
Abstract
Objective
To evaluate the endovascular repair of the transplanted renal artery anastomotic pseudoaneurysm using the snorkel technique.
Methods
From April 2012 to December 2017, we performed endovascular repair in six patients, who were diagnosed with transplanted renal artery anastomotic pseudoaneurysm, using the snorkel technique. The “snorkel” stent and the “parallel” stent were placed in the transplanted kidney and the external iliac artery, respectively. Another covered stent was implanted at the proximal end of the external iliac artery to match the diameter of the iliac artery.
Introduction
Renal artery pseudoaneurysms following renal transplantation are rare but can cause severe complications, such as renal allograft loss or even death. The treatment methods reported in the literatures include open surgical repair, endovascular repair, and ultrasound-guided percutaneous thrombin injection.1,2 No matter which method is used, most patients had to undergo transplant nephrectomy after endovascular repair because of the dysfunction of the transplanted kidney.
We first reported the successful treatment of a patient with transplanted renal artery anastomotic pseudoaneurysm using the snorkel technique in April 2012. 3
In this case, we used cover stents to block pseudoaneurysm and to successfully preserve the transplanted kidney. As of December 2017, we have treated six patients with this technique. In this article, we provide a review of these patients to evaluate the advantages and disadvantages of this technique.
Methods
Patients
Between April 2012 and December 2017, six patients were diagnosed with transplanted renal artery anastomotic pseudoaneurysm in our hospital. All patients underwent allograft renal transplantation: five from related donors and one from a deceased donor. All patients had been treated at the same kidney transplant center and undergone the same procedure: the transplanted kidney was implanted in the iliac fossa, and end-to-side anastomosis was used for the transplanted renal artery and the external iliac artery. The time from transplantation to the diagnosis of pseudoaneurysm was 75 ± 54 days. Three asymptomatic patients (case nos. 1, 2, and 4) were diagnosed by routine postoperative review, and two (case nos. 5 and 6) were diagnosed through symptoms of fever, pain in the waist and abdomen, and oliguria. In the most serious case (case no. 3), the patient suffered from sudden lower-right quadrant pain with shock. All patients were diagnosed by ultrasonography, and five patients (except case no. 3) were further assessed by computed tomography angiography. In five patients (except case no. 3) three blood cultures were done before surgery. Because of the emergency operation, case no. 3 did not have a blood culture before surgery. Ten days after the operation, she developed fever, abdominal pain, and anuria and was advised blood culture tests. Escherichia coli was found in case no. 3 and Staphylococcus aureus was found in case no. 6 , and the blood culture of the rest of the cases was negative. All patients’ demographics are presented in Table 1.
Patients’ demographics.

TKF: Transplanted kidney function.
Procedure
All patients’ treatment plans were approved by the hospital ethics committee. All patients were treated with the snorkel technique to repair the anastomotic pseudoaneurysm with covered stents. One patient (case no. 3) underwent emergency surgery for hemorrhagic shock due to pseudoaneurysm rupture, and the other five patients underwent an elective procedure.
In the first patient, FLUENCY stents (Bard Peripheral Vascular, Inc., Tempe, Arizona) were used, and in the remaining five patients, VIABAHN stents (GORE, Inc., Flagstaff, Arizona) were used. A sheath was inserted in the contralateral femoral artery. A 5F VER catheter (Johnson & Johnson Cordis Corporation, Miami, FL) crossed over the bifurcation of abdominal aorta and was placed on the common iliac artery for angiography. In all patients, a longitudinal incision in the groin on the side of the transplanted kidney was used to expose the common femoral artery, followed by the retrograde implantation of two sheaths. A guidewire was inserted into the external iliac artery to implant the “parallel” stent and into the transplanted renal artery to implant the “snorkel” stent. To match the diameter of the iliac artery and avoid type I endoleak, another covered stent was implanted at the proximal end of the external iliac artery. The specific surgical procedure has previously been described in detail. 1
Follow-up
All patients were treated with aspirin + clopidogrel for three months, and long-term oral antibiotics were administered to patients with a prominent infection. Patients who survived kidney transplantation underwent review of color ultrasounds and renal function tests every 3–6 months.
Results
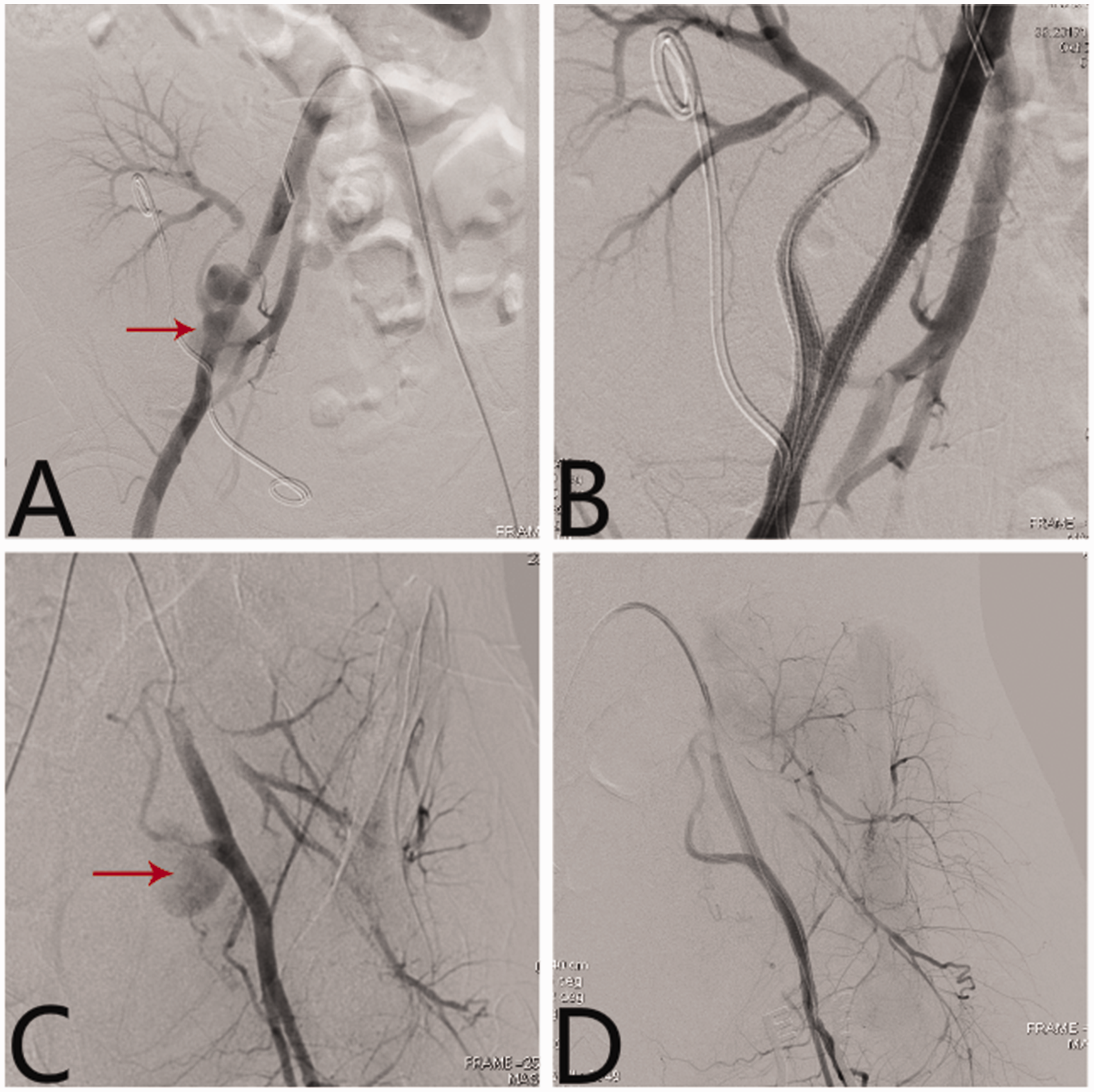
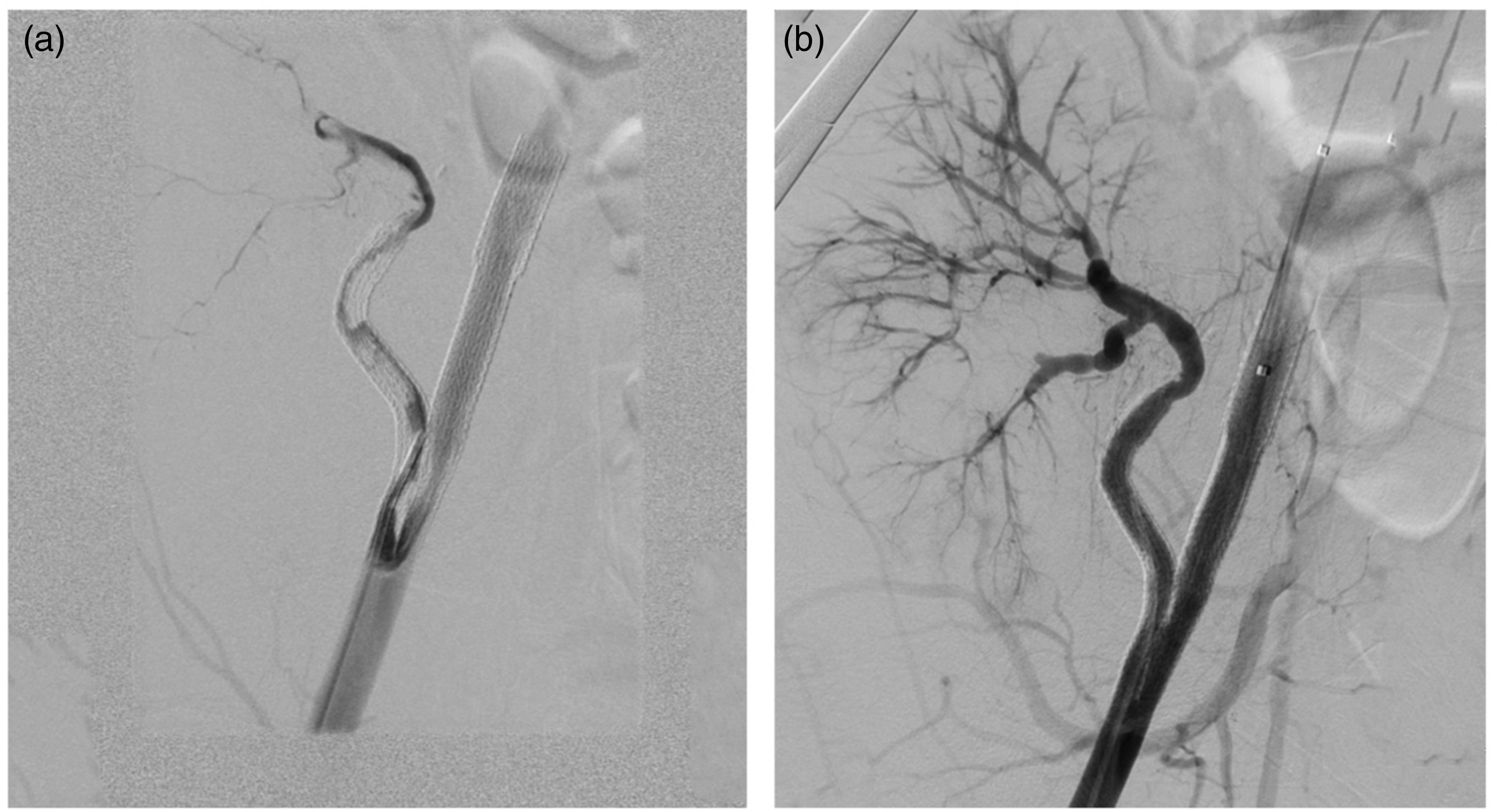
All patients underwent surgery successfully. There were no instances of immediate death, arterial rupture, endoleak, lower extremity arterial embolization, or renal artery occlusion (Figures 1 and 2). However, over the long term, the transplanted kidney functioned well in three patients (case nos. 1, 2, and 4) and was not functioning in the other three patients (case nos. 3, 5, and 6).

(a) and (b): Case no. 2 before and after stent implantation, red arrow indicates the location of the pseudoaneurysm. (c) and (d) Case no. 3 before and after stent implantation, red arrow is the location of the pseudoaneurysm.
(a) and (b): Case no. 4 before and after stent implantation, red arrow indicates the location of the pseudoaneurysm. (c) and (d): Case no. 6 before and after stent implantation, red arrow indicates the location of the pseudoaneurysm.
Three patients were followed up for more than two years with ultrasound examinations. The transplanted renal artery blood supply was good, the kidney function was normal, and there were no acute or chronic symptoms of ischemia in the lower extremities. One patient (case no. 5) developed stent thrombosis and renal failure four months after the surgery. Although the trunk and branches of the renal artery were restored through thrombolysis, the transplanted kidney was not rescued due to the extensive obstruction of small blood vessels in the renal parenchyma (Figure 3). Nephrectomy was subsequently performed. The stents were removed, and the iliac artery was repaired during the operation. One patient (case no. 6) presented with recurrent fever, abdominal pain, and oliguria three weeks after the operation. Emergency nephrectomy, stent removal, ligation of the right external iliac artery, and autologous saphenous vein bypass of the left and right femoral arteries were performed. One patient (case no. 3) developed fever, abdominal pain, and anuria 10 days after the operation. Therefore, emergency nephrectomy was performed. Because of the poor general condition of the patient, the iliac artery stent was not removed, and the right inguinal incision healed poorly. After three months, the stent was removed (Figure 4), and the iliac artery was reconstructed with an autologous saphenous vein.
(a) Stent and renal artery thrombosis. (b) After thrombolysis, the stent and the main artery of the transplanted kidney were restored. DSA shows that the contrast agent was obviously retained, suggesting that the outflow obstruction and the renal parenchyma still have thrombus.

The stent (VIABAHN) is discharged from the inguinal incision.
Discussion
Transplanted renal artery anastomotic pseudoaneurysm is a rare but serious complication after renal transplantation that often leads to the loss of function of the transplanted kidney or even death of the patient. 4 The etiology of anastomotic pseudoaneurysms may be a faulty suture technique, arterial wall injury, infection, or immunological factors.5,6 Due to the low incidence rate, most of the studies in the literature on this topic consist of case reports. Some researchers have proposed that the indications for the repair of symptomatic pseudoaneurysms are a pseudoaneurysm size greater than 2.5 cm, significant growth, or a pseudoaneurysm confirmed to be caused by infection.1,7
Because of the deep anastomotic site and the occlusion of transplanted kidneys, open surgery can easily injure the kidney, and allografts are lost in many cases. 8 The main methods for endovascular treatment include coils, covered stents, and embolic agents.2,9 However, due to the complex anatomical relationship of the local blood vessels, successful occlusion of the aneurysm and preservation of the function of the transplanted kidney are difficult. In 2014, we first reported the use of “snorkel” technology for endovascular repair. 3 The patient was followed up for more than two years, and the renal artery blood supply and function were good. From March 2012 to December 2017, five other patients at our hospital were identified and treated with this method.
Technical advantages
Less trauma and easy operation. The femoral artery is exposed through a lateral inguinal incision in the transplanted kidney. The retrograde operation complies with the angle of anastomosis, so the guide wire can be implanted into the transplanted renal artery very quickly, allowing the operation to be completed quickly. No complicated techniques are required. Sealing the anastomotic pseudoaneurysm while conserving the blood supply of the transplanted renal artery avoids the occurrence of early graft loss. Because two kissing stents (the snorkel stent in the transplant renal artery and the stent in the external iliac artery) need to be implanted in the external iliac artery, the caliber of the stent must be selected appropriately. VIABAHN stents with a diameter of 5 mm or 6 mm and a length of 50 mm are usually selected for the transplanted renal artery. Usually, the kissing stent is the same as the snorkel stent. The “anchorage zone” of the stent in the transplanted renal artery and the external iliac artery should be at least 2 cm, which means that a 50-mm-long snorkel stent should be released at the center of the anastomosis. The third stent is implanted in the proximal external iliac artery, with partial overlap with the kissing stent, to avoid type I endoleak; this overlap is usually more than 20% of the diameter of the external iliac artery.
The following points should be considered during the operation:
Defects of the technique
Because of the change in the blood flow in the transplanted renal artery, there is the possibility of ischemia and loss of function of the transplanted renal artery. The technique is still inappropriate for the treatment of pseudoaneurysms caused by infection or immune factors. In two cases of infected pseudoaneurysms, although the operation was successful and sensitive antibiotics were used according to the bacterial culture, anastomotic rupture and hemorrhage occurred after the operation. The stents were removed, and an autologous saphenous vein was used for reconstruction. The transplanted kidney was removed at the same time.
The transplanted renal artery anastomotic pseudoaneurysm, once it occurs, whatever the reason, whether open or endo, has a low success rate. In our group, half of patients successfully preserved the function of transplanted kidneys. Stent thrombosis and vascular rupture after stent infection are the causes of renal allograft loss in our group. Regardless of the cases in our article or in the literatures, all the anastomotic pseudoaneurysms caused by infection ultimately underwent a nephrectomy, and some even died. So we provide a new approach to the treatment of this disease, which is however applicable to only some cases of pseudoaneurysms. Individualized treatment plans are necessary for the appropriate management of the transplanted renal artery anastomotic pseudoaneurysms.
If the pseudoaneurysm is not caused by infection or immune factors, the anatomy of the transplanted renal artery is similar to what we have described, and our technique can be attempted. Any interventional procedure may eventually fail if infection exists. Open surgery, removal of the transplanted kidney, and repair of the iliac artery may be the best choices. However, if anastomotic pseudoaneurysm rupture occurs, the patient’s general condition is too poor to tolerate the trauma of open surgery. Our technique might be an appropriate choice to block the pseudoaneurysm rupture quickly and preserve the function of the transplanted kidney to the greatest extent, thus providing valuable time for follow-up treatment.
Conclusions
In summary, the endovascular treatment of transplanted renal artery anastomotic pseudoaneurysms with the snorkel technique is a feasible method but needs to comply with certain indications.
Limitations of the study
Notably, our study is limited by its retrospective nature, small patient population, and lack of standardized follow-up imaging. Rare and unpredictable publications limit the study of this disease, and it is difficult to evaluate treatment effects from a statistical perspective.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.