
Abstract
Objectives
The main purpose of this study was to document the radiation doses to patients during carotid stenting.
Material and method
Fluoroscopy and exposure time, air kerma and dose-area product during carotid artery stenting in 160 patients were retrospectively reviewed with regard to body mass index, degree of stenosis and use of cerebral protection devices.
Results
Total air kerma was lower than 0.5 Gy in 80%, 0.5–1 Gy in 17% and higher than 1 Gy (maximum 1.2) in 3% of patients. Mean total dose-area product value for carotid stenting was 54 Gy cm2. The mean air kerma (fluoroscopy), air kerma (exposure), total air kerma and dose-area product (fluoroscopy), dose-area product (exposure), total dose-area product of patients with body mass index within the range 25–29.9 and with body mass index >30 were significantly increased compared to that of patients with body mass index 18–24.9 (H = 40.2, df = 2; p = 0.0000001 and p = 0.000003, respectively).
Conclusion
Carotid artery stenting is a relatively safe radiological procedure in terms of the radiation dose acquired by the patient. The main factors contributing to possible radiation overdosing are body mass index value and complexity of the carotid lesion. Proper preoperative planning in obese and complicated patients may reduce the fluoroscopy time and contribute to reduced dose acquisition.
Introduction
Previous studies contributing the radiological safety allowed to determine the role of factors contributing to high-patient dose including extended exposure and fluoroscopy time, dose-area product (DAP), kinetic energy released in matter, the large numbers of runs and maximized image contrast.1,2 DAP is an index of the X-ray energy delivered to a patient during a procedure. DAP is independent of the distance between X-ray generator and exposed area; normally, the intensity of radiation decreases with the square of the distance. Exposed area is simultaneously growing with the distance, and DAP allows 0° to calculate the dose of X-ray and the radiation risk. To obtain the radiation dose in gray, DAP should be divided by radiated field. Air kerma (energy released in a unit mass of air) provides an index of radiation reaching the skin and the risk of skin injury.1,2 Air kerma is expressed in the unit of gray Gy, used for the absorbed dose. Air kerma is measured (or calculated) at a point where soft tissue is located, and the absorbed dose in the tissue will be just about equal to the air kerma. When X-ray is used, the gray unit is similar to Sievert, because the factor of relative biological effectiveness in this case is 1. The International Commission on Radiological Protection (ICRP) standardized these factors in 1991, described in report 92. 3 Fluoroscopy uses X-ray to produce real-time video images. The radiation dose may be estimated based on the fluoroscopy time measured with dosimeters and transmission ion chambers and expressed in terms of the DAP and air kerma.4–16
During carotid stenting (CAS), the use of X-rays inducts the deterministic (DE) and stochastic (SE) effects of radiation.2,3 Radiation exposure is known to cause cancer (SE) and also leads to acute skin injury (DE).2,3,17 Patients undergoing carotid stenting are sometimes at a young age, which means that the risk of inducing cancer increases (usually 10–20 years after exposure). 2 Skin injury is apparent when the dose exceeds about 1 Gy. 1 Carotid artery surgery, both open or endovascular, has been a topic of constant discussion over the past 20 years. Since the results of ACAS, NASCET and ESCT studies were published, open surgery became a standard-proven procedure in the management of carotid artery stenosis. 18 However, the discussion over the indication to any intervention is still the ‘hot topic’. The last 10 years have shown an increasing interest towards endovascular treatment of carotid artery stenosis. Despite the unfavorable results of EVA-3S and ICSS trials, the recent publication of the results from CREST trial may suggest that CAS is equivalent to CEA, if minor MI would be included as one of the comparative endpoints, that allowed approval of the carotid artery stenting in the United States by FDA.19–25 CAS, despite a higher risk of a major stroke, is generally preferred by patients and medical practitioners not skilled in CEA. Currently, indications for CAS in Europe are based on ESVS guidelines from 2009. 26 However, these guidelines hardly respect the data from ICSS and CREST trials. The qualification for CAS and CEA is still based on the degree of the stenosis. Generally, asymptomatic stenosis greater than 60% (70%) may be treated by CAS or CEA.
Aim of the study
The aim of the study was to evaluate the relationship between radiation time (fluoroscopy and exposure time) of DAP, air kerma, regarding body mass index (BMI), severity of stenosis and use of the cerebral protection systems to optimize radiation dose during CAS.
Material and methods
Risk factors and concomitant medical conditions.
All the procedures were performed by two certified interventional radiologists with initial experience of more than 100 CAS on a Philips Allura system using pulsating X-ray radiation. X-ray tube angulation was fixed. All patients gave informed consent for the procedures. The consent of the patient was not required for the purpose of the study by local regulatory board. Carotid angiography was performed by femoral access. The diagnostic catheter 5 F (Cook) was positioned in the arch of thoracic aorta followed by one or two series of digital subtraction angiography (DSA). Then, through the guiding catheter 6 F (Cook, Cordis), the left carotid catheter (Balton) was selectively positioned in the common carotid artery, and DSA examination was performed with angulation (90°, 60° and 30°) (2–5 series).
The procedure was carried out using non-ionic contrast agent. The contrast medium injection was performed with an automatic syringe (Medrad). Depending on the clinical indication, there were one to two series for the aortic arch and two to five selective series for the carotid arteries. The cerebral protection device was used in each case (Abbott). In most cases, one stent was implanted (Cordis, Boston, Abbott). The stents were 7–12 mm in diameter and their length ranged 20–60 mm.
In all cases, imaging was performed with a rotation angle; in addition, depending on the need, the following rotation angles were used: 30° (22% of the total number of runs), 60° (32% of the total number of runs) and 90° (81% of the total number of runs). In most cases, an 80/90 kV tube voltage (95% of total) was used.
The dose data were calculated from the exposure values and expressed as DAP (Gy cm2) and air kerma (AK) (Gy) together with the total fluoroscopy time (min) and exposure (ms) in the C-arm unit.
Statistics
Patient doses were analysed with the Kruskal–Wallis test (H-test) according to subgroups regarding BMI, and with the Mann–Whitney U test, regarding the degree of carotid stenosis, use of cerebral protection and any difficult anatomy. A p-value of ≤0.05 was considered significant. Correlation between radiation time (fluoroscopy and exposure) and radiation dose (DAP and AK) was calculated with nonparametric Spearman r coefficient.
Results
Analyzed factors in terms of DAP, air kerma, and radiation times.

In 80% of the analysed patients, total air kerma was lower than 0.5 Gy, and for 17%, it exceeded 0.5 Gy. For 3% of patients, this value was higher than 1 Gy, and the maximum obtained air kerma was 1.2 Gy. The results have shown that the mean total DAP value for CAS was 54 Gy cm2.
The mean AK (fluoroscopy) for patients with BMI within the range 25–29.9 and with BMI > 30 was significantly increased compared to that of patients with BMI 18–24.9 (H = 23.5, df = 2; p = 0.0000005, p = 0.000001 and p = 0.000003, respectively). For the mean AK (exposure), there were only significant differences between BMI 18–24.9 and BMI > 30 (H = 9.41, df = 2; p = 0.000006). Significant differences in the mean total AK were observed regarding BMI 18–24.9 compared to that of patients with BMI > 30 and regarding BMI 25–29.9 compared to that of patients with BMI > 30 (H = 22.2, df = 2; p = 0.000005 and p = 0.00000008, respectively). The same dependence was found in the case of total DAP, DAP (exposure) and DAP (fluoroscopy) (H = 19.8, df = 2; p = 0.000006 and p = 0.0000005, H = 11.2, df = 2; p = 0.00002 and p = 0.0001, H = 19.1, df = 2; p = 0.000006 and p = 0.0000005, respectively). A similar relationship was found for fluoroscopy time (H = 3.15, df = 2; p = 0.000006 and p = 0.00002, respectively).
Significant differences in the mean AK (fluoroscopy) and DAP (fluoroscopy) were observed in patients with stenosis within the range 70–79% compared to patients with 90–99% stenosis and stenosis ranged 80–89% compared to that of patients with stenosis 90–99% (H = 20.95, df = 2; p = 0.00000001 and p = 0.00000001, H = 14.91, df = 2; p = 0.0003 and p = 0.0000003, respectively). The same dependence was found in the case of the total AK (H = 15.52, df = 2; p = 0.0001 and p = 0.000002). In the mean total DAP, significant differences were observed in patients with stenosis within the range 70–79% compared to patients with 90–99% (H = 8.22, df = 2; p = 0.001). The mean FT of patients with stenosis within 80–89% and 90–99% was significantly increased compared to that of patients with 70–79% stenosis (H = 32.2, df = 2; p = 0.000000001, p = 0.0000001 and p = 0.000001, respectively). Significant differences in the total AK, total DAP, AK (fluoroscopy), DAP (fluoroscopy) and fluoroscopy time was observed (U = 2521, p = 0.03; U = 2477, p = 0.03, U = 2440, p = 0.01, U = 2326, p = 0.004, U = 2482, p = 0.02, respectively).
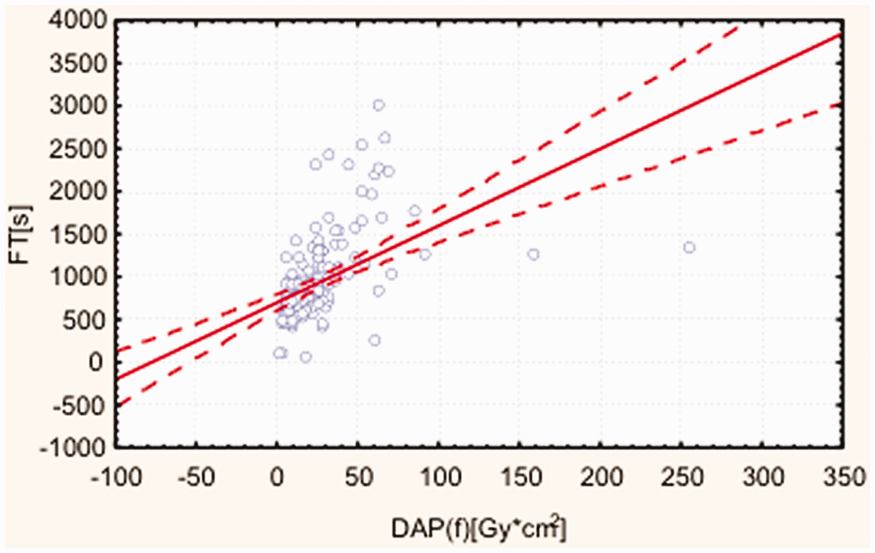
Figures 1 and 2 graphically present the data on AK for fluoroscopy and total AK in relation to fluoroscopy time and exposure time as well as fluoroscopy DAP in relation to fluoroscopy time.
AK for fluoroscopy and total AK in relation to fluoroscopy time and exposure time. AK: air kerma. Fluoroscopy DAP in relation to fluoroscopy time. DAP: dose-area product.
Age and gender were not significant factors for DAP and AK in either fluoroscopy or radiography acquisition (p > 0.05).
No DE and SE of acquired radiation were observed in short (21 days) or middle-term (12 months) observations.
Discussion
Medical professionals have to take into account the DE and SE of radiation for their patients. High-dose ionizing radiation (DE) can cause syndromes like hematologic disorders and gastrointestinal symptoms.2,17,18 Acute skin injury is the major radiation risk, which is mentioned in ICRP Report 103.27–29 The threshold for radiation damage to skin (DE) varies from individual to individual, but is generally estimated to be 2 Gy. 3 This type of skin injury usually appears several days (<30 days) after the procedure. 1 Radiation is known to cause cancer induction (SE), where there is no threshold (at any dose level), and the likelihood of cancer increases with the increasing dose. 30 Our data demonstrated that patients undergoing carotid stent implantation receive a mean radiation dose lower than 1 Gy.
Large numbers of parameters affect the radiation dose received by the patient during an intervention procedure. Parameters can be divided into those that depend on the operator (user-controllable) and those that are not operator-dependent. Some parameters are related to the design of the equipment and its calibration. Some of them depend on the size of the patient and anatomical difficulties, and others depend on the operator’s (user-controllable) experience. User-controllable parameters such as adjustment of the irradiation geometry and management of the exposure parameters may also have remarkable effects on radiation doses.
The following factors should be discussed.
BMI
In obese patients, the X-ray beam penetrates deeper layers of tissues; for this reason, higher energy is used. In our study, all patients who received a radiation dose exceeding 1 Gy had a BMI above 30. Attempts to reduce the radiation dose (total AK) with the use of collimators, pulsed fluoroscopy and minimized fluoroscopy time should always be made. 31 BMI exceeding 25 is an independent risk factor contributing to higher radiation dose (mean total AK > 1 Gy).
Severity of the carotid stenosis
The degree of carotid stenosis is the next factor, which affects the radiation dose.
In general, it is more likely to expect technical trouble with passing with the guide wire through a narrow calcified artery, especially during protection device placement. Stenosis greater than 90% often requires predilatation before stent placement. This means that the dose acquired by the patient is mainly determined by fluoroscopy time (as shown in our study). Repeated DSA is not an additional risk factor, because working on the ‘road map’ with proper pre-implantation diagnostics of the stenosis does not force the operator to perform additional contrast imaging even in severe, challenging stenosis.
The use of a cerebral protection device cannot be treated as a separate risk factor for increased radiation, because the problems with the implantation of the device are mainly caused by the complexity of the stenosis. Passing with the guide wire through the lesion with or without protection represents the same degree of difficulty for the operator, and fluoroscopy time depends only on the lesion itself.
As a result, the use of DSA is not an additional risk factor for the radiation overdose, as opposed to aortic stent-graft placement or interventions on lower limbs.32–36
Technical parameters
Patient exposure to ionizing radiation is dependent on two factors: exposure time/fluoroscopy and radiation dose (DAP/AK) that was generated during the procedure. The dose is dependent on the absorbent. The change of the angle of the radiation beam from the natural (orthogonal angle) increases the radiation dose. This is a consequence of increasing the route, which the beam of radiation must cover, at the same time being acquired by the human body. 27 The second factor (exposure time/fluoroscopy) depends on the complexity of the procedure being performed and the skills of the operator (user-controllable). While performing the procedure, it is advisable to reduce the amount of repetitions and the number of image frames to a minimum.35 Since the source of ionizing radiation is located in the vicinity of the patient’s head, one must remember that such large doses of radiation may cause changes in the cornea – part of an eye, which is very sensitive to ionizing radiation. The angulation should therefore be limited according to the principle of ‘As Low As Reasonably Achievable’ to a possible minimum. 36
The complexity of the lesion and the experience of the operator in passing with the guide wire through the lesion are probably the most important factors influencing patient doses. 29 However, in our case, the experience of the operator was not an important issue, and both operators possessed the required level of the expertise necessary for safe carotid stenting.
Conclusion
Carotid artery stenting is a relatively safe radiological procedure in scope of radiation dose acquired by the patient. The main factors contributing to possible radiation overdosing are BMI value and complexity of the carotid lesion.
Proper preoperative planning in obese and complicated patients may reduce the fluoroscopy time and contribute to reduced dose acquisition.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.