
Abstract
The objective of this study was to assess the safety of a new developed sutureless vascular adapter system in a porcine model. In five pigs, 4-cm-long polyester prosthesis (6 mm diameter) were implanted and anastomosed with the newly developed adapter proximally and suture anastomosis distally. The integration of the adapter was investigated in comparison to the suture anastomosis. These investigations were performed by light microscopy and scanning electron microscopy. Median operative time for performing the adapter anastomosis was significantly shorter compared to suture anastomosis (66 s vs. 246 s, p < 0.05). Median estimated blood loss during adapter anastomosis implementation was 22.5 mL (range 19.0–25.0 mL) compared to 48.2 mL (range 45.4–63.5 mL, p < 0.05). In five hand-sewn anastomoses, overall eight additional stitches were necessary whereas all adapter anastomoses showed primary leak tightness. This in vivo study shows the technical feasibility of the newly developed adapter.
Introduction
Whilst especially in gastrointestinal surgery anastomotic devices are broadly used, in vascular surgery suture anastomosis remains the gold standard. This standard was implemented in the beginning of the 20th century by Carrel et al. 1 In general, hand-sewn anastomoses show in their finishing large intra-individual differences. Target of the application of anastomotic devices is to improve the standardization of surgeries and to reduce individual differences caused by the surgeons. Unfortunately, none of the currently available devices did make its way into clinical daily practice. 2
Aside from interventional vascular therapies, there are a large number of patients requiring a conventional vascular surgery with the respective vessel anastomoses. Therefore, it is no wonder that in coronary vessel surgery 3 as well as in aortic and peripheral bypass surgery attempts are constantly made to establish a robust alternative to the hand-sewn anastomosis.4,5
The objectives of this study were to assess the development of a new adapter vascular system regarding its safety in a porcine model. Our hypothesis is that the adapter has an improved primary blood tightness and may be implemented into the vessel in a shorter time.
Technical note
The adapter we would like to introduce here is made completely of polyethyleneterephthalate (PET) (Figure 1). It has fenestrations to reduce contact surface and device depending pressure on the vessel wall. Via the extraluminal clamp fixation mechanism, contact pressure on the vessel wall may be adjusted to the individual situation with this clamp mechanism. The adapter is equipped on one side with a hinge; closing is performed over the other side with a ratchet mechanism. Four rows of teeth stand against each other and allow for pressure-adapted closure of the adapter, which is adjusted to the delicacy of the vessel wall. Closing the adapter is performed stepwise until blood tightness (Figure 1(c)). The adapter can be produced in any diameter from 4 mm internal diameter upwards. In a previously performed in vitro study, the maximal load capacity was evaluated according to Shifrin et al.
2
Here were used cadaveric arteriosclerotic iliacal vessels, which also showed primary patency. The here presented in vivo feasibility study was performed in pigs according to the guidelines of the Ethical Committee for Animal Research and is fully compliant with the recommendations outlined in the Guide for the Care and Use of Laboratory Animals (Institute of Laboratory Animal Resources, Commission on Life Sciences, National Research Council, Washington, DC).
Technical data sheet of the vascular adapter: (a) three-dimensional animation, (b) technical drawing, (c) schematic picture of the ratchet mechanism.
Five pigs (hybrid of German black pied, German Edelschwein and Pietrian, Fa. Kilian, Germany), 3 months old with a body weight of 35–40 kg were used for this study. Primary planned observation period was 6 weeks. A distance of 5 cm of the infrarenal aorta was dissected. Prior to implantation, the Dacron® prosthesis is folded into a notch of the connector and secured on the outside by a pushed over ring. Proximally in every case, the vascular adapter was connected with the 6 mm coated Dacron® prosthesis (Braun, Germany) and inserted into the aorta. Distally the anastomosis was performed with a continuous polypropylene suture (Prolene® 5/0, Ethicon, Germany). Closure of the abdomen was performed. In order to achieve a better comparability of both procedures and due to a higher clinical relevance the clamping time was measured in seconds. The clamping time was defined from the clamping of the inflow vessel till tightness of the anastomosis. A fixing zone of the adapter of maximal 10 mm (for all available adapter diameters) provides the possibility of an application of the adapter close to the vessel junction; therefore, postulating additional 5 to 10 mm way for the so-called “clamping zone” during implementation to limit the additional tissue damage.
Prior to the aortotomy, blood dryness in the operation field was established. Blood lost during performance of each anastomosis was collected by an operation sucker and measured in milliliters (mL). Body weight was measured (in kg) as a surrogate parameter for the clinical wellbeing of the pigs. Diameter of the pig aorta was measured before and after implantation period in millimeters (mm).
A 7-cm-long segment including the native porcine aorta, the adapter, the Dacron® prosthesis, as well as the suture anastomosis was harvested. Every explant was divided into five segments (Figure 2): first segment (A–C) – porcine proximal aorta, second segment (D–F) – adapter anastomosis with the aorta, third segment (G–I) – vascular prosthesis with the adapter, fourth segment (J–L) – vascular prosthesis, and fifth segment (M–O) – suture anastomosis. Specimens were divided and fixed for immunohistochemistry in 4% buffered formalin and for scanning electron microscopy (SEM) in glutaraldehyde.
Investigation of the explanted specimens. Specimens were divided and fixed. Column 1: macroscopic separation, column 2: immunostaining of the sections, column 3: SEM investigation. Row A–C: Porcine aorta section: arrow a: intima of the porcine aorta. Row D–F: adapter anastomosis: arrow a: neointima in the adapter, arrow b: endoluminal part of the adapter, arrow c: extraluminal part of the adapter, arrow g: vital aortic wall, white distance between vessel wall and outer part is artificial due to tissue shrinkage during fixation. Row G–I: Vascular prosthesis with adapter: arrow a: neointima, arrow c: outer fixation ring of the vascular prosthesis on the adapter, arrow e: polyester material of the vascular prosthesis. Row J–L: Vascular prosthesis: arrow a: neointima of the coated Dacron® prosthesis, arrow e: polyester material of the vascular prosthesis. Row M–O: Suture anastomosis section: arrow a: intima of the porcine aorta, arrow f: focal compression of the aortic wall by vascular sutures.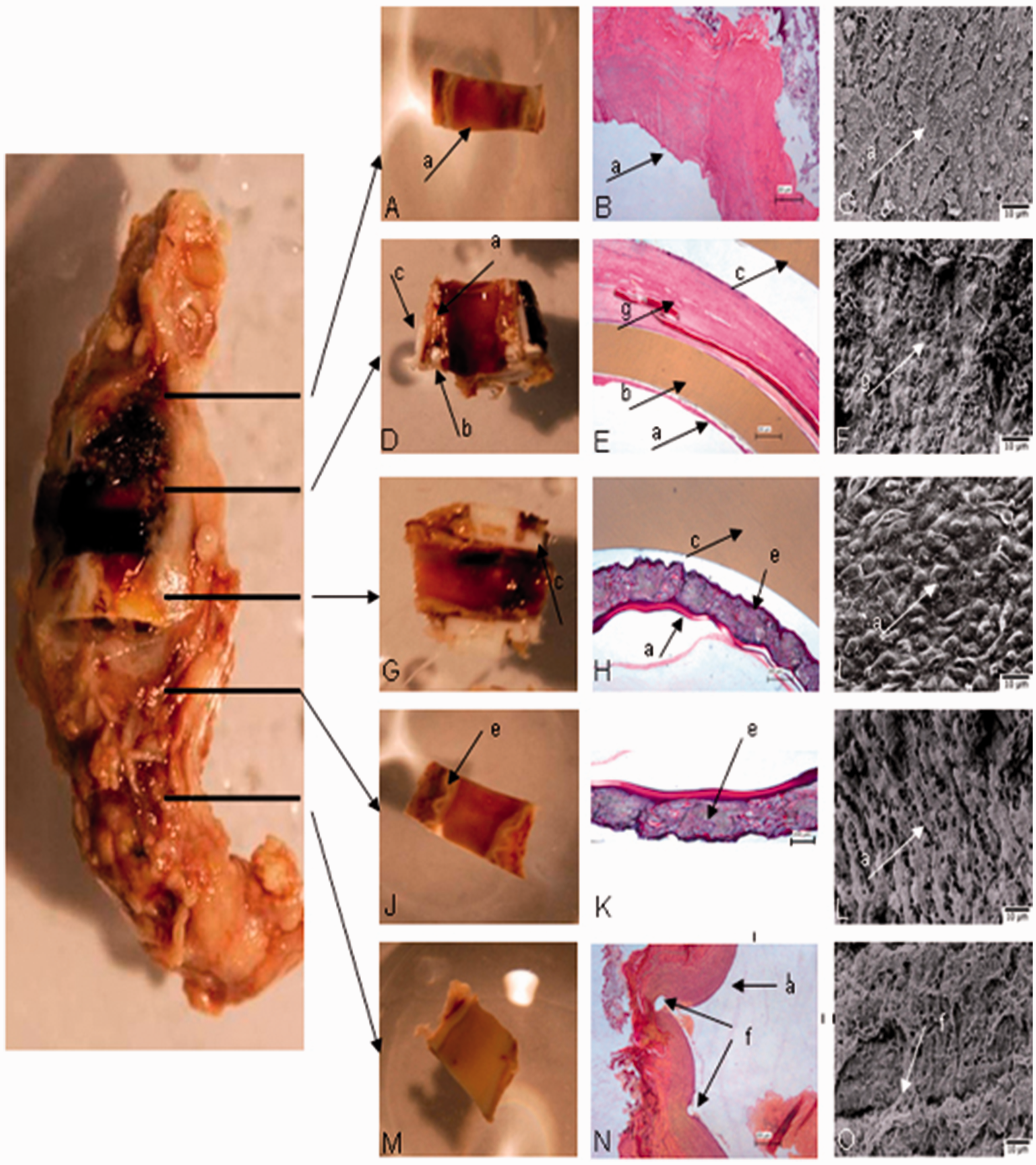
In light microscopy, a neointimal surface could be determined in all investigated segments. In one pig a thrombus had been detected in the region of the suture anastomosis, which occluded the aortal lumen up to 30% (one of five anastomoses = 20%). The aortic wall between the clamping trays of the adapter was vital 6 weeks after implantation. No thrombotic sediments were detectable (zero of five anastomoses = 0%). All segments showed a vital aortic wall. No pressure-induced necrosis or destruction of the aortic wall was detectable (Figure 2, D–F). SEM confirmed a complete neointimal surface development of adapter-, prosthesis- and suture-anastomosis region. Neointimal surface was positive for CD34 and CD31 in immunostaining; this in combination with the SEM observations confirmed the internal layer as neointima.
First segment and fifth segment showed the normal anatomic structure of the porcine aorta. This was used for comparison with the artificial regions second to fourth segment. The proximal (adapter) anastomosis showed no intimal hyperplasia whereas in three of five pigs a local intimal layer hyperplasia in the suture anastomosis was detected. In one pig, the mentioned hyperplasia of the intima was circular (Figure 2, SEM column). The post mortal destruction of the tissue surface showed many fibroblastic cells in deeper levels, as an indication of integration of the alloplastic material into the perivascular tissue.
Discussion
Sutureless anastomosis for arterial vessel reconstruction remains a suitable alternative to hand-sewn anastomosis; this has not changed with the wide application of endovascular techniques. Frequently there are studies of polymer-based techniques but more for small vessels; until now these were not established for large vessel in daily clinical practice. 3 Stapling devices appear time and again as patent registration without significant animal experiments or even clinical trial results to follow. 6 Furthermore, adapter-based devices are introduced that occasionally find their way into clinical trials.7,8
The adapter with its fixation mechanism, tested here in a porcine model, was well tolerated. During study period, these pigs nearly doubled their median body weight of 37.2 kg (range 35.3–38.0 kg) before implantation versus 61.8 kg (range 60.2–63.5 kg) before harvesting. Pigs’ aortic diameter increased during observation from median 6.2 mm to 7.5 mm (p = 0.008). Compared to the suture anastomosis, median clamping time for the adapter was significantly shorter 66.0 s (range 60.0–78.2 s) versus 246 s (range 201–325 s, p < 0.05). Estimated blood loss during adapter anastomosis implementation was 22.5 mL (range 19.0–25.0 mL) compared to 48.2 mL (range 45.4–63.5 mL, p < 0.05) during suture anastomosis. For the five hand-sewn anastomoses, eight additional stitches were required to achieve leak tightness while in all adapters primary tightness was accomplished.
Previous technical tests showed that ratchet technique provides the possibility to adjust the system lyrical to different vessel walls of different thickness. This mechanism did not show any pressure-induced impairment of the vessel wall. This would be a crucial advantage for the arteriosclerotic vessel wall in humans, compared to the stapler alternative that maltreats the rigid arteriosclerotic vessel wall with the folding. 6 This is also an advantage especially compared to the BYFix device, which especially in the initial phase fixes in the vessel wall only with the barbs. 7
The adapter is well integrated into the vessel wall and does not increase the thrombogenity of the junction to the original vessel wall. Even better, there was no endoluminal thrombus and intimal layer hyperplasia to be seen compared to the hand-sewn anastomosis. A characteristic trait is the easy handling. Based on the very reasonable production costs, it is possible to have adapters in 2 mm size differences in store, which enables the individual customizing to the vessel of the patient.
Primary tightness after implementation reduces the time effort compared to the hand-sewn anastomosis significantly.
Without any doubt, there are limitations of this proof of principle study. The incorporation of the adapter has been done in soft vessels without any arteriosclerotic changes. Further investigations of the adapter (results shown not here) showed that a high rate of primary tightness can be achieved even in arteriosclerotic impaired vessels. It is difficult to provide data on the loss of elasticity of the vessel wall induced by the adapter. The investigation in humans may be considered challenging since the arteriosclerotic vessel wall of the patient shows intrinsically a significant loss of elasticity. Furthermore, data about the long-term patency of the adapter in situ are limited. The porcine model was chosen here since these animals show similar vessel-healing mechanisms like humans. It is sure that the growth period of the animal and the implemented adapter did not influence each other in a negative manner. Comparing the aging process of the pig to the human, a 6-weeks follow-up period in the porcine model would equal approximately 18 months in the human. 9
Conclusion
Adapters for vessel reconstructions and sutureless anastomoses are of broad interest in vascular medicine.10,11 The adapter system presented here is considered a step towards increased reproducibility of vessel anastomoses. Intuitive handling, shorter clamping time, and reduced blood loss are the first proven advantages of this new adapter compared to hand-sewn techniques.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.