
Abstract
A 63-year-old woman presented with a symptomatic aneurysm and a pelvic transplant kidney on the side of an external iliac artery occlusion. A commercially available bifurcated endograft was introduced through the common iliac artery contralateral to the kidney. The external iliac artery occlusion required antegrade delivery of an iliac limb through the contralateral endograft gate and cannulation of the common iliac artery to allow for deployment proximal to the transplant kidney artery. This technique was successful and remains so six months postoperatively. Endovascular repair of aneurysms proximal to pelvic transplant kidneys remains the preferred method of repair. However, inadequate access vessels may require antegrade delivery of endograft components which is facilitated by advances in endograft design.
Introduction
The coexistence of a pelvic transplant kidney and an abdominal aortic aneurysm (AAA) offers a unique therapeutic challenge. Many surgeons would now recommend an endovascular repair of the aneurysm in this situation. This prevents the often prolonged transplant kidney ischemia that results from an open approach where, by definition, clamping is suprarenal. 1 However, standard transfemoral delivery of endografts requires adequate iliac artery access or, in its absence, an alternative delivery approach. Carotid and subclavian artery approaches have been previously described in other clinical situations. 2,3
In the following case report, we describe the successful endovascular repair of an AAA with a coexisting pelvic transplant kidney and an occluded ipsilateral external iliac artery. By delivering the contralateral iliac limb of a bifurcated endograft via the left subclavian artery, the advantages of an endovascular approach, namely minimal renal ischemia, were maintained.
Case report
A 63-year-old woman presented with a several-day history of non-specific lower back pain, not associated with any hemodynamic instability. Relevant medical history included a previous coronary artery bypass graft and a left pelvic transplant kidney that had been functioning well for 20 years. She also described bilateral moderate distance thigh claudication (Rutherford Class II). Physical examination revealed a hemodynamically stable patient with a mildly tender pulsatile abdominal mass and a faint right femoral pulse with no left femoral pulse. There were no signs of acute lower-extremity ischemia.
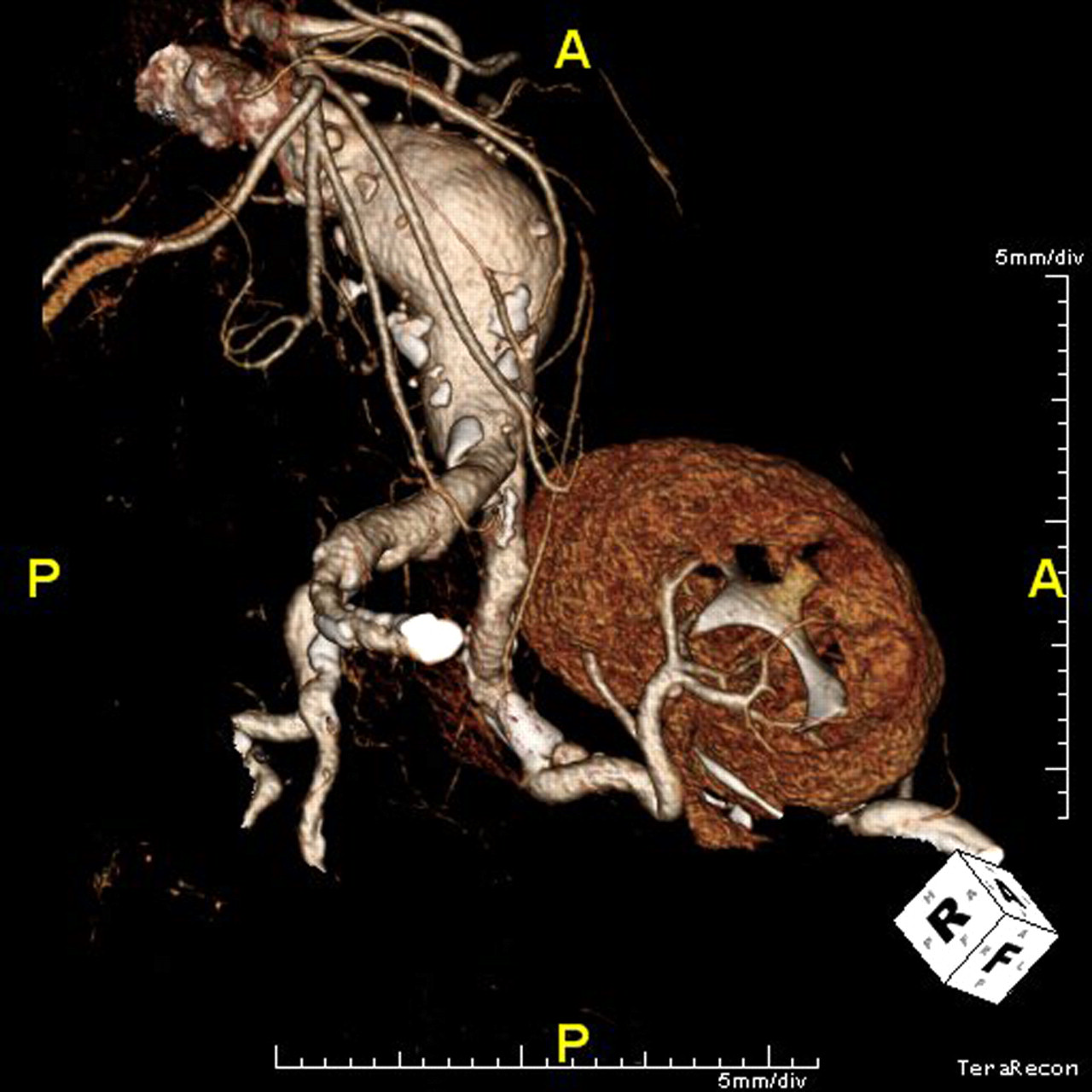
A computed tomography (CT) scan was performed which revealed a 6 cm AAA originating at her occluded renal arteries (Figure 1). Her right external iliac artery was patent, but of small caliber and diffusely diseased, and her left external iliac artery was occluded (Figure 2). Her left pelvic transplant kidney was well perfused with its arterial supply originating from the left internal iliac artery. There was no evidence of rupture, but with her persistent symptoms, and no other explanation for them, she was taken to the operating room for endovascular repair of her symptomatic AAA.
Three-dimensional reconstruction of a preoperative computed tomography scan showing a 6 cm abdominal aortic aneurysm with left pelvic transplant kidney Preoperative computed tomography scan showing pelvic transplant kidney with arterial supply originating from the left internal iliac artery, and an occluded left external iliac artery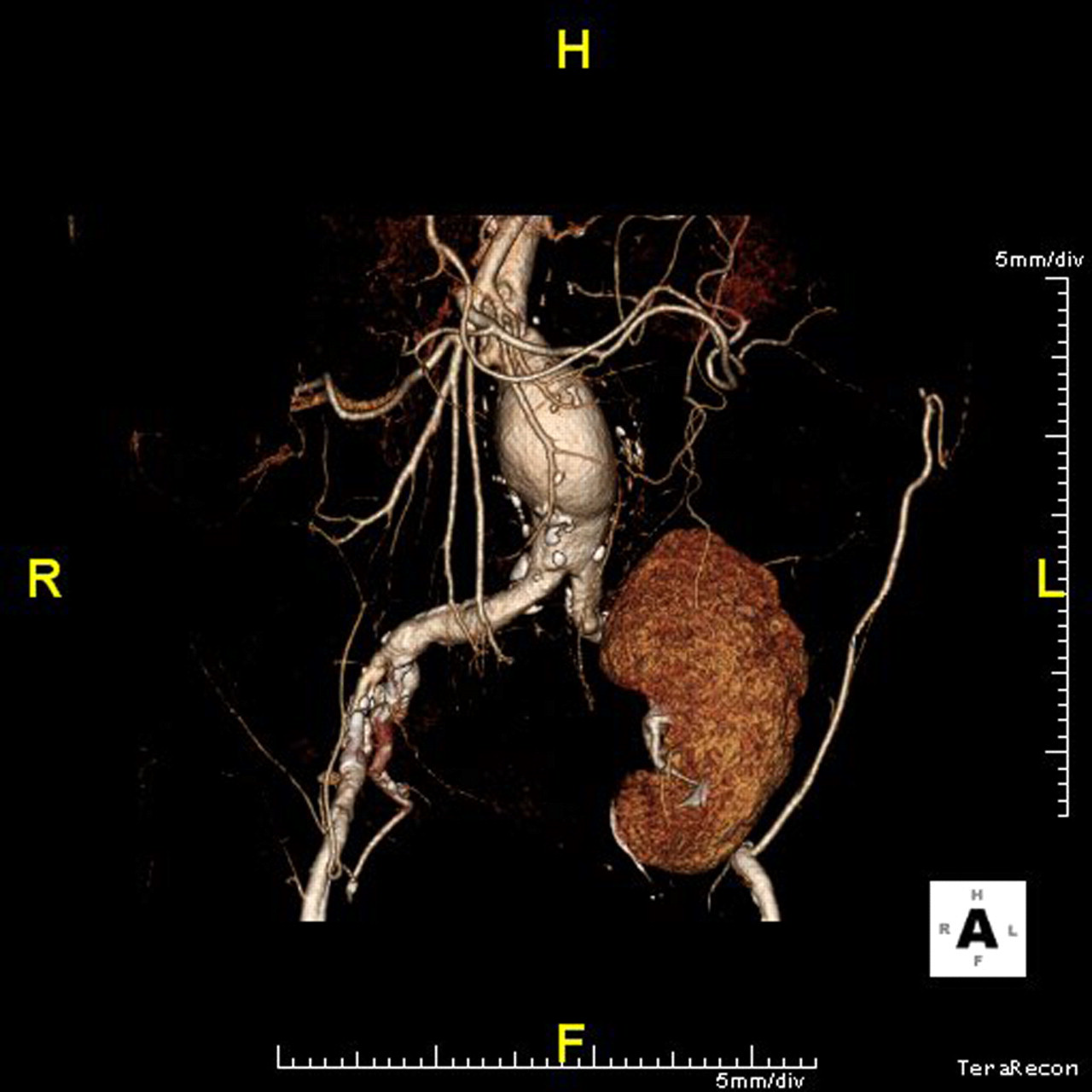
The procedure was performed under general anesthesia and with a portable C-arm fluoroscope. An oblique right lower quadrant muscle splitting incision was made and the right common iliac artery was exposed through a retroperitoneal approach. A 10 mm diameter Dacron conduit was sewn end-to-side to the right common iliac artery to allow for delivery of the main body and ipsilateral limb of a bifurcated endograft. The left subclavian artery was exposed via a transverse infraclavicular incision and another 10 mm diameter Dacron conduit was sewn end-to-side to this artery. Preoperative intravenous hydration and N-acetyl cysteine were used as renal protective strategies.
A pigtail angiographic catheter was introduced through the subclavian artery conduit into the visceral aortic segment. The main body of a bifurcated 28 mm proximal diameter Endurant endograft (Medtronic, Santa Rosa, CA, USA) was introduced via the right common iliac artery conduit and deployed with the fabric just below the superior mesenteric artery, across the origins of the occluded renal arteries. An ipsilateral iliac extension was placed via the same conduit. The contralateral gate of the bifurcated graft was then cannulated from above from the left subclavian artery conduit (Figure 3). The origin of the left common iliac artery was then cannulated and an angled catheter was carefully introduced into the left internal iliac artery, followed by a Lunderquist stiff wire (Cook Medical, Bloomington, IN, USA). An 80 mm long (13 mm diameter proximally and distally) Endurant iliac extension was then introduced via the subclavian conduit and the Lunderquist wire with careful positioning of the delivery system's proximal cap into the left internal iliac artery. This limb was deployed with the distal markers in the common iliac artery proximal to the internal iliac artery. A 16 × 16 × 80 limb was then introduced from above to bridge the short gap between this distally placed limb and the contralateral gate. All attachment sites and overlap zones were then molded with a Reliant balloon (Medtronic). At the completion of the procedure, the conduit on the right common iliac artery was tunneled to the common femoral artery as an ileofemoral bypass.
Intraoperative angiogram showing cannulation of the bifurcated graft's contralateral gate and the left common iliac artery
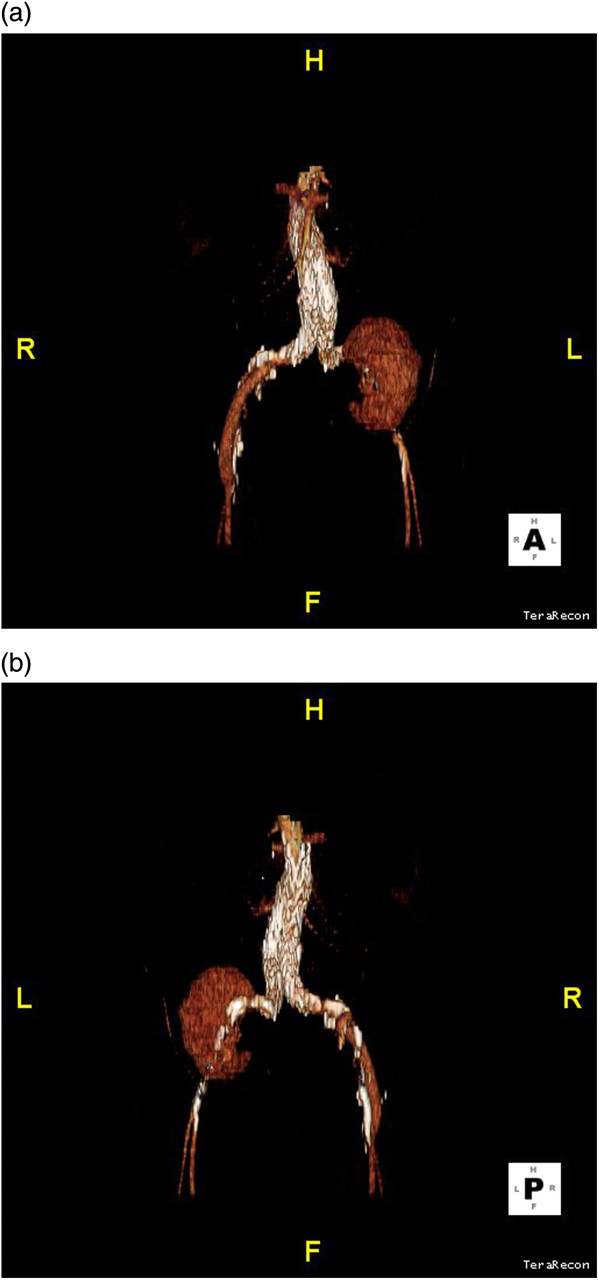
Completion angiograms revealed successful exclusion of the aneurysm and maintenance of perfusion to the transplant kidney (Figure 4). A total of 50 cm3 of omnipaque contrast agent was used. No blood transfusion was required and the patient did well postoperatively with resolution of her back pain and a minimal, but short-lived, serum creatinine elevation. She was discharged home on the fourth postoperative day. She continues to do well six months postoperatively, with follow-up CT scans showing good endograft placement with no endoleak and a well-perfused transplant kidney (Figure 5). Her renal function remains stable.
Completion angiogram showing placement of the left limb of the bifurcated endograft in the left common iliac artery and maintenance of perfusion of the left internal iliac artery and the pelvic transplant kidney Three-dimensional reconstructions of a postoperative (6 months) computed tomography scan showing successful aneurysm exclusion and maintenance of perfusion to the transplant kidney. (a) anterior view; (b) posterior view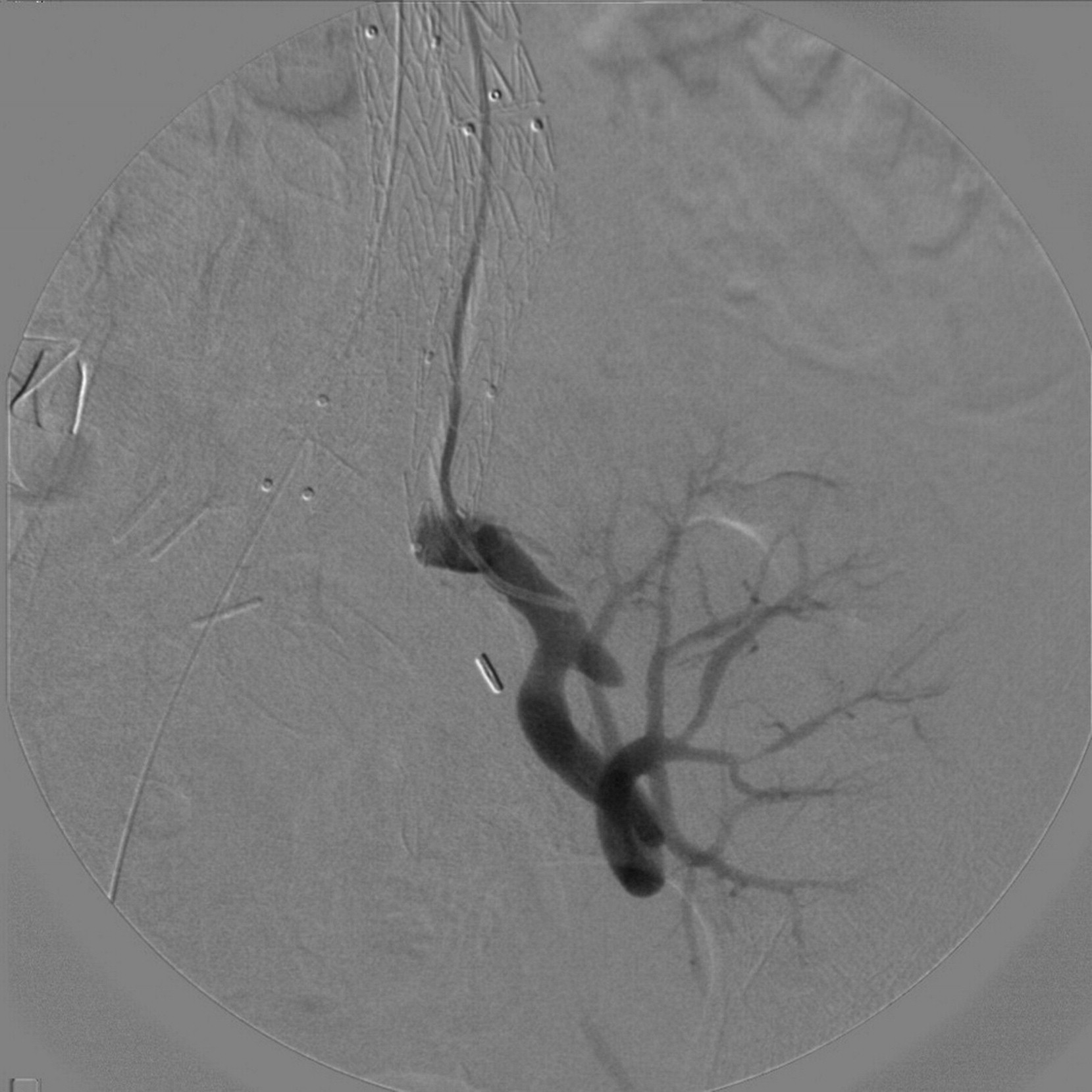
Discussion
Endovascular repair is the preferred method of repair when AAAs lie proximal to a pelvic transplant kidney. 1 A major advantage over open repair is the near complete absence of any renal ischemia, other than the short time periods when the stent graft is ballooned. However, when access vessels are inadequate, some innovative strategies are necessary, as with the present case.
In the case described, the small caliber contralateral (to the transplant kidney) external iliac arteries necessitated the surgical placement of a common iliac artery conduit that allowed delivery of the bifurcated main body of the endograft. The ipsilateral (to the transplant kidney) external iliac artery occlusion prevented femoral delivery of the contralateral limb and we were concerned that a retroperitoneal approach to the common iliac artery might increase the risk of kidney injury. In addition, we were concerned that an interventional approach and stent placement in the external iliac artery might also cause damage at the level of the renal artery anastomosis. Our strategy was to deliver this limb as one would deliver a bridging covered stent in a branched thoracoabdominal repair. 4 A conduit was placed on the left subclavian artery to shorten the delivery distance and to avoid traversing the aortic arch. Once the common iliac artery was cannulated, the internal iliac artery was cannulated and the stiff wire was placed carefully to avoid injury to the transplant kidney artery. The distal of the two Endurant limbs was introduced first with the nosecone positioned in the internal iliac artery to permit for sufficient overlap in the common iliac artery during deployment.
The Endurant stent graft system has been used for several years in Europe and Canada and has recently received approval in the USA. Early results are favorable. 5 The flexible delivery system has allowed for other novel delivery methods including up-and-over the aortic bifurcation to treat an internal iliac artery aneurysm. 6 As mentioned previously, there are other reports of antegrade deployment of stent grafts via a carotid approach. 2,3,7 Unlike the present case, however, these cases required customization of the stent graft or deployment and reverse loading. This was not necessary in our case because of the configuration of the Endurant limbs and the diameters of the recipient common iliac artery.
One concern regarding our approach is the diminished outflow that the external iliac artery occlusion provides the iliac limb. Outflow is via the renal transplant artery and any decrease in flow will result in allograft dysfunction or loss. The renal artery is a low resistance vessel, however, and should provide adequate outflow to maintain patency of the endograft limb, despite the external iliac artery occlusion. Endograft limb thrombosis has been observed to occur in up to 7.2% of cases and is related to the use of first-generation endografts, younger patients and limb kinking. 8 This patient will be subjected to serial CT scan surveillance and any evidence of graft kinking will be intervened upon promptly to ensure allograft survival. At least in the short term, this approach has proven effective in this patient, but it is yet to be determined whether or not it proves successful in the longer term.
Conclusion
Endovascular repair remains the method of choice for aneurysms proximal to pelvic transplant kidneys. However, when faced with challenging and suboptimal access, vessel anatomy innovative maneuvers are necessary and facilitated by advances in endograft technology. The present case illustrates that antegrade deployment of a bifurcated endograft limb is possible, similar to the techniques learned with branched endovascular thoracoabdominal repairs.