
Abstract
The classic procedure for aortobifemoral bypass is open surgery. Laparoscopy has been accepted by several authors as a minimal invasive alternative for aortoiliac occlusive disease. The totally retroperitoneal laparoscopic procedure has been described as an alternative to the transperitoneal approach. Whatever the approach, the aortoprosthetic anastomosis is a major difficulty making those techniques unpopular despite obvious advantages for the patients. We report a clampless and sutureless approach for the proximal anastomosis of a totally retroperitoneal laparoscopic aortobifemoral bypass using an EndoVascular REtroperitoneoScopic Technique (EVREST). This approach was proposed to a 56-year-old man with severe aortoiliac occlusive disease. There was no indication for endovascular re-vascularization. The patient was placed in a 30° right lateral decubitus position. The dissection of the retroperitoneal space was performed and the infrarenal aorta was exposed. A bifurcated graft was inserted into the retroperitoneal space. Under videoscopic control the prosthetic limbs were brought to the groins. The main body of the graft was connected on the left side of the aorta by an intra and extra aortic covered stent-graft. This connection was performed without the use of an aortic clamp and without suture. The femoral anastomoses were performed by classic open surgery.
Keywords
Introduction
The classic procedure for aortobifemoral bypass is open surgery. Since the first totally laparoscopic aortobifemoral bypass reported in 1997 by Yves-Marie Dion, 1 laparoscopy has been accepted by several authors as a minimal invasive alternative for aortoiliac occlusive disease.2,3 The totally retroperitoneal laparoscopic procedure has been described as an alternative to the transperitoneal approach.4,5 We report a clampless and sutureless approach for the proximal anastomosis of a totally retroperitoneal laparoscopic aortobifemoral bypass using an EndoVascular REtroperitoneoScopic Technique (EVREST). This approach using existing materials could make the laparoscopic aortic surgery for occlusive disease accessible to all vascular surgeons. To the best of our knowledge, this procedure has not been used or described before.
Case report
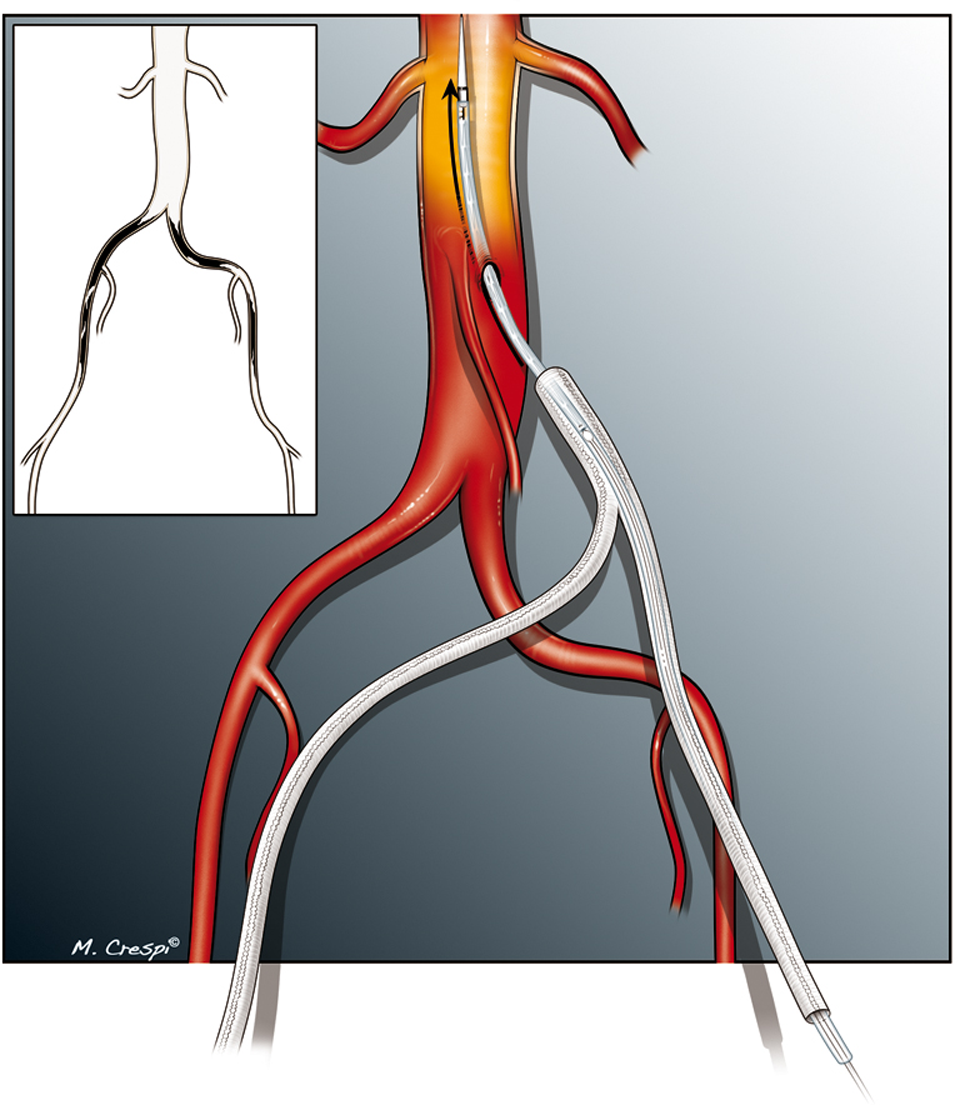
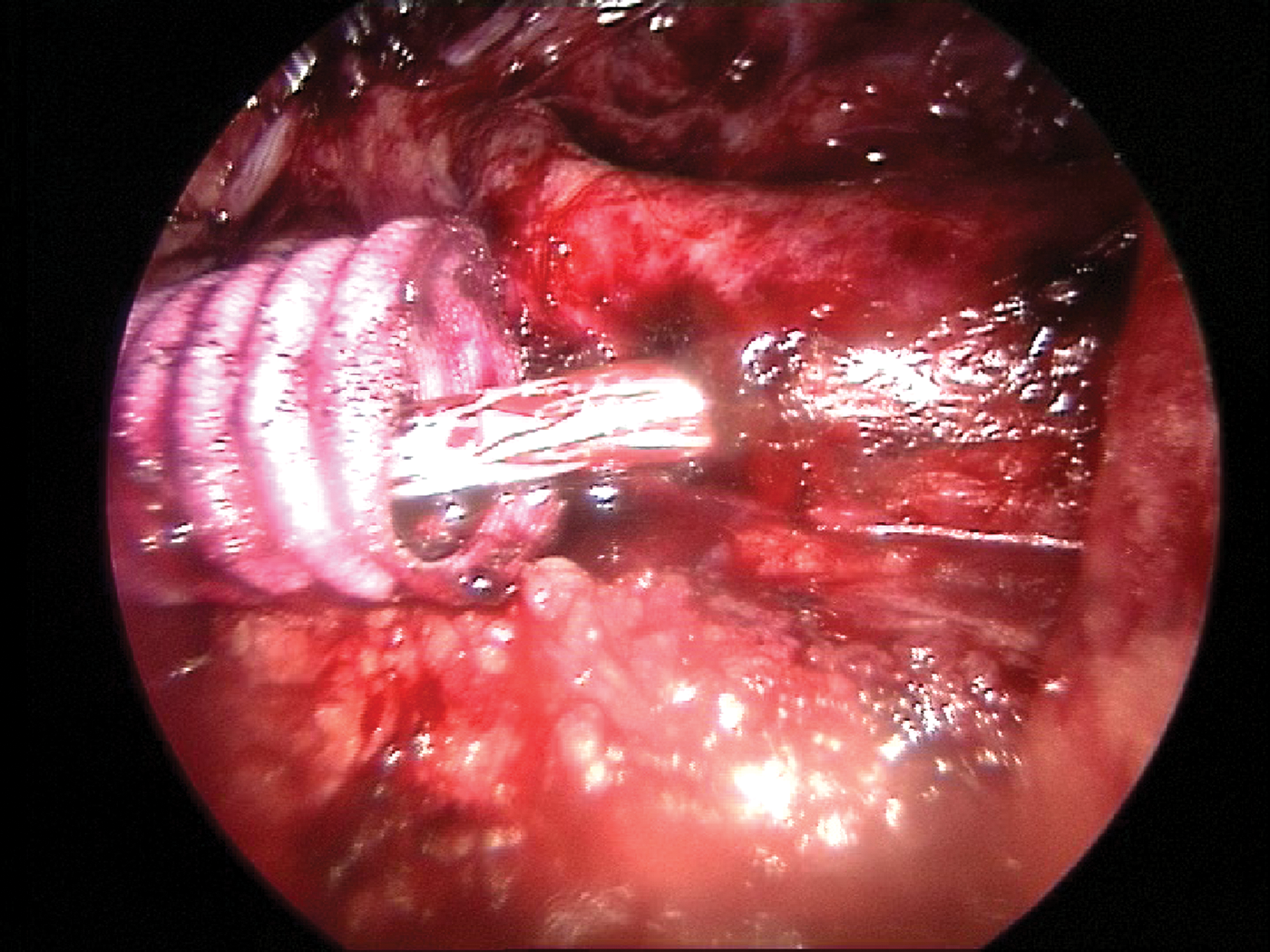
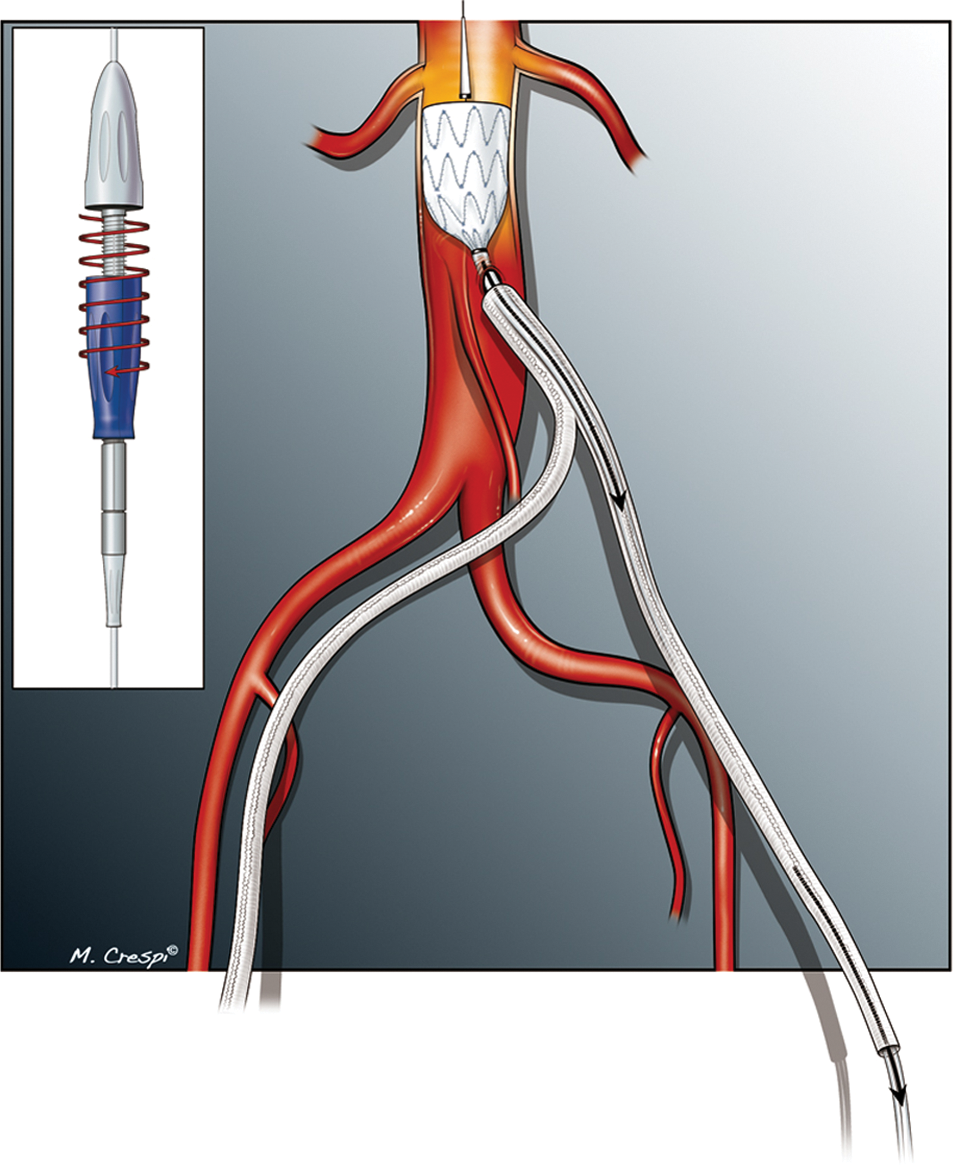
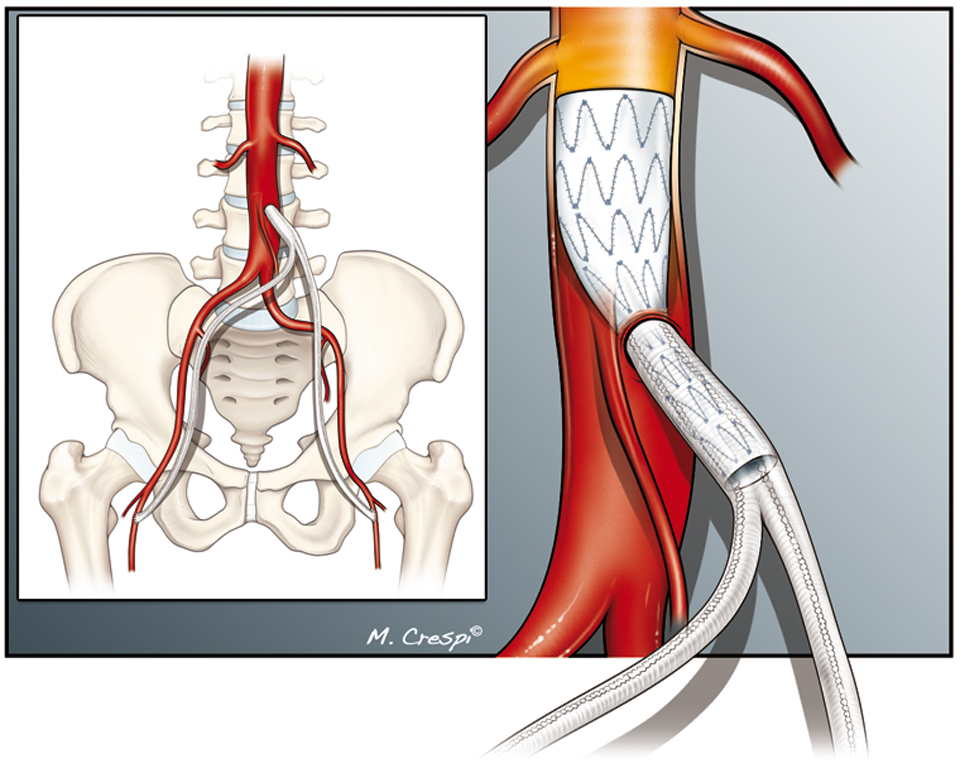
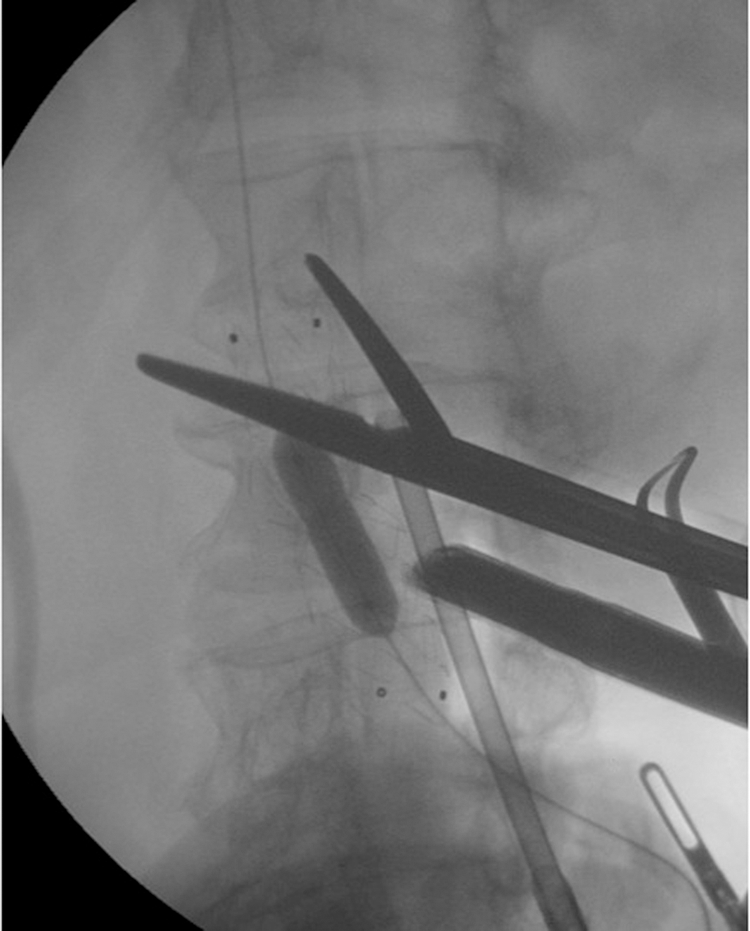
We report the case of a 56-year-old man with aortoiliac occlusive disease and no indication for endovascular re-vascularization. The predominant symptom was a 50 m bilateral intermittent claudication. Relevant clinical history included smoking and bilateral peripheral arterial disease. The patient had been treated before by endovascular stenting of the common iliac which led to intimal hyperplasia and thrombosis of the stents. The cardiovascular risk factors were smoking, arterial hypertension, hyperlipemia and type II diabetes. Daily treatment included Clopidogrel 75 mg, Metformine, statines and Angiotensin-converting enzyme inhibitor. Clinical examination revealed no femoral pulses and lower limbs coldness. The computed tomography-angiography showed bilateral common and external iliac occlusions, a patent inferior mesenteric artery and moderate calcifications of the infrarenal abdominal aorta (Figure 1). Cardiac and carotid investigations (Doppler, cardio-echography) were normal. There was no indication for endovascular revascularization, so we decided to perform an endovascular retroperitoneoscopic aortobifemoral bypass. The patient was positioned, under general anesthesia, in a 30° right lateral decubitus. The operator, first assistant and scrub nurse were on the left side of the patient. The monitor was positioned on the right side. A pneumo-peritoneum was created by a Verres needle introduced on the umbilicus. A 30° optical system was first inserted in intra-abdominal position to check good positioning of three trocars in the left retroperitoneal space. After exsufflation of the pneumo-peritoneum, dissection of the retroperitoneal space was performed by CO2 insufflation at a maximum pressure of 14 mmHg and by blunt dissection with a laparoscopic forceps. The left common iliac artery was easily visualized above the psoas muscle and dissected with monopolar electrocoagulation. The left ureter was then visualized and the aorta was isolated up to the left renal artery. One additional 12-mm trocar was placed between the 11th rib and the umbilicus, to support a laparoscopic aortic clamp (AesculapR AG & Co KG Company, Tuttlingen, Germany). A bifurcated prosthesis (Gelsoft™ Plus Bifurcate, Vascutek Terumo, Scotland) was inserted into the retroperitoneal space through the 12-mm trocar. Under videoscopic control the prosthetic limbs were brought to the groins which had been previously surgically dissected. A 18G, 27 cm catheter needle (Transhepatic cholangiography catheter needle, Cook Medical Inc, Bloomington, IN, USA) was inserted through the left prosthetic limb in the retroperitoneal space. The left lateral side of the infrarenal aorta was then punctured at the level of the origin of the inferior mesenteric artery. A 0.035″ hydrophilic guide wire (Terumo Corporation, Tokyo, Japan) was positioned into the aorta. 100 UL/kg of heparin were given intravenously. A pigtail catheter was positioned for an angiography to localize the renal arteries. The hydrophilic guide was changed for a stiff guide wire (Lunderquist, Cook Medical Inc). A 20 mm diameter and 80 mm length iliac extension of an Endurant stent-graft system (Medtronic, Endovascular, Santa Rosa, CA, USA) was introduced over the wire up to 4 cm into the aorta through the left prosthetic limb of the bifurcated graft (Figures 2 and 3). The covered stent-graft, used as a connector, was deployed into the infra-renal aorta and into the main body of the bifurcated graft (Figures 4 and 5). A 10 mm diameter non-compliant balloon (Passeo-35, Biotronik, Berlin, Germany) and a compliant balloon (Coda balloon catheter) were inflated to ensure sealing of the aorto-prosthetic junction and perfect deployment of the endograft (Figure 6). The deployment was controlled by fluoroscopy and by direct retroperitoneal vision on the monitor. The femoral anastomoses were performed by classic open surgery with 6/0 polypropylene running sutures. A drain was left in the retroperitoneal space for 24 hours. Operative time was four hours. The use of the aortic clamp was not necessary during the procedure. Blood loss was 50cm3. No transfusion was needed. Postoperative course was uneventful. Postoperative medication consisted in oral Aspirin (160 mg daily). The patient was released at day 4. Both postoperative CT-angiographies at one week and at three months showed patency of the covered stent and bifurcated graft without significant narrowing, and the absence of leak (Figure 7).
Preoperative computed tomography-angiography Endurant stent-graft system introduced into the aorta through the left prosthetic limb of the bifurcated graft Endurant stent-graft system introduced over the wire into the aorta through the bifurcated graft The covered stent-graft is deployed into the aorta The covered stent-graft is deployed into the aorta and into the main body of the bifurcated graft A non-compliant balloon (10 mm) is inflated to ensure sealing of the aorto-prosthetic junction. The aortic clamp is left open, ready to be used in case of bleeding Three months postoperative computed tomography-angiography

Discussion
Since 2004 we have performed several retroperitoneal aortobifemoral bypasses using a short left-sided transverse incision. This procedure, described by Charles Rob in 1963, 6 is not very popular because of the difficulties encountered to expose the aorta. Using a surgical retractor system (CondorR GmbH Medicaltechnik, Salzkotten Germany) the procedure remains challenging but feasible. With growing experience our incisions got smaller and it became logical to attempt a retroperitoneal laparoscopic approach. Some of our patients underwent successfully total laparoscopic retroperitoneal aortobifemoral bypass. 5
The most popular way for laparoscopic aortobifemoral bypass is the prerenal transperitoneal approach.1–3,7 Whatever the described techniques1–5,7 the aortoprosthetic anastomosis is a major problem making those techniques unpopular despite obvious advantages for the patients. 7 Vascular laparoscopic experts agree that the learning curve is long, that a mini-laparotomy is often needed to complete the aortic anastomosis and that new materials are needed to make the aortic suture more feasible.2,3,8 Some vascular surgeons have presented new devices to facilitate the aortic suture but those materials were generally used only in vitro, on pigs and cadavers or only by the authors themselves.8,9
Connecting blood vessels is done mostly the same way today with sutures as it was 100 years ago, when the French surgeon Alexis Carrel described the technique in 1902. 10 This standard anastomotic technique requires large exposure, circumferential dissection and clamping of vessels. Moreover, the classical surgical access can be quite difficult and time consuming especially with patients who have heavily calcified vessels. 11 These aspects are all the more true for aortic laparoscopic surgery.
In 2007, Lachat 12 published the VORTEC technique (Viabahn Open Revascularisazion TEChnique) which is a clampless and sutureless method that appears to be faster, safer and easier than the classic arterial sutures for complex anastomoses in open surgery. It is a prosthetic graft anastomotic technique that uses self-expanding stent grafts that are ‘telescoped’ into aortic branches. This technique requires only minimal vessel exposure, obviates the need for vessel cross-clamping or anastomotic suturing and significantly reduces the duration of blood flow interruption. Lachat described its experience over more than 300 cases. 13 He encountered no major bleeding or leaks. This technique represents a significant improvement over the traditional vascular anastomotic surgical techniques.
We decided to apply this technique for the totally retroperitoneal laparoscopic aortobifemoral bypass. EVREST greatly facilitates the laparoscopic aortic surgery in occlusive disease with no need of suture or clamping of the aorta. This technique offers the advantages of laparoscopy and those of endovascular surgery, especially in challenging conditions encountered during aortic laparoscopic surgery.
For patients who are candidates for an aortobifemoral bypass we now propose EVREST as an alternative to an open procedure. More patients are required to assess the value of this promising technique. As for other new techniques, the aspects of reproducibility and long-term results will need to be evaluated.
Footnotes
Aknowledgements
The authors gratefully acknowledge the contribution of Massimiliano Crespi for his splendid drawings. This work would not have been accomplished without the support of our marvellous scrubb nurse, Nathalie Denaeijer.