid and UA levels and reduce subsequent HAPC and related chronic disease risk through lifestyle interventions (e.g., appropriate exercise, dietary regulation).
Pre-HAPC state and oxygen supply-demand imbalance
Traditional views hold that Hb elevation is a compensatory adjustment to high-altitude hypoxic environments, helping improve oxygen transport capacity. However, we found that blood oxygen saturation (SpO2) is already significantly decreased in the intermediate group (males: 83% vs. 85%, females: 83% vs. 84%), suggesting that hemoglobin elevation has not effectively improved oxygen supply-demand balance but may actually affect microcirculatory oxygen transport due to increased blood viscosity. Simonson et al. (2010) found that different ethnic groups have different adaptation strategies to high-altitude environments, with Tibetan possibly adapting through increased hemoglobin oxygen affinity rather than simply increasing hemoglobin concentration. Tang et al. (2024) noted that increased blood viscosity in HAPC patients can lead to microcirculatory disorders, reducing tissue oxygen utilization efficiency. Our study found that pulmonary arterial pressure begins to increase (shortened AcT) in intermediate group individuals, suggesting that increased cardiopulmonary load may worsen hypoxic states. Therefore, even when hemoglobin levels don’t reach HAPC diagnostic criteria, the body has already entered a state of compensatory imbalance, increasing subsequent cardiovascular event risk. This finding emphasizes the importance of early blood oxygen level monitoring, with interventions to improve microcirculation (e.g., increased high-altitude adaptation training, appropriate antioxidant use) when necessary.
Pre-HAPC state and cardiovascular functional changes
Our echocardiographic analysis revealed that individuals in the intermediate group exhibited increased RVWT and shortened pulmonary artery AcT, indicating early signs of elevated right ventricular load. This aligns with findings by Titz et al. (2024), who reported that chronic hypoxia at high altitudes induces pulmonary vasoconstriction, increases blood viscosity, and leads to right ventricular remodeling, ultimately contributing to pulmonary HTN and right heart failure.
Further, Sun et al. (2024) demonstrated through advanced imaging that right ventricular adaptations in high-altitude residents correlate with Hb levels, with structural changes occurring even at mild Hb elevations. Similarly, Wang et al. (1998) found that chronic hypoxia promotes pulmonary vascular remodeling, thereby increasing right heart workload and predisposing individuals to right ventricular hypertrophy.
Our study also established a significant association between the pre-HAPC state and HTN risk. Although blood pressure changes in the intermediate group were not statistically significant, a marked increase in hypertension prevalence was observed in the HAPC group (OR = 2.566, p < 0.001). Liu et al. (2024) previously reported that for every 10 g/l rise in Hb levels, the risk of HTN increases by ∼8%. This suggests that elevated Hb contributes to progressive vascular resistance, eventually triggering HTN.
Given these findings, individuals in the intermediate group should undergo regular cardiovascular assessments to monitor early functional changes. Potential interventions to mitigate cardiovascular risk include strategies to reduce blood viscosity and improve vascular function, such as controlled oxygen therapy, exercise regimens tailored for high-altitude adaptation, and pharmacological approaches targeting pulmonary HTN.
Study limitations
Several limitations of this study merit consideration. First, the cross-sectional design precludes causal inference; the directionality of associations between the identified biomarkers and HAPC progression cannot be established from the present data. Second, although all participants were indigenous Tibetan residents of three or more generations living in pastoral communities at altitudes ≥4,500 m—which minimizes genetic heterogeneity related to high-altitude adaptation—potential confounding from lifestyle factors cannot be fully excluded. Future studies should incorporate detailed dietary assessments, physical activity monitoring, and targeted genetic analyses to disentangle these effects. Third, PSG-based screening for obstructive sleep apnea was not performed. Furthermore, screening for obstructive sleep apnea syndrome (OSAS) was not included in the study design. Given the observed association between elevated Hb and increased BMI, and the clinical overlap between OSAS phenotypes and HAPC, future studies incorporating polysomnography are warranted to clarify the contribution of OSAS to HAPC development. Future prospective cohort studies with serial Hb measurements and clinical follow-up are needed to validate the predictive utility of the pre-HAPC phenotype proposed here and to evaluate the long-term outcomes of early intervention in the intermediate group.
Conclusion
This study introduces the concept of the “pre-HAPC state” and demonstrates its association with metabolic dysregulation, increased cardiovascular load, and oxygen supply-demand imbalance. These findings underscore the need for early screening and individualized interventions, including monitoring Hb, lipids, UA, and oxygen saturation; optimizing metabolic function through lifestyle modifications; and mitigating vascular resistance in high-risk individuals. Future research should further explore the molecular mechanisms underlying this state and its long-term health implications, enabling more precise preventive strategies for high-altitude populations.
Consent for Publication
All authors have reviewed the final article and approved its submission for publication. Participants consented to the use of their anonymized data for research purposes.
Availability of Data and Material
Data used in this study are available upon reasonable request. To access the data, please get in touch with the corresponding author at
Authors’ Contributions
G.S.L.B. designed research and revised manuscripts; D.Z.Z.G. designed the questionnaire survey, drafted and revised manuscripts; W.Y.S. and B.M.Y.J. conducted UCG; C.B., H.J., and Z.R., Z.X.Q.Z. performed experiments; C.R.Z.M. and L.M.Z.G. performed epidemiological investigations. S.N.Y.Z. analyzed data; L.B.Y. interpreted results of experiments;
Footnotes
Acknowledgments
The authors would like to express their gratitude to the Nagqu Health Commission and the 51 township health centers in Nyima County, Amdo County, and Shuanghu County for their invaluable support and cooperation in the development of this study.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This study was supported by the Science and Technology Projects of Xizang Autonomous Region, China (Grant No.