
Abstract
Objectives
The purpose of this study was to investigate whether there are differences among clinical conditions and traditional atherosclerotic risk factors between patients with large abdominal aortic aneurysm and those with occlusive non-coronary arterial disease.
Methods
We clinically examined 519 patients with asymptomatic abdominal aortic aneurysm and 672 with severe obstructive arterial diseases before surgical repair.
Results
In patients with abdominal aortic aneurysm, we identified a clear predominance of males (p < 0.001), more alcohol consumers (p < 0.05), higher values of diastolic blood pressure (p < 0.05), higher values of serum creatinine (p < 0.005), more hyperuricemic patients (p < 0.005) and less diabetics (p < 0.001). In patients with occlusive atherosclerotic vasculopathies, we observed more smokers (p < 0.05), higher systolic blood pressure and more hypertensives (p < 0.05 respectively) and a prevalence of hypertriglyceridemia (p < 0.05).
Conclusions
Patients with abdominal aortic aneurysm were mostly males with diastolic hypertension, impaired renal function and less diabetics, while patients with occlusive arteriopathy were more smokers, hypertensives and more hypertriglyceridemics.
Introduction
Obstructive arterial diseases (OADs) and abdominal aortic aneurysms (AAAs) share the same risk factors and today are still considered atherosclerotic events. The hypothesis that an AAA develops as a pathological response to aortic atherosclerosis, which was suggested more than half a century ago when the term ‘atherosclerotic aneurysms’ was commonly used, is still prevalent today. 1 However, there are epidemiological, biochemical and structural differences between occlusive atherosclerosis and AAA. Currently, there is evidence that OADs and AAAs affect distinct layers of the arterial wall: atherosclerosis mainly affects the inner layers, intima and media, whereas AAA typically affects the outer layers, media and adventitia. Moreover, the dilatative manifestation of AAA is the opposite of the occlusive atherosclerosis. The reasons for the occurrence of these two differing conditions remain obscure. 2 Whether the presence of atherosclerosis in the AAA development is an epiphenomenon rather than the cause itself still remains unknown. Patients with AAAs and those with OADs, including ischemic heart disease, carotid artery stenosis (CAS) and peripheral artery disease (PAD), have overlapping cardiovascular risk profiles. Although conventional cardiovascular risk factors, such as age, male gender, diabetes mellitus, hypertension, smoking and dyslipidemia, are often observed in patients with AAA, a number of studies report conflicting results on the relationship between these risk factors and AAA. 3 Moreover, it is still unclear why some people develop AAAs, whereas others develop OADs, despite similarities in their cardiovascular risk profiles. This study was performed during the preoperative cardiac assessment of patients with arterial diseases of the three main districts, prior to surgical revascularization, with the aim to investigate whether there are differences among major atherosclerotic risk factors in patients with large AAAs and those with OADs.
Patients and methods
Clinical characteristics of the two subgroups with obstructive arterial disease.
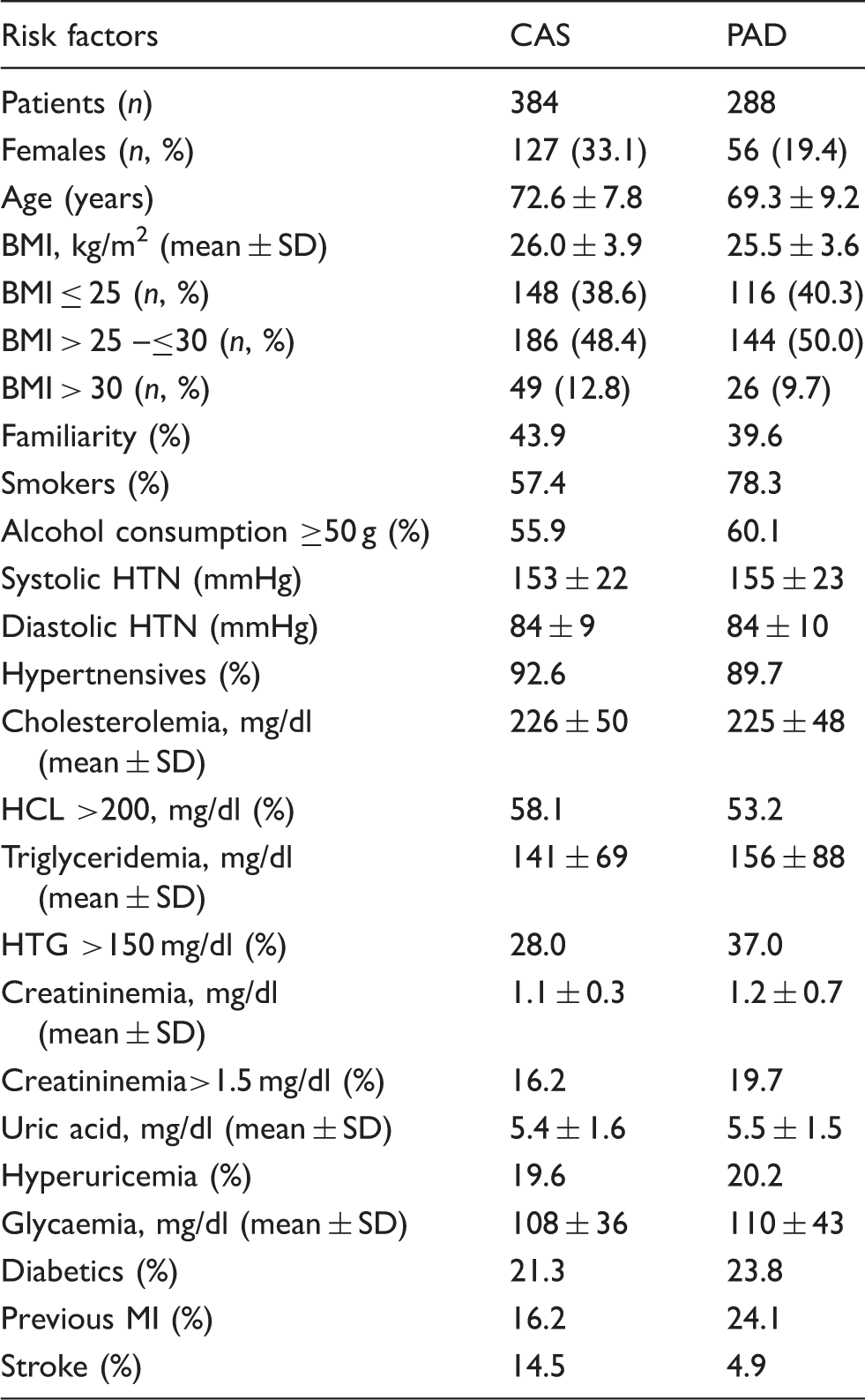
PAD: peripheral artery disease; CAS: carotid artery stenosis; BMI: body mass index; HTN: hypertension; HCL: hypercholesterolemia; HTG: hypertriglyceridemia; MI: myocardial infarction.
The data were expressed as a percentage with respect to the prevailing measurements and were statistically evaluated using the Chi-square and Student t tests. Some clinical variables were expressed as mean values and SDs, while the intergroup differences were considered significant at a p < 0.05 level. Statistical analysis was performed using SPSS (type 14.0).
Results
Clinical characteristics of the study population according to vascular disease.
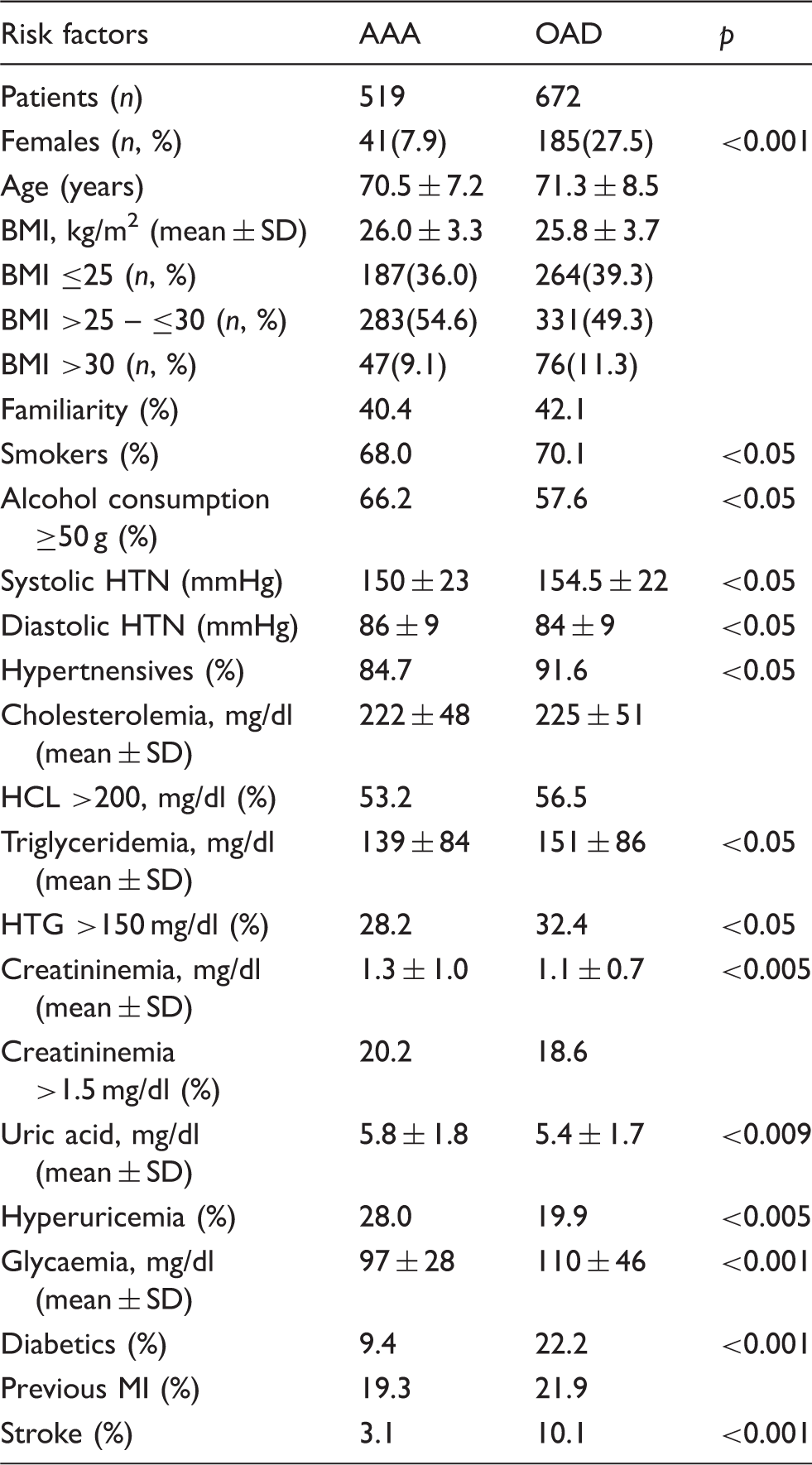
OAD: obstructive arterial disease; AAA: abdominal aortic aneurysm; BMI: body mass index; HTN: hypertension; HCL: hypercholesterolemia; HTG: hypertriglyceridemia; MI: myocardial infarction.
In the group of OADs, we found higher values of systolic BP, more hypertensives (p < 0.05 respectively). In addition, in the same group we observed elevated serum triglyceride levels, as well as more patients with hypertriglyceridemia (p < 0.05 respectively).
Discussion
This study demonstrates a close association between advanced age and the prevalence of occlusive and non-occlusive atherosclerotic arterial diseases. In fact, all participants had an average age of above 70 years. Thus, advanced age can be considered an essential risk factor for the development of arterial disease in different territories.
Atherosclerosis and vascular dysfunction increase with age because of decreased vascular compliance, angiogenesis and endothelial antithrombotic properties and increased inflammation due to vascular endothelial cell senescence. The prevalence of CAS and PAD increases dramatically with age following an exponential curve, while the prevalence of AAA is lower and increases linearly with age. 4
Males were widely present in both groups, especially in the group of AAAs. This fact confirms the notion that advanced age along with male gender are crucial risk factors for systemic atherosclerosis. 5 In addition, AAAs are less common in women than in men. 6
In every group, half of the patients were overweight and approximately 10% were obese. Central obesity is independently associated with AAA and appears to have the highest mortality risk in open surgery. 5 Also, abdominal obesity was independently associated with carotid wall thickening in middle-aged women and with occlusive PAD, independently of other concurrent cardiovascular risk factors.7,8
Smoking is actually considered the major environmental risk factor for atherosclerotic disease in the different vascular territories. The risk is strongly associated with AAAs and PAD and less associated with cerebrovascular diseases. 9 There is compelling evidence that nicotine alters the structural and functional characteristics of vascular smooth muscle and endothelial cells achieving a negative effect on flow-mediated, endothelium-dependent arterial vasodilatation.10,11 We confirm that smoking is a very strong risk factor for OADs and large AAAs. In fact, more than two-thirds of all vascular patients were active smokers or had recently stopped. Although smoking is an important cause of AAA development and progression, we identified more smokers in the group of OADs.
Alcohol appears to have a dose-dependent relationship to ischemic heart disease, whereby it is protective in moderate doses but harmful in large doses. 12 Conversely, there is conflicting evidence about the potential role of alcohol intake in the development and progression of AAA and PAD.12,13 There is now evidence that moderate alcohol consumption may reduce the hazard of AAA, PAD and stroke.13,14 The effect of higher doses of alcohol on the risk of arterial diseases still remains unknown. In our series, alcohol intake was tightly associated with AAAs. In fact, two-thirds of patients with AAA and more than half of those with OADs usually consumed alcoholic beverages, mainly wine, at least half a liter daily (50 g).
Family history is considered a remarkable risk factor for the development of AAA and OADs, suggesting that genetic factors play an important role in the pathogenesis of these distinct arterial diseases. 15 In this series, approximately more than one-third of vascular patients had a family history for the same condition.
We found a significant association between systolic hypertension and all artery diseases, especially with obstructive arteriopathies. It is presently unknown whether hypertension is a risk factor for AAA. Some studies suggest such a relation while others found no association. 16 However, there is evidence of an interesting association between AAA and diastolic hypertension.16,17 This fact was also confirmed by our results.
Aging is characterized by a chronic low-grade arterial wall inflammation, stiffness and an increase in BP. On the other hand, hypertension is also characterized by proinflammation in the arterial wall. 18 It is therefore clear that age related remodelling of the arterial wall provides fertile soil for the acceleration of atherogenesis. Hypertension and atherosclerosis may promote both the development, but especially the aneurysmal progression and expansion. 18
Besides the association between hypertension and AAA, we also confirm an association between hypercholesterolemia and AAA. However, the presence of hyperlipidemia in the AAA group, particularly of triglycerides, is less than that seen in the OAD group. Hypercholesterolemia facilitates inflammatory cell infiltration and increases the expression and secretion of proteolytic enzymes, such as metalloproteinases, that break down collagen, elastin and other matrix proteins, thereby facilitating aneurysm progression by weakening the extracellular matrix of the aortic wall. 19 On the other hand, several clinical studies have suggested that high triglyceride levels could become an independent risk factor for the early development of atherosclerosis. High triglyceride levels were also correlated with cardiovascular obstructive diseases. 10
The mean values of creatininemia and urea, as well as the number of hyperuricemic patients were significantly higher in the AAAs than in the OADs. It was found that creatinine levels rise progressively with age, especially after 60 years, along with a significant association between higher creatinine levels and the development of AAA. 20 The strong relationship between increased creatinine levels and AAAs could be due to a higher prevalence of atherosclerotic renal artery disease or to the involvement of the renal arteries from the adjacent aneurysmatic process of the aortic wall. This chronic decreased renal function, highly prevalent in AAA patients, affects their prognosis and mortality. Moreover, the presence of chronic kidney disease in patients with PAD also had a higher mortality rate.21,22 Uric acid has been formerly considered a major antioxidant in human plasma with possible beneficial anti-atherosclerotic effects. In contrast, increased levels of uric acid were found to be associated with AAAs and carotid plaques, even in the absence of other cardiovascular risk factors. 23 In fact, elevated uric acid increases platelet adhesiveness, mediates inflammation and stimulates smooth muscle cell proliferation. 23 Our findings are consistent with the above-described considerations.
Diabetes remains one of the major risk factors for atherosclerosis. In particular, it is closely associated with the more severe forms of occlusive atherosclerosis including coronary artery disease and peripheral arteriopathies. 24 Conversely, the relationship between diabetes and AAA appears unclear, ambiguous and surprisingly not so adverse. Moreover, the progression of AAA was shown to be slower in diabetics, suggesting a pathobiological mechanism through which the aortic media may be protected from aneurysmal degradation. 25
In fact, the pathobiology of AAA and obstructive atherosclerosis exhibits substantial histological differences. Occlusive atherosclerosis is characterized by an initial necrotic process in the intima and absence of arterial dilation. Conversely, AAA atherothrombosis involves the entire vascular wall exhibiting a necrotic process localized in the matrix-rich media, the presence of an intraluminal thrombus and the association with a significant adventitial reaction. 26 Our results confirm the strong association of diabetes with the OADs, as well as the weak association with the large AAAs. Finally, a decent number of all vascular patients (about one-fifth of each group) had had a previous myocardial infarction, without differences between the groups.
Conclusions
We remark a strong negative association of diabetes and female gender with large AAA. In addition, the positive association of AAA with male gender, diastolic hypertension, serum creatinine, serum uric acid and alcohol consumption is confirmed. Although the number of smokers and hypertensives was significantly larger in both groups, a greater number of smokers and hypertensives were observed among patients with occlusive atherosclerotic vasculopathies. In the same group, we observed more patients with systolic hypertension, as well as patients with hypertriglyceridemia. The significant presence of smoking, obesity, hypertension and hypercholesterolemia observed in an almost similar way, in both giant AAAs and obstructive atherosclerosis, suggests that these risk factors might be involved in the pathogenesis of the occlusive atherosclerosis and, perhaps, engaged in the aneurysmal development and expanding process.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.