
Abstract
Objective
The Food and Drug Administration and the Vascular Quality Initiative still utilize fluoroscopy time as a surrogate marker for procedural radiation exposure. This study demonstrates that fluoroscopy time does not accurately represent radiation exposure and that dose area product and air kerma are more appropriate measures.
Methods
Lower extremity endovascular interventions (N = 145) between 2013 and 2015 performed at an academic medical center on a Siemens Artis-Zee floor mounted c-arm were identified. Data was collected from the summary sheet after every case. Scatter plots with Pearson correlation coefficients were created. A strong correlation was indicated by an r value approaching 1.
Results
Overall mean AK and DAP was 380.27 mGy and 4919.2 µGym2. There was a poor correlation between fluoroscopy time and total AK or DAP (r = 0.27 and 0.32). Total DAP was strongly correlated to cine DAP and fluoroscopy DAP (r = 0.92 vs. 0.84). The number of DSA runs and average frame rate did not affect AK or DAP levels. Mean magnification level was significantly correlated with total AK (r = 0.53).
Conclusions
Fluoroscopy time shows minimal correlation with radiation delivered and therefore is a poor surrogate for radiation exposure during fluoroscopy procedures. DAP and AK are more suitable markers to accurately gauge radiation exposure.
Introduction
Patients and practitioners alike are regularly exposed to significant doses of radiation during image-guided procedures that are considered routine in this day and age. Already in the mid-2000s, there was an exponential rise in endovascular interventions such that there was at least a fourfold difference between endovascular and open surgical procedures performed per year. 1 Patients undergoing endovascular treatment can now expect to have extensive follow-up surveillance imaging as well as secondary endovascular interventions. Moreover, with the ability to perform more complex endovascular aortic reconstructions, the dose of radiation after one case can reach significant levels. 2 Overall increase in radiation has led to a greater awareness of radiation exposure to both the patient and operator. Since 1994, the Food and Drug Administration (FDA) has required documentation of total fluoroscopy time as the surrogate marker for radiation exposure after every case. 3 The Vascular Qualitative Initiative (VQI) has also adopted this method of tracking.
Current digital fluoroscopy machines are more sophisticated than their previous counterparts and now have multiple features that can manipulate image intensity, magnification, and frame rate to moderate radiation levels. All current machines regularly record radiation delivered, fluoroscopy time, cine runs, magnification levels, and calculated variables such as total radiation burden. Delivery of radiation is measured in air kerma (AK), which is the amount of energy released per unit mass (Gy) from a beam of radiation on a single point in the X-ray field.4,5 As a reference point, patients experience transient erythema and temporary epilation at 3 Gy and permanent epilation with prolonged erythema at 7 Gy. 6 The total radiation burden, or Dose Area Product (DAP), to the area being irradiated is then calculated from the product of AK and the X-ray field (cm2). The size and location of the irradiated field is important in the consideration of vital organs being exposed to penetrating X-rays. 7
Although fluoroscopy time was the best available indicator of radiation exposure in the past, it is now an anachronistic measuring tool. Major factors that affect total exposure such as patient size, rate of delivery, site of skin exposure, and fractionation of exposed dose cannot be accounted for by fluoroscopy time. In this single-center study, we demonstrate that fluoroscopy time is not a reliable surrogate for the radiation delivered to the patient.
Methods
Study design
A single academic institution database of lower extremity endovascular procedures was queried for all lower extremity endovascular interventions between the years of 2013 and 2015. These procedures were identified by the following Current Procedural Terminology (American Medical Association, Chicago, IL, USA) codes: 37220, 37221, 37224, 37225, 37226, 37227, 37228, 37230, 37231. All procedures were performed in an angiosuite with a Siemens Artis-zee (Siemens AG, Munich, Germany) floor-mounted c-arm. The number of DSA runs, total fluoroscopy time, fluoroscopy DAP, fluoroscopy AK, cine DAP, cine AK, total DAP, and total AK were collected from the radiation summary sheet generated by the system at the completion of each case. Total fluoroscopy time was inclusive of all fluoroscopy and cine/DSA runs.
The magnification levels of each cine run were averaged to generate a simple marker of the amount of magnification used for the case. We extrapolated that the majority of fluoroscopy time preceding a cine run would mirror a similar magnification level. Magnification level, measured in cm2, is inversely related to the area of the irradiated field such that the greater the magnification the smaller the field.
Means for all collected values were calculated. We assessed for correlation between fluoroscopy time and AK or DAP with a primary endpoint of a non-correlation between these variables. Secondary endpoints were correlation between magnification level, number of cine runs, average frame rate, and AK or DAP.
Statistical analysis
Means and margin of error were calculated for all measured variables. A confidence interval of 95% was used to express all variables. A comparison of continuous variables was completed using the Student’s t-test. Scatter plots were created and Pearson correlation coefficients were calculated to assess for correlation. An r-value of 0 indicated no correlation and an r-value of 1 indicated a complete correlation. Values between 0 and 1 were graded based on degree of strength as they approached complete correlation. An r > 0.5 was considered a significant correlation.
Results
Procedure characteristics
A total of 145 patients were identified who underwent peripheral endovascular procedures between 2013 and 2015. The majority of cases were for single-level intervention (119, 79%) followed by double-level intervention (29, 20%) and triple-level intervention (1, 1%) as indicated in Figure 1. Single-level interventions include iliac, femoral-popliteal, or tibial angioplasty or stenting. Double intervention included combination of iliac and femoral-popliteal or tibial and femoral-popliteal angioplasty or stenting. Atherectomy was another possible femoral-popliteal intervention. Twenty-three of 29 double intervention cases included the femoral-popliteal and tibial vessel segments. One case required triple-level intervention, which included iliac, femoral-popliteal, and tibial angioplasties.
Levels of endovascular intervention.
Mean values collected from radiation summary sheets upon case completion.

Relationship between fluoroscopy time and AK or DAP
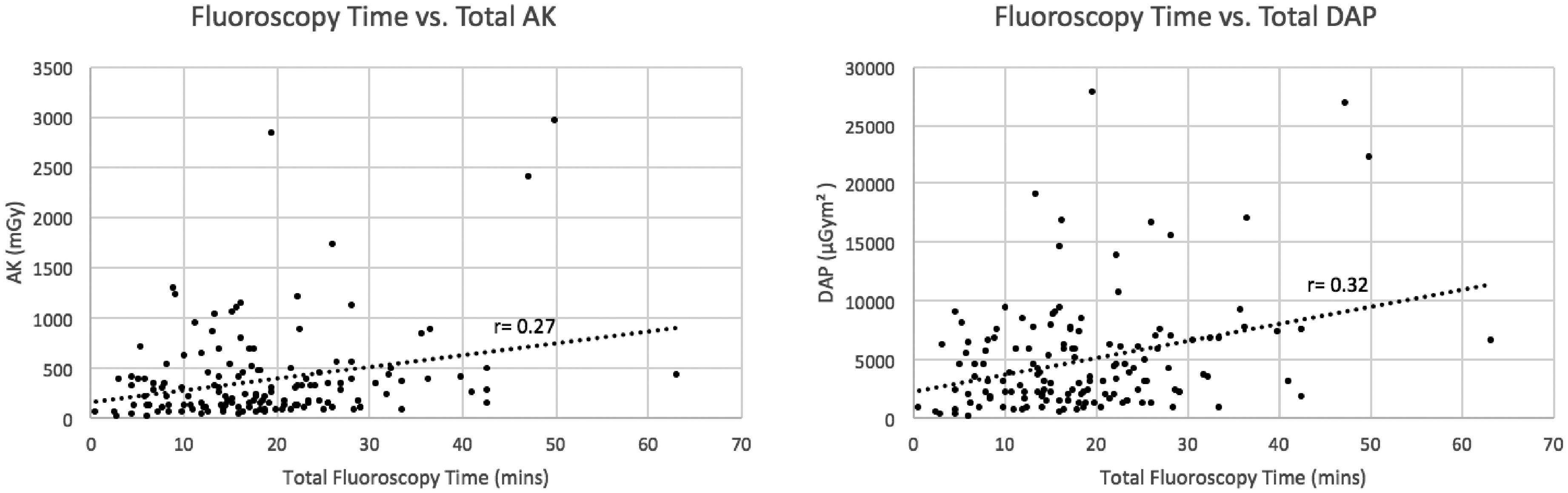
Cine AK and fluoroscopy AK were both strongly correlated to total AK (r = 0.95 and r = 0.92, respectively, Figure 2). Not surprisingly, fluoroscopy DAP correlated strongly with total DAP (r = 0.84) and cine DAP correlated very strongly with total DAP (r = 0.92, Figure 2). Fluoroscopy time showed a poor correlation with total AK (r = 0.27) and a poor correlation with total DAP (r = 0.32, Figure 3).
Fluoroscopy AK/DAP and cine AK/DAP vs. total AK/DAP. Fluoroscopy time vs. total AK/DAP.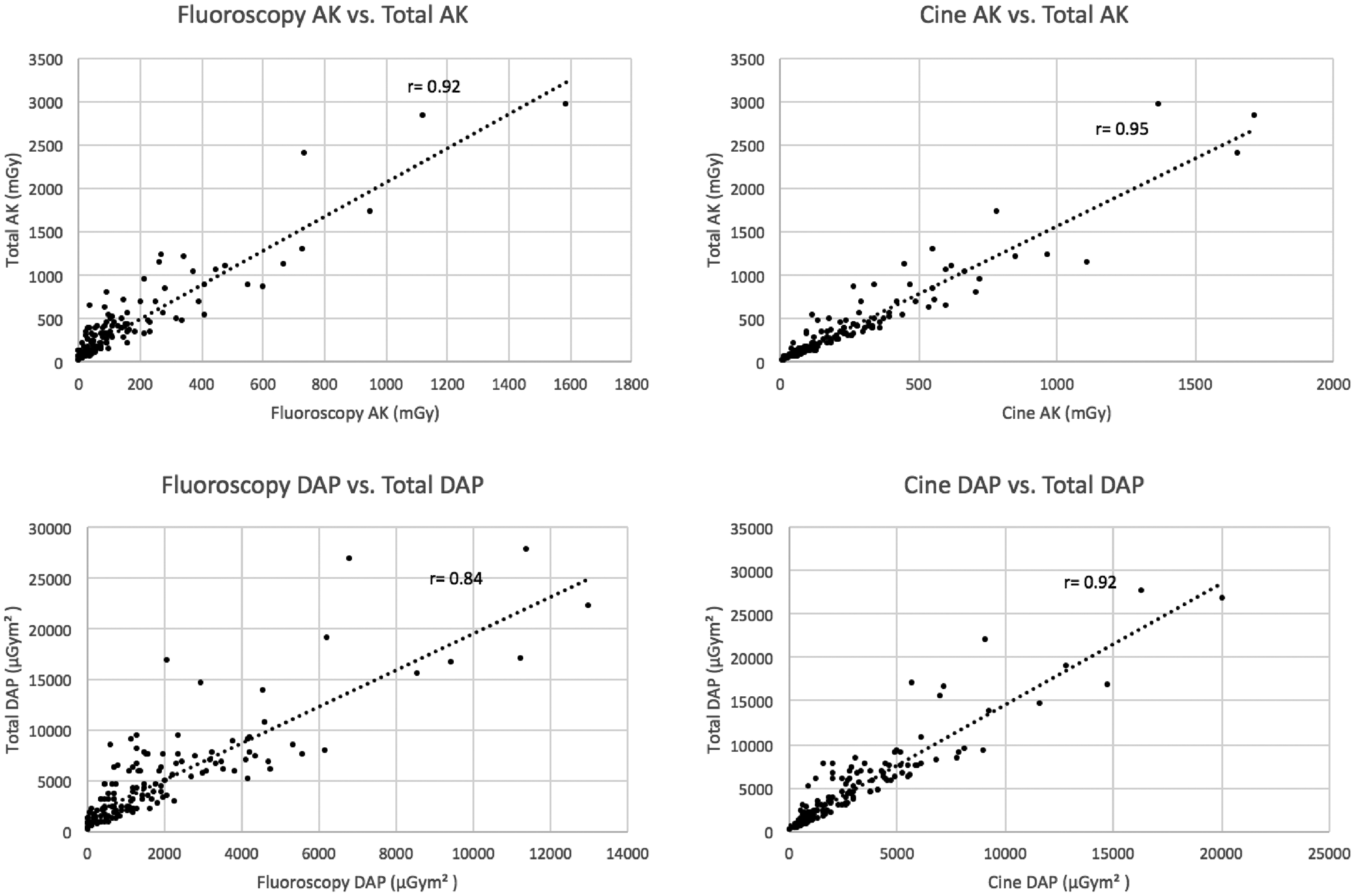
Relationship between AK or DAP and other user controlled variables
Operator-controlled variables were tested against AK and DAP. The number of DSA runs did not correlate with total AK (r = 0.07) or total DAP (r = 0.07). The mean frame rate neither correlated to AK (r = 0.037) or to DAP (r = 0.01). There was a significant correlation between mean magnification level and total AK (r = −0.53, Figure 4). Higher magnification levels correlated with higher radiation delivered. Meanwhile, there was no correlation between average magnification and total DAP (r = 0.08). This non-correlation is expected as the calculation of DAP includes the adjustment of magnification to a set field of view.
Mean magnification vs. total AK.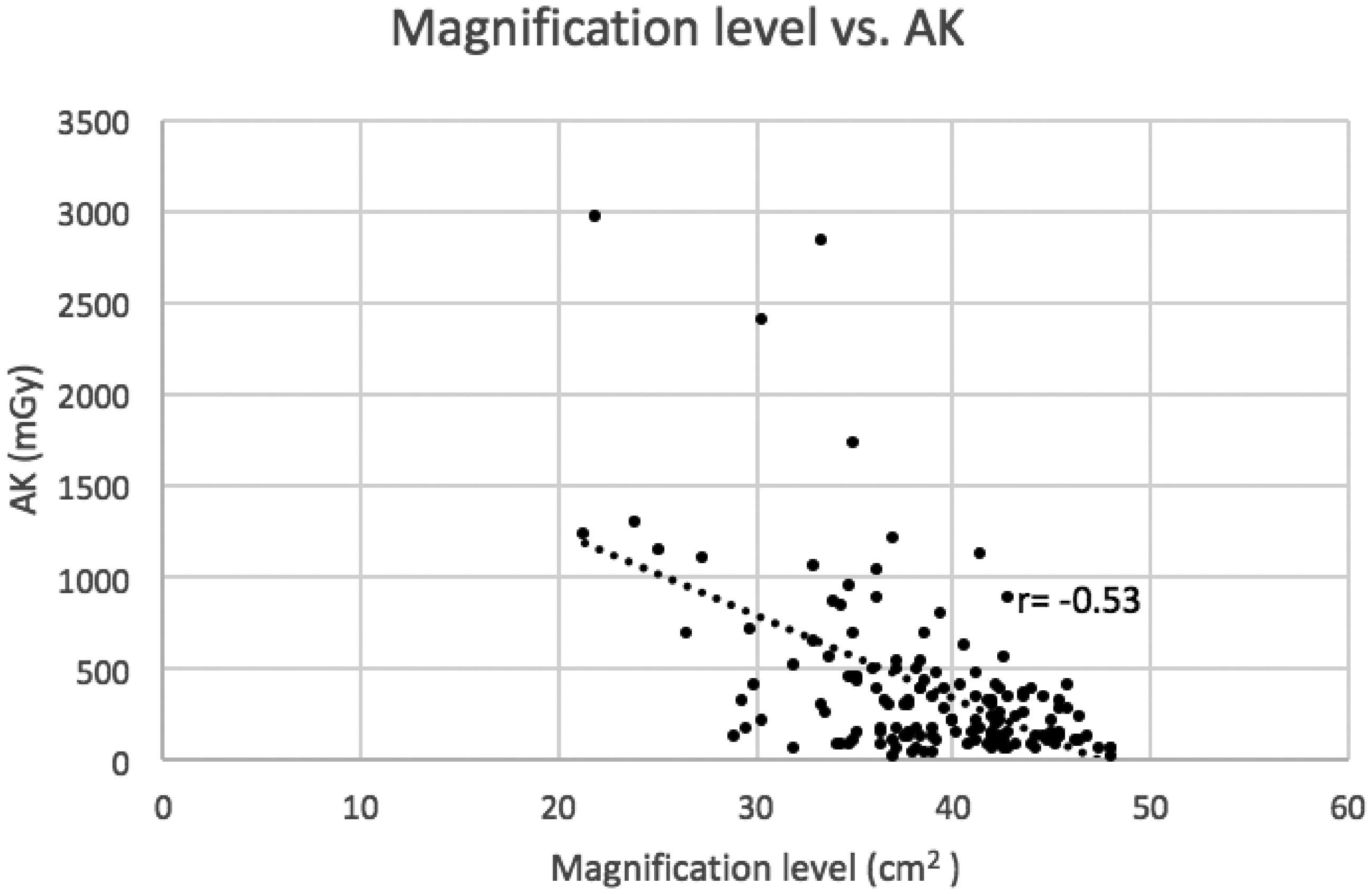
Discussion
AK and DAP are among the most often used measures of radiation delivery and exposure to the patient during fluoroscopic-guided procedures. Tracking and quantifying radiation exposure is useful in both the acute and long-term setting. Immediately post-op, patients are given instructions to monitor their skin for the deterministic effects of radiation, which include erythema, epilation, pruritus, and burning. Some sensitive sites including the anterior neck, chest, and abdomen can show signs of radiation injury within hours of high exposure. In the long term, documentation of radiation exposure is both helpful in choosing procedures to reduce total exposure as well as monitoring cumulative exposure. Although there is no clear evidence of lifetime diagnostic radiation leading to cancer, there are studies that show that with increased medical radiation, patients are being exposed to levels that exceed recommended lifetime limits. 8
Reduction of procedural radiation has become an important endeavor in medicine and various improvements have been made in both equipment and procedure technique. Radiation machines are now able to decrease radiation without compromising image quality. The Siemens Combined Application to Reduce Exposure (CARE) protocol provides built-in radiation reduction mechanisms: filtration of overly high/low X-ray beams that do not contribute to the final image, lower default frame rate, re-positioning of the beam without active fluoroscopy, and collimator adjustment with image hold. 9 These new technologies have also encouraged operators to use certain maneuvers to reduce radiation including decreasing distance between the patient and the X-ray detector, initiating fluoroscopy at the optimal time, minimizing number of cine runs, and avoiding use of high magnification. 10 Kenneth et al. found that the combination of an overall cultural change in the angiosuite as well as the institution of protocols has led to a reduction of radiation delivery to patients by 40% over three years. 5 To increase operator awareness at our institution, we have introduced alarms at intervals of 1 Gy to alert the operator of real-time total radiation. We maximize collimation, reduce frame rate, and reduce to low-dose energy regularly to reduce patient exposure. To reduce operator exposure, we use power injection and distance ourselves from the beam at every opportunity. This seems to vary the most amongst operators.
Advancements in imaging technology have also allowed for reduction in radiation. Post-EVAR surveillance with duplex ultrasound and abdominal X-ray has become more prevalent as technicians gain comfort with these techniques. Harrison et al. showed that these imaging modalities were appropriate for identifying endoleaks, aneurysm growth, stent migration, stenosis, and occlusion prior to obtaining CT angiography. 11 Intraoperative intravascular ultrasound (IVUS) has been shown to be a useful technique during lower extremity interventions and EVAR to reduce contrast load and radiation in contrast allergic and renal impaired patients while maintaining precision of deployment. 12 3D Fusion CT is a newer technique that provides precise mapping for complex aortic repairs involving multiple branched vessels. McNally et al. demonstrated a significant radiation reduction (3400 mGy vs. 1380 mGy) in 31 patients undergoing FEVAR with the assistance of fusion CT. 13
Of course, there are other major factors that are beyond the control of the operator and technology for which one needs to be mindful. The type of procedure being performed is another crucial factor in determining overall radiation. In a systematic review of 24 articles, Monastitiriotis et al. demonstrated that greater level of technical difficulty will result in greater total AK and DAP. 14 The authors showed that there was higher radiation delivery and exposure in aortic cases ranging from infrarenal to thoracic and to fenestrated. Infrarenal EVAR delivered on average 7948 µGym2 per case. 14 Thoracic EVAR (TEVAR) had a mean DAP of 17,300 µGym2 in a study of 232 cases by Howells et al. 15 In 53 Fenestrated EVAR (FEVAR) procedures, Howells et al. showed a whopping DAP of 32,060 µGym2. Patients with high body mass index (BMI) were found to have an almost 3-fold increase in radiation compared with patients with normal BMI. 14 Total AK and DAP are both increased because more radiation is required for adequate penetration and there is more surrounding tissue that absorbs that radiation. These lessons can be extrapolated to the lower extremity.
To further compare, Majewska et al. described the radiation levels in other common endovascular procedures. 16 Total AK and DAP after carotid stenting was 317 mGy and 5300 µGym2, 687 mGy and 14800µGym2 after renal stenting, and 662 mGy and 19900 µGym2 after iliac stenting. 17 Comparatively, our study patients fall in the lower spectrum of radiation exposure, as expected. Our mean total AK was 380.3 mGy and total DAP was 4919.2 µGym2.
Currently, the only standardized value used by the FDA and the Vascular Quality Initiative (VQI) to estimate and regulate the total radiation exposure to the patient is fluoroscopy time. This dates back to 1994 when the FDA was alerted of radiation skin injuries by anecdotal evidence. 18 At the time, the administration issued a set of recommendations for the reduction and regular surveillance of fluoroscopic procedures. A call for new protocols for radiation reduction was paramount. The FDA suggested a frame rate reduction, from 0.02 to 0.05 Gy/min at the time, and documentation of fluoroscopy time. 6 Our study shows that fluoroscopy time does not correlate with radiation exposure. The mean fluoroscopy time in our case series was 18.7 ± 1.7 min with a mean frame rate of 3.0 ± 0.1 fr/s. Magnification rate had a significant correlation to total AK (r = −0.53). Fluoroscopy time was poorly predictive of total AK or DAP (AK, r = 0.27, DAP, r = 0.32). As shown by the student’s t-test, we found that cine is a greater contributor to overall exposure than fluoroscopy as it delivered significantly greater AK and DAP (p < 0.05). This highlights the probable cause of inaccuracy of fluoroscopy time as a marker of radiation. We show that cine is the primary component of total radiation but the time spent in cine mode is minimal compared to the time spent in fluoroscopy mode. This demonstrates that time is a misrepresentation of overall radiation because it is skewed by the overwhelming majority of time spent in fluoroscopy mode.
Our study is not without limitations. There was operator variability in case volume and technique such that the type of cases performed and total radiation per case varied. Due to low case numbers of certain procedures, we could not show radiation differences between anatomic levels of intervention. BMI, which can affect AK levels, was not collected and assessed in this study. Body shape is an important factor as fat distribution (whether in the legs or abdomen) can significantly affect the radiation dose. To approximate mean magnification during each case, we were forced to assume that the levels during fluoroscopy were the same as the preceding cine or DSA run.
The lack of correlation between fluoroscopy time and total radiation exposure demonstrates that fluoroscopy time is a poor surrogate for radiation delivered during a case. Recording fluoroscopy time as the marker of radiation was perhaps the best available method with respect to older, simpler machines. At this time, it has little value in predicting exposure. There has been a recent movement to recognize that radiation surveillance is especially important in complex EVAR, TEVAR, and FEVAR cases that deliver >2 Gy. Some authors have broached the topic of the inadequacy of fluoroscopy time in complex TEVAR and FEVAR cases but none have shown such a clear difference between AK/DAP and fluoroscopy time, especially in peripheral interventions. AK and DAP, which are easily obtained, would offer an excellent source for predicting total radiation during fluoroscopic interventions and should therefore be universally incorporated and recorded in our quality databases. These measures may be the best for preoperative planning and tracking lifetime exposure in the endovascular era. A more accurate awareness of radiation levels using AK and DAP may encourage further behavioral change and development of improved protocols to reduce radiation to our patients.
Footnotes
Acknowledgement
This article has been presented at the 26th Annual VESS Meeting 2016.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.