
Abstract
Aim
Peripheral arterial disease is frequently associated with significant atherosclerosis of other vascular beds. The aim of the present study was to investigate a possible association between peripheral arterial disease segment-specific disease burden and cerebrovascular disease.
Methods
Two-hundred and twenty-six patients with clinically symptomatic peripheral arterial disease from the prospective PureASO registry were followed up after revascularization. The breadth of peripheral arterial disease was quantified at the time patients entered the study. The segment-specific peripheral arterial disease burden was correlated to cerebrovascular disease and imaging findings during a five-year follow-up.
Results
At five years, cerebrovascular disease-free survival after lower limb revascularization was 31%. Patients with peripheral arterial disease involving the crural arteries had significantly more ischemic degenerative changes at brain imaging (p = 0.031), whereas patients with aorto-iliac and femoropopliteal segment peripheral arterial disease had more significant (>50% uni- or bilaterally) internal carotid artery stenosis compared to patients with crural peripheral arterial disease (p = 0.006). According to Cox regression analyses, crural arteries burden was associated with a significantly increased risk of mortality (adjusted HR 2.07, CI 95% 1.12–3.28, p = 0.021) and cerebrovascular events (adjusted HR 1.97, CI 95% 1.19–3.26, p = 0.008).
Conclusions
Present results suggest that atherosclerosis burden at different lower limb artery segments is associated with defined cerebrovascular disease. This further suggests that risk factors and pathophysiological mechanisms are congruent across particular vascular beds.
Introduction
Lower extremity arterial disease (peripheral arterial disease (PAD)) is associated with decreased survival and increased resource use.1,2 In particular, chronic limb-threatening ischemia (CLTI) is the most severe clinical presentation of PAD and markedly increases the risk of limb loss and cardiovascular events.3–5 Currently, an estimated 200 million people worldwide are affected by PAD with its prevalence constantly increasing, not solely due to longer life expectancy but also due to manifestation of the disease at a younger age.1,6–8
Atherosclerotic vascular disease overlaps in many patients on all three major vascular territories, i.e. cardiac, cerebrovascular and peripheral arteries.9–11 PAD has been shown to increase the risk of carotid artery stenosis (CAS) and stroke.12,13 In addition, the risk of myocardial infarction and cardiovascular death is strongly associated with decreased ankle brachial index (ABI < 0.9).14,15 Therefore, the early detection of PAD and initiation of optimal medical treatment are becoming increasingly important in preventing further cardiovascular events among these patients. 5
Although atherosclerosis burden on different lower limb vascular beads is known to be overlapping,16–18 the possible association between localization of peripheral vascular disease burden and that of cerebrovascular disease has not been thoroughly investigated.
The aim of the present study was to evaluate a possible association between localization of lower limb PAD burden and cerebrovascular disease. The PAD burden at defined lower limb artery segments was analysed according to our recent classification.19,20
Methods
Study population
The present study is part of the prospective PureASO registry, 21 which included a consecutive series of patients from the Turku University Hospital catchment area admitted to the Vascular Department for lower limb endovascular or surgical revascularization. During the enrolment period, 25 November 2013 to 6 January 2014, 227 patients undergoing elective or urgent revascularization for PAD were screened and 226 patients gave their written informed consent to participate the study. A complete medical history including the patient’s cardiovascular risk factors were collected from each patient. This study was approved by the Ethics Committee of the South-western Hospital District of Finland (desition numbers; T75/2011 and TO3/017/15).
Classification of disease burden
Digital subtraction angiography (DSA) images of all patients were scrutinized, and the burden of PAD was graded according to the classification proposed by Jalkanen et al. 19 In brief, the burden of atherosclerosis involving crural arteries was graded by analysing the atherosclerotic lesions at each of the three vessels as follows: 0: no detectable occlusion or minor stenosis; 1: total occlusion less than 5 cm; 2: total occlusion less than 10 cm; 3: total occlusion less than 15 cm; 4: total occlusion longer than 15 cm. The Crural Index was calculated by summing the scores of each crural vessel and stratified as follows: Crural Index 0: 0; Crural Index I: 1–3; Crural Index II: 4–6; Crural Index III: 7–9; Crural Index IV: 10–12. Aorto-iliac and femoropopliteal segments were classified according to the TASC II criteria.17,18 Categorical variables for aorto-iliac and femoropopliteal segments (TASC II classification A–D) were graded as follows: no disease: 0; TASC II A: 1; TASC II B: 2; TASC II C: 3; TASC II D: 4.
In order to assess the prognostic effects of lesion distribution in different arterial segments, each patient was assigned into a group of predominant disease localisation: (1) aorto-iliac, (2) femoropopliteal and (3) crural, based on which four points gave the highest score. 19 If even score was detected, the patient was assigned to the more proximal segment.
Cranial imaging
All clinical cerebrovascular events leading to diagnostic brain imaging after a patient was entered into the PureASO registry were reviewed. Images were evaluated and graded by a neuroradiologist as: cerebellar-, cerebral infarction, ischemic vascular degeneration, spontaneous subdural haematoma and spontaneous subarachnoid haematoma. The presence and severity of any stenosis of the cerebral arteries were recorded. A stenosis of a cerebral artery was considered significant when >50%. The etiology of cardioembolic stroke was based on electrocardiographic and echocardiographic findings.
Statistical analysis
Statistical analysis was performed using an SPSS v. 24.0 statistical software (IBM Corporation, New York, USA). Nominal variables are reported as counts and percentage and continuous variables as mean and standard deviation. Nominal variables were compared using the Fisher’s exact test. For continuous variables, a Shapiro-Wilk test was run to test the normality of the variables. If normally distributed, continuous variables were then compared with ANOVA test. Continuous variables not normally distributed were compared with the Kruskal-Wallis non-parametric test. Only cerebrovascular events that occurred after patient had entered into the PureASO registry were considered for survival analyses. Kaplan-Meier method was used for estimation of survival analyses, and the survival between defined PAD burden groups was compared with Wilcoxon statistics. A Cox regression analysis was performed to adjust the burden of PAD on the outcomes for other comorbidities (CAD, AF, COPD, hypertension, diabetes, dyslipidaemia, renal insufficiency and smoking history). Factors with a p <0.2 in Cox proportional hazard univariate analysis were included into the regression models. p < 0.05 was considered as a threshold for statistical significance.
Results
Patient population
The mean age of the study cohort was 71.3 ± 12.0 years. Smoking years, hypertension, diabetes, renal insufficiency and smoking history differed significantly across different lower limb vascular beds (Table 1).
Demographic data.

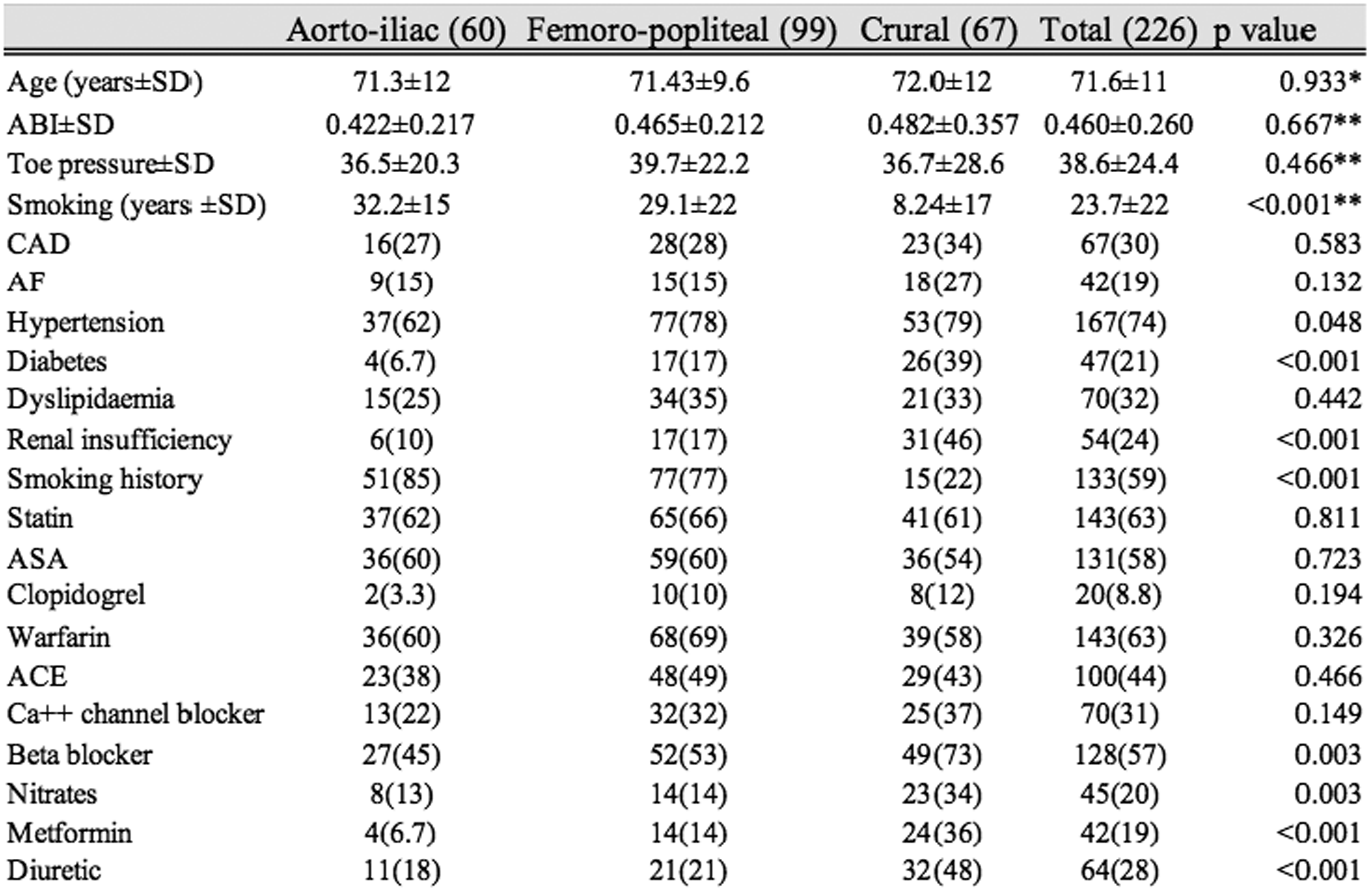
Note: The nominal variables are reported as counts and percentages and continuous variables as mean ± standard deviation.
CAD: coronary artery disease; AF: atrial fibrillation. Nominal variables were compared using the Fisher’s exact test. For continuous variables, a Shapiro-Wilk test was run to test the normality of the variables. If normally distributed, continuous variables were then compared with ANOVA test. Continuous variables not normally distributed were compared with the Kruskal-Wallis non-parametric test.
Brain imaging
During a mean follow-up of 54 ± 70 months, 131 patients (58%) had cerebrovascular symptoms indicating brain imaging. The imaging detected following findings: cerebellar infarction (8 patients), cerebral infarction (43 patients), vascular degeneration (64 patients), spontaneous subdural hematoma (5 patients), spontaneous subarachnoid hematoma (3 patients). Some patients had up to three findings and some patients such as transient ischemic attack patients had none. Fisher’s exact test showed significant difference in the ischemic vascular degeneration across PAD burdens (p < 0.031) (Table 2).
Results of brain imaging in the PureASO registry.
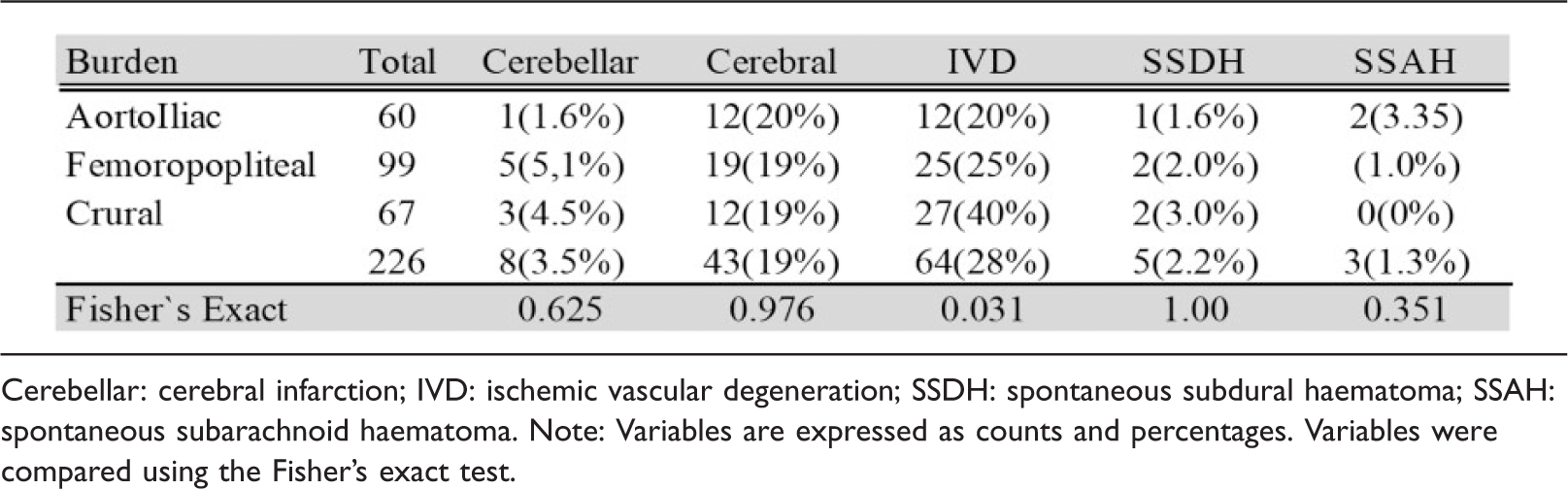

Cerebellar: cerebral infarction; IVD: ischemic vascular degeneration; SSDH: spontaneous subdural haematoma; SSAH: spontaneous subarachnoid haematoma. Note: Variables are expressed as counts and percentages. Variables were compared using the Fisher’s exact test.
Association between PAD burden and cerebrovascular disease
The PAD was most severe in the aorto-iliac segment in 25.2%, femoropopliteal in 43.8% and in crural segment in 29.2% of patients. The burden of PAD involving the femoropopliteal was significantly associated with internal carotid artery stenosis (p < 0.006) (Table 3).
Subjects with stenosis of over 50% in the affected artery.
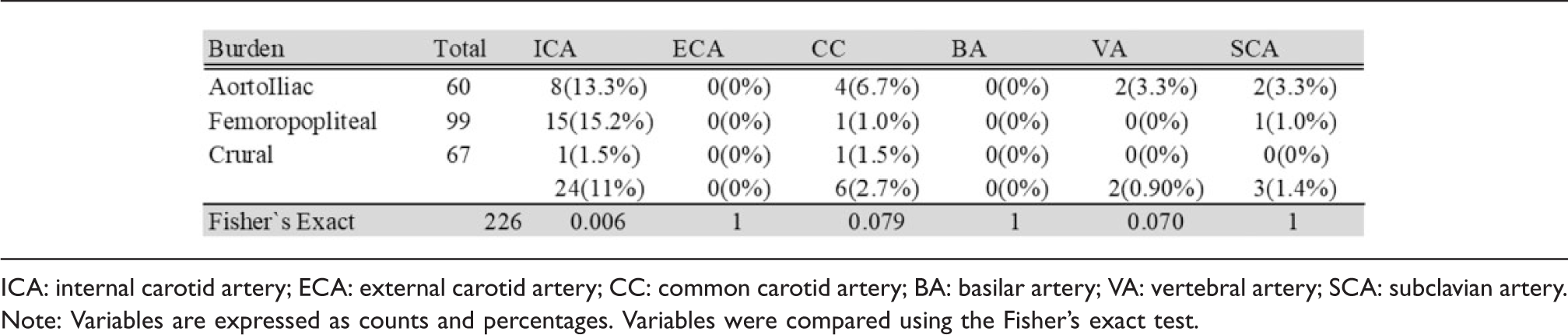

ICA: internal carotid artery; ECA: external carotid artery; CC: common carotid artery; BA: basilar artery; VA: vertebral artery; SCA: subclavian artery. Note: Variables are expressed as counts and percentages. Variables were compared using the Fisher’s exact test.
Survival and cerebrovascular event-free survival
Overall survival of patients with PAD of the aorto-iliac segment was 90% (20 months), 82% (40 months) and 65% (60 months), for the femoropopliteal segment was 89%, 82% and 48% and for the crural segment were 67%, 59% and 32%. The mean estimated survival of patients with crural PAD was shorter than those with aorto-iliac (p < 0.001) and femoropopliteal (p = 0.001) PAD. The cerebrovascular survival according to PAD burden was: aorto-iliac segment 73%, 57% and 40%, femoropopliteal segment 75%, 59% and 33% and crural segment 46%, 39% and 18% 20, 40 and 60 months correspondingly. The mean estimated survival on crural segment was significantly shorter compared to aorto-iliac (p = 0.001) and femoropopliteal (p = 0.001) segments (Figure 1(a) and (b)).
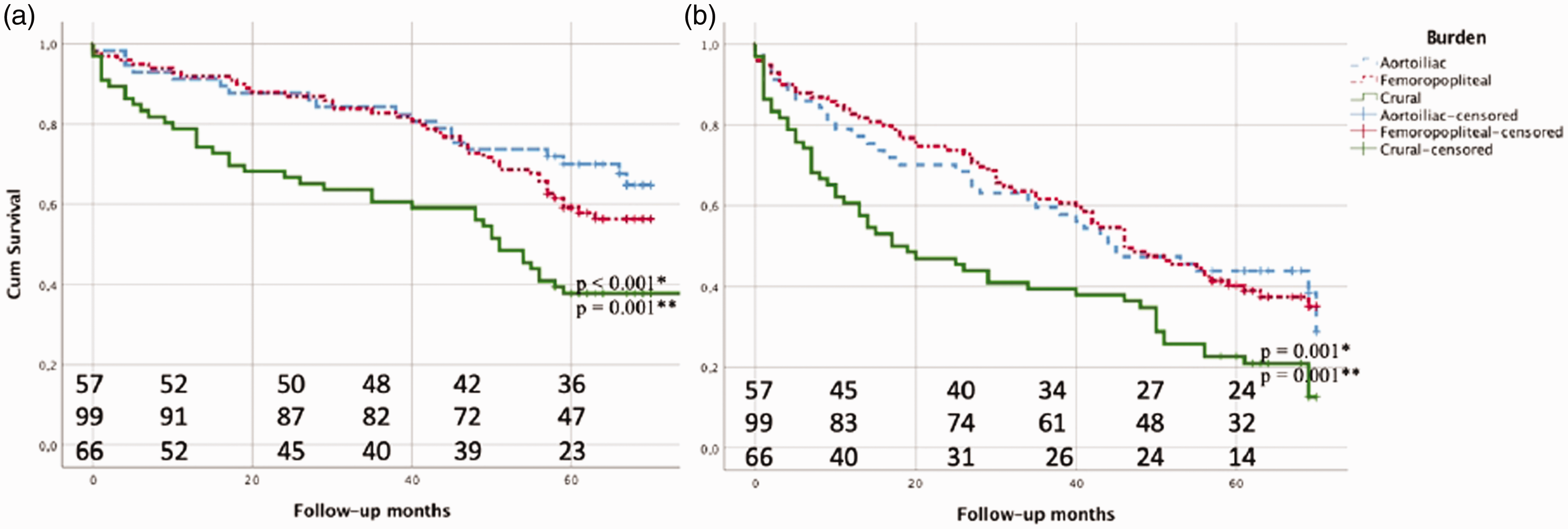
Kaplan-Meier estimates of all-cause mortality (a) and cerebrovascular event-free survival (b) according to the localization of PAD.
Cox regression models including coronary artery disease, atrial fibrillation, hypertension, chronic obstructive pulmonary disease and smoking history showed that crural PAD was an independent predictor of late mortality (adjusted HR 2.07, CI 95% 1.12–3.28, p = 0.021) and cerebrovascular events (adjusted HR 1.97, CI 95% 1.19–3.26, p = 0.008) (Table 4).
Results of Cox regression analyses. The confounding variables were CAD, AF, HT, COPD and history of smoking.

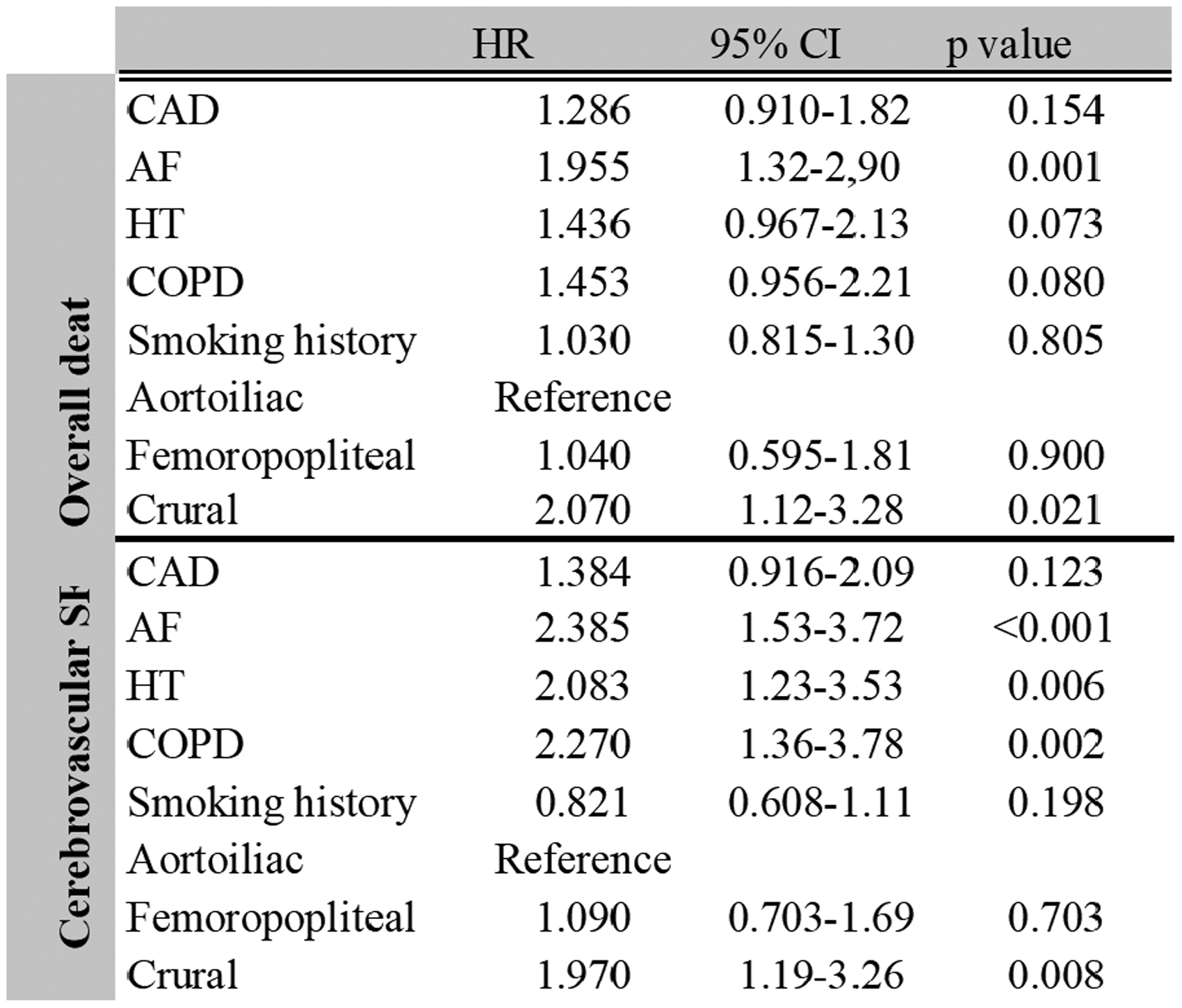
CAD: coronary artery disease; AF: atrial fibrillation; HT: hypertension; COPD: chronic obstructive pulmonary disease.
Discussion
This study showed that 68% of patients with the crural PAD burden died during five years’ follow-up. Among the remaining survivors (32%), cerebrovascular symptoms were frequent (44%). Based on our earlier studies, crural PAD is associated with increased risk of mortality and amputation.19,20 The present study indicates that this cohort of patients presents also an increased risk of cerebrovascular disease.
ABI is an indicator of atherosclerosis disease severity5,17,18 and in turn ABI <0.80 is associated with cardiovascular events and atherosclerosis of large cerebral vessels. 22 The present cohort consists of clinically symptomatic PAD high-risk patients with low ABI and toe pressure (Table 1). As suggested by earlier investigations, the cerebrovascular disease among these patients is frequent. Interestingly, the disease burden of defined lower limb arterial segments associates with the occurrence of defined cerebrovascular disease. Patients with most extensive atherosclerosis on either the aorto-iliac segment or femoropopliteal segment have significantly more ICA stenosis compared to patients with high burden of PAD involving the crural segment. Both aorto-iliac and femoropopliteal disease are associated with identical risk factors like smoking16,23 Recently, an association between defined cardiovascular risk factors and cytokine levels was demonstrated on PAD patients. 24 Taken together these observations support similarities in pathophysiological mechanisms leading to atherosclerosis of aorto-iliac artery segment, femoropopliteal artery segment and internal carotid artery are concurrent. Based on present results, crural atherosclerosis is not associated with atherosclerosis of large cerebral vessels further supporting different pathophysiological etiology of crural disease compared to lower limb and cerebrovascular large vessel disease.
Although PAD and AF are associated, the relation between PAD and stroke seems not to be solely mediated by AF.12,25 Earlier studies have demonstrated that both are independently associated with stroke, cardiac failure hospitalization and cardiovascular death.12,25 In the present study, the cerebrovascular events were analysed as an clinical outcome. Only 20% of the patients had AF, whereas 59% had cerebrovascular disease requiring brain imaging. Based on our present data, AF is not the only significant cause of cerebrovascular disease among PAD patients. Still according to multivariable analyses, AF is a significant risk factor for both overall death and cerebrovascular symptom-free survival. Therefore, AF cannot be ignored as a significant factor affecting PAD patient outcome.
Lower limb artery disease is associated with cerebral white matter lesions. 26 Additionally, carotid artery intimal thickening is related to peripheral artery disease.27,28 In the PureASO registry, 28% (64) of ischemic degenerative cerebral changes were frequent at brain imaging, and of all cerebral symptoms on the present cohort, 32% were considered originating from small arteries. Based on present data, the small vessel lower limb atherosclerosis, namely tibial artery disease, is associated with ischemic degenerative cerebral vascular disease.
Major vessel disease as significant >50% carotid artery stenosis either uni- or bilateral was present in 11% of cases. Interestingly, carotid artery stenosis was associated with large lower limb artery disease at femoropopliteal and aorto-iliac segment and not with crural vessel disease. These observations suggest that there is association between defined cerebral vascular disease and the burden of PAD at defined arterial segments. It remains an interesting target for further studies to understand the molecular pathology behind the similarities of atherosclerosis at these two different vascular beds. Patients with severe PAD also present high burden of cerebrovascular disease and require best medical treatment available for atherosclerosis.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HH is a consultant at Bayer Oy.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by an EVO grant, Turku University Hospital.